
Abstract
Problem drinking and depression are common following sexual assault. The current study applied a coping motives model of drinking and examined the association between rape experiences and problem drinking serially mediated by depression symptoms and coping-depression drinking motives among Hispanic college women. A total of 330 college women were classified into a single rape experience (SGL) group (n = 44), a multiple rape experiences (MLT) group (n = 70), and a no sexual assault experience group (n = 221). Participants completed self-report measures online. Serial mediation analyses with multi-categorical predictors found that significantly increased alcohol consumptions in rape survivors compared to individuals with no sexual assault experience were largely explained by the serially connected underlying mechanisms of depression symptoms and coping-depression drinking motives. The prevalence rates of rape experiences in this Hispanic female sample are alarming, suggesting Hispanic college women as a particularly vulnerable group for rape. The current results contribute to a greater understanding of the effects of rape experiences on behavioral and emotional outcomes among young Hispanic women who have been underrepresented in sexual victimization research. The findings emphasize the importance of assessing depression symptoms and coping-depression drinking motives in Hispanic rape survivors to reduce risks for hazardous drinking behavior.
Introduction
Rape Experiences in the United States
Nearly 55% of women in the United States report experiencing sexual violence during their lifetime, according to the most recent report of the Centers for Disease Control and Prevention (CDC: Basile et al., 2022). Among sexual victimization types, research suggests that there may be a continuum of severity, with rape considered the most severe (e.g., Carretta and Burgess, 2013; Davis et al., 2014; Testa et al., 2004). For example, Testa et al. (2004) found that survivors rated completed rape as the most traumatic relative to other sexual victimization experiences. Davis et al. (2014) scored rank ordering (from unwanted sexual contact to attempted rape up to completed rape) and reported that higher severity scores were associated with more psychological symptoms including depression. Following previous research (e.g., Koss et al., 2007), in the current study, completed rape was defined as a nonconsenting experience of vaginal, anal, or oral intercourse or penetration with threat, physical force, or use of alcohol or drug.
Among adult women in the U.S., the lifetime prevalence of completed rape is 16.3% (CDC: Basile et al., 2022). Estimated prevalence rates of rape among college women vary, typically ranging from 10% to 20% (e.g., Carey et al., 2015; Krebs et al., 2016; Marsil et al., 2016). College women are also at high risk of sexual revictimization, with over 60% of female college sexual assault survivors reporting two or more sexual assault experiences (e.g., Katz et al., 2010; Walsh et al., 2020). These data suggest that rape and revictimization, particularly in young women, are serious concerns.
Sexual Victimization Among Hispanic Women
Research on sexual victimization is especially needed for the Hispanic community, which makes up approximately 18.7% of the U.S. population (U.S. Census Bureau, 2020) and is expected to reach 27.5% by 2060 (Vespa et al., 2020). Prevalence estimates of rape vary by minority group, with 19.7% of Hispanic women reporting lifetime rape (CDC: Basile et al., 2022). Sparse studies report prevalence of rape among Hispanic college women, reporting 16%–21% (Kalof, 2000; Yeater et al., 2016).
Hispanics are an underrepresented group in clinical research generally and in sexual assault research in particular. Most of the recent research on sexual victimization in young adults either did not report the ethnic composition of the sample or had an underrepresentation of Hispanic young adults, ranging between 2% and 11% (e.g., Chang et al., 2020; Rhew et al., 2017; Woerner et al., 2019). One notable exception is a recent study that recruited for even numbers of Caucasian, Black, and Hispanic college women (Rothman et al., 2021). Sexual assault research focusing on Hispanic women is desperately needed, particularly in light of findings that Hispanic female rape survivors experienced poor mental health compared to those without a sexual assault experience (Basile et al., 2015; Fedina et al., 2020).
Problem Drinking and Depression Symptoms as Significant Consequences of Rape Experiences
A range of negative psychological consequences, such as problem drinking and depression, are common following sexual assault, including rape (e.g., Campbell et al., 2009; Chang et al., 2020; Chang et al., 2015; Dir et al., 2021; Dworkin et al., 2017; Rothman et al., 2021). An association of problem drinking with various sexual victimization experiences has been well-documented (e.g., Dardis et al., 2021; Dworkin et al., 2017; Kaysen et al., 2006; Mouilso et al., 2012). Although different roles of alcohol use in sexual assault, including rape, are possible, such as alcohol use as a precursor to sexual victimization (e.g., Dardis et al., 2021; Mouilso et al., 2012), a consequence of sexual victimization (e.g., Dworkin et al., 2017), or both a predictor and a consequence (e.g., Kaysen et al., 2006), a meta-analytic study concluded that alcohol use was one of the identified consequences of sexual victimization (Dworkin et al., 2017). More recent empirical studies support this association in young adult sexual assault victims, including rape survivors (e.g., Chang et al., 2020; Rhew et al., 2017; Stappenbeck et al., 2023). For example, in their longitudinal study, Rhew et al. (2017) reported that severity and frequency of sexual assault experiences predicted increased alcohol consumption, with young women with MLT as the most vulnerable to subsequent alcohol misuse. Evidence also supports multiple victimization as a potential risk factor for developing problem drinking (Najdowski & Ullman, 2009; Walsh et al., 2014). In addition, Khantzian’s self-medication theory (1997) supports the association between past sexual victimization and current problem drinking. According to this theory, individuals who are experiencing psychological distress in response to a traumatic event may self-medicate with substances. The empirical results and theoretical formulations converge to suggest that alcohol use is best understood as a consequence of sexual victimization.
Reviews and meta-analytic studies find significantly elevated depression symptoms in sexual assault survivors compared to those without a sexual assault experience (Campbell et al., 2009; Dworkin et al., 2017) and suggest that sexual revictimization likely increases depression (Campbell et al., 2009). More recent studies confirm this. Dir and Colleagues (2021) found that over two-thirds of those with forcible sexual assault history reported clinically significant levels of depression. Rothman et al. (2021), in an ethnically diverse sample, found that women with a history of sexual assault during college, including over 60% of those reporting completed rape, had significantly higher depressive symptoms than those without a sexual assault experience during college. Chang et al. (2020) found sexual victimization was a predictor for negative psychological outcomes including depression symptoms and alcohol use in college women. In addition, history of MLT was significantly associated with the presence of a major depressive episode in college women (Zinzow et al., 2010). Altogether, it can be concluded that experiencing depression symptoms is a likely consequence of sexual assault including rape in women.
A Serial Mediation Model
It is not uncommon for female survivors of sexual assault, including rape, to experience both problem drinking and depression (e.g., Chang et al., 2020; Dir et al., 2021; Rhew et al., 2017; Rothman et al., 2021). Specific directional associations among sexual victimization and subsequent problem drinking and depression may be explained by introducing a coping motives model of drinking. A prominent motivational model of drinking (Cooper et al., 1995) suggests that drinking to cope is a strong motivational contributor to subsequent alcohol use, and negative emotions and tension reduction expectations are determinants of levels of drinking to cope for those 19 years or younger. Grant et al. (2007) elaborated on the model, adding drinking motives for specific forms of psychological distress, such as drinking motives to cope with depression. Taken together, we can hypothesize the following model: after experiencing rape, depression develops and expectations that alcohol will help alleviate depression symptoms leads to problematic alcohol use.
No research has examined the full proposed model of serial associations among rape experiences, depression, drinking to cope, and alcohol use, but limited research has examined sub-elements of the proposed model in sexually victimized young adults. A few studies (Ehlke et al., 2019; Fossos et al., 2011; Woerner et al., 2019) report an association between a history of sexual coercion specifically or a wide range of sexual assault experiences and alcohol use mediated by coping motives for drinking. Stappenbeck et al. (2023) reported coping motives as a mediator of the association between negative affect and increased drinking in women with different severity levels of victimization. These studies provide some evidence to support several components of the proposed model, but an investigation of the specific serial associations among rape experiences, depression, drinking to cope, and alcohol use is needed.
As noted above, rape is generally considered the most severe case of sexual assault (e.g., Carretta and Burgess, 2013; Rhew et al., 2017; Testa et al., 2004) and is typically associated with severe psychological and behavioral consequences. Moreover, revictimization is a potential risk factor for exacerbated psychological symptoms (e.g., Najdowski & Ullman, 2009). These facts suggest the importance of examining the effects of single and MLT within the model. Such an attempt could identify specific pathways among psychological and behavioral symptoms and drinking motives for rape survivors, which could then contribute to designing and developing preventive actions and interventions for rape survivors who are most likely to experience severe consequences.
The Current Study and Hypothesis
The current study sought to test a mediation model assessing the relationships between sexual victimization and alcohol use serially mediated by depression and coping-depression drinking motives in a sample of Hispanic women. It was hypothesized that the association between rape experiences and elevated alcohol use would be serially mediated by depression and coping-depression drinking motives (Figure 1).
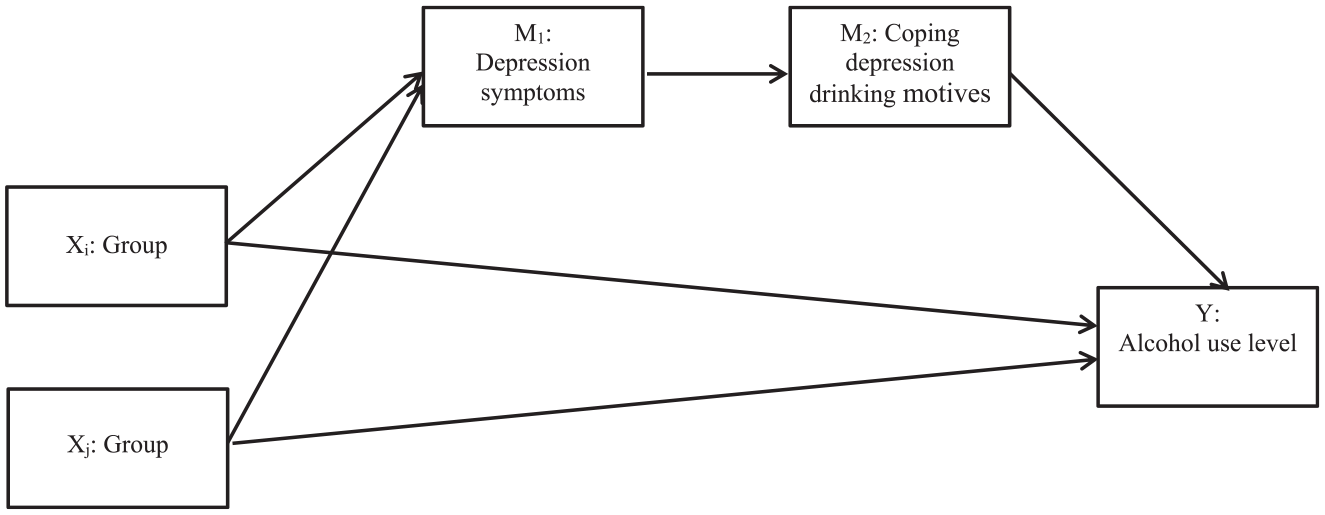
Hypothesized model.
Method
Procedure
The current study was conducted at a state university located in a south Texas region where over 90% of the student population is Hispanic, which gave us the opportunity to focus exclusively on Hispanic college women. This study was approved by the Institutional Review Board of the university. Hispanic college women who were 18 years or older were recruited from the subject pool of a psychology department at the university. Those who agreed to participate were directed to an online anonymous survey developed on Qualtrics (Qualtrics, Provo, UT, USA) and upon completion received course credit points as compensation.
Participants
A total of 405 Hispanic college women completed the survey. Hispanic women who reported at least one rape experience or no sexual assault experience were included in the current study (n = 330). Those women reporting a range of other sexual victimization experiences (n = 75) were outside the study scope and their data was excluded. The mean age of the final sample was 21.4 (SD = 4.58).
Measures
Sexual Experiences
The Sexual Experiences Survey-Short Victimization version (SES-SFV; Koss et al., 2007) asks about experiences of different types of unwanted sexual behaviors (e.g., fondling, attempted or completed oral, vaginal or anal penetration) and tactics used to obtain each outcome (e.g., coercion, intoxication, and threat or use of physical force). Participants indicated how many times (0, 1, 2, 3, or more times) in the past 12 months and how many times since age 17 they experienced each unwanted sexual behavior by each tactic. The current study used 17 years old (the age of consent in Texas) as an index year of age to count unwanted sexual experiences in adulthood. Individuals who reported at least one experience of oral sex, vaginal penetration, or anal penetration while being threatened, forced, or with alcohol since 17 years of age were identified as rape survivors.
Alcohol Use
The Alcohol Use Disorders Identification Test (AUDIT; Bohn et al., 1995) is a self-rated 10-item questionnaire with each item rated 0 to 4 for frequency of various drinking behaviors (e.g., “How often do you have a drink containing alcohol?,” “How often do you have six or more drinks on one occasion?”), giving a total score up to 40. A score of 1 to 7 suggests low-risk consumption according to World Health Organization guidelines. Scores from 8 to 14 suggest hazardous or harmful alcohol consumption and a score of 15 or more indicates the likelihood of alcohol dependence (moderate to severe alcohol use disorder). Several studies have shown its validity and reliability in the detection of hazardous drinking, alcohol misuse, and alcohol dependence (Bohn et al., 1995). Cronbach’s alpha for the scale for college students was .81 (Kokotailo et al., 2004). The Cronbach’s alpha for the current sample was .74.
Drinking Motivation
The Modified Drinking Motives Questionnaire-Revised (MDMQ-R; Grant et al., 2007) was developed based on the Drinking Motives Questionnaire-Revised (Cooper, 1994). The MDMQ-R consists of 28 items, each contributing to one of five subscales: social, coping-anxiety, coping-depression, enhancement, or conformity (Grant et al., 2007). The current study used the coping-depression subscale, which consists of items regarding drinking in order to cope with feelings of depression (e.g., “To cheer me up when I’m in a bad mood”). Respondents report drinking motives using a five-point Likert scale ranging from 1 (almost never/never) to 5 (almost always/always) for each item. Cronbach’s alpha for the subscale has been reported at .91(Grant et al., 2007) and was .93 for the current sample.
Depression
The Patient Health Questionnaire-9 (PHQ9; Kroenke et al., 2001) is a nine-item self-report depression symptom questionnaire developed based on DSM-IV (American Psychiatric Association, 1994) criteria and consistent with DSM5 (APA, 2013) criteria. The respondent is asked to rate each item on a four-point Likert scale (0 = not at all, 3 = nearly every day). The total symptom cutoff scores are 5 for mild, 10 for moderate, 15 for moderately severe, and 20 for severe depression symptoms (Kroenke et al., 2001). Scores of 15 or greater indicate potentially diagnosable levels of depression symptoms (Kroenke et al., 2001). Good internal reliability estimates (alpha = .86–.89) have been reported (Kroenke et al., 2001). The Cronbach’s alpha for the current sample was .89.
Analysis Plan
Based on responses to the SES-SFV, participants were assigned to one of three groups: no previous sexual assault experience (NOE), SGL, and MLT. PROCESS for SPSS IBM SPSS Statistics (Hayes, 2022) was used to perform a series of moderation analyses. To generate predictors to compare the three groups, dummy codes were prepared (Hayes & Montoya, 2017). In order to perform full comparisons between the three groups, two mediation analyses were run. In the first set the no sexual assault (NOE) group was the reference group to generate two group comparison predictors: NOE(0) versus SGL(1) and NOE(0) versus MLT(1). In the second set, the SGL group was set as the reference group to generate a group comparison predictor: SGL(0) versus MLT(1). Figure 1 shows the mediation model to test, in which two dummy-coded group membership variables were the predictors, alcohol use was the criterion, and depression symptoms and coping-depression drinking motives were serially entered mediators. To obtain 95% bias-corrected confidence intervals for the moderation models, 5,000 bootstrap estimates were used.
Results
Descriptive Statistics and Group Comparisons
Among 405 survey completers, 26.9% (109 women) reported at least one rape experience. Data from 75 women who reported sexual assault experiences other than rape were excluded. Data were analyzed for 221 who reported NOEs, 43 who reported one previous adult rape experience, and 66 who reported multiple adult rape experiences.
Means, standard deviations, and correlations for the variables of interest are presented in Table 1. All correlations were significant (ps < .01). Levels of current alcohol consumption and depression symptoms are presented in Table 2. Hazardous alcohol consumption (indicated by a score of 8 or above on the AUDIT) was reported by 4.1% in the no sexual assault group, 14.0% in the SGL group, and 25.8% in the MLT group. Regarding depression symptom severity, 10.0% in the no sexual assault group, 18.6% in the SGL group, and 27.3% in the MLT group scored 15 or above on the PHQ9, indicating a likely diagnosable level of depression symptoms. Chi-squire analyses and post hoc tests with Bonferroni corrections (Beasley et al., 1995) revealed that the multiple rape group had a significantly higher proportions of diagnosable levels of depression symptoms and hazardous levels of drinking (ps < .008) than the expected proportions. The no assault experience group had significantly lower proportions of diagnosable levels of depression symptoms and hazardous levels of drinking than the expected proportions (ps < .008).
Means, Standard Deviations, and Correlations.
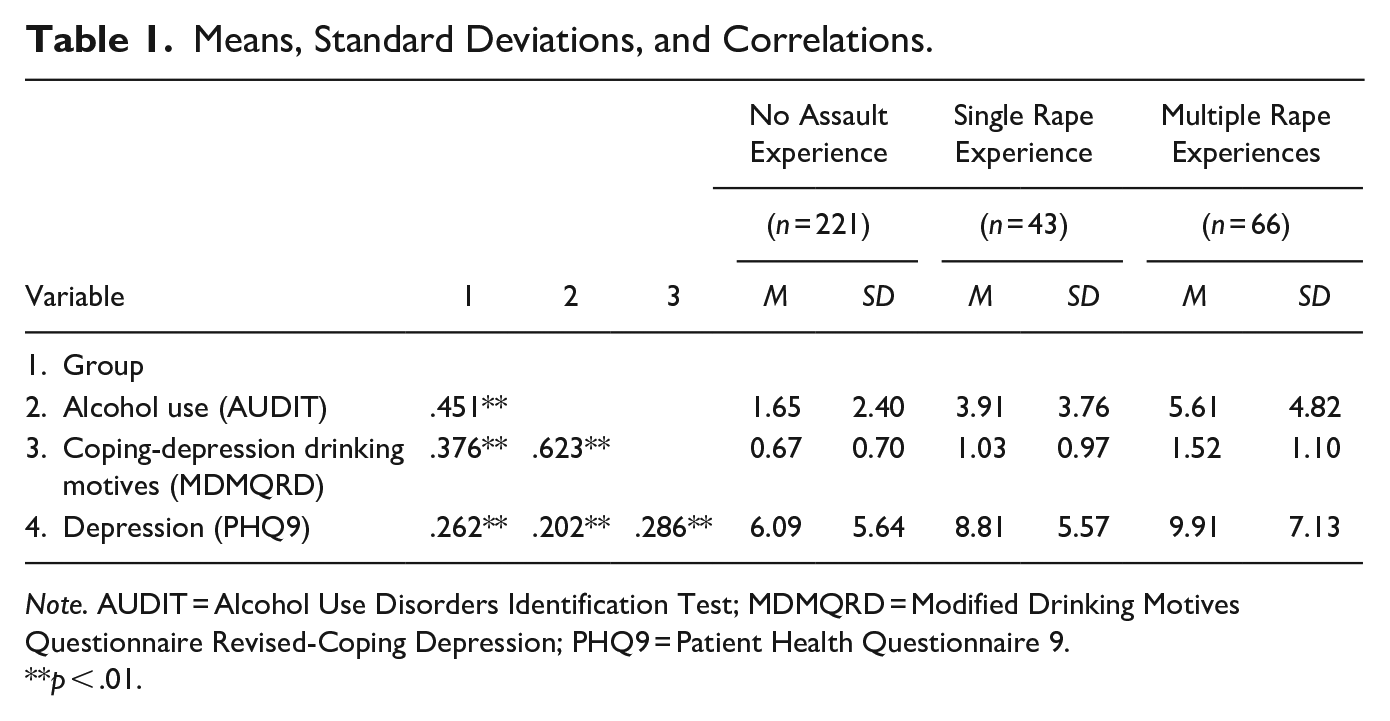
Note. AUDIT = Alcohol Use Disorders Identification Test; MDMQRD = Modified Drinking Motives Questionnaire Revised-Coping Depression; PHQ9 = Patient Health Questionnaire 9.
p < .01.
Levels of Problem Drinking and Depression Symptoms.
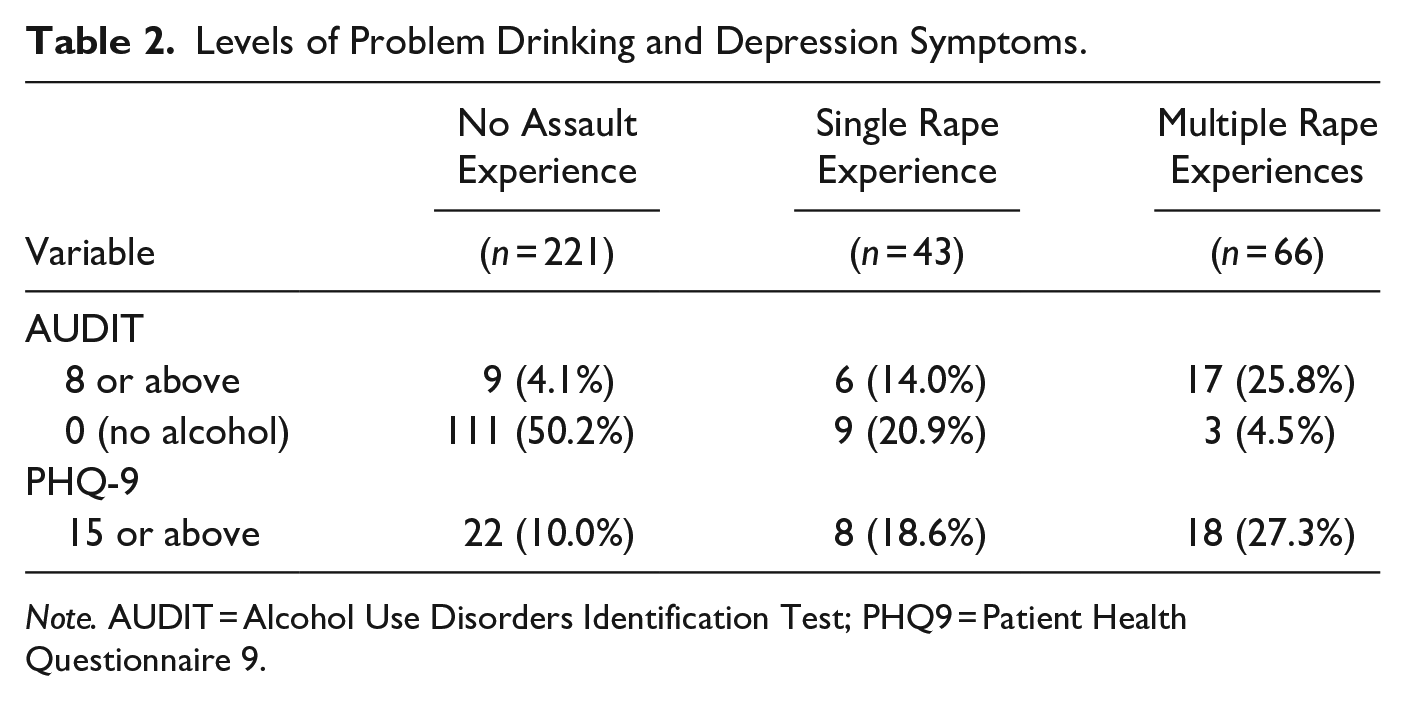
Note. AUDIT = Alcohol Use Disorders Identification Test; PHQ9 = Patient Health Questionnaire 9.
There were 14 (32.6%) in the SGL group and 26 (39.4%) in the MLT group who reported alcohol intoxication at the time of (at least one) rape experience. A factorial ANOVA showed that neither the main effect of intoxication at the time of rape nor the interaction effect of group × intoxication was significant for current levels of alcohol use (ps > .07).
Serial Mediation Model
Whether the association between group and current levels of alcohol use was serially mediated by depression symptoms and coping-depression drinking motives was examined (Figure 1). Results are presented in Table 3. Results for the SGL-NOE comparison predictor (X1 in Table 3) revealed that differences in current levels of alcohol use between the SGL and no sexual assault groups were partially serially mediated by depression symptoms and coping-depression drinking motives. The partial mediation paths suggest that compared to the no sexual assault group, the SGL group reported significantly elevated alcohol use as a result of more elevated depression symptoms followed by greater levels of coping-depression drinking motives, which led to more increased alcohol use. Similarly, the MLT-NOE comparison (X2 in Table 3) showed that differences in current levels of alcohol use between the MLT and no sexual assault groups were also partially serially mediated by depression symptoms and coping-depression drinking motives. The direct effects of the groups were also significant, revealing that relative to the no sexual assault group, the SGL and MLT groups directly predicted elevated alcohol consumption. When comparing the SGL and MLT groups (X3 in Table 3), group membership did not predict differential levels of alcohol use directly or via the serial mediation path. For all comparisons, the direct effects were still significant (p < .01).
Mediation Model Summary.
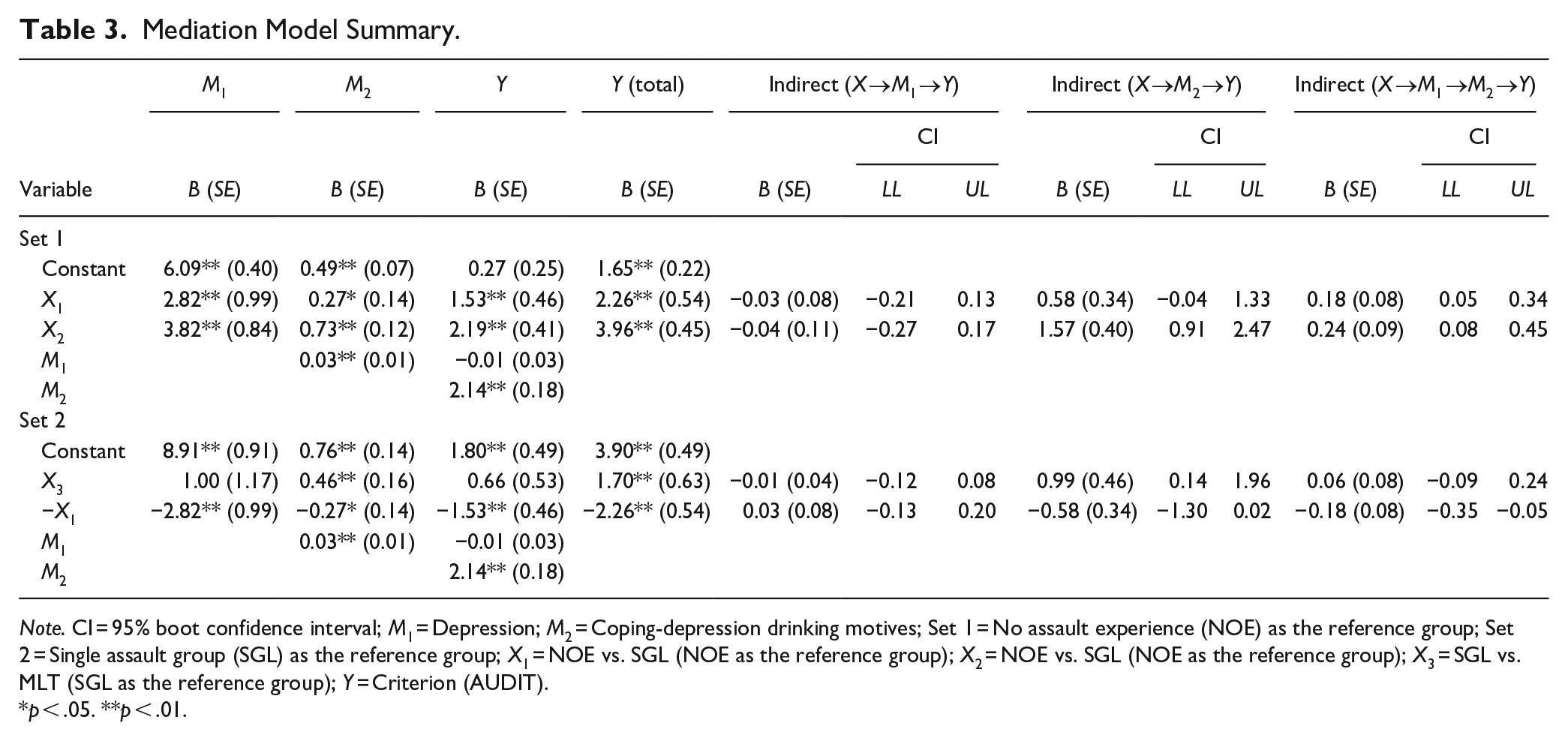
Note. CI = 95% boot confidence interval; M1 = Depression; M2 = Coping-depression drinking motives; Set 1 = No assault experience (NOE) as the reference group; Set 2 = Single assault group (SGL) as the reference group; X1 = NOE vs. SGL (NOE as the reference group); X2 = NOE vs. SGL (NOE as the reference group); X3 = SGL vs. MLT (SGL as the reference group); Y = Criterion (AUDIT).
p < .05. **p < .01.
The model also tested the two single mediation paths, one via drinking motives and the other via depression, to the alcohol consumption variable. Coping-depression drinking motives alone partially mediated the association between two group comparisons (NOE vs. MLT and SGL vs. MLT) and alcohol consumption. Depression symptoms alone did not mediate the association. When these paths were removed, and the model was re-run, the serial mediation patterns described above remained.
Discussion
The current study investigated the effects of rape experiences in Hispanic undergraduate women on two common emotional and behavioral consequences: alcohol use and depression symptoms. A serial mediation model was developed in which the association between rape experiences and alcohol use was serially mediated by depression symptoms and coping-depression drinking motives.
The current study revealed that 26.9% of Hispanic female undergraduate students reported at least one rape experience at the age of 17 years or older and 60.6% of rape survivors reported two or more rape experiences. The current rates found in this Hispanic female college sample are particularly alarming, as they are higher than estimated rates of sexual victimization and rape in college women in past studies, which ranged from 10% to 20% (e.g., Carey et al., 2015; Krebs et al., 2016; Marsil et al., 2016), suggesting Hispanic college women as a particularly vulnerable group for rape.
The hypothesized serial mediation model was largely supported. Relative to the group with no sexual assault experience, both the single and MLT groups endorsed more alcohol consumptions as a result of elevated depression symptoms and then elevated motives to drink to cope with depression. This serial pathway as an underlying mechanism along with the direct path from group membership significantly predicted increased alcohol use in the two rape-experience groups compared to the no sexual assault experience group. The single and MLT groups did not differ on the magnitudes of the pathways. Although overall indirect effects were significant, the direct effects were still significant as well, suggesting the presence of other underlying mechanisms that may also help explain group differences for levels of alcohol use.
Interestingly the mediation results showed that experiencing higher depression symptoms itself did not lead to more alcohol use. This suggests that coping-depression drinking motives are a critical factor for explaining increased alcohol use in female rape survivors with depression, compared to those without sexual assault experiences. This is consistent with motivational models of drinking (Cooper et al., 1995; Grant et al., 2007). Rape survivors likely develop a pattern of drinking in response to emotional distress stemming from their rape experiences, as the self-medication hypothesis suggests (Khantzian, 1997). Drinking motives mediated the association between group membership and alcohol consumption when comparing the MLT group and the other two groups. For survivors of multiple rapes, it might be the case that elevated drinking motivation and the problematic alcohol use that can follow may take on a life of its own.
More than one third of survivors in the rape experiences groups (14 in the single rape group and 26 in the multiple rape group) reported alcohol intoxication at the time of rape experience. This rate appears somewhat low compared to rates of sexual assault cases under alcohol influence reported previously, with an average of 50% across studies (Abbey et al., 2004). However, the current proportion may need to be interpreted with caution as it is possible that some of the current Hispanic participants may have been hesitant to report drinking when under the legal drinking age of 21.
The relatively large proportions of Hispanic women in the multiple rape group who reported diagnosable levels of depression symptoms and hazardous alcohol use are concerning. It is also notable that only 4.5% of multiple rape survivors report no alcohol consumption compared to 20.9% of the single rape survivors and 50.2% of the non-victims. These findings are consistent with past research with predominantly non-Hispanic white college women, which reports strong associations between a history of MLT and subsequent problem drinking and depression (Najdowski & Ullman, 2009; Rhew et al., 2017; Zinzow et al., 2010). Similar to these findings, MLT may have had more powerful adverse effects on Hispanic young women than SGLs. Compounding this problem, past research has found that Hispanic individuals disproportionately experience some treatment barriers, such as stigma attached to psychological disorders and limited access to transportation, leaving this cultural group underserved (e.g., Cardemil et al., 2007; Hirai et al., 2015). This highlights the critical need to prevent sexual revictimization in this vulnerable population, which could contribute to reducing risks of developing subsequent psychological disorders and leaving the mental conditions untreated.
The results of this study have several clinical implications. First, the findings emphasize the importance of assessing depression symptoms and coping-depression drinking motives in Hispanic female rape survivors to reduce risks for hazardous drinking behavior, particularly when alcohol intoxication may put them at further risk for repeated sexual victimization. When rape survivors report depression, effective coping methods should be discussed. The finding that the serial mediation model was supported similarly by the single and multiple rape groups is also noteworthy. Although levels of psychological distress and negative behavioral outcomes may differ significantly between women with one rape experience and those with MLT, how they develop problem drinking as a result of their rape victimization history may be similar, suggesting a possible adoption of the same preventive and intervention strategies for both groups. These results obtained from a sample of Hispanic young women indicate the high prevalence of rape cases in this population and highlights the need for adequate resources and support for sexual assault survivors in Hispanic serving universities and communities.
It would be valuable for future research to expand the present model, testing the role of additional psychopathology symptom variables as mediators. It is notable that the current model’s direct effects were significant in addition to the significant overall indirect effects, suggesting additional potential underlying mechanisms of differential group alcohol use. For example, posttraumatic stress symptoms (PTSS) have been found as a mediator for the association between sexual victimization in young adults, children, and youth and alcohol and other substance use in young adults (e.g., Hannan et al., 2017; Walsh et al., 2014). Although the results of these studies cannot tell us whether PTSS is a causal mechanism of differential levels of problem drinking between single and MLT in young women, they suggest the potential incremental gains of future research adding PTSS as an additional mediation path to the current model.
The current results should be interpreted in light of study limitations. First, findings from college students may have limited generalizability to community and clinical samples. However, it should be noted that sexual victimization history was determined by a well-established sexual victimization assessment instrument (Koss et al., 2007), and sizable minorities of the participants in the single (14%) and multiple (27%) rape groups reported what are likely to be clinically significant levels of depression symptoms and/or alcohol use. Thus, the identified outcomes associated with the rape experience groups could be applicable to symptomatic Hispanic women with rape victimization histories. Second, both the single rape and MLT groups had relatively small sample sizes, which might explain some non-significant effects found for the comparisons between these groups. In addition, the cross-sectional nature of the study design does not allow for definitive causal claims. Future research should examine the model longitudinally in larger community and clinical samples with both men and women with different sexual victimization histories.
The current study developed and tested a model of influences on post-rape depression, coping-depression drinking motives, and drinking behavior among Hispanic college women. Hispanic women have been underrepresented in sexual victimization research. The study revealed Hispanic college women as a vulnerable group for rape. The current results were obtained from a solid theoretical model that explains the serial mediation path and contributes to a greater understanding of the effects of rape experiences on emotional and behavioral outcomes among Hispanic college women. Results from the identified model highlight the importance of providing adequate resources and support for Hispanic rape survivors and designing prevention measures aimed at sexual victimization and revictimization for the cultural group. Such efforts are needed to prevent young Hispanic women from developing psychological and behavioral symptoms stemming from sexual assault experiences, which might then go untreated.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research and/or authorship of this article.