
Abstract
Trauma exposure and posttraumatic stress symptoms (PTSS) are established risk factors for poorer physical health. Prior work has focused on childhood adversities and PTSS in relation to physical health conditions, but trauma exposure over the lifespan has been overlooked. Further, the associations between trauma and PTSS and other physical health markers, such as diet and exercise, are less clear. Very little is known regarding how different trauma types (i.e., interpersonal, non-interpersonal), may be tied to aspects of physical health. To expand this area of research, this study aimed to: (a) examine the links between cumulative trauma and PTSS, and body mass index (BMI), diet, and exercise; and (b) investigate the relations between interpersonal and non-interpersonal trauma and these three health indices, while controlling for PTSS. Participants were 493 Midwestern University students (Mage = 23.87, standard deviation [SD] = 6.90, range = 18–63; 79.3% female; 57.4% White). Cumulative trauma corresponded with higher BMIs and less exercise use (B = 0.10; B = −0.09), while PTSS were unrelated. Conversely, PTSS were tied to greater consumption of added sugars (B = 0.11), and cumulative trauma was not linked with diet. Interpersonal and non-interpersonal traumas were not tied to BMI or exercise, although interpersonal trauma and PTSS were linked with greater sugar intake and non-interpersonal trauma was associated with fruit and vegetable consumption. Trauma exposure and PTSS may have complicated and distinct associations with physical health indices, such as BMI, diet, and exercise, and additional research is needed to further parse out these relations.
In the United States, epidemiological studies show that 89.7% of adults report experiencing at least one Criterion A traumatic event in their lifetime (Kilpatrick et al., 2013). Posttraumatic stress disorder (PTSD) is often thought of as the primary outcome of trauma exposure, but there are also numerous non-psychological consequences that have been associated with PTSD, including obesity, diabetes, lung disease, and cardiovascular disease (Brewerton et al, 2015; Garfin et al., 2018; Roberts et al., 2015; Ryder et al., 2018; Sumner et al., 2015). To date, there has been a prior focus on the relationships between specific child maltreatment types (Brewerton et al., 2015; Gooding et al., 2015; Rodgers et al., 2004) or adverse childhood experiences (ACEs; Gavrieli et al., 2015; Monnat & Chandler, 2015) and indices of health, such as body mass index (BMI), diet, and physical activity. This important work has demonstrated that childhood adversity has the potential for a lasting and serious toll on physical health. Yet, much less is known regarding how trauma exposure throughout the lifespan may correspond with physical health markers, even though it may be more directly impactful.
Interpersonal traumas, such as sexual or physical assault, have been specifically linked with poorer physical health (Brewerton et al., 2015; Gooding et al., 2015); however, the possible physical health consequences of non-interpersonal traumas (e.g., natural disaster, car accidents) have been overlooked. Non-interpersonal trauma exposures are the most commonly reported traumatic events (Kilpatrick et al., 2013), and thus, also merit investigation. As interpersonal trauma is associated with more severe psychological outcomes (Fowler et al., 2013; Spinazzola et al., 2018; Young & Widom, 2014), it is also critical to determine whether interpersonal trauma differentially relates to physical health outcomes compared to non-interpersonal traumas. The present study therefore sought to: (a) investigate the relations between cumulative trauma exposure and three indices of physical health (i.e., BMI, diet, and exercise), as these health markers have received sparse attention in the prior literature; and (b) examine the associations between interpersonal and non-interpersonal trauma, and the three health outcomes.
Trauma Exposure and Physical Health Indices
As noted, PTSD has been strongly associated with poorer physical health (Brewerton et al., 2015; Gooding et al., 2015; Schnurr et al., 2014). This is understandable as PTSD is thought to negatively impact the functioning of the hypothalamic-pituitary-adrenal (HPA) axis, the main biological network that regulates the stress response (De Bellis & Zisk, 2014; Schnurr & Green, 2004). Persistent activation of the HPA axis following trauma exposure is related to poorer health given the negative impact on one’s body through their autonomic nervous system and immune system (McEwen & Gianaros, 2010; Shonkoff et al., 2009). Prior theoretical and empirical work has emphasized that individuals with PTSD have trauma-related biological (e.g., dysregulation of the HPA axis) and psychological (e.g., trauma-related distress) impacts, which may result in greater engagement in unhealthy behaviors (e.g., poor diet, lack of exercise), thereby elevating one’s risk for poorer physical health and disease (Schnurr & Green, 2004; Schnurr et al., 2014). Consistent relations between PTSD/posttraumatic stress symptoms (PTSS) and health outcomes have been identified, and yet, potential ties between trauma exposure and indices of health have been examined less frequently, despite critical distinctions between trauma exposure and PTSS.
BMI is a commonly used index of health and elevated BMIs are tied to a variety of serious health conditions, such as obesity, cancer, diabetes, cardiovascular disease, stroke, and hypertension (Bhaskaran et al., 2014; Brewerton et al., 2015; Kim et al., 2014; Monnat & Chandler, 2015; Sumner et al., 2015). BMI is a body fat classification tool where less than 18.5 is considered underweight, 18.5 to 24.9 is normal, 25 to 29.9 is overweight, 30 to 39.9 is obese, and greater than 40 is considered extreme obesity (Centers for Disease Control and Prevention [CDC], 2020). Most of the existing research on trauma exposure and BMI has focused either on specific childhood trauma types (e.g., child physical [CPA] or sexual abuse [CSA], intimate partner violence) or more broadly on early adversities, such as ACEs. For instance, ACEs have been associated with higher BMIs, along with greater weight circumference and body fat percentages (Gavrieli et al., 2015). Cumulative childhood adversity may place individuals at greater risk for elevated BMI as adults; however, this study did not examine or control for other forms of childhood trauma or trauma exposure in adulthood. In one of the few studies to account for adult trauma exposure, Brewerton et al. (2015) investigated specific trauma types and reported that CSA, cumulative child abuse, and rape in adulthood were each linked with extreme obesity, with rape in adulthood being the most strongly related to elevated BMI. This study suggests that adult trauma exposure may therefore be more impactful in understanding health among adults. Additional work is needed to examine trauma exposure across the lifespan and BMI, in addition to other health markers, as these findings may have critical public health implications.
Like BMI, dietary intake is another key contributing factor to physical health. Dietary factors (e.g., caloric intake, consumption of added sugars, fruit, vegetables) are associated with a range of dangerous health outcomes, including obesity, heart disease, type 2 diabetes, certain cancers, and increased risk for stroke (National Center for Chronic Disease Prevention and Health Promotion, 2021). At this time, the links between trauma exposure and dietary factors have received scant attention; however, a preliminary report observed that child maltreatment, was tied to poorer diet quality (e.g., fewer fruits and vegetables, more processed meat, and sugary beverages) in adults (Gavrieli et al., 2015). Here, specific exposure to CPA, emotional abuse, and neglect were also associated with poorer diet quality, indicating the importance of examining specific trauma types as well (Gavrieli et al., 2015). Nevertheless, this study did not account for current level of trauma symptoms. Further research is needed to better understand the potential relations between cumulative trauma exposure, trauma types, and diet while also considering the role of PTSD. To the authors’ knowledge, the relationships between specific types of trauma exposure and diet are unknown, despite the potential for poorer diet to be linked with long-term health consequences (Brewerton et al., 2015; Roberts et al., 2015).
Beyond BMI and diet, another relevant aspect to one’s physical health and well-being is engagement in physical activity. Trauma exposure has been tied to less exercise use overall in a preliminary study (Smith-Marek et al., 2016). Nevertheless, in the small literature to date, cumulative trauma exposure has not been consistently related to the specific aspects of exercise (e.g., the intensity, frequency, or duration of activity; for a review, see Lee and Park 2018) and further work is needed. A few studies have also observed that specific trauma types may have differing associations with exercise. CPA has been tied to less exercise among female veterans (Rodgers et al., 2004). Similarly, CPA and emotional abuse have been linked with a lack of physical activity among adolescents (Chen et al., 2020). Presently, the role of specific trauma types beyond maltreatment have not been examined in relation to exercise, to the authors’ knowledge. This gap in the literature is noteworthy, as specific types of interpersonal trauma in adulthood, such as rape, have also been strongly linked with poorer physical health functioning (Brewerton et al., 2015). There is also no known work focused on exercise among individuals exposed to non-interpersonal trauma, which would also further enhance our understanding of the unique ties between types of trauma exposure and engagement in physical activity.
PTSS and Physical Health Indices
The preponderance of the existing research on trauma and physical health outcomes has focused on either PTSD or childhood trauma, without account for PTSD (for reviews, see Lee & Park, 2018; Schnurr et al., 2014). While informative, it is consequently challenging to distinguish whether physical health outcomes are the result of experiencing a traumatic event or are more strongly tied to trauma-related symptoms. PTSS have been previously related to poorer diet, higher obesity, and reduced physical activity (for a meta-analysis, see van den Berk-Clark et al., 2018). Moreover, the onset of PTSS may influence one’s BMI trajectory over time. The presence of at least four PTSD symptoms was associated with a faster increase in BMI over the course of 16 years, along with a greater risk for becoming overweight or obese (Kubzansky et al., 2014). PTSS have also been found to be predictive of a poorer diet over a 20-year period (Kim et al., 2021), indicating that an unhealthy diet may be one pathway that ties PTSS with more chronic health problems. Critically, the longitudinal nature of this research also signals that PTSD may be a driver of these physical health changes.
PTSD includes numerous symptoms, such as changes in mood, increased hyperarousal, and increased reactivity, and these difficulties may make engagement in exercise more challenging. Indeed, individuals with a PTSD diagnosis have been reported to be 22% less likely to be physically active than the general population (de Assis et al., 2008) and engage in less vigorous exercise (Godfrey et al., 2013). There also appears to be a dose-response relationship where exercise engagement decreases as the severity of PTSS increases (Vujanovic et al., 2013). Significant reductions in exercise have also been identified in the first year after a PTSD diagnosis (Talbot et al., 2014). Yet, it is unclear whether trauma-exposed individuals without PTSD also participate in less physical activity. Although there is certainly overlap between trauma exposure and PTSS, very few trauma-exposed individuals meet PTSD criteria, but most individuals will experience at least one traumatic event in the course of their lifetime (American Psychiatric Association, 2013). It is therefore critical to determine the unique implications of both trauma exposure and PTSD as they may substantially differ in their relations with physical health outcomes. It is also vital to study the potential physical health consequences associated with trauma exposure independent of PTSS, as this may reveal an at-risk population that is currently understudied.
Current Study
There is compelling evidence that childhood maltreatment and ACEs or PTSS are risk factors for longer-term poorer health conditions (Brewerton et al., 2015; Chen et al., 2020; Garfin et al., 2018; Monnat & Chandler, 2015; Roberts et al., 2015; Ryder et al., 2018); yet, there is a lack of understanding of how trauma exposure over the lifespan may correspond with physical heath. Additionally, prior work has not examined both trauma exposure and current trauma symptoms in tandem and research is still needed to investigate cumulative trauma and PTSS to determine how they may be differentially tied to physical health. Further, there may be distinctions between trauma types and health outcomes, and to the authors’ knowledge the specific links between interpersonal and non-interpersonal trauma types and physical health are unexplored. Finally, there is very limited work regarding trauma exposure and other key health outcomes outside of BMI, such as diet and exercise.
The first aim of this study was to extend the existing literature on trauma exposure, PTSS, and physical health by examining cumulative trauma and their associations with BMI, diet, and exercise. Cumulative trauma was hypothesized to be linked with greater BMI, greater consumption of added sugar, fewer intake of fruits and vegetables, and less engagement in exercise. PTSS was also expected to be related to all poorer health outcomes. The second study aim was to investigate the relations of interpersonal and non-interpersonal trauma and physical health. Both interpersonal and non-interpersonal trauma exposure were expected to be associated with worse health outcomes for BMI, diet, and exercise. Interpersonal traumas were hypothesized to evince stronger ties to the health outcomes than non-interpersonal trauma.
Method
Participants
Four hundred and ninety-three undergraduate students who were recruited from a Psychology Human Subjects Pool participated in this study. Participants ranged in age from 18 to 63 (Mage = 23.87, standard deviation [SD] = 6.90) and largely included individuals identifying as female (79.3%). More than half of participants self-identified as White (57.4%), and 29.3% identified as Black or African American, 7.4% as multiracial, 3.7% as Asian, 1.6% as Middle Eastern, and 0.8% as American Indian or Alaska Native. Six percent (6.2%) of participants identified as being Hispanic/Latinx.
Procedures
This study used data that were collected from a research study at a Midwestern University investigating trauma exposure, beliefs about race, and health behaviors (n = 516). Participants self-selected into the study and completed the survey online using Qualtrics. All participants received psychology course credit for their participation. Inclusion criteria for the present study were (a) being a student at the university and (b) being exposed to a traumatic event (n = 23), resulting in the final sample of 493 participants. There were no exclusion criteria. All study procedures were approved by the IRB University of Missouri-St. Louis.
Measures
Demographics
Demographic information including age, sex, race, ethnicity, annual household income, marital status, and employment status were collected through a brief questionnaire.
Life Event Checklist for DSM-5
Each participant completed the Life Event Checklist for DSM-5 (LEC-5) to assess for lifetime trauma exposure (Weathers et al., 2013). The LEC-5 measures one’s exposure to 16 traumatic or stressful events that could potentially result in PTSD. An additional item is also included for participants to endorse their exposure to a potentially traumatic event that was not captured in the other 16 items. Participants indicate if the event “Happened to me,” “Witnessed it,” “Learned about it,” “Part of my job,” “Not Sure,” or “Doesn’t Apply.” Cumulative trauma exposure was summed to create a total score (range = 0–17). Scores were also calculated for interpersonal trauma (Range 0–9) and non-interpersonal trauma exposure (range = 0–7). Physical and sexual assault, other unwanted sexual experiences, assault with a weapon, combat or exposure to a war zone, being held in captivity, severe human suffering, sudden violent/accidental death, or serious injury, harm, or death that you caused to someone else were coded as interpersonal trauma. Exposure to natural disasters, fire and explosion, transportation accident, serious accident, exposure to toxic substances, and life-threatening illness/injury were considered non-interpersonal traumatic events. The “other” item was not included in either the interpersonal or non-interpersonal trauma exposure score.
PTSD Checklist for DSM-5
Participants completed the PTSD Checklist for DSM-5 (PCL-5; Weathers et al., 2013), which is a 20-item self-report measure designed to assess DSM-5 PTSD symptoms experienced in the last month. Participants rate their distress levels on a 5-point Likert-type scale, 0 = Not at all to 4 = Extremely. The scores on the PCL-5 range from 0 to 80, with greater scores indicating higher levels of PTSS. The PCL-5 has established evidence of good reliability and validity (Wortmann et al., 2016). For the present study, Cronbach’s α was excellent (α = .92).
Body Mass Index
Height and weight information were gathered by each participant during the survey. This information was utilized to calculate each individual’s BMI. BMI was calculated manually using the CDC’s Adult BMI Calculator (CDC, 2020). The CDC uses set guidelines for their standard BMI cut-offs—<18.5 = underweight, 18.5 to 24.9 = normal, 25 to 29.9 = overweight, 30 to 39.9 = obese, and >40 = extreme obesity (CDC, 2020). BMI was assessed continuously, where greater scores were tied to higher BMIs.
Dietary Screener Questionnaire
Each participant completed the Dietary Screener Questionnaire (DSQ; National Health and Nutrition Examination Survey, 2009), which is a 26-item self-report screener that is used to assess dietary intake across several dimensions (e.g., consumption of fruits and vegetables, added sugars, dairy, fiber). Participants rate their intake for each item on a 9-point Likert-type scale, where (1 = Never to 9 = 2 or more times per day). The scores on the DSQ range from 0 to 234. The DSQ has been shown to have adequate reliability and validity (Thompson et al., 2017). For the present study, the authors used two dimensions to measure diet, specifically, fruit and vegetable intake and the consumption of added sugars. A sum score was calculated for each dimension used in the study, which included 7 items for consumption of fruits and vegetables and 10 items for consumption of added sugars.
Exercise Screener
Participants completed a brief 5-item screener of their engagement in physical activity per week based on the Global Physical Activity Questionnaire (World Health Organization, 2002). Participants reported whether or not they currently regularly engage in an exercise program (yes or no), and if so, the total time exercising per week. Participants also reported the types of exercise they engage in (e.g., lifting weights, walking, running, hiking, swimming, playing team sports) per week. For the present study, the total amount of time in minutes spent exercising each week was summed for the analyses.
Data Analytic Plan
All data analyses were conducted using SPSS 27. Prior to running analyses, the data were cleaned, assessed for normality and other violations of statistical assumptions such as multicollinearity, and checked for missingness and attention checks. A small portion of cases had missing data (<1%) on participant’s age and was imputed using mean imputation. Participant’s demographic variables, such as age, sex (1 = Men, 2 = Women), racial minority status (0 = Racial Minority, 1 = White), ethnicity (1 = Hispanic/Latinx, 2 = not Hispanic/Latinx), and annual family income were examined as potential covariates using bivariate correlations and independent samples t-tests (Table 1). Factors that were related to the dependent variables were included as covariates. Two sets of four linear regressions were computed, one for cumulative trauma and the second with interpersonal and non-interpersonal traumas, and the physical health markers (i.e., BMI, exercise use, fruit and vegetable intake, and sugar consumption) (Tables 2 and 3). PTSS was included as an independent variable for both models. An a priori power analysis using G*Power indicated that a sample size of 122 would provide 80% statistical power to detect a medium effect size.
Bivariate Correlations.
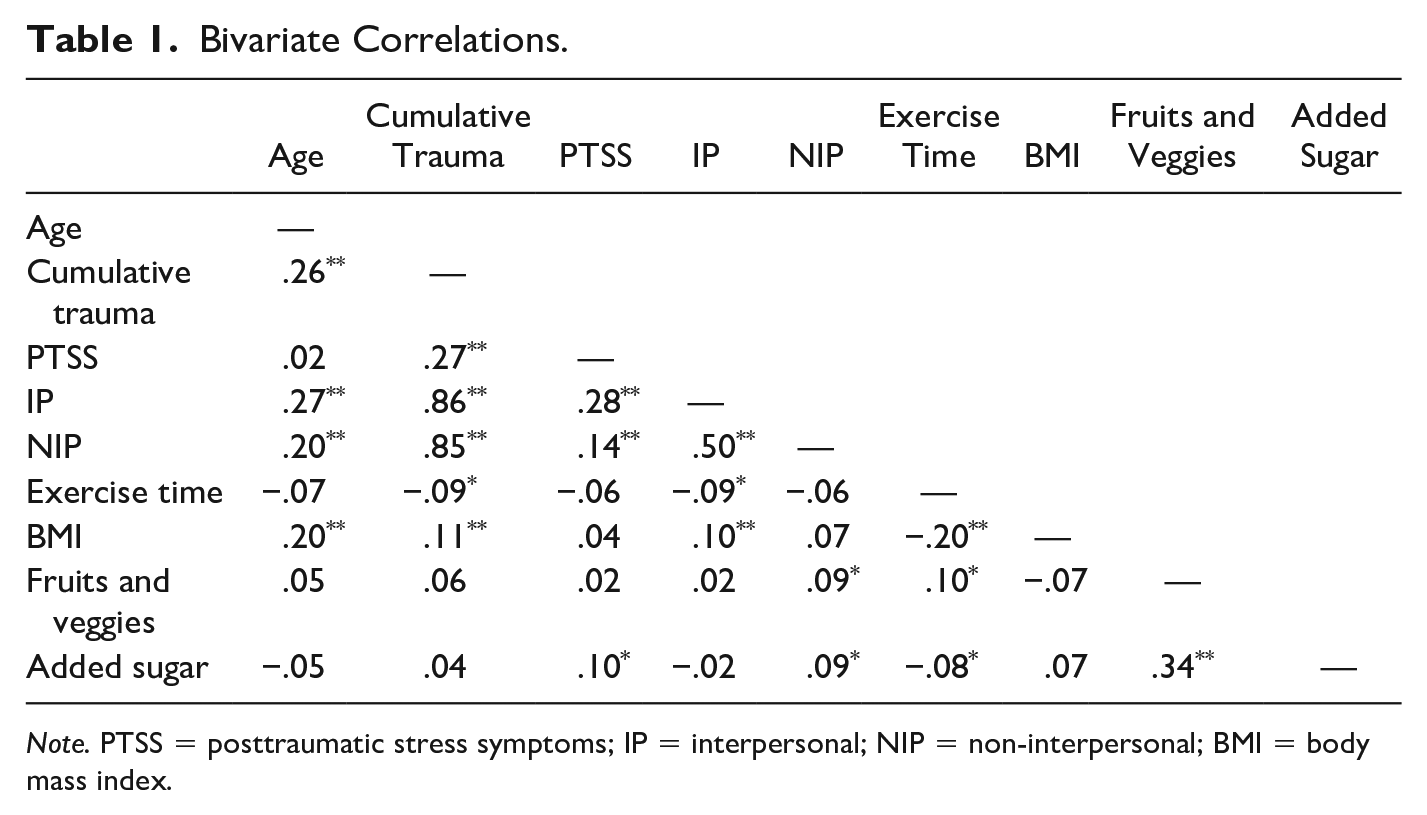
Note. PTSS = posttraumatic stress symptoms; IP = interpersonal; NIP = non-interpersonal; BMI = body mass index.
Results From Linear Regression Models for Cumulative Trauma.
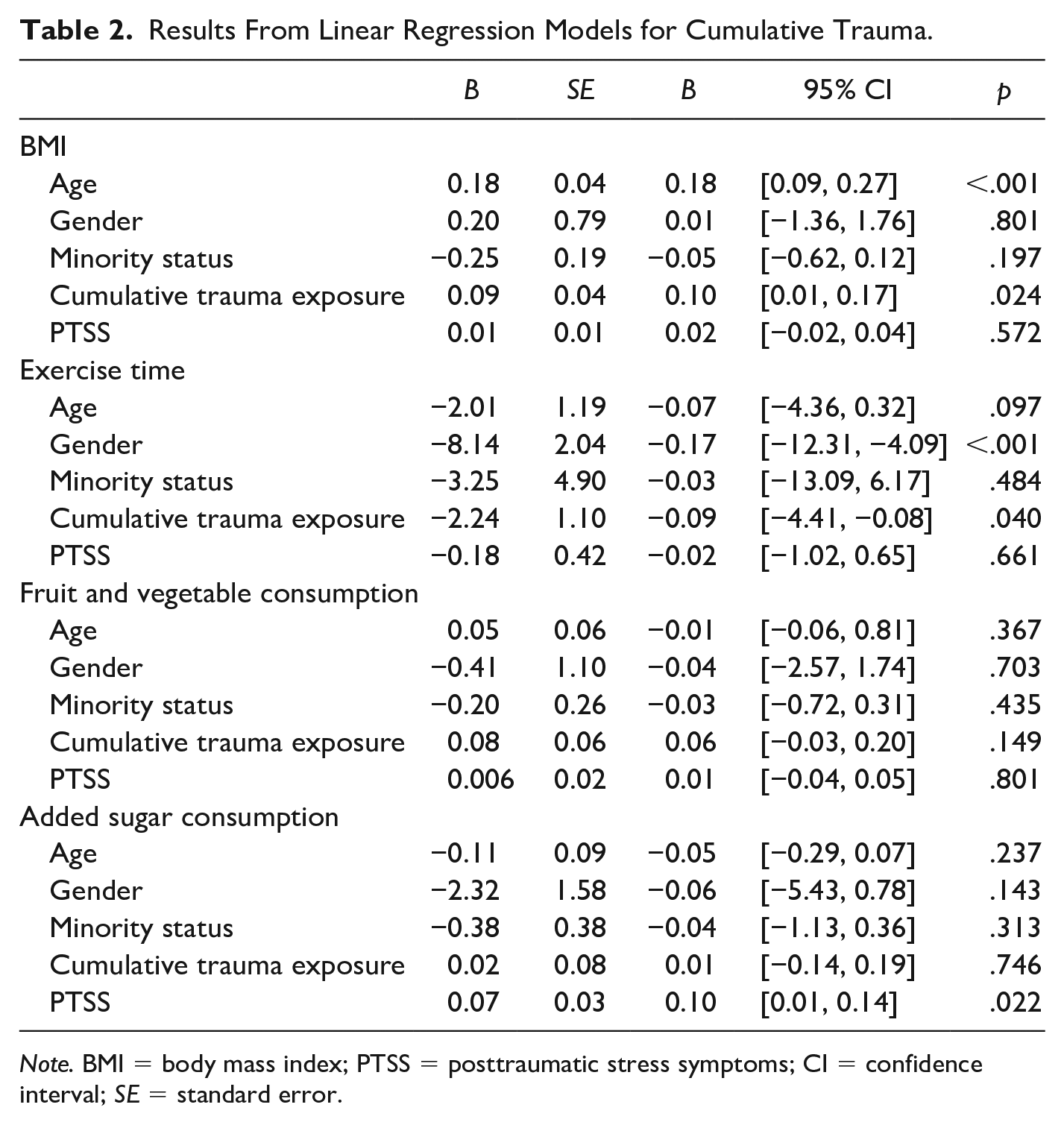
Note. BMI = body mass index; PTSS = posttraumatic stress symptoms; CI = confidence interval; SE = standard error.
Results From Linear Regression Models for Interpersonal and Non-Interpersonal Trauma.

Note. BMI = body mass index; PTSS = posttraumatic stress symptoms; CI = confidence interval; SE = standard error.
Results
Preliminary Analyses
Mean BMI in the present sample was 27.07 (SD = 7.05, range = 15.90-58.10). Forty-two percent (42.8%) of the participants reported height and weight measurements that were consistent with a normal BMI, while 57.2% had BMIs that were outside of the normal BMI range: 2.7% underweight, 27.5 overweight, 20.7% obese, and 6.2% extremely obese. Participants reported being exposed to an average of five traumatic events (M = 5.17, SD = 3.40, range = 1–17), including an average of two interpersonal traumas M = 2.14, SD = 1.94, range = 0–9) and over two non-interpersonal traumas (M = 2.44, SD = 1.68, range = 0–7). Mean levels of PTSS on the PCL-5 were 33.34 (SD = 19.65, range = 0–80). Age was related to trauma exposure (r = .19, p = .001) and BMI (r = .20, p = .001), but it was not associated with PTSS, exercise time, or diet (i.e., number of fruits and vegetables consumed, added sugars). Women reported higher levels of PTSS and lower levels of exercise time than men. Women and men did not differ by BMI or diet. Participants did not differ on BMIs by race outside of Asian participants having lower BMIs than Black participants. Racial groups also did not differ on cumulative trauma, PTSS, exercise time, or dietary factors. Age, gender, and race were included as covariates in the model.
Cumulative Trauma Regressions
The model for cumulative trauma accounted for a significant amount of variance in BMIs, F(5, 487) = 5.36, p < .001, r2 = .05, adj. r2 = .04. Age was positively related to BMI. As expected, cumulative trauma was associated with BMI, with greater trauma exposure relating to elevated BMIs. However, gender, race, and PTSS were unrelated. The regression model focused on added sugar was not significant, F(5, 487) = 1.89, p = .09, r2 = .01, adj. r2 = .009; however, higher levels of PTSS were associated with greater consumption of added sugar. Level of trauma exposure was not. When fruit and vegetable consumption was examined, the regression model that included cumulative trauma was not significant, F(5, 483) = .87, p = .496, r2 = .01, adj. r2 = .009. Neither cumulative trauma, nor PTSS, were tied to fruit and vegetable intake. The regression model examining exercise time was significant, F(5, 487) = 4.84, p < .001, r2 = .05, adj. r2 = .04. Cumulative trauma was tied to fewer exercise minutes per week, whereas PTSS was unrelated. Men also reported engaging in more exercise time than women.
Interpersonal Versus Non-interpersonal Regressions
When interpersonal trauma exposure was contrasted with non-interpersonal trauma, the overall model was significant, F(6, 486) = 4.24, p < .001, r2 = .04, adj. r2 = .03. However, neither were specifically related to BMIs and only age was a significant factor. Levels of PTSS, along with race and gender, were also unrelated. The model for added sugar was significant, F(6, 486) = 3.12, p = .005, r2 = .05, adj. r2 = .04. Here, greater interpersonal trauma exposure was related to lower levels of sugar consumption whereas non-interpersonal traumas were associated with greater sugar consumption. Higher levels of PTSS were tied to greater sugar intake. When vegetable and fruit intake was investigated, the overall model was not significant, F(6, 486) = 1.03, p = .402, r2 = .02, adj. r2 = .01. Yet, levels of non-interpersonal trauma exposure were positively related to greater fruit and vegetable consumption, in contrast to expectations. Surprisingly, levels of interpersonal trauma and PTSS, were unrelated. The regression model examining exercise time was significant, F(6, 486) = 4.41, p < .001, r2 = .03, adj. r2 = .02; yet, only gender evinced an association with exercise time. Both forms of trauma exposure and PTSS did not correspond with exercise minutes per week.
Discussion
Even though trauma and PTSD may increase the risk for poorer physical health, much of the literature has focused on childhood maltreatment or ACEs or PTSD and the links between physical health and lifetime trauma exposure, along with non-interpersonal traumas, have received less attention. Trauma that occurs after childhood is paramount to study, given its closer time frame with adult physical health. Critically, the majority of the literature has focused exclusively on the role of PTSD, not accounted for trauma symptoms at all, and work is still needed to investigate both in tandem to more precisely pinpoint the precipitant of poor physical health. There may also be key distinctions between interpersonal and non-interpersonal traumas and physical health. The aims of the present study were to examine the associations between cumulative trauma and physical health markers (i.e., BMI, fruit and vegetable intake, added sugar consumption, and exercise), as well as to investigate the distinct relationships between interpersonal and non-interpersonal trauma exposure and these health indices.
Cumulative trauma was related to higher BMIs, along with fewer exercise minutes, as expected. Prior studies examining ACEs or forms of maltreatment have similarly observed that experiencing childhood adversities or traumatic events are tied to higher BMIs (Brewerton et al., 2015; Gavrieli et al., 2015), and this finding expands this literature to demonstrate that cumulative lifetime trauma is also linked with higher BMIs. Critically, we found that this association remained after accounting for current levels of trauma-related symptoms. This is also the first known study to examine cumulative lifetime trauma and exercise, as much of the extant work has focused on specific trauma types and physical activity (Chen et al., 2020; Rodgers et al., 2004). Repeated exposure to stressful life events and trauma may increase vulnerability to less manageable stress levels and HPA axis disruptions, and this altered stress response can engender a variety of neurological, biological, and psychological changes. The summation of these collective negative impacts likely place trauma survivors at greater risk for poorer health behaviors possibly through the use of maladaptive coping strategies. This may include the use of emotional eating, or the tendency to eat or overeat in response to negative emotions (Evers et al., 2010), which has been tied to trauma exposure (Michopoulos et al., 2015). Longitudinal research is warranted to determine whether there are specific developmental windows or a number of trauma exposures that are associated with the greatest risk for weight and exercise changes. The timing of the trauma exposure in relation to diet and exercise modifications should also be assessed to help identify critical prevention periods. Perhaps there is an opportunity for intervention following trauma exposure to target the impact of experiencing the traumatic event before the onset of less healthy eating and exercise behaviors.
Approximately half of the participants in this study endorsed levels of PTSS that were at or above the clinical cut-off for probable PTSD based on the cut scores utilized in studies of college students (Blevins et al., 2015). Thus, the lack of an association between PTSS and BMIs was unexpected and not in line with prior research (Kubzansky et al., 2014); however, cumulative trauma was not controlled for in this previous work. As cumulative trauma was related to BMIs in the present study, it is unclear if PTSS would have remained linked with BMIs if these studies had accounted for cumulative trauma exposure. PTSS was also unrelated to exercise use, which aligns with some previous findings (Spitzer et al., 2010) but not others (de Assis et al., 2008; Godfrey et al. 2013). The inconsistency in the literature may be due to the presence of key sub-groups. As an example, those with more prominent symptoms of hyperarousal and hypervigilance feel “keyed up” or on edge, and therefore use exercise more frequently as a way to cope with hyperarousal difficulties. It is possible that others, however, may be more reluctant to engage in exercise due to these cardiovascular changes. Thus, it may be prudent to tease apart the specific PTSD symptom clusters in future research to answer this question. As another example, individuals with comorbid PTSD and depression may be less likely to exercise. Depression is strongly related to negative physical health, including increased risk for obesity (Michopoulos et al., 2015). The present study did not examine levels of depressive symptoms, and perhaps these mood difficulties may be relevant in the link between trauma exposure, PTSS, and both BMI and exercise.
Interestingly, neither of the dietary factors (i.e., added sugar and fruit/vegetable consumption) were related to cumulative trauma. It is possible that other indices of poorer diet, such as greater consumption of carbohydrates or larger portions, would have emerged as being tied to cumulative trauma, given the significant BMI finding. Individuals exposed to more traumatic events may not be more prone to eating higher levels of sugar or fewer fruits and vegetables, but they may be eating larger portions of food, or more calorie-dense “comfort food,” consistent with the concept of “emotional eating.” Higher levels of PTSS were related to greater added sugar consumption. Perhaps higher levels of trauma symptoms, through biological changes and the “fight or flight” response being activated more often, may prompt the individual to experience greater sugar cravings, as these cravings are part of the stress response. Taken together, more work is needed to examine both trauma exposure and PTSS, along with depression, and additional dietary aspects.
When interpersonal and non-interpersonal traumas were specifically investigated, neither demonstrated unique associations with BMI, nor with exercise. These findings may suggest that cumulative trauma is more important to consider than the specific forms of trauma; however, replication of this preliminary finding is needed. There may also be distinctions in terms of specific types of interpersonal or non-interpersonal traumas, such as sexual assault or traumatic grief, that are more strongly related to health outcomes. Interestingly, non-interpersonal traumas and PTSS were associated with greater sugar consumption, whereas interpersonal trauma was tied to lower sugar intake. The finding regarding interpersonal trauma may be spurious, as it is not clear why interpersonal traumas would be tied to lower consumption of added sugar. However, it is possible that certain trauma types, such as sexual trauma, may be associated with body image issues and a heightened need for control over one’s body (Dyer et al., 2013). Also unexpectedly, non-interpersonal trauma was related to greater fruit and vegetable consumption. As this form of trauma was also linked with greater sugar intake and BMIs, non-interpersonal traumas may be more strongly related to comfort eating, resulting in higher weight and greater food consumption more generally. Interpersonal trauma and PTSS were unrelated to fruit and vegetable consumption, which may indicate that other dietary factors, such as sugar consumption, are more relevant in understanding dietary choices in the context of interpersonal trauma. Overall, this pattern of findings may further support the idea that there is specificity in terms of trauma types, PTSS, and physical health markers.
Limitations
The results of the present study should be interpreted within the context of several limitations. The sample consisted of undergraduate students and was largely female (79.3%), and thus, is not representative of the United States. There may be differences in the associations between trauma exposure, PTSS, and physical health among other sub-populations, which should be prioritized in future work. Given the cross-sectional nature of the study, we have no way to determine if individuals exposed to trauma, or those with PTSS, have had weight changes or modified their diet or exercise, as a result of these experiences. The reliance on self-report measures may have also impacted the findings. The LEC-5 includes an “other” item that limits the ability to determine whether participants experienced a DSM-5 Criterion A event. Self-report measures of diet and exercise may be problematic as some participants may be prone to social desirability, be unaware of their height and weight, and/or have limited insight into their dietary intake. Future research would benefit from the use of medical data to investigate trauma and health indices to ensure greater accuracy. While BMI is a commonly used index of health linked with a range of adverse health outcomes (Bhaskaran et al., 2014; Brewerton et al., 2015; Kim et al., 2014; Monnat & Chandler, 2015; Sumner et al., 2015), it is an imperfect measurement tool as other factors are relevant in determining BMI (e.g., muscle mass, bone density, etc.).
Future Directions and Conclusions
The present study nevertheless is the first known investigation of the distinct associations between interpersonal and non-interpersonal traumas and physical health indices (i.e., BMI, diet, and exercise use). Moreover, it was one of very few studies to examine the ties between cumulative trauma exposure and these physical health markers, while accounting for PTSS, as opposed to focusing on specific maltreatment types or ACEs. Cumulative trauma was related to BMI and exercise use, whereas PTSS was not associated with either. Replication is warranted as cumulative trauma may have a weathering effect on health, such that exposure to additional traumatic events may adversely impact physical health and health behaviors over time compared to current levels of trauma symptoms. Dietary factors were largely unrelated to the variables of interest, although individuals with higher PTSS may be more likely to have greater sugar consumption. Interestingly, cumulative trauma appears to have a more robust relationship with health markers than interpersonal or non-interpersonal trauma did. Neither interpersonal nor non-interpersonal trauma evinced ties with BMI or exercise. Yet, this finding may be spurious, and it seems prudent to examine specific trauma types. Certain traumas, such as traumatic grief, may be more likely to engender depression, increasing risk for emotional eating and less exercise use. Work is still needed to explore distinctions between trauma types and physical health.
These results have several implications for future study that may improve our understanding of lifetime trauma exposure, PTSS, and physical health markers. Ongoing work in this area should utilize other sub-groups and more refined measures methods and it is important to parse out the roles of other psychopathology, such as depression or anxiety, as well as comorbid eating disorders. Other dietary factors should also be considered (e.g., carbohydrate intake, larger portions), as well as the type and/or duration of exercise. Longitudinal work is essential to determine whether the timing of trauma exposure(s) have a differing impact on weight, diet, and/or exercise in order to ensure that prevention efforts target trauma-related changes in physical health as timely as possible. There may be significant opportunities for trauma-focused intervention efforts to aid in managing changes in health behaviors that may lead to longer term consequences (e.g., significant weight changes) to help promote better physical health among trauma survivors.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research and/or authorship of this article.