
Abstract
This study examines the influence of offender, victim, and case characteristics along with available forensic evidence on legal outcomes of nonfatal strangulation (NFS) cases. Research points to the importance of NFS forensic evidence collection to corroborate the attack during legal proceedings. However, little is known regarding the factors associated with legal decisions for NFS cases with forensic evidence. Law enforcement reports, forensic medical examinations, and legal outcomes for 63 NFS cases in Florida were analyzed. Findings have implications for the criminal justice system, as forensic medical exams can be used to collect valuable evidence to support prosecution outcomes.
Introduction
Violence committed against those in domestic and intimate relationships is a common issue that can bring about a host of health consequences (Bhole et al., 2014). Domestic violence (DV) includes any combination of physical, psychological, sexual, and coercive behaviors (Huecker et al., 2023). DV may be completed, attempted, or threatened and may be perpetrated by a current or former partner, those who share children, or those currently or formerly cohabitating (Federal Bureau of Investigation [FBI], 2017). Within this context, nonfatal strangulation (NFS) is a major area of concern due to the potential for increased long-term injury and future lethality (De Boos, 2019; Glass et al., 2008; Jacob et al., 2020; Mcquown et al., 2016).
NFS is the purposeful restriction of air or blood to a person’s head by means of outer physical compression of the neck or upper chest area, completed manually or with the aid of a ligature or other object (Bendlin & Sheridan, 2019; Pritchard et al., 2017; Sauvageau & Boghossian, 2010). Strangulation, as a modality of violence, is frequently reported by intimate partner violence (IPV) victims and commonly experienced multiple times by an abusive partner (Messing et al., 2018; Wilbur et al., 2001). As high as 68% of women who have experienced IPV report experiences with NFS (Messing et al., 2018; Wilbur et al., 2001). In addition, Messing et al. (2018) found an additional 12% of women in their sample experienced attempted strangulation.
Signs and symptoms of NFS victimization may include dizziness, abrasions, neck pain, petechiae, sore throat, skin markings, scratches, loss of consciousness, headaches, and difficulty breathing (De Boos, 2019; Hawley et al., 2001; Smith et al., 2001; Wilbur et al., 2001). In addition, psychological consequences of NFS victimization may include posttraumatic stress disorder (PTSD), nightmares, anxiety, sleep issues, substance use issues, suicidal ideation, and depression (De Boos, 2019; Smith et al., 2001; Wilbur et al., 2001). Strokes, brain injury, and delayed death are also possible (Clarot et al., 2005; Funk & Schuppel, 2003; Monahan et al., 2020). Smith et al. (2001) found that symptoms and injuries of NFS increased with the number of NFS attacks experienced. Furthermore, NFS is a significant risk factor for intimate partner homicide (Glass et al., 2008). Glass et al. (2008) found that when a victim experienced NFS by an intimate partner, the chance of being killed in the future by their partner was more than 7 times higher than if they had never experienced NFS.
Legal outcomes of DV incidents are complicated by a multitude of factors (Bechtel et al., 2012; Epstein & Goodman, 2019; Lippman, 2013; Maalouf, 2017), with the presence of NFS furthering hindering prosecution efforts (Reckdenwald et al., 2020; Strack et al., 2001). This is additionally problematic as NFS is a more common tactic used by perpetrators than originally thought to display power and control over their victims (Pritchard et al., 2017; Taliaferro et al., 2001; Thomas et al., 2014). Prosecution of NFS is complicated, in part, by the often invisible, delayed, or apparently minor presentation of physical injuries (De Boos, 2019; Hawley et al., 2001; Smith et al., 2001). Even in death, strangulation injuries may only present in the following days (Hawley et al., 2001). In addition, many NFS victims do not seek immediate medical attention, may avoid accessing health care altogether, and may not even recognize a health issue has been experienced (Mcquown et al., 2016; Patch et al., 2018; Smith et al., 2001).
Victim cooperation, a significant predictor of conviction, often complicates successful prosecution outcomes for DV cases as victims are often reluctant to cooperate for a variety of reasons (Bechtel et al., 2012). In addition, when a DV victim does cooperate, their testimony may be called into question due, in part, to the effects of trauma on statement consistency (Epstein & Goodman, 2019). For instance, brain injury resulting from IPV may be a major impediment (St Ivany et al., 2021). Research showing NFS has the potential to cause detrimental changes to the brain (Daugherty et al., 2022) only adds to the difficulties of successfully prosecuting DV cases involving NFS. Adding to this challenge, scholars argue that DV victims often experience gender bias in the judicial system by having their credibility discounted and their abuse experiences dismissed (Epstein & Goodman, 2019). Prosecutorial success of DV cases, and NFS cases specifically, would be drastically improved with an increase in the quality of evidence, irrespective of victim cooperation (Reckdenwald et al., 2020; Westera & Powell, 2017).
The prosecution of NFS cases varies on the state level due to strangulation statutory differences (Laughon et al., 2009), but there are felony strangulation statutes in many states reflecting the seriousness of NFS victimization (Jordan et al., 2020; Pritchard et al., 2017). However, the lack of training involving the identification, forensic documentation, and medical treatment of NFS victims among criminal justice system personnel further complicates effective prosecution (Douglas & Fitzgerald, 2014; Reckdenwald et al., 2020). For instance, Strack et al. (2001) noted the limited detail provided in police reports when strangulation was the modality of violence, and other existing literature demonstrates that officers responding to DV cases commonly neglect to properly identify or document cases of NFS (Garza et al., 2021; Reckdenwald et al., 2020, 2022; Strack et al., 2001). Law enforcement and prosecutors generally focus on signs of visible injury; yet half of NFS cases present with no visible injuries resulting in severe and potentially lethal signs and symptoms of NFS over-looked (Strack et al., 2001).
Training to improve the identification and documentation of NFS, as well as forensic evidence collection, are key to the successful prosecution of NFS cases (Brady et al., 2023; Jordan et al., 2020; Reckdenwald et al., 2021, 2022; Zilkens et al., 2016). Without training in place, Reckdenwald et al. (2020) found that no charges were filed in over half of NFS cases, and of those charged, only 4.4% resulted in a felony strangulation conviction. To improve the response to NFS, scholars have argued for universal definitions and identification techniques (Baker & Sommers, 2008; Douglas & Fitzgerald, 2022), along with consistency and communication between officers, medical personnel, and prosecutors (Jordan et al., 2020; Reckdenwald et al., 2019). Research also notes the critical role of health care providers and the need for improved practices (Bhole et al., 2014; Jacob et al., 2020), including the crucial role imaging can have on the determination of abuse (Bhole et al., 2014). Studies have identified magnetic resonance imaging (MRI) scans (Yen et al., 2005, 2007) and computed tomography angiography (CTA) scans (Jordan et al., 2020) as useful for identification of significant injury resulting from NFS. Holbrook and Jackson (2013) stated alternative light sources may help in the identification of hard to see NFS injuries. Overall, quality evidence collection can help corroborate NFS in legal proceedings regardless of victim cooperation, which in turn will enhance the response to these cases (Reckdenwald et al., 2022).
In 2007, NFS became a felony offense in the state of Florida (domestic battery by strangulation, 2007). Under this law, it is a third-degree felony to
knowingly and intentionally, against the will of another, impedes the normal breathing or circulation of the blood of a family or household member or of a person with whom her or she is in a dating relationship, so as to create a risk of or cause great bodily harm by applying pressure on the throat or neck of the other person or by blocking the nose or mouth of the other person. (domestic battery by strangulation, 2007)
Yet, enforcement of the law has been incredibly challenging (Reckdenwald et al., 2020). Forensic evidence as a means of corroborating the NFS attack has shown to be an important piece in holding NFS offenders accountable (Reckdenwald et al., 2021).
This study expands previous research by examining 63 NFS cases that were identified by law enforcement at the scene of an incident and were referred to a forensic medical examination for evidence collection to determine what factors are associated with legal system decisions. Data for this were collected through a partnership between criminal justice and health organizations in Florida and researchers to improve the response to NFS in a Florida county by facilitating evidence-based prosecution (see Pritchard et al., 2018; Reckdenwald et al., 2019, 2021). To achieve this goal, law enforcement officers were trained to identify and document NFS in police reports and refer NFS victims to no-cost forensic medical examinations. During the forensic medical examination, specially training forensic nurse examiners (FNEs) assessed the seriousness of the incident and comprehensively identified and documented signs and symptoms of NFS to (a) mitigate severe and potentially life-threatening consequences and (b) provide valuable evidence in prosecutors’ efforts to hold offenders accountable.
With many NFS cases lacking visible injury (Strack et al., 2001), improved documentation of NFS symptoms and injuries in law enforcement reports along with evidence collected during a forensic medical examination can be incredibly useful during legal proceedings. While recent research has shown the advantages of training law enforcement to screen for NFS and document symptoms and injuries (Reckdenwald et al., 2019) and the importance of having forensic documentation of NFS available to use as evidence for prosecution purposes (Reckdenwald et al., 2021), little is known regarding factors associated with legal decisions. As such, this seeks to determine what characteristics (offender, victim, and case) and available evidence are associated with the prosecution (i.e., filing as a formal criminal charge with the court) of a NFS case with forensic evidence. Findings from this study can point to the type of evidence that is deemed most important for case viability and may highlight inadequacies in the response to NFS. In addition, findings may have implications for NFS policy at the intersection of health care and the administration of justice.
Method
NFS Training and Evidence Documentation
As part of the multi-agency effort, a county-wide training was conducted by the National Family Justice Center Alliance’s Training Institute on Strangulation Prevention. Higher ranked law enforcement supervisors, Special Victim Unit agents, prosecutors, health department personnel, victim advocates, and researchers involved in the project participated in the training. The NFS training encompassed the lethality of strangulation, signs and symptoms of NFS, anatomy and medical aspects of NFS, investigative and legal aspects of NFS, and using experts in courts to aid NFS cases (for more details see Reckdenwald et al., 2019, 2021). Training and protocols were developed to document evidence in law enforcement reports and during a forensic medical examination. Once the county-wide training was complete, law enforcement officers were trained by supervisors and Special Victim Unit agents to identify NFS, document signs and symptoms on a strangulation investigative form, and refer NFS victims to forensic medical examinations. Sexual Assault Nurse Examiners (SANE; here on referred to as forensic nurse examiners [FNEs]) were trained by health department staff to identify and assess the severity of the NFS assault, question victims about the assault, document injuries, conduct a forensic examination and collect forensic evidence, and testify as an effective expert witness during a criminal trial. On November 1, 2015, forensic medical examinations became available to victims of NFS at the local domestic violence center who were referred by law enforcement in the county. 1 Once consent was given for a forensic medical examination, law enforcement would either provide the NFS victim transportation, or the NFS victim would drive themselves (if able) or arrange for transportation. 2 During the examination, FNEs documented all evidence of NFS on a newly developed strangulation documentation form.
Data
Data for this study were collected as part of a multi-agency effort between researchers, law enforcement, and medical and legal personnel to develop a county-wide response to incidents of NFS in the context of domestic violence in one Florida county (see Pritchard et al., 2018; Reckdenwald et al., 2019, 2021). 3 The goal of this effort was to facilitate evidence-based prosecution by training law enforcement officers how to identify and document NFS signs and symptoms and providing NFS victims with no-cost forensic medical examinations completed by specially trained FNEs. This study examines offender, victim, and case characteristics, forensic medical evidence, and legal outcomes for a sample of NFS cases during a 3-year period (November 1, 2015, and October 31, 2018). Data utilized were collected from three sources: (a) domestic violence law enforcement reports, (b) forensic medical examinations, and (c) domestic violence public court records. During this 3-year period a total of 64 NFS victims were referred (by law enforcement) and consented to a forensic medical examination by a trained FNE. However, for purposes of this study, information from 63 cases was examined as one perpetrator’s criminal information was expunged which resulted in any law enforcement and forensic medical evidence being unavailable.
To collect information from law enforcement incident reports, an agency-wide electronic record system, the Law Enforcement Record Management System (LERMS), was utilized. Information about the offense, offender, and victim were coded. For purposes of this study victim and offender sex (i.e., male or female), age, and race (i.e., Black, White, Asian, Hawaiian or Pacific Islander, Hispanic or Latinx, another) were examined as well as case characteristics including whether the victim and offender were current or former intimate partners (i.e., yes or no) and whether there was a history of domestic violence in the relationship noted in the report (i.e., yes or no). Although documentation of NFS from law enforcement was also coded (e.g., modality of the NFS and evidence of symptoms related to the strangulation such as neck injuries, “shoulder,” “chest,” or “back” injuries, petechiae-like injuries (e.g., “red eye” or “red spots” in ears, face, mouth), voice abnormalities, breathing difficulties, trouble swallowing, psychological symptoms (e.g., memory problems, slurred speech), whether the victim sought medical attention for injuries, and if photographs were taken to document injuries), more detailed information from the forensic medical exams were used for analysis purposes.
To collect information about forensic medical evidence, forensic medical examination data were coded from a forensic examination strangulation documentation form. This form was created as part of the coordinated effort and included details about whether an Emergency Medical Services (EMS) evaluation was conducted, the timing of the incident and exam, the NFS incident (i.e., length of time NFS occurred, number of times strangled during current incident, history of NFS in relationship, and about whether the victim experienced loss of consciousness, incontinence, difficulty/pain swallowing, loss of memory, loss of voice or changes, throat pain, breathing difficulties, nausea/vomiting, and headache), the physical exam symptoms and locations (i.e., any indication of pain/tenderness, swelling, coughing, drooling, voice changes, combativeness, uncontrolled shaking, dyspnea, petechiae, and bruising), method of strangulation (i.e., one hand, two hands, ligature, approached from front, approached from behind, or other method), a description of the NFS incident, and body sketches/locations of injuries along with photographs using specific forensic equipment (e.g., cameras, UV lights).
Once coding of the forensic exams was complete, NFS cases were separated into three physical exam severity groups (i.e., light, moderate, severe/life-threatening) 4 based on Plattner et al.’s (2005) categorization of physical exam findings and symptomology of victims of manual NFS. Light strangulation was characterized by superficial skin lesions, abrasions, and/or reddening of the neck. Moderate strangulation was characterized by bruising to, and/or bleeding from the neck, and/or damage to soft tissues or larynx as exhibited by sore throat, difficulty swallowing, and hoarseness of voice. Severe, life-threatening strangulation was characterized by petechial bleedings with or without loss of consciousness.
To collect information about domestic violence court records, public records data from the Clerk of Courts were utilized for all NFS cases where the victim consented to a forensic medical examination. The following information was collected from the court records: disposition of the case (sent as formal complaint to the prosecutor, filed or not filed as a formal criminal charge), charge(s) that was filed against the defendant (e.g., domestic battery by strangulation, 2007; aggravated battery, 1988; felony battery, battery, or misdemeanor battery, 2001; all possible charges for domestic violence in Florida [definition of domestic violence, 2002]), whether the defendant pled guilty and which charge(s) the defendant pled guilty to (i.e., original or lesser charge(s)), whether there was an entry of nolle prosequi (i.e., legal termination of prosecution after a charge(s) has been filed with the court), and adjudication decision (i.e., guilty, not guilty, conviction withheld 5 ).
Design and Data Analysis
First, we describe demographic characteristics of offenders and victims, case characteristics, and forensic medical documentation (i.e., reported symptoms by victim, physical exam symptoms documented by FNE, physical exam injuries documented by FNE, and other forensic evidence) of NFS cases (Table 1). Next, we describe the criminal justice response to NFS cases with forensic evidence (Table 2). Finally, we examine offender, victim, and case characteristics, along with NFS forensic medical documentation across legal outcome (i.e., filed as a formal charge or not) to determine what, if any, characteristics and available evidence are associated with the prosecution of NFS. Following prior research, we report results that are significant at the .10 level to account for the small sample size and resulting low statistical power (Gillespie & Reckdenwald, 2017; Montanez et al., 2023; Reckdenwald et al., 2018).
Demographic, Case Characteristics, and Forensic Medical Documentation in Nonfatal Strangulation Cases (n = 63).
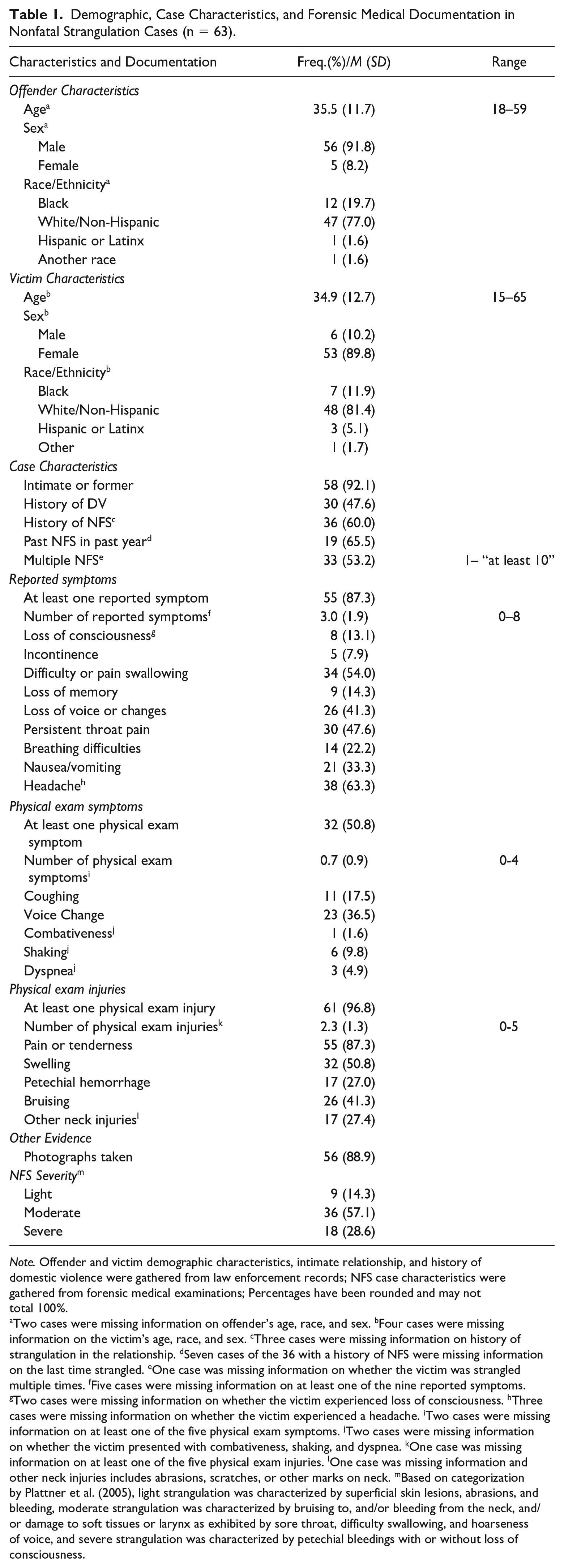
Note. Offender and victim demographic characteristics, intimate relationship, and history of domestic violence were gathered from law enforcement records; NFS case characteristics were gathered from forensic medical examinations; Percentages have been rounded and may not total 100%.
Two cases were missing information on offender’s age, race, and sex. bFour cases were missing information on the victim’s age, race, and sex. cThree cases were missing information on history of strangulation in the relationship. dSeven cases of the 36 with a history of NFS were missing information on the last time strangled. eOne case was missing information on whether the victim was strangled multiple times. fFive cases were missing information on at least one of the nine reported symptoms. gTwo cases were missing information on whether the victim experienced loss of consciousness. hThree cases were missing information on whether the victim experienced a headache. iTwo cases were missing information on at least one of the five physical exam symptoms. jTwo cases were missing information on whether the victim presented with combativeness, shaking, and dyspnea. kOne case was missing information on at least one of the five physical exam injuries. lOne case was missing information and other neck injuries includes abrasions, scratches, or other marks on neck. mBased on categorization by Plattner et al. (2005), light strangulation was characterized by superficial skin lesions, abrasions, and bleeding, moderate strangulation was characterized by bruising to, and/or bleeding from the neck, and/or damage to soft tissues or larynx as exhibited by sore throat, difficulty swallowing, and hoarseness of voice, and severe strangulation was characterized by petechial bleedings with or without loss of consciousness.
Criminal Justice System Response to Nonfatal Strangulation Cases with Forensic Evidence (n = 63).
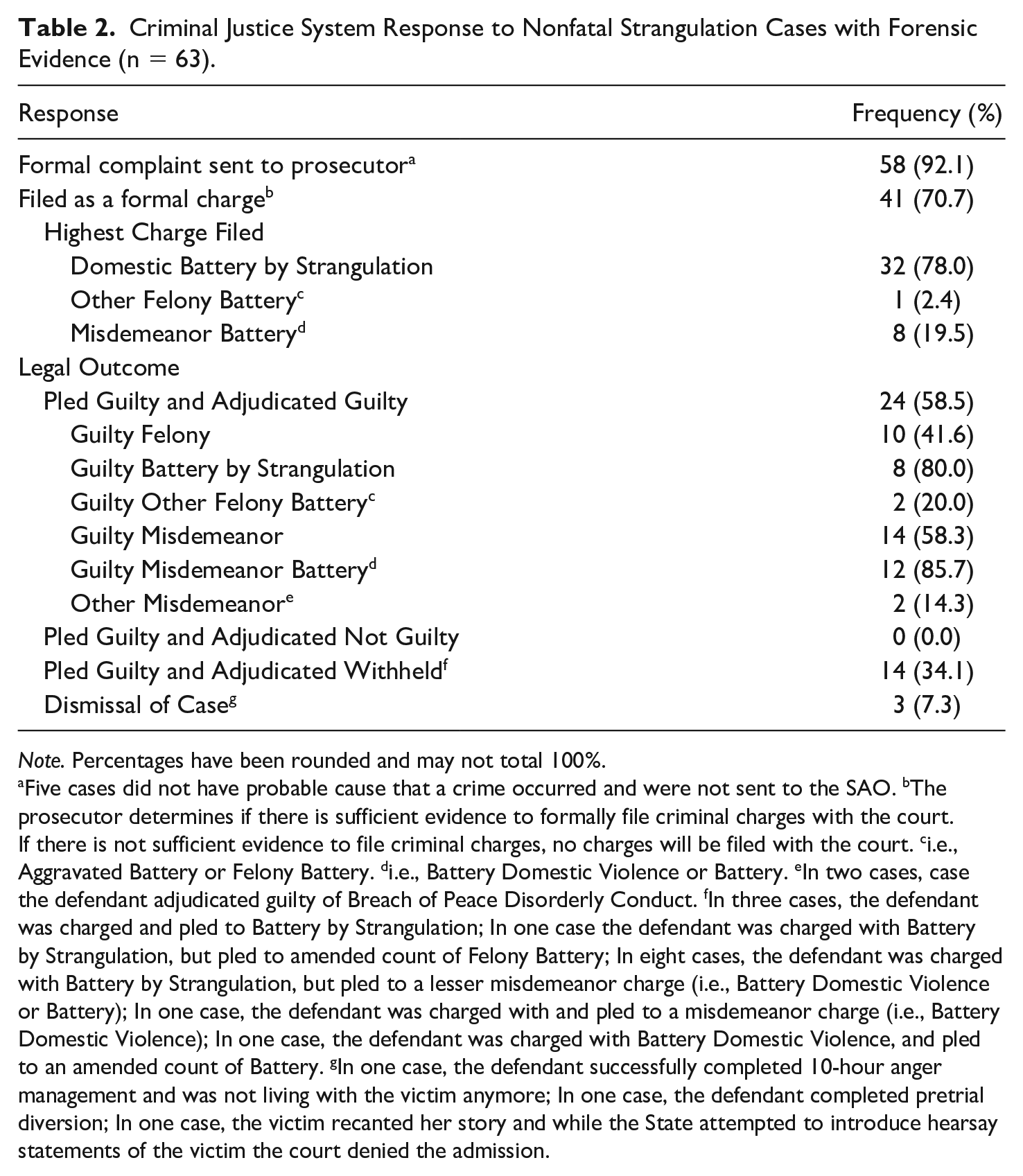
Note. Percentages have been rounded and may not total 100%.
Five cases did not have probable cause that a crime occurred and were not sent to the SAO. bThe prosecutor determines if there is sufficient evidence to formally file criminal charges with the court. If there is not sufficient evidence to file criminal charges, no charges will be filed with the court. ci.e., Aggravated Battery or Felony Battery. di.e., Battery Domestic Violence or Battery. eIn two cases, case the defendant adjudicated guilty of Breach of Peace Disorderly Conduct. fIn three cases, the defendant was charged and pled to Battery by Strangulation; In one case the defendant was charged with Battery by Strangulation, but pled to amended count of Felony Battery; In eight cases, the defendant was charged with Battery by Strangulation, but pled to a lesser misdemeanor charge (i.e., Battery Domestic Violence or Battery); In one case, the defendant was charged with and pled to a misdemeanor charge (i.e., Battery Domestic Violence); In one case, the defendant was charged with Battery Domestic Violence, and pled to an amended count of Battery. gIn one case, the defendant successfully completed 10-hour anger management and was not living with the victim anymore; In one case, the defendant completed pretrial diversion; In one case, the victim recanted her story and while the State attempted to introduce hearsay statements of the victim the court denied the admission.
Results
Offender, Victim, and Case Characteristics of NFS Cases With Forensic Evidence
Demographic characteristics of the victim and the offender as well as case characteristics for the sample of NFS cases that have forensic medical evidence are displayed in Table 1. Based on law enforcement records, offenders involved in the NFS cases were on average 35.5 years old and victims were 34.9 years old. Generally, offenders were male (91.8%, n = 56) and victims were female (89.9%, n = 53). The majority of both offenders and victims were White (77.0%, n = 47 and 81.4%, n = 48, respectively), followed by Black (19.7%, n = 12 and 11.9%, n = 7, respectively). Almost all NFS cases involved intimate or former intimate partners (92.1%, n = 58) and almost half (47.6%, n = 30) had a documented history of domestic violence in the relationship by law enforcement.
During the forensic medical exam, FNEs converse with NFS victims and record details about the assault (e.g., date and time of assault and exam, number of times strangled, history of NFS in relationship and when, modality of the NFS assault; see Reckdenwald et al., 2022, for detailed descriptive analysis of the forensic evidence and a detailed look at the NFS incident). The majority of the NFS cases had a history of NFS in the relationship (60%, n = 36), with 65.5% of those documenting past NFS within the last year (n = 19).
Documentation of NFS Symptoms and Injuries in Forensic Medical Examinations
Evidence documentation of NFS symptoms and injuries as reported in forensic medical examinations for the sample of NFS cases are also displayed in Table 1. After a discussion about the NFS incident, FNEs would record any symptoms victims reported in the time following the NFS incident. FNEs would next conduct a comprehensive physical exam to document NFS symptoms and injuries for health and safety reasons and evidentiary purposes. The majority of forensic exams contained reports of at least one NFS symptom after the assault (87.3%; n = 55), with three symptoms on average reported by victims (range 0–8 reported symptoms). Most forensic exams included reports of headaches (63.3%; n = 38) and pain or difficulty swallowing (54%; n = 34). Thirteen percent of forensic exams documented a loss of consciousness after the assault (n = 8). In addition, more than half of forensic exams had documentation of at least one physical exam symptom (50.8%; n = 32), with 0.7 symptoms on average recorded by FNEs (range 0–4 physical exam symptoms). The highest recorded symptom was voice change, with documentation in 36.5% of forensic exams (n = 23). FNEs recorded at least one physical exam injury in almost all cases (96.8%; n = 61), with 2.3 injuries on average recorded (range 0–5 injuries). Most forensic exams contained evidence of pain or tenderness (87.3%; n = 55) and swelling (50.8%; n = 32). Photographs of injuries were included with 88.9% of forensic exams (n = 56). Based on Plattner et al.’s (2005) physical injury severity categorization of NFS, most NFS cases could be classified as involving moderate strangulation (57.1%; n = 36). Roughly 29% of the NFS cases (n = 18) could be classified as severe, life-threatening strangulation and the remaining 14% of the cases (n = 9) could be classified as light strangulation.
Criminal Justice System Response to NFS Cases With Forensic Evidence
The criminal justice system response to NFS cases with forensic evidence is reported in Table 2. Of the 63 cases identified by police officers as involving NFS and having forensic medical evidence of the assault, 58 (92.1%) cases were determined to have probable cause that a crime occurred and were sent to the prosecutor as a formal complaint. The remaining five cases were determined not to have probable cause that a crime occurred for the following reasons: law enforcement was not able to establish probable cause (n = 2), insufficient evidence (n = 1), inconsistent statements and lack of injuries (n = 1), and unable to determine the primary aggressor and conflicting statements (n = 1). Yet, further examination of the forensic evidence shows that most of these cases (80%) had reported physical injuries and symptoms that could be considered moderate strangulation (n = 2) or severe, life-threatening strangulation (n = 2), and only one could be classified as light strangulation.
In Florida, when a formal complaint is received from a law enforcement agency, police reports are reviewed to determine if there is sufficient evidence to pursue criminal prosecution. If there is sufficient evidence, the formal charging document (i.e., “Information”) with be filed with the court. If there is not sufficient evidence to file criminal charges, no charges will be filed with the court. Of the 58 NFS cases with forensic evidence that were determined to have probable cause a crime was committed and were sent to the prosecutor as a formal complaint, 41 (70.7%) cases were filed as a formal criminal charge with the court. The remaining 17 cases (29.3%) were not considered viable cases for prosecution. Further examination of the forensic evidence shows that almost all of these cases had evidence to support physical injuries and symptoms that could be considered moderate strangulation (82.4%; n = 14). The remaining three cases (17.6%) could be classified as light strangulation.
Of the 41 NFS cases with forensic evidence that were filed as a formal charge, 80.4% (n = 33) were charged as a felony offense as the highest charge, with almost all of those charged with domestic battery by strangulation (97%, n = 32). Legal outcomes were a bit more complex. More than half of the defendants pled guilty (to the original charge or a lesser charge) and were found guilty of a crime (58.5%; n = 24), with the majority being found guilty of a misdemeanor (58.3%, n = 14). Of those found guilty of a misdemeanor, over 85% were found guilty of misdemeanor battery (i.e., battery domestic violence or battery). Defendants in 10 cases (41.6%) pled guilty to a felony (original charge or lesser charge) and were found guilty of a felony, with the majority of these defendants found guilty of battery by strangulation (80%, n = 8). Approximately 34% of defendants pled guilty to the original or a lesser charge, felony (n = 4) and misdemeanor (n = 10), but their conviction was withheld, resulting in no formal conviction with the court. Three defendants had their case dismissed (7.3%) due to various circumstances (i.e., successful completion of 10-hour anger management course, completion of pretrial diversion, victim recanted story).
Demographic, Case Characteristics, and Forensic Documentation by Filing Decision
To further examine legal decisions for the sample of NFS cases with forensic evidence and to determine whether offender, victim, and case characteristics, along with forensic documentation differentiate between those cases that were filed as a formal charge and those cases that were not bivariate tests were conducted. Table 3 reports the associations between NFS case characteristics and legal outcomes (i.e., filing decision). Results suggest that a few factors do indeed differentiate between these cases. Cases that were filed, compared with those that were not, were more likely to be characterized by a greater number of physical exam wounds (2.6 wounds vs. 1.8 wounds, respectively; t = -2.46, p ≤ .05), and physical exam injuries including petechial hemorrhage (36.6% vs. 0%, respectively; χ2 = 8.40, p ≤ .05) and bruising (53.7% vs. 17.6%, respectively; χ2 = 6.36, p ≤ .05). In addition, it appears that cases filed as a formal charge, compared with those that were not, were more likely than expected to involve symptoms and injuries classified as more severe, life-threatening strangulation as characterized by petechial hemorrhages with or without loss of consciousness (39.0% vs. 0%, respectively; χ2 = 9.16, p ≤ .01), and less likely than expected to involve moderate strangulation as characterized by bruising to, and/or bleeding from the neck, and/or damage to soft tissues or larynx as exhibited by sore throat, difficulty swallowing, and hoarseness of voice (48.8% vs. 82.5%, respectively; χ2 = 5.58, p ≤ .05; Plattner et al., 2005). Finally, cases filed as a formal charge, compared with those that were not, were more likely to be characterized with victims experiencing multiple strangulation assaults in the current incident under prosecution (61.0% vs. 35.5%, respectively; χ2 = 3.19, p ≤ .10).
Demographic, Case Characteristics, and Forensic Documentation of Nonfatal Strangulation Cases by Filing Decision (n = 58).
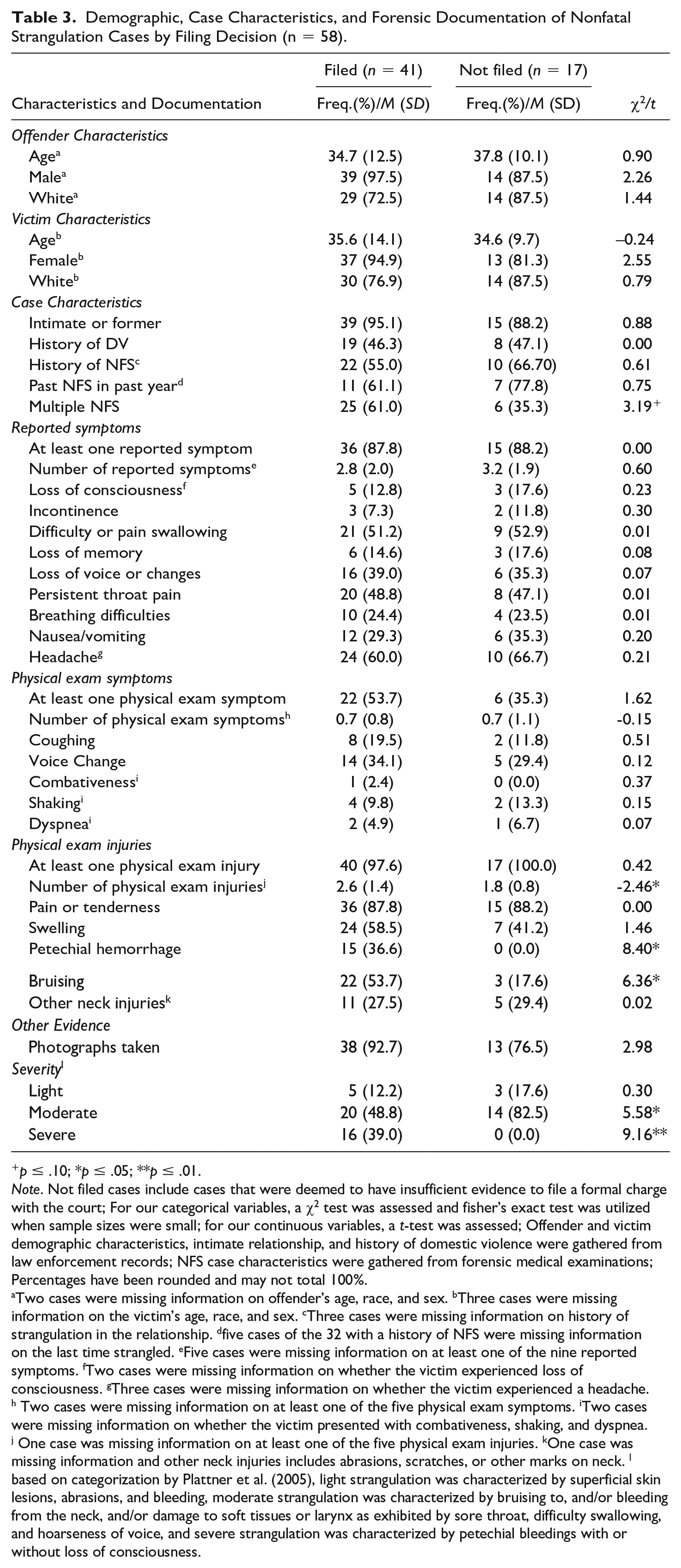
p ≤ .10; *p ≤ .05; **p ≤ .01.
Note. Not filed cases include cases that were deemed to have insufficient evidence to file a formal charge with the court; For our categorical variables, a χ2 test was assessed and fisher’s exact test was utilized when sample sizes were small; for our continuous variables, a t-test was assessed; Offender and victim demographic characteristics, intimate relationship, and history of domestic violence were gathered from law enforcement records; NFS case characteristics were gathered from forensic medical examinations; Percentages have been rounded and may not total 100%.
Two cases were missing information on offender’s age, race, and sex. bThree cases were missing information on the victim’s age, race, and sex. cThree cases were missing information on history of strangulation in the relationship. dfive cases of the 32 with a history of NFS were missing information on the last time strangled. eFive cases were missing information on at least one of the nine reported symptoms. fTwo cases were missing information on whether the victim experienced loss of consciousness. gThree cases were missing information on whether the victim experienced a headache. h Two cases were missing information on at least one of the five physical exam symptoms. iTwo cases were missing information on whether the victim presented with combativeness, shaking, and dyspnea. j One case was missing information on at least one of the five physical exam injuries. kOne case was missing information and other neck injuries includes abrasions, scratches, or other marks on neck. l based on categorization by Plattner et al. (2005), light strangulation was characterized by superficial skin lesions, abrasions, and bleeding, moderate strangulation was characterized by bruising to, and/or bleeding from the neck, and/or damage to soft tissues or larynx as exhibited by sore throat, difficulty swallowing, and hoarseness of voice, and severe strangulation was characterized by petechial bleedings with or without loss of consciousness.
Discussion
The dangers associated with NFS have been well documented in the literature (see e.g., Glass et al., 2008; Joshi et al., 2012; Smith et al., 2001). Yet, lack of evidence typically characteristic of NFS cases makes prosecuting offenders incredibly difficult (Reckdenwald et al., 2020). Under domestic battery by strangulation (2007) in Florida the prosecutor must prove beyond a doubt that the defendant “knowingly and intentionally, against the will of another, impedes the normal breathing or circulation of blood.” This is challenging when law enforcement collecting evidence lack training on NFS and the signs and symptoms (Reckdenwald et al., 2020). A coordinated effort to provide evidence-based prosecution in one Florida county highlighted the valuable evidence that could be available to prosecutors if forensic medical examinations were offered to victims (Reckdenwald et al., 2021). While forensic evidence is essential to corroborate that the victim’s air flow and circulation was disrupted, it is unclear what specific evidence and factors related to the case may impact legal decisions, specifically the prosecutor’s decision to file a criminal charge against the offender, which is largely based on whether the admissible evidence is sufficient to support a conviction.
Our study supports prior research emphasizing the importance of forensic medical evidence in the prosecution of NFS offenders (Reckdenwald et al., 2021). Seventy percent of NFS cases with forensic evidence were filed as a formal charge with the state prosecutor, which is more than the 46.5% found in prior research of NFS cases without forensic medical evidence (Reckdenwald et al., 2020). Of those filed, 78% were filed with domestic battery by strangulation as the highest charge, suggesting that not only did the available forensic medical evidence make the cases more viable for prosecution, but it also helped corroborated the NFS assault so that prosecutors felt confident pursuing the highest felony charge.
Legal outcomes were more complicated, but it appears that convicting offenders of battery by strangulation (even with forensic evidence) is challenging in Florida. The majority of offenders did plead guilty and were adjudicated guilty to either a felony (41%, n = 10) or a misdemeanor (58%, n = 14); however, only eight offenders were found guilty of the felony offense domestic battery by strangulation, representing only 19.5% of all NFS cases that were filed as a formal charge by the prosecutor and only 13.8% of all NFS cases that were sent as a formal complaint to the prosecutor. Despite having forensic evidence to corroborate the NFS assault, there are still several cases in which NFS occurred and no one was charged with a crime. Our results show that in total there were 22 cases (35% of all cases) where trained law enforcement identified strangulation and FNEs collected evidence of the NFS assault, and no one was charged with a crime (five were never sent to the prosecutor to review).
While these findings do show progress in holding offenders accountable when forensic evidence is available in the case (see Reckdenwald et al., 2020 in over 60% of NFS cases no one was charged with a crime), the overall inability of the criminal justice system to hold NFS offenders accountable to the highest degree under the law is still evident. Afterall, these cases have quality forensic evidence to corroborate the NFS assault and based on scholarly evidence, represent cases that have a high risk of future lethality (Glass et al., 2008). These results indicate that there is still work to be done to improve the criminal justice response to NFS, but also underscore the significance of ongoing efforts to address credibility discounting based on social constructs such as gender in the context of domestic violence more broadly (Epstein & Goodman, 2019).
This study also highlights factors that influence prosecutors’ decisions regarding case viability. Much of the factors that were significant represented visible physical evidence of the assault (i.e., number of physical exam injuries, petechial hemorrhaging, bruising), which many tend to associate with NFS. In addition, experiencing multiple strangulations during the assault, which may be seen as an indicator of severity of the assault, was also related to the prosecutor’s decision to file the case. Prosecutors may reason that being able to present this type of evidence would make a guilty verdict more likely, as it may be a more persuasive means to convey the seriousness of the assault to judges and jurors. However, most NFS does not result in visible physical injuries (Strack et al., 2001). For instance, brain injury (traumatic and anoxic-hypoxic), identified by a neurological evaluation, is especially high among abused women who have experienced NFS (Nemeth et al., 2019; Raskin et al., 2023) leading to significant impairments to cognitive and psychological functioning such as deficits in attention, memory, and executive functioning (Valera et al., 2022). Furthermore, research shows that many women who have experienced IPV NFS are unsure whether they have suffered a possible brain injury (Raskin et al., 2023). While forensic medical evidence of the assault is essential as another mechanism in corroborating the assault, considering other nonvisible injuries, such as brain injury, is important too.
Our findings have important policy implications for the criminal justice system, as forensic medical documentation is essential in collecting valuable evidence of a NFS assault to support prosecution outcomes. Along with multidisciplinary collaborations (e.g., Coordinated Community Response Teams, Family Justice Centers) toward IPV and NFS to support the safety and well-being of victims as well as offender accountability, universal NFS policies and protocols are necessary. While professional organizations such as the International Association for Forensic Nurses (IAFN, 2023) have published recommendations and tools to support clinicians to provide medical care and forensic documentation of injuries caused by NFS, oversight and standardization of protocols associated specifically with identification, assessment, documentation, and treatment of NFS are critical. Policies and protocols must be implemented that prioritize routine IPV and NFS screening, appropriate interventions, quality forensic evidence collection via a standardized evaluation tool, nurse examiner resource expansions to include NFS exam fees (similarly to forensic examinations for sexual assaults) to avoid burdening victims with costs, and screening for brain injuries of all NFS victims. In addition, policies addressing training for all professionals involved in the criminal justice process of NFS victims is imperative. All actors in the criminal justice process must fully understand the nature and consequences of NFS—including an understanding that visible physical evidence is commonly lacking in these types of situations, and this lack of visible physical evidence does not mean this was any less of a life-threatening assault. If juries and judges are not trained about the seriousness of strangulation beyond what is visibly apparent, prosecutors are going to have to continue to rely on physical evidence as a key factor when determining case viability.
While considering these results, one needs to also be aware of the limitations to our study. First, our results are based on 63 NFS cases that came to the attention of law enforcement and included forensic medical evidence of the NFS assault during a limited time period. Due to the small number of cases, we were only able to perform descriptive and bivariate analyses. Plus, due to the complexity of legal outcomes, we decided to only examine the filing decision by the prosecutor. Likewise, it is important to note the complexity of prosecutorial decisions (Frederick & Stemen, 2012; Henning & Feder, 2005) and the many factors we were unable to examine in our analyses. This is evident in our finding that cases involving moderate strangulation were less likely to be filed as a formal charge by the prosecutor than what was expected. Clearly, there are other factors and/or a combination of factors that go into the decision to file a NFS case beyond simply noting the presence of certain evidence. Research has shown that this decision involves consideration of a multitude of legal and extralegal factors (Henning & Feder, 2005). Finally, while this is the total number of cases that received a forensic medical exam during this 3-year period, we are aware that we are unable to generalize our results to other counties in Florida or outside of the state due to the nonrepresentativeness of our group of NFS cases.
Conclusion
Research on NFS has expanded in recent years and we have learned a great deal about the nature/context of the use of NFS (Joshi et al., 2012; Nemeth et al., 2012; Thomas et al., 2014; Wilbur et al., 2001), signs, symptoms, and health consequences of NFS (Hawley et al., 2001; Nemeth et al., 2019; Smith et al., 2001; Strack et al., 2001; Thomas et al., 2014; for a review see De Boos, 2019), the association with brain injury (Nemeth et al., 2019; Raskin et al., 2023), best practices for evaluation and treatment (Faugno et al., 2013; Funk & Schuppel, 2003; Plattner et al., 2005), and the value in implementing coordinated efforts in the response to NFS (Reckdenwald et al., 2019, 2021). Our findings extend prior research by highlighting the importance of understanding what factors and evidence are related to NFS legal outcomes, as this can help future collaborative prevention efforts in enhancing NFS evidence collection and can also point to areas that are lacking in the understanding of NFS, including conveying the importance of both physical and nonphysical evidence in the seriousness of NFS along with screening for brain injury in NFS victims. Policy implications point to the necessity of universal protocols for the response to NFS, which include mandated training for all personnel involved in the health and safety response of NFS victims and the availability of no-cost forensic medical examinations to all NFS victims to address any medical issues and acquire quality forensic evidence should they decide to engage in the legal system. Future research should continue to examine NFS prosecution outcomes to further understand the intricacies behind criminal prosecution to hold all NFS offenders accountable and prevent future violence and lethality.
Footnotes
Acknowledgements
This project was made possible from support of the County’s Sheriff’s Office, Florida Health Department, Office of the State Attorney’s Domestic Violence Unit, and the Training Institute on Strangulation Prevention.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability
Due to the sensitive nature of the research, supporting data are not available.