
Abstract
Youth with serious emotional disturbance involved in juvenile justice systems have complex needs that often are best addressed through collaborative systems that coordinate the efforts of individual agencies. This study examines the effectiveness of a system-of-care-grant-funded community in Birmingham, AL compared to a matched comparison community in Montgomery, AL in reducing youth contact with the juvenile justice system. Logistic regression results demonstrate greater reductions in the likelihood of juvenile justice involvement among youth served in systems of care over time compared to those served in a services-as-usual environment. These findings show the benefits of the incorporation of system-of-care principles for youth with a multitude of needs.
Research shows that youth with serious emotional disturbance also have significant problems in areas other than mental health such as troubles in school and involvement in the juvenile justice system (Graves, Frabutt, & Shelton, 2007; Grisso, 2008; Hansen, Litzelman, & Milspaw, 2004; Hinton, Sims, Adams, & West, 2007; Lyons, Baerger, Quigley, Erlich, & Griffen, 2001). 1 Even though youth likely encounter problems in several domains, individual agencies may provide services for youth without any sort of coordination or communication across agencies. As a result of disjointed service provisions, youth are often placed in more restrictive environments such as detention and commitment facilities unnecessarily (Gurian-Sherman, 2001; Lyons et al., 2001; MacKinnon-Lewis, Kaufman, & Frabutt, 2002). For example, youth with mental health conditions are frequently incarcerated in facilities for nonviolent acts (Gurian-Sherman, 2001). This is especially problematic because punishment rather than treatment is the primary goal of these secure facilities and mental health problems are exacerbated as a result (Gurian-Sherman, 2001; MacKinnon-Lewis et al., 2002).
To alleviate these challenges, the federal government began supporting a system-of-care (SOC) philosophy, which was first articulated by Stroul and Friedman (1986). The system-of-care approach asserts that service delivery systems need to offer a wide array of services that are accessible, community based, individualized, culturally competent, and that include the family in treatment planning and delivery. These services should be provided in the least restrictive setting possible. In addition, because of the variety of services needed by youth with serious emotional disturbance and the number of contacts with various child-serving agencies that they and their families experience, service coordination and interagency collaboration are critical. Thus, agencies in various child-serving sectors, such as mental health, education, juvenile justice, and child welfare should work together to provide the services needed (Grisso, 2008; Hansen et al., 2004). Explicit in this approach to service delivery is the assertion that if services are provided in this manner, outcomes in multiple areas (e.g., mental health, school performance, and juvenile justice involvement) will be better than those that can be achieved in traditional service delivery systems (Hansen et al., 2004; MacKinnon-Lewis et al., 2002; Manteuffel, Stephens, & Santiago, 2002). Since 1993, the Center for Mental Health Services (CMHS) has funded the Comprehensive Community Mental Health Services for Children and Their Families Program. To date, 126 communities have received funding to develop systems of care for youth with serious emotional disturbance.
This study examines the effectiveness of systems of care compared to services-as-usual in reducing the likelihood of juvenile justice involvement among youth with serious emotional disturbance. Also, this study examines whether youth in the system-of-care community commit less serious crimes than those receiving services-as-usual. It is important to examine changes in outcomes among youth with serious emotional disturbance because of the link between mental disorders and contact with the juvenile justice system (Armistead & Wierson, 1992; Cauffman, Scholle, Mulvey, & Kelleher, 2005; Rosenblatt, Rosenblatt, & Biggs, 2000; Scott, Snowden, & Libby, 2002). The present sample included 202 youth receiving services in a system-of-care-grant-funded community in the Birmingham, AL vicinity and 189 youth receiving services in a matched comparison community in the Montgomery, AL vicinity.
Overlap Between Juvenile Justice and Mental Health Populations
A large overlap exists between youth with mental health problems and youth involved in the juvenile justice system (Grisso, 2008; Lyons et al., 2001; Maschi, Hatcher, Schwalbe, & Rosato, 2008; Potter & Jenson, 2003; Shelton, 2001; Shufelt & Cocozza, 2006; Teplin, Abram, McClelland, Dulcan & Mericle, 2002). Many youth who engage in delinquency suffer from mental health problems, and many youth who receive mental health services engage in delinquency (Atkins et al., 1999; Cuellar, Libby, & Snowden, 2001; Dembo, La Voie, Schmeidler, & Washburn, 1987; Foster, Qaseem, & Connor, 2004; Lyons et al., 2001; Rosenblatt et al., 2000; Vander Stoep, Evens, & Taub, 1997). Although the exact proportion of mentally ill youth involved in the juvenile justice system is unknown, youth with mental health problems are seemingly overrepresented in the juvenile justice system (Maschi et al., 2008; Potter & Jenson, 2003), particularly among certain age and ethnic groups (Vander Stoep et al., 1997). Various studies have found a significant difference in the prevalence of mental illness when comparing the general juvenile population and the juvenile justice population. Prevalence of mental disorders in community samples of adolescents is estimated to be approximately 20% while in the juvenile justice community it is above 66% (Cauffman, 2004; Teplin et al., 2002). Furthermore, Cocozza and Skowyra (2000) estimate that at least 20% of youth involved in the juvenile justice system have serious mental health disorders. A more recent estimate suggests that more than a quarter of youth involved in the juvenile justice system experience a mental health disorder severe enough to require significant and immediate treatment (Shufelt & Cocozza, 2006). The overlap between these two populations cannot be explained solely by similarities in mental health disorders such as conduct disorder or substance abuse disorder and delinquent behavior (Shufelt & Cocozza, 2006). Because evidence suggests that there is a strong association between mental illness and involvement with the correctional system (Cauffman, 2004; Teplin et al., 2002; Wasserman, McReynolds, Lucas, Fisher, & Santos, 2002), cross-agency collaboration in the community may address the complex needs of those with emotional and behavioral problems and reduce future criminal offending (Cocozza & Skowyra, 2000; Foster et al., 2004; Grisso, 2008; Lurigio, 2000; Manteuffel et al., 2002; Maschi et al., 2008; Stephens, Holden, & Hernandez, 2004). Ensuring that there is the capacity within the juvenile justice system to respond to the treatment needs of this significant population through involving parents and other agencies in verifying the screening of mental health problems in youth as well as providing mental health services in detention centers is imperative to the rehabilitation of these youth (Cauffman, 2004; Wasserman et al., 2002).
Juvenile Justice Outcomes in Collaborative Systems
Numerous studies indicate the advantages of a system-of-care approach to service delivery for improving the outcomes of youth with mental health problems. Systems of care may take a variety of forms emphasizing one or all of the guiding principles. Lyons, Griffin, Quintenz, Jenuwine, and Shasha (2003) evaluated a collaborative initiative between the Illinois Juvenile Justice Department and the division of mental health of the Illinois Department of Human Services. In this study, youth with mental health problems involved in the juvenile justice system were referred to individualized mental health services in the community consistent with a system-of-care philosophy. Lyons et al. (2003) found that within 3 months of receiving services, emotional problems of the participants decreased significantly. Although this study did not include a comparison or a control group, the rearrest rate of all youth who had been arrested and detained in Illinois was 72% while the rearrest rate for youth who participated in the program was 42%. This study suggests that improved mental health services for youth that are consistent with an SOC philosophy leads to reduced future involvement with the juvenile justice system.
Foster et al. (2004) examined whether youth who received services in a system-of-care community were less likely to become involved with the court system and less likely to recidivate than the comparison group who received services as usual. They found that an SOC approach involving the integration and coordination of services among mental health and juvenile justice agencies reduced the likelihood of youth involvement with the court after program entry and lowered the likelihood of subsequent offending. The difference was especially pronounced for serious offending. Specifically, the likelihood of committing a serious offense was reduced by 57% in the SOC community while the likelihood remained unchanged in the comparison group receiving services as usual.
Manteuffel et al. (2002) found that juvenile justice and mental health outcomes improved over 2 years for youth involved in system-of-care communities funded in 1993 and 1994. Youth served by a system of care had fewer contacts with law enforcement and showed significant decreases in behavioral and emotional symptoms. Similarly, other studies evaluating the effectiveness of SOC communities find that youth exposed to services implementing system-of-care principles showed greater improvements in behavioral and emotional symptoms than those who received services lower in SOC principles (Foster, Stephens, Krivelyova, & Gamfi, 2007; Manteuffel, Stephens, Brashears, Krivelyova, & Fisher, 2008; Stephens et al., 2004).
The findings for the Fort Bragg Demonstration Project reveal mixed support for the systems-of-care approach. Initial studies showed that youth served in a continuum of care based on system-of-care principles were no more likely to improve in clinical outcomes than youth in the comparison group (Bickman 1996). In addition, Bickman, Noser, and Summerfelt (1999) failed to find group differences in the number of police or juvenile court contacts. These studies have been critiqued for a number of methodological reasons (Friedman, 1996; Friedman & Burns, 1996; Mordock, 1997). Recently, the data were reanalyzed to address possible important differences between the treatment and comparison groups (Foster, Wiley-Exley, & Bickman 2009). Foster et al. (2009) confirm that youth served though a system-of-care approach did not improve in clinical outcomes compared to the control group. However, youth in the Fort Bragg Demonstration Project were less likely to report delinquency than the comparison group at 18 months posttreatment.
Finally, wraparound, an approach to services consistent with system-of-care principles, provides services that are individualized, child-centered, family-focused, community-based, and culturally competent (Kamradt, 2000). Wraparound services play a key role in systems of care, with most communities implementing wraparound (Bruns, Walrath, & Sheehann, 2007). Overall, the evidence is favorable that wraparound services reduce juvenile offending as well as improve clinical outcomes (Anderson, Wright, Kooreman, Mohr, & Russell, 2003; Bruns, Burchard, & Yoe, 1995; Carney & Buttell, 2003; Kamradt, 2000; Pullmann et al., 2006), with very few exceptions (Bickman, Smith, Lambert, & Andrade, 2003).
Overall, the literature suggests that communities that implement system-of-care principles are successful at reducing youth’s involvement with the juvenile justice system. This study represents one piece of the national evaluation of the Comprehensive Community Mental Health Services for Children and Their Families Program which is mandated by congress to
. . . (1) describe the children and families served by the systems-of-care initiative, (2) assess how systems of care develop and what factors impede or enhance development, (3) measure whether children served through the program experience improvement in clinical and functional outcomes, (4) determine whether the consumers are satisfied with the services they receive, and (5) measure the costs associated with the implementation of a system of care and determine its cost effectiveness (Holden, Stephens, & Santiago, 2005, p. 390).
Specifically, in this study we assess the effectiveness of a system-of-care community in reducing contact with the juvenile justice system for youth with serious emotional disturbances compared to youth residing in a services-as-usual community.
Method
Participants
The Comprehensive Community Mental Health Services for Children and Their Families Program provides support for communities to enact system-of-care principles. Communities are evaluated on a variety of outcomes including evaluations of services and costs and functioning in the school and at home (Brannan, Baughman, Reed, & Katz-Leavy, 2002; Foster & Conner, 2005; Foster et al., 2007; Stephens et al., 2004, Holden et al., 2005). As part of the national evaluation, data are collected on matched comparison communities. Participants were drawn from youth and families enrolled in the comparison study component of the national evaluation conducted in communities funded in 1997. 2 The present sample included 202 youth served by the system-of-care-grant-funded program, the Jefferson County Community Partnership (Birmingham), which serves Jefferson County and includes the city of Birmingham, and 189 youth from the matched community located in Montgomery, Lowndes, Elmore, and Autauga counties that are served by the Montgomery Area Health Authority (Montgomery). Because we include control variables from entrance into the study and rely on official data for our dependent variable, sample attrition did not pose a problem for this study. 3
Study Sites
Because youth and their families could not be randomly assigned to service delivery systems, this study relies on a quasi-experimental design where communities were matched on selected characteristics. Communities without federal funding were selected to match with grant communities on key characteristics such as the service delivery approach, geographic, demographic, and economic characteristics, rate of child enrollment, and child referral patterns (Foster et al., 2007). In addition, using data from the 1990 Census, communities were matched on population size, child age distributions, racial and ethnic composition, per capita income, size of catchment area, the percentage of people living below the poverty level, and the percentage of adults with a high school education (Center for Mental Health Services [CMHS], 2000, 2001, 2003; Hernandez et al., 2001). Also, appraisals of the utilization of juvenile justice, mental health, and special education services were used in the selection process of comparison communities. Montgomery was selected as the comparison community because it came closest to meeting the selection criteria and because it contrasted in its service delivery approach from the SOC approach.
One limitation of the comparison community is that the Jefferson County Community Partnership focused explicitly on youth with mental health or behavioral problems who were also involved with the juvenile justice system while the Montgomery Area Health Authority had no such relationships with collaborating agencies. Because this study focuses on how the intervention at the community level affects individual reactions to service delivery approach, important differences in the youth residing in the two communities must be taken into account.
To evaluate whether a system-of-care site may prove more effective in reducing juvenile justice contact of community members, it is important to know that these sites uphold the core principles of the system-of-care philosophy more so than the comparison sites. Numerous studies have shown that system-of-care sites do in fact exemplify system-of-care principles and do so more than comparison sites (Brannan et al., 2002; Foster et al., 2007; Hernandez et al., 2001; Stephens et al., 2004) although some sites find it challenging to implement all principles (Stout & Holleran, 2011; Vinson, Brannan, Baughman, Wilce, & Gawron, 2001). Based on the assessment of system-of-care principles at the infrastructure and service delivery levels in Birmingham and Montgomery for the comparison study, the funded site consistently averaged higher than the comparison site on each system-of-care principle: being more family focused, individualized, culturally competent, collaborative, accessible, community based, and being lower on restrictiveness of service setting (Foster et al., 2007).
Measures
Dependent variable
Official juvenile justice records were compiled using administrative data provided by the Jefferson County Family Court and the Montgomery Area Probation Administration Office. The dependent variable for this study is contact with the juvenile justice system regardless of whether or not the court case was formally processed (coded 1 for contact, 0 for no contact). For example, these records included the types of charges brought against the youth, intake disposition value, court disposition value, and adjudication value. In some cases, a charge was brought to the court’s attention but no petition was filed because the case was handled informally. Other cases resulted in a petition being filed, a disposition such as probation or commitment, and an adjudication of delinquent or in the case of status offenses, youth were adjudicated as a child in need of supervision (CHIN). Contact with the juvenile justice system was defined as at least one charge including status offenses, technical violations, property, and violent offenses identified in the court record, whether this charge occurred before or after intake into system-of-care services or mental health services in the comparison site. We are focusing on the change in contact within the juvenile justice system over time. Therefore, our sample includes all youth including those with no juvenile justice contact prior to entry into the study.
The User’s Guide to Alabama Juvenile Justice Case Records, 1990-1998 (National Juvenile Court Data Archive, 2005) was used to further classify charges into Part I and Part II offenses. Part I offenses include violent and property crimes such as aggravated assault or burglary, which are generally more serious. Part II crimes include less serious offenses such as receiving stolen property, possession of a weapon, possession of drugs, trespassing, and status offenses. 4
Independent variables
We include a dummy variable for the system-of-care community (1 = SOC, 0 = Non-SOC). The evaluation period was coded 1 indicating the 18 months post intake and 0 indicating the 18 months prior to intake. Our key variable of interest is the interaction between type of community and time period. The “difference-in-differences” estimator allows us to determine whether juvenile justice contact declined over time as a result of service delivery approach.
Control variables
To account for possible differences in the two samples that may influence contact with the juvenile justice system, we include a number of control variables. Gender was coded 1 for males and 0 for females. In addition, we created a dummy variable for race (1 if Black and 0 if White or a race other than Black). 5 Youth ranged in age from 6 years to 17 years in Birmingham and 5 years to 17 years in Montgomery. Not surprisingly, youth who had contact with the juvenile justice system were older, ranging in age from 11 to 17 in Birmingham and 10 to 16 in Montgomery. Self-reported annual household income was defined as the income for the family (including foster family) the child lived with for the majority of the 6 months prior to intake. Income was dummy coded such that 1 = below US$15,000 and 0 = above US$15,000.
We also include a number of controls that represent strain for the youth as well as possible opportunities to learn that crime is acceptable (Agnew, 2006; Akers, 1998). For example, we control for physical and sexual abuse (1 = ever abused and 0 = no abuse) because these strains likely increase negative emotions, which then lead to delinquent coping (Agnew, 2006) and because delinquent behavior is modeled for the youth (Akers, 1998). In addition, we control for child’s history of substance abuse, running away, psychiatric hospitalization, and suicide attempt (1 = present, 0 = not present) because prior deviant/delinquent behavior is one of the strongest predictors of future deviant/delinquent behavior (Sampson & Laub, 1993).
Family risk factors include a history of domestic abuse in the biological family, history of mental illness in the biological family, psychiatric hospitalization of a biological parent, history of criminal conviction of a biological parent, and history of substance abuse in biological family (1 = present, 0 = not present). These family risk factors may influence delinquent behavior of the youth because they represent a source of strain and they may present opportunities for youth to learn that crime is justifiable (Agnew, 2006; Akers, 1998).
We also control for clinical functioning captured by the Child and Adolescent Functional Assessment Scale (CAFAS) due to the interrelationship between mental health problems and juvenile justice contact (Shufelt & Cocozza, 2006). In addition, previous research indicates that higher CAFAS scores are positively related to contact with the juvenile justice system (Doucette-Gates, Hodges, & Liao, 1998; Hodges & Kim, 2000; Hodges, Doucette-Gates, & Liao, 1999; Quist & Matashazi, 2000; Rosenblatt et al., 2000). The CAFAS is a widely used reliable and valid instrument that assesses the degree to which a child’s emotional, behavioral, or substance abuse disorder is disruptive to his or her functioning in each of eight psychosocial domains (Hodges, 1994; Hodges & Wong, 1996). Caregivers reported on the child’s functioning during the past 6 months in the 8 CAFAS domains: in school/work, at home, in the community, behavior toward self and others, moods/emotions, self-harmful behavior, substance use, and thinking. A score was assigned to each domain indicating levels of impairment: 0 = minimal to no impairment, 10 = mild impairment, 20 = moderate impairment, and 30 = severe impairment. A total CAFAS score is calculated by summing the subscale scores with higher numbers indicating greater functional impairment. Scores in Birmingham ranged from 0 to 210 and ranged from 0 to 220 in Montgomery.
The Behavioral and Emotional Rating Scale (BERS) identifies the emotional and behavioral strengths of youth (Epstein & Sharma, 1998). Unlike the CAFAS, which focuses on emotional and behavioral disorders, BERS focuses on the strengths of youth in the areas of interpersonal, family involvement, intrapersonal, school functioning, and affective strengths (Epstein, Ryser, & Pearson, 2002). The BERS has been found to be a reliable and valid measure (Epstein, 1999; Epstein et al., 2002; Epstein, Harniss, Pearson, & Ryser, 1999). Caregivers or staff members who were knowledgeable about the child responded to 52 statements on how well each item described the child’s behavior over the past 6 months (0 = Not at all like the child; 1 = Not much like the child; 2 = Like the child, 3 = Very much like the child). Scores were then standardized based on scale norms.
Most of these items overlap with social control explanations of crime (Hirschi, 1969). For example, items in the interpersonal strengths subscale assess the child’s beliefs about his or her behavior (e.g., expresses remorse for behavior that hurts or upsets others; respects the rights of others; apologizes to others when wrong). The 10 family involvement items focus on attachment, commitment, and involvement with the family (e.g., demonstrates a sense of belonging to family; interacts positively with family; participates in family activities; complies with rules at home). The third subscale, intrapersonal strengths, focuses on the child’s outlook (e.g., is self-confident; is enthusiastic about life). The school functioning subscale consists of 9 items which assesses the child’s competence in school and in the classroom (e.g., completes school tasks on time; reads at or above grade level). Finally, the affective strengths subscale focuses on the ability of the child to share affection with others and likewise receive affection from others (Epstein et al., 2002). When the subscales are combined they form an overall strengths index. Because of the high correlations among these subscales and the overall score, we included the overall BERS strengths index as a variable in the analysis to control for potential between group differences in social control. The strength index ranged from 48 to 131 in the system-of-care community and from 45 to 128 in the comparison community.
Analytical Approach
First, we describe the intake characteristics of the two samples paying particular attention to significant differences between youth residing in the communities that may affect contact with the juvenile justice system. Next, we present a comparison of offense seriousness by community followed by a comparison of the types of offense charges. We then examine whether youth in the system-of-care community were less likely to come into contact with the juvenile justice system during the 18 months after intake than youth in the services-as-usual environment with an equality of proportions test. Finally, we present two logistic regression models. The base model excludes the interaction between system-of-care community and time period. The full model examines the change in the likelihood of contact with the juvenile justice system in the two communities using the difference-in-differences method controlling for gender, race, age, family income, individual and family risk factors, and clinical characteristics. Robust standard errors are used to take into account heteroskedasticity at the individual level as each youth had 2 observations, one prior to intake and one post intake.
The difference-in-differences statistical technique is widely used in economics when comparing an untreated control group with a treatment group pre- and posttreatment and is ideal for a quasi-experimental design because “this strategy ensures that any variables that remain constant over time (but are unobserved) that are correlated with the selection decision and the outcome variable will not bias the estimated effect” (Buckley & Shang, 2003, p. 2). A simple regression analysis that only examines posttreatment outcomes confounds treatment effects with pretreatment group differences. The difference-in-differences estimator provides an unbiased estimate because it subtracts out both pretreatment group differences and trends over time that could be confounded with the treatment effect.
In our study, the difference-in-differences method is used to examine the change in juvenile justice contact over the 36-month period comparing the likelihood of contact 18 months prior to intake (t = 0) to 18 months after the service intake date (t = 1) for the youth in the two communities. In our model, we define i = 1 for youth who resided in the system-of-care community and i = 0 for youth in the non-SOC group. The treatment effect refers to the difference in juvenile justice contact between the SOC group and the non-SOC group 18 months after program entry adjusting for the difference between the groups 18 months prior to program entry, hence the term “difference-in-differences.” The difference in means between the SOC community and the comparison community 18 months post intake is the unadjusted estimate of the treatment effect (µ11 – µ01) with µ it representing the mean of the outcome in group i at time t. Adjusting for the baseline differences, the adjusted estimate of the treatment effect is (µ11 – µ10) – (µ01 – µ00); (Liu, Yan, & Wang, 2010). The difference-in-differences estimator is captured in the interaction term between type of community and time period.
There are several key assumptions that must be met for the difference-in-differences estimator to be unbiased. First, to assume that the treatment, or receiving system-of-care services, is more effective at reducing juvenile justice contact than services-as-usual received in the comparison community, the two groups must be similar before entering the treatment and/or important differences must be taken into account in the model (Boyle & Lahey, 2010). Our study includes comprehensive control variables that account for most major causes of delinquency. Second, no crossover should occur where the comparison community is also receiving the same delivery approach. This assumption is met given that communities were selected based on contrasting delivery approaches. Third, the difference-in-differences method assumes that both the treatment and control group are affected in the same way by unobserved changes over time such as state laws or macroeconomic conditions (Meyer, 1995). For example, if Montgomery suffered a recession while Birmingham did not and this affects juvenile justice contact, then this assumption would be violated. The assumption is likely met in this study given that these communities are drawn from the same state and given their geographic proximity. In addition, communities were matched on characteristics that influence crime rates such as population density, racial composition of an area, poverty level, age distribution, and education level (Land, McCall, & Cohen, 1990).
Results
Descriptive Analysis
Table 1 summarizes selected intake characteristics of youth in the sample for each community. Descriptive data collected on youth and families from primary caregivers included information on gender, race, age, annual household income, and other risk factors. Significance tests and effect sizes measured by Cohen’s d are shown between the two communities for the total sample (Cohen, 1992). Summary statistics are also presented for the samples broken down by youth who had juvenile justice contact 18 months prior to program entry and those who had no prior contact.
Intake Sample Description.

Note: JJ = juvenile justice; CAFAS = Child and Adolescent Functional Assessment Scale; BERS = Behavioral and Emotional Rating Scale. Some N’s are slightly lower than reported due to missing values. Significance tests are for comparisons by community for all youth.
p < .05.
Overall, youth in the system-of-care community present more risk factors for juvenile justice involvement than youth in the comparison community. This is also evident by the high percentage of youth in the system-of-care community who had more preprogram contact with the juvenile justice system (66.8% compared to 9.5% in the comparison community). Approximately 62% of the youth served in the system of care (Birmingham) were male while 56% of youth served in the comparison community (Montgomery) were male. The majority of youth in both communities were African American (Approximately 61% in Birmingham and 66% in Montgomery). Youth in Birmingham were significantly older averaging 13.8 years of age compared to 11.5 years of age in Montgomery based on a difference of means t test (t = −8.094, p < .01). The effect size was large for age differences (Cohen’s d = −0.82).
In addition, youth in Birmingham were significantly more likely to have experienced physical abuse in the past, have a history of drug problems, have a history of running away, have a history of psychiatric hospitalization, have attempted suicide in the past, have a family history of substance abuse, and have high levels of functional impairment as measured by CAFAS than youth in the comparison community. The effect size was moderate for differences in drug abuse, having a history of running away, and functional impairment. The effect size was small for history of physical abuse, psychiatric hospitalization, attempted suicide, and history of family substance abuse. In contrast, youth in Montgomery were more likely to live in households with a family income below US$15,000 per year than youth in the system-of-care community and the effect size is moderately strong. With the exception of physical abuse and history of family substance abuse, statistical power was well above 0.80 for all significant comparisons indicating that a true difference exists between the groups (Cohen, 1992). In sum, youth in the system-of-care community present more risk factors for involvement in delinquency than those in the comparison community. These differences are considered in the multivariate analysis of the outcome data. 6
An analysis of type of crime and crime category 18 months postintake reveals that youth in the system-of-care community were less likely to engage in serious crimes compared to those in services-as-usual. In both communities, the majority of offenses brought to the court’s attention fell into the less serious Part II category of offenses. The youth in the Birmingham system-of-care community were less likely to be charged with more serious Part I crimes than youth in the Montgomery comparison community postintake. In the system-of-care community, 31.0% of the charges brought to the court’s attention were Part I crimes, while in the comparison community the corresponding number was 39.4% (p < .10). 7
Examining the most frequent allegations brought against the youth in the two communities during the 18 months following entry into services also show some evidence that youth in the system-of-care community were less likely to engage in serious offenses than youth in the non-SOC community. 8 In the Birmingham system of care, youth were most likely to be charged with technical violations such as revocation of probation (29.7%), followed by status offenses (18.8%) such as truancy, running away, and uncontrollable/ungovernable behavior, and theft (12.4%). In Montgomery, offenses against public order were most likely to be documented with the courts (25.0%), followed by theft (22.2%), and damage to property (19.4%). In sum, it appears that when youth in the Birmingham SOC did have contact with the juvenile justice system it was of a more trivial nature than youth in the comparison community.
Finally, bivariate analysis of the change in juvenile justice contact over time indicates the possible efficacy of the incorporation of system-of-care principles into the service delivery system. Among the 202 youth served by the Birmingham system of care, 135 youth (66.8%) had juvenile justice records prior to enrolling into the system of care. In Montgomery, 18 out of 189 (or 9.5%) of the youth participating in the evaluation had contact with the juvenile justice system prior to intake. The proportion of youth charged with various crimes decreased significantly to 46.5% (z = 4.1, p < .001) during the first 18 months of services in the system of care. Conversely, the rates of juvenile justice involvement during the first 18 months after program entry among youth in Montgomery, Alabama, increased to 13.7%. 9
Multivariate Analysis
Table 2 presents the logistic regression results predicting contact with the juvenile justice system. Model 1 includes all variables except the interaction and Model 2 includes the interaction between type of community and time period as well as the control variables. Model 2 captures the difference-in-differences estimator which takes into account baseline differences in juvenile justice contact. Based on a comparison of the log likelihood ratio from the full model and the restricted model, the interaction term significantly improves the model. In addition, the coefficient associated with the interaction of the system-of-care indicator and time trend (SOC × Postintake) is significant in Model 2. The analysis reveals that the reduction in contact with the juvenile justice system among youth served in the Birmingham system-of-care community relative to the Montgomery comparison community is significant when demographic and clinical characteristics are taken into account. In addition, African American youth were 1.9 times more likely to have contact with the juvenile justice system than non-African American youth. In addition, for each unit increase in age, the odds of juvenile justice contact increases by 1.3 times. Finally, youth whose parents have been convicted of a crime were 2.3 times more likely to have contact with the juvenile justice system than those who did not have a parent who had been convicted of a crime.
Logistic Regression Estimates Predicting the Likelihood of Contact With the Juvenile Justice System (N = 732).
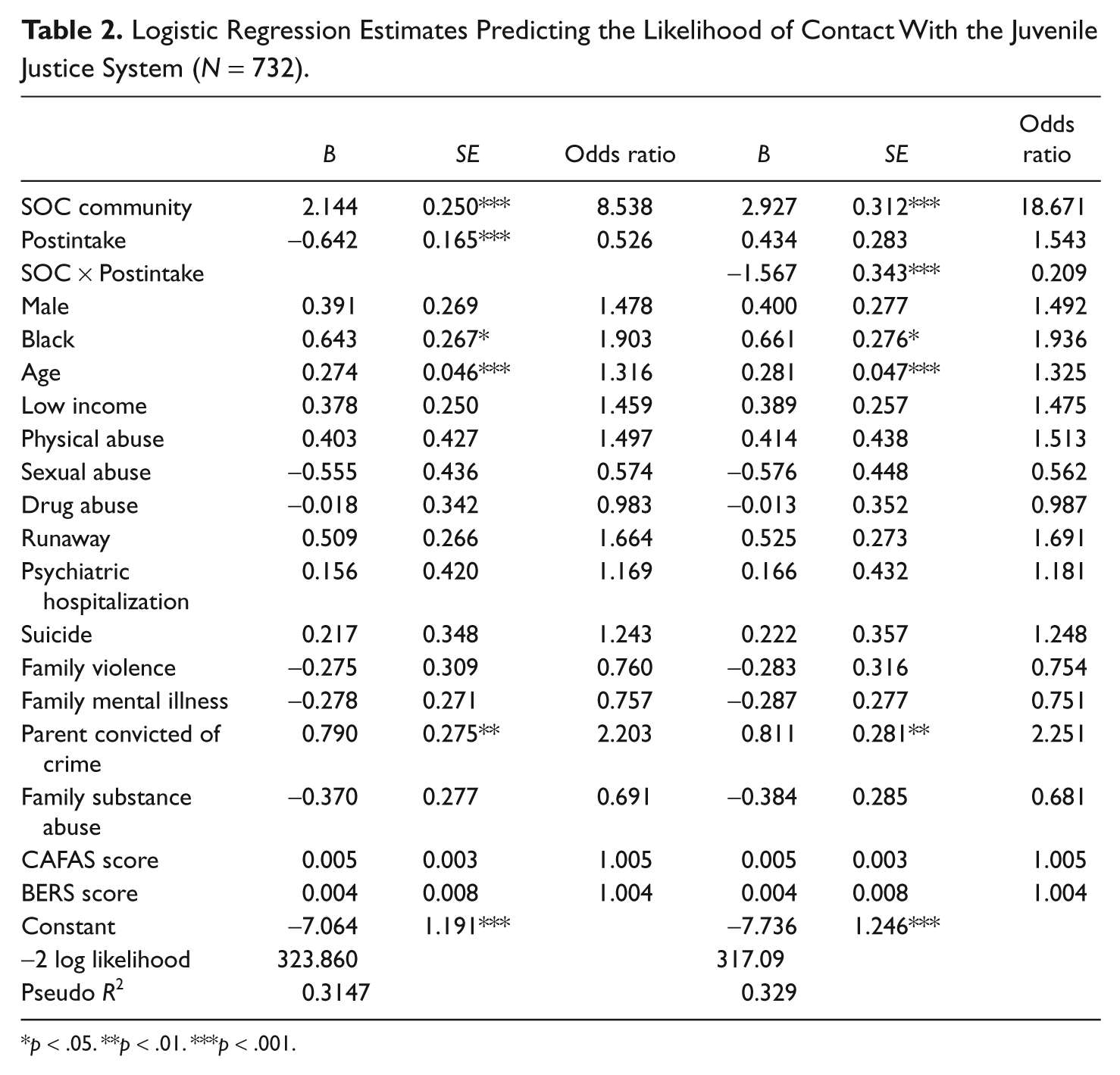
p < .05. **p < .01. ***p < .001.
To more easily interpret the interaction term, we calculated the predicted probability of contact with the juvenile justice system for youth in each community at the two evaluation periods holding all other variables at their means (see Table 3). The predicted probability of contact with juvenile justice for youth in the system-of-care community significantly decreased from 0.64 to 0.36 from preintake to postintake. The predicted probability for youth in the comparison community increased slightly from 0.09 to 0.13 although the increase was not significant. In sum, youth in the system-of-care community were less likely to have contact with the juvenile justice system over time compared to youth in the non-SOC community.
Predicted Probabilities of Contact With the Juvenile Justice System.

Note: SOC = system of care. All control variables held at means.
Discussion
The findings from the longitudinal comparison study demonstrate reduced involvement in the juvenile justice system for youth in Alabama served in the system-of-care setting, as compared to those served in a services-as-usual environment. In particular, the predicted probability of juvenile justice contact decreased from 0.64 to 0.36 in Birmingham, while it increased slightly in the comparison community. The findings confirm previous research showing that youth served by systems of care experience reductions in their involvement with the juvenile justice system (Anderson et al., 2003; Carney and Buttell, 2003; Foster et al., 2004; Kamradt, 2000; Lyons et al., 2003; Manteuffel et al., 2002; Pullmann et al., 2006).
Another difference in the sites that is worthy of note is that the “offending” that did take place in Birmingham was of a much different nature than that in Montgomery, reflecting status offending and probation violations as the primary reasons for referral, with theft being third. This is in contrast to the youth from Montgomery, whose referrals during the 18-month follow up period were dominated by public order offenses, theft, and property damage. Not only was there a significant difference in the levels of offending in Birmingham, but the type of referral was also of a much less serious nature. It is unclear why youth in Birmingham had less serious offense referrals than those in Montgomery. It may be that the SOC approach is especially effective for reducing the seriousness of offending for youth (see Foster et al., 2007). In contrast, it may be that the system-of-care approach is more successfully implemented for youth who present less destructive behaviors (Stout & Holleran, 2011). Future research should examine how offense seriousness changes over time depending on service delivery approach.
The success of the system-of-care community may likely be attributed to its focus on serving the multitude of needs of youth in areas such as at home, in school, and in various government agencies. In addition, many of the system-of-care principles such as being community based, individualized, culturally competent, and including the family in treatment decisions may reduce factors known to influence crime. Programs that are more successful at reducing delinquency focus on multiple causes of crime such as the strain youth experience, the negative influence of delinquent peers, and levels of self-control and social control (Agnew, 2005). System-of-care communities are well situated to affect these various causes of crime. For example, self-control is developed at a young age in the family context (Gottfredson & Hirschi, 1990). Families are encouraged to participate in the process of improving youths’ emotional and behavioral outcomes (CMHS, 2000). This early involvement will likely increase the youth’s level of self-control and attachment to parents. Finally, the system-of-care philosophy encourages placing youth in the community rather than in detention and commitment facilities, which reduces the opportunity for these youth to associate with delinquent peers in secure facilities.
Another factor that likely affected the success of the system-of-care community in reducing youth contact with the juvenile justice system is the unique organizational structure of the mental health service environment in Birmingham. In the Birmingham SOC, the Jefferson County Community Partnership expanded on State funding for the Family Integrity Network Demonstration (FIND), a project designed to work collaboratively with other public child-serving agencies. FIND teams were outstationed at the family court (juvenile justice) and the Department of Human Resources (child welfare). For systems of care targeting particular agency-based populations, a key element of success may be the organizational placement of mental health workers within those targeted agency environments. The impact of this approach should come as no surprise, as the kind of multisystem response inherent in the systems-of-care approach is geared to provide the mental health related supports needed by the youth involved in this study. In this regard, the FIND teams were prepared to interact effectively with the juvenile justice, child welfare, education, and behavioral health systems. Future research should examine the differences in service experiences of the youth served in the two communities as well as the relationship between mental health and juvenile justice outcomes. This research should also provide an analysis of any impact that differences in age at the time of referral may have in terms of system responses and outcomes.
It is important to acknowledge possible limitations of the research design and data used in this study. One important limitation of our study is that communities were matched rather than individuals, which led to differences between youth who reside in the system-of-care community compared to the matched community. While we attempted to control for factors known to cause crime, it is possible that unknown third variables may explain our findings such as the functionality of the courts in the two communities. However, the differences between youth in the two communities likely bias the results toward more favorable outcomes in the comparison community given that youth in Birmingham exhibited more numerous risk factors for delinquency. This lends support to the efficacy of the system-of-care approach in reducing involvement in the juvenile justice system.
Another limitation of this study is that we cannot determine which services within the system-of-care approach in Birmingham are more effective in reducing juvenile justice contact. As part of the National Evaluation, data were collected on services youth received in the two communities although it is not possible to determine whether particular services provided in the SOC setting were more effective than other services or if services of the same type such as family therapy are comparable in the two communities (see Foster et al., 2007 for a discussion of the services in the two communities). It may be that youth in the SOC community had better outcomes because services were received for more days than in the non-SOC community (Foster et al., 2007). Therefore, it is difficult to determine which particular treatments benefit youth (Holden et al. 2005). Future research should determine which specific programs within the systems-of-care framework are more effective and how the amount of time in which services are received affect outcomes.
Another shortcoming of our data is that we rely on official court records to determine delinquency. Crime is largely underreported as demonstrated in self-report surveys (Elliot & Ageton, 1980). Therefore, we are only able to determine differences in youth who are caught and processed through the court system rather than differences in actual offending. Youth in the system-of-care community may have been monitored more closely, which would increase their contact with the court system. There is some evidence of this given that youth in the system-of-care community were more likely to have contact with the court system due to technical violations and status offenses. If youth were monitored more closely in the system-of-care community, then the reduction of their contact compared to Montgomery youth postintake would demonstrate greater effectiveness of the system-of-care approach. Future research should assess how closely youth are monitored in system-of-care communities to determine how this affects their involvement with the juvenile justice system. In addition, further research should determine whether this enhanced level of surveillance, when coupled with a more rehabilitative response, inclusive of additional supports and services, contributes to better outcomes and thus lowers court referrals among SOC youth.
In conclusion, despite potential limitations of the data, this study shows the continued positive impact a system-of-care community can have on youth with serious emotional disturbance. Youth served in the system-of-care community were significantly less likely to have contact with the juvenile justice system than youth in the comparison community, indicating the merits of collaborative systems of care.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
Funding
The author(s) received the following financial support for the research and/or authorship of this article: This work was supported by the Center for Mental Health Services of the Substance Abuse and Mental Health Services Administration in United States Department of Health and Human Services [Contract numbers: 280-97-8014, 280-03-1604, and 280-07-0702].
Disclaimer
The views expressed in this article are those of the authors and do not necessarily reflect the official policies of the U.S. Department of Health and Human Services, nor does the mention of trade names, commercial practices, or organizations imply endorsement by the U.S. Government.