
Abstract
Human immunodeficiency virus type 1 (HIV-1) binds to CD4 receptors. Chemokine receptors such as C-C chemokine receptor type 5 (CCR5), C-C chemokine receptor type 2 (CCR2), and stromal-derived factor (SDF1) are involved in HIV cell entry, and mutations in the genes encoding these chemokine receptors and their ligands may play a role against HIV and acquired immunodeficiency syndrome (AIDS) progression. This study aims to investigate the frequency of the above polymorphisms within the Iranian population, evaluating their contribution to a protective genetic background against HIV acquisition and progression. Two hundred eighty-five healthy individuals and 100 people with HIV were selected. CCR5 genotyping was performed by polymerase chain reaction (PCR). CCR2 and SDF-1 polymorphism were analyzed by tetra-primer amplification refractory mutation system-polymerase chain (Tetra-ARMS-PCR). No CCR5-Δ32 mutants were found in either group. The screening for the CCR2 polymorphism yielded 44 (44%) and 127 (44.6%) heterozygous genotypes in the people with HIV and healthy individuals. Homozygous mutants were seen in 1 (1%) and 28 (9.8%) of the people living with HIV and healthy individuals, respectively, revealing a CCR2-64I allele frequency of 29.7%. CCR2-64I is associated with HIV resistance and reduced AIDS progression (p-value = .018). Among our 385 analyzed samples, 2 (2%) and 12 (4.2%) were found to be SDF1 heterozygous in persons with HIV and healthy individuals, respectively. Three (3%) of the people with HIV and 25 (8.8%) of the healthy individuals carried homozygous mutant variants. The allele frequency of the above polymorphism reached 9.1%, but no statistically significant association was observed, albeit it is borderline (p-value = .062). There are different distributions between people with HIV and healthy individuals, suggesting that CCR2-64I and SDF1-3′A may have a protective effect on HIV and that CCR2-64I (genotype I/I) has an effect on protecting against HIV and delaying progression from HIV status to AIDS. It could be used for prognostic genotyping in people with HIV.
Introduction
Acquired immunodeficiency syndrome (AIDS) arises from infection with two types of human immunodeficiency viruses (HIV-1 and HIV-2) belonging to the Retroviridae family. The lack of an effective vaccine against this virus has made HIV one of the most destructive diseases in the world. 1 According to the World Health Organization, as of 2020, approximately 37.7 million people were living with HIV worldwide, including 36 million adults and 1.7 million children aged 0 to 14, and more than half (53%) were women and girls.2,3 Based on the data of UNAIDS spectrum and modeling, 59,000 people in Iran were infected with HIV in 2019, with nearly 4,100 new infections and 2,500 AIDS-related deaths occurring annually. 4
Of the millions of people who become infected with HIV each year, a small number are resistant to HIV/AIDS.5,6 Genetic mutations are more common in people from the European population, which cause a delay in the progression of AIDS and in some cases even cause immunity, so host genetic diversity plays an important role in susceptibility or resistance to AIDS. 7
Humans are constantly exposed to infectious pathogens. Selective pressure can result in genetic changes necessary to avoid or fight infection. The interesting interaction between HIV and the chemokine receptors has greatly advanced our understanding of AIDS pathogenesis and opened new perspectives for developing effective prophylactic and therapeutic approaches. In HIV acquisition, the CD4 molecule and fusion co-receptors on T cells, which allow the virus to enter the host cell, are critical to achieve the infection. However, there are several other chemokine receptors that are critical for HIV entry into cells. 8
Based on the use of CCR5 or C-X-C chemokine receptor type 4 (CXCR4) as co-receptor, HIV-1 strains are divided into three groups. 9 CCR5 (R5), CXCR4 (X4), and R5X4-tropic strains. 10 Other chemokine receptors, CCR2, C-C chemokine receptor type 3 (CCR3), C-C chemokine receptor type 8 (CCR8) and C-C chemokine type 9 (CCR9), can act as alternative co-receptors. 11 Numerous reports have shown that polymorphisms in CCR5, CCR2 genes, and stromal-derived factor 1 (SDF1) are strongly or weakly correlated with the variable rate of progression of viral infection to AIDS. 12 However, the precise impact of polymorphisms on these genes on susceptibility to HIV-1 infection and AIDS progression is still challenging and controversial. 13
The CCR5 wild-type (CCR5-wt) protein consists of 352 amino acids. The CCR5 mutation is by deletion of 32 bp (CCR5-Δ32) in the coding region, resulting in a short protein that is undetectable on the cell surface. 14 The CCR5-Δ32 has been shown to significantly affect HIV entry as well as progression to AIDS. Individuals homozygous for CCR5-Δ32 appear to be resistant to HIV-1 infection, while individuals heterozygous for this defect result in delays in infection progression. 15 Different distribution patterns of CCR5-Δ32 have been observed in different ethnic populations, with a high frequency appearing in Caucasians and northern European individuals (10%) and a low frequency in Asians. 16
CCR2 is a co-receptor for HIV-1, and CCR2-64I is a point mutation (valine at position 64 is replaced by isoleucine) that delays disease progression to AIDS for 2–4 years. 17 Similar studies have shown that people with one or two copies of CCR2-64I had a 58% reduction in AIDS risk in the first 4 years after HIV acquisition and a 19% reduction in the next 4 years. 8 Recent studies have shown that the homozygous allele CCR2-64I could be the cause of the natural resistance to sexual contact transmission of HIV-1 in Asia. Similar analyses showed a reduced risk of death in the first 8 years after HIV acquisition in carriers of the CCR2-64I allele. 18
SDF1 is the principal ligand of CXCR4, which is also called C-X-C motif chemokine ligand 12(CXCL12). In SDF1-3′A, G to A mutation at position 801 has been shown to inhibit AIDS progression in homozygous individuals, particularly in the late stages of HIV-1. 19 The functional interaction of CCR5/CCR2 and SDF1 may explain the increased protection against HIV/AIDS in individuals with the previously mentioned mutations. CCR5/CCR2 variants are thought to slow disease progression by limiting the number of CCR5 receptors that mediate R5 HIV-1 infection. Furthermore, the SDF1-3′A variant has been shown to limit the emergence of X4 HIV-1 strains. 8
The prevalence of these genetic variants, particularly among HIV-1 seropositive and seronegative high-risk individuals, is unknown in Iran. It will be crucial to comprehend how these genetic variants affect Iran’s vulnerability to HIV-1 infection. Identification and the distribution of allelic variants CCR5-Δ32, CCR2-64I, and SDF1-3′A may help to understand the burden and course of the disease. In this study, we investigated three chemokine variants in Khuzestan province, Ahvaz city, and analyzed the host gene polymorphisms and its association with CD4+ T-lymphocyte counts and viral load levels as progression markers in an attempt to elucidate its role in the Iranian population.
Material and Methods
Ethical issues
The current research was approved by the ethics committee of Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran, with the registration number OG-9922 and ethical code IR.AJUMS.MEDICINE.REC.1399.022. Volunteers were informed of the present research, and written consent was obtained before their enrollment.
Study population
A total of 385 individuals from Khuzestan province participated in this case-control study in 2021. Of these, 285 were healthy individuals, and 100 were people with HIV. Samples of healthy group were collected from a high-incidence population consisting of surgeons and their assistants, nurses, and Laboratory worker from Allameh Karami Hospital. Samples of case group were obtained from Behavioral Diseases Counseling Center in Ahvaz. Informed consent was obtained from all study participants. All patients were receiving antiretroviral therapy (ART) when the study was conducted. The inclusion criteria for the case group were as follows: (1) patients were HIV-Ab positive and confirmed with Real-time polymerase chain reaction (PCR) assay. (2) The participants were residents of Khuzestan province, and (3) they had the intellectual capacity to give written informed consent, and. The inclusion criteria for the control group were as follows: high incidence population with HIV-Ab negative test. Patients’ medical profiles were checked for demographic information, clinical history, and laboratory characteristics such as viral load and CD4 count. Patients were classified according to current Centers for Disease Control and Prevention criteria in three CD4+ T lymphocyte categories, defined as (1) ≥500 cells/mL, (2) 200–499 cells/mL, and (3) <200 cells/mL. On the other hand, HIV-1 RNA levels in plasma cover a dynamic range of 400–750,000 copies of HIV-1 RNA per ml of blood, allowing us to classify patients according to the amount of HIV-1 RNA as low-level or undetectable (<400 copies/mL), middle (400–100,000copies/mL), and high-level (>100,000 copies/mL). 20
Collection and preparation of the specimens
Approximately 5 mL of peripheral blood was collected from all volunteers in a sterile Ethylenediaminetetraacetic acid (EDTA)-containing vacutainer tube. Peripheral blood mononuclear cells (PBMCs) were isolated, and 2 cc of blood for preparation of serum sample for screening (HIV Ab) and confirmatory test (real-time PCR) were collected. The PBMCs and serum samples were stored at −70°C until testing.
Serological and real-time PCR tests
Anti-HIV antibodies in healthy serum samples were detected using a third-generation commercial Enzyme-linked immunosorbent assay (ELISA) kit (PISHTAZTEB, Diagnostic, Tehran, Iran, REF:PT-HIV1-2 Ag-Ab 192) according to the manufacturer’s instructions. Real-time quantitative PCR was performed by HI Virus-1 RG RT-PCR (Qiagen, product of Germany, REF:4513265) for the case group at the Behavioral Diseases Counseling Center.
Isolation of genomic DNA
PBMCs were obtained from 5 cc whole blood by density centrifugation using ficoll gradients (Inno-train-Germany). Briefly, after removing the plasma, an equal volume of blood phosphate buffered saline (PBS) was added and mixed gently. Then the blood and buffer mixture was carefully layered onto a 4 mL ficoll in a 10 mL tube and centrifuged at 400 g for 20 min at 18–24°C. The top layer was aspirated, and the undisturbed PBMC layer was transferred to a new tube. Finally, mononuclear cells were washed using PBS at a 400×g centrifuge for 10 min. Genomic DNA extraction was performed from PBMC samples using the salting-out procedure, which consists of lysing the cell with a lysis buffer (NaCl 5 M, Tris-HCl 1 M, and EDTA 0.5 M), proteinase k, and detergent Sodium dodecyl sulfate (SDS 10%); removing proteins with salt (NaCl 6 M); and finally ethanol precipitation according to the protocols described in previous studies.21,22 DNA purity and concentration were assessed by a Nanodrop (Thermo), estimating the A260/A280 ratio stored at −70°C until investigation. Also, DNA purity by gel electrophoresis was shown in Figure 1.

Electrophoresis analysis of DNA purity. Lane 1: DNA ladder 1 kb, lane 2: sample 1 (S1), lane 3: sample 2 (S2).
Evaluation of CCR5-Δ32, CCR2-64I, and SDF1-3′A polymorphisms by PCR and tetra-ARMS PCR
The PCR was used to detect CCR5 genotypes with primers listed in Table 1. The PCR reaction mixture contained 12.5 µL Master mix 2 × (Amplicon), 1 µL of each primer, 2.0 µL genomic DNA, and D/W up to 25 µL. PCR program was performed in a thermocycler (Peglab). The reaction mixture was subjected to an initial denaturation of 95°C for 5 min followed by 35 cycles of 95°C for 30 seconds, 51°C for 30 s, and 72°C for 55 s. The final extension was done at 72°C for 10 min. The amplified products were analyzed on 2% agarose gel, and bands were visualized on Ultraviolet (UV)-transilluminator (Biorad). The wild-type gene resulted in a 276 bp fragment (Fig. 2), while the Δ32 mutant variant resulted in a 244 bp fragment. Heterozygotes produced both of the bands. 23
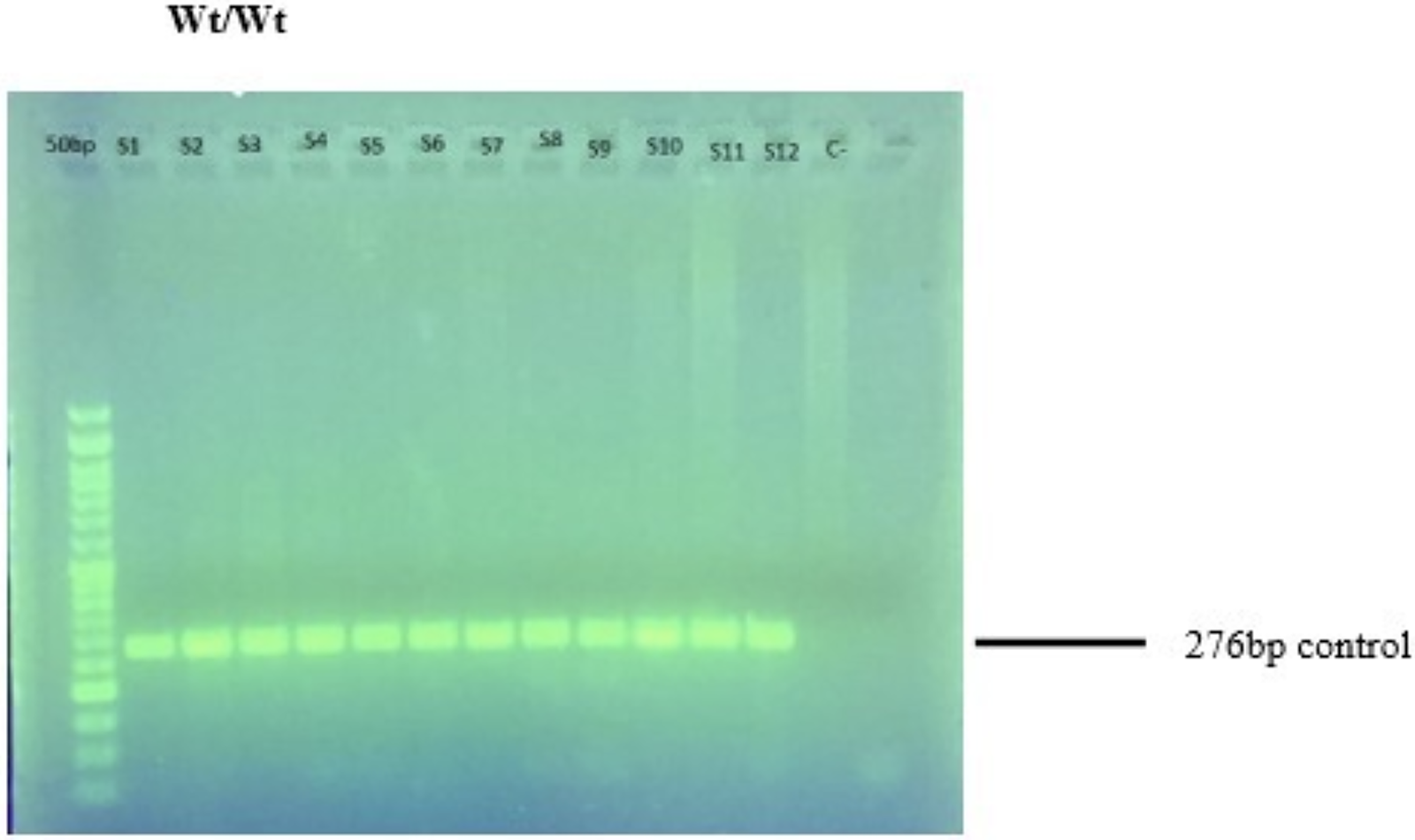
Electrophoresis analysis of CCR5. Amplification results in a 276-bp product for CCR5 wild type. Lane 1: DNA ladder; S1–S12: CCR5 wild type (Wt/Wt). CCR5, C-C chemokine receptor type 5.
The Sequences of Primers, Amplicon Size
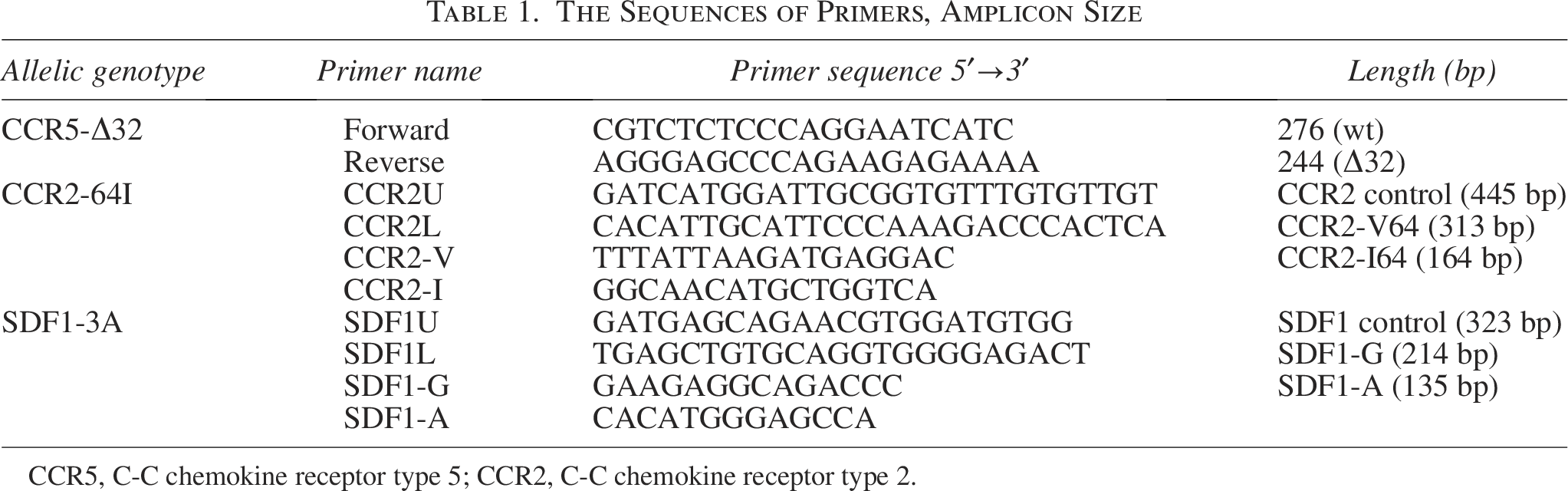
CCR5, C-C chemokine receptor type 5; CCR2, C-C chemokine receptor type 2.
CCR2-64I and SDF1-3′A gene polymorphisms were studied by tetra-ARMS PCR using specific primers (Table 1). The reaction was carried out in a total volume of 25 µL consisting of 12.5 µL of PCR master mix, 1 µL of each primer, 3 µL of genomic DNA (∼50 ng/µl), and 5.5 µL of distilled water with the following thermal cycling condition: 10 min. at 94°C, 22 cycles (first round) of 94°C for 30 s, 58°C for 30 s, 72°C for 60 s, 28 cycles (second round) of 94°C for 30 s, 42°C for 30 s, 72°C for 60 s, and a final extension of 7 min. at 72°C. PCR products were examined in 2% agarose gel with DNA-safe Stain (0.5 µL) and visualized with a UV transilluminator. Amplification results with PCR products 445 bp, 313 bp, and 164 bp were shown for the CCR2 locus (control), CCR2-V64 allele, and CCR2-64I allele, respectively. Two PCR products on the gel (Fig. 3) represent wild-type (CCR2-V64) or mutant homozygous (CCR2-64I), while three bands on the gel represent mutant heterozygous (CCR2-V64I). 24
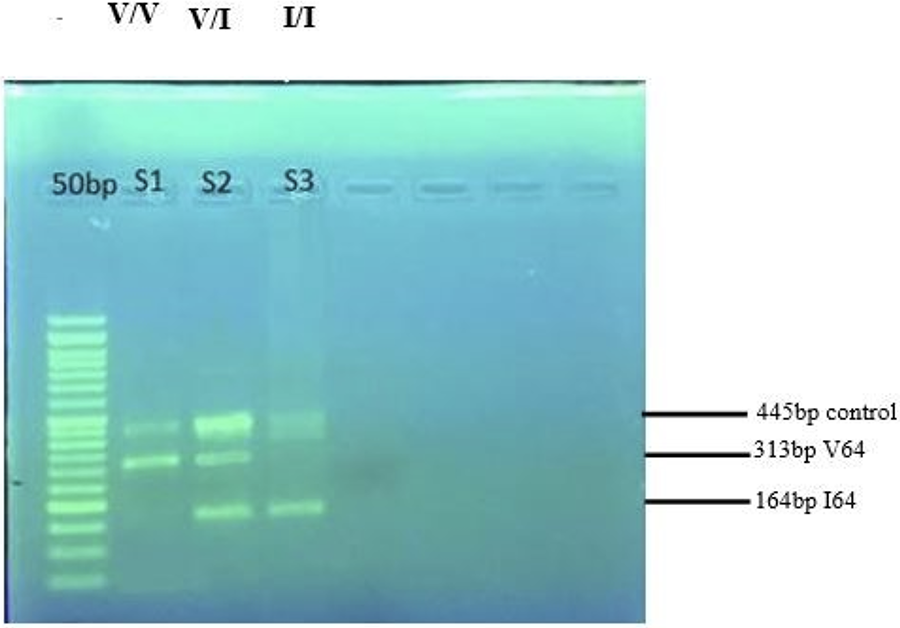
Electrophoresis analysis of CCR2-V64I. The first band in the PCR results in amplification of 445 bp of CCR2 locus (control). Amplification results in a 313-bp product for CCR2-V64 and a 164-bp product for the CCR2-I64 allele. Lane 1: DNA ladder; lane 2 (S1): homozygous wild-type CCR2-V64 (V/V); lane 3 (S2): heterozygous CCR2-V64I (V/I); and lane 4 (S3): homozygous mutant CCR2-64I (I/I). CCR2, C-C chemokine receptor type 2; PCR, polymerase chain reaction.
SDF1-3′A Tetra arms PCR carried out in the same reaction with CCR2. The reaction mix was amplified with the following conditions: 10 min. at 94°C, 14 cycles (first round) of 94°C for 30 s, 64°C for 30 s, 72°C for 60 s, 39 cycles (second round) of 94°C for 30 s, 53°C for 30 s, 72°C for 60 s, and a final extension of 7 min. at 72°C. The expected product was electrophoresed on a 2% agarose gel and stained with a DNA-safe stain for visualization (Fig. 4). Genotypes Wild-type SDF1- (G/G), heterozygous (G/A), and homozygous mutant (A/A) were distinguished according to band number and size (Table 1). 24
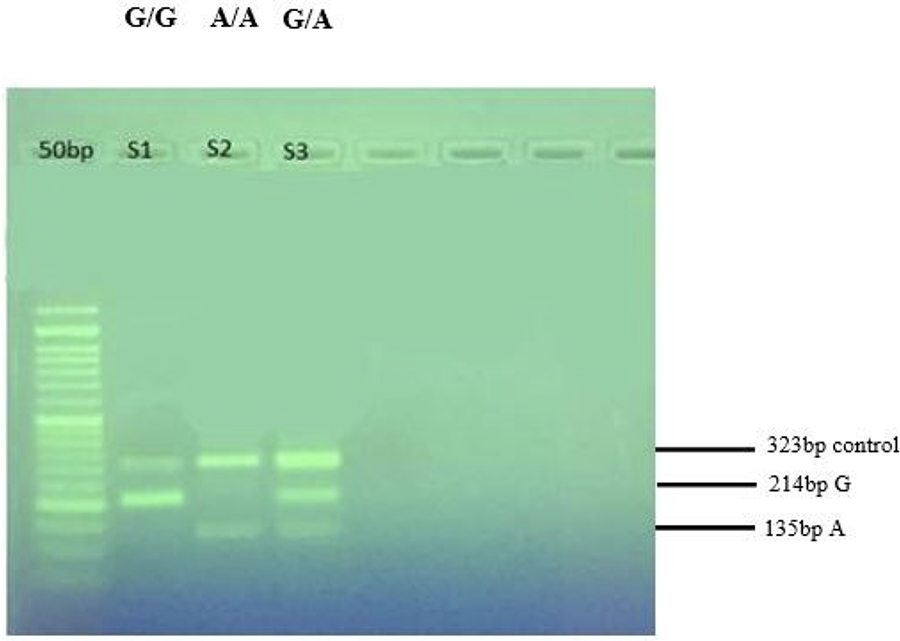
Electrophoresis analysis of SDF1-3′A. The first band in the PCR results in amplification of 323 bp of SDF1 locus (control). Amplification results in a 214-bp product for SDF1-G and in a 135-bp product for SDF1-A. Lane 1: DNA ladder; lane 2 (S1): homozygous for SDF1-G801 (G/G); lane 3 (S2): one homozygous for the SDF1-A801 allele (A/A); and lane 4 (S3): heterozygous (G/A). PCR, polymerase chain reaction.
Statistical analysis
Mean and standard deviation are used to describe quantitative variable data, while frequency and percentage are used for qualitative variables. The normality of the data was checked using the Kolmogorov–Smirnov test, the QQ plot (quantile–quantile plot), skewness, and the kurtosis coefficient. A univariate analysis of the data was performed using the chi-square test, the Mann–Whitney test and simple logistic regression. Multiple logistic regression was used for multivariate data analysis. The allelic frequencies were calculated by Hardy–Weinberg equilibrium (HWE) analysis. The level of significance was considered p < .05. All analyses were performed using SPSS version 22 software.
Results
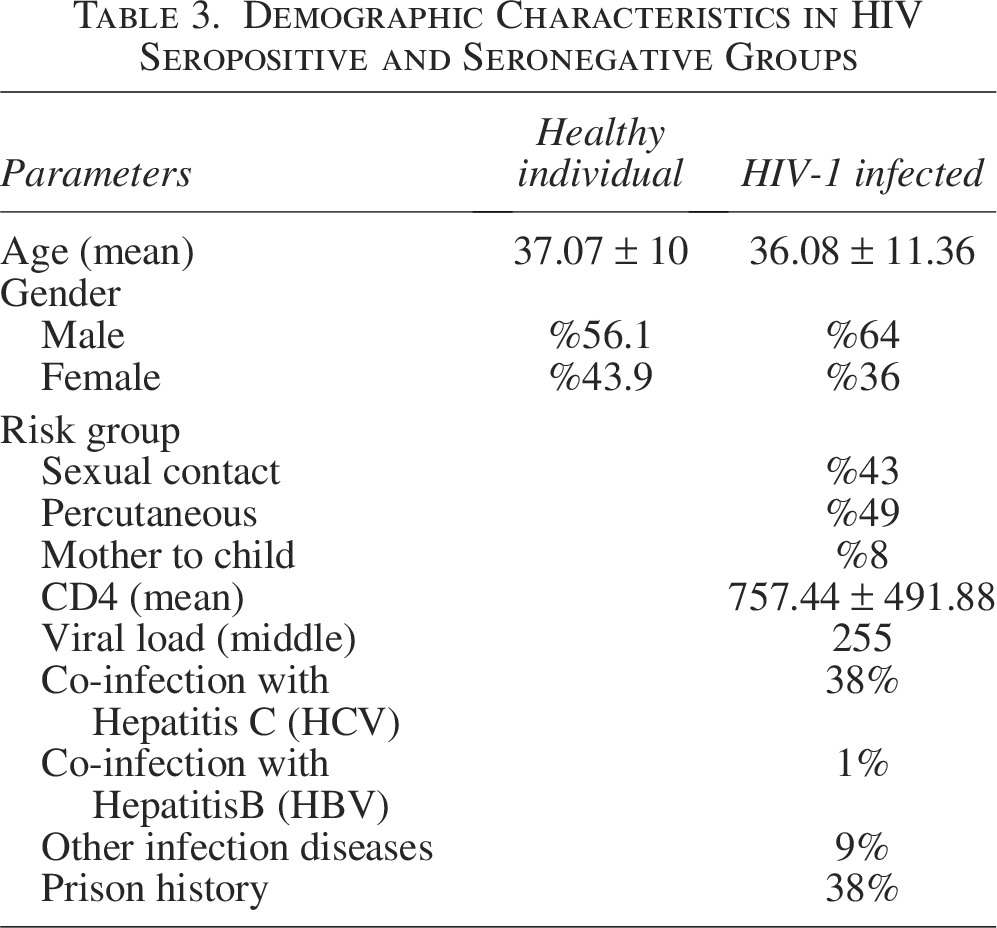
A total of 385 individuals comprising 224 males (58.2%) and 161 females (41.8%) with a mean age of 36.82 ± 10.37 were enrolled in the study. Of these individuals, 100 (25.97%) were infected with HIV and 285 (74.03%) were healthy. Age and gender distribution of the study population are shown in Table 2. The mean age was 36.08 ± 11.36 for people with HIV and 37.07 ± 10 for healthy individuals. Demographic data are shown in Table 3. In this study, there was no statistically significant difference observed between people living with HIV and healthy individuals from age and gender (p = .17).
Age and Gender Distribution of the Study Population

Demographic Characteristics in HIV Seropositive and Seronegative Groups
Genotyping
Of all samples subjected to the genotyping process, homozygous and heterozygous variants of CCR5-Δ32 were not found in either group. This means that all participants were wild-type for CCR5.
The V/V genotype represents the wild-type genotype (CCR2 V/V), whereas V/I codes for the heterozygous mutant CCR2 V/64I and I/I for the homozygous mutant genotype CCR2 64I/64I. CCR2-V64 was seen in 185 individuals (48.1%), including 55 (55%) people with HIV and 130 (45.6%) healthy individuals. The frequencies of the CCR2-V64I genotype in people with HIV and healthy individuals were 44 (44%) and 127 (44.6%), respectively. CCR2-64I genotype was also detected in one (1%) of the people with HIV and 28 (9.8%) of the healthy individuals. Univariate and multivariate analyses showed that the acquisition and progression of HIV status in participants with heterozygous CCR2-V64I genotype is 0.82 times lower than in patients with wild-type genotype, but there is no statistically significant difference (p-value = .396). The homozygous for the CCR2-64I allele is highly protective against HIV acquisition or AIDS progression toward CCR2-V64 genotype (p-value = .018).
SDF1 wild-type genotype (G/G) was observed in a total of 343 patients (89.1%), including 95 (95%) people with HIV and 248 (87%) healthy individuals. A heterozygous mutant genotype (G/A) was reported in 2 patients (2%) and 12 (4.2%) in people with HIV and healthy individuals, respectively. Homozygous mutant genotype (A/A) was observed in 3 patients (3%) from people living with HIV and 25 (8.8%) from healthy individuals. People with the heterozygous genotype had a 0.43 times lower chance of HIV acquisition or progress to AIDS compared with participants with the wild-type SDF1 genotype, but it is not significant (p-value = .278). In addition, the probability of susceptibility to infection or delayed HIV disease progression in homozygous mutants is about 0.31 times lower than in individuals with wild-type genotype. There was no statistically significant difference, but it is borderline (p-value = .063) (Table 4).
Distribution of CCR2-64I and SDF1-3′A Gene Polymorphisms

n = number of subjects.
CCR2, C-C chemokine receptor type 2.
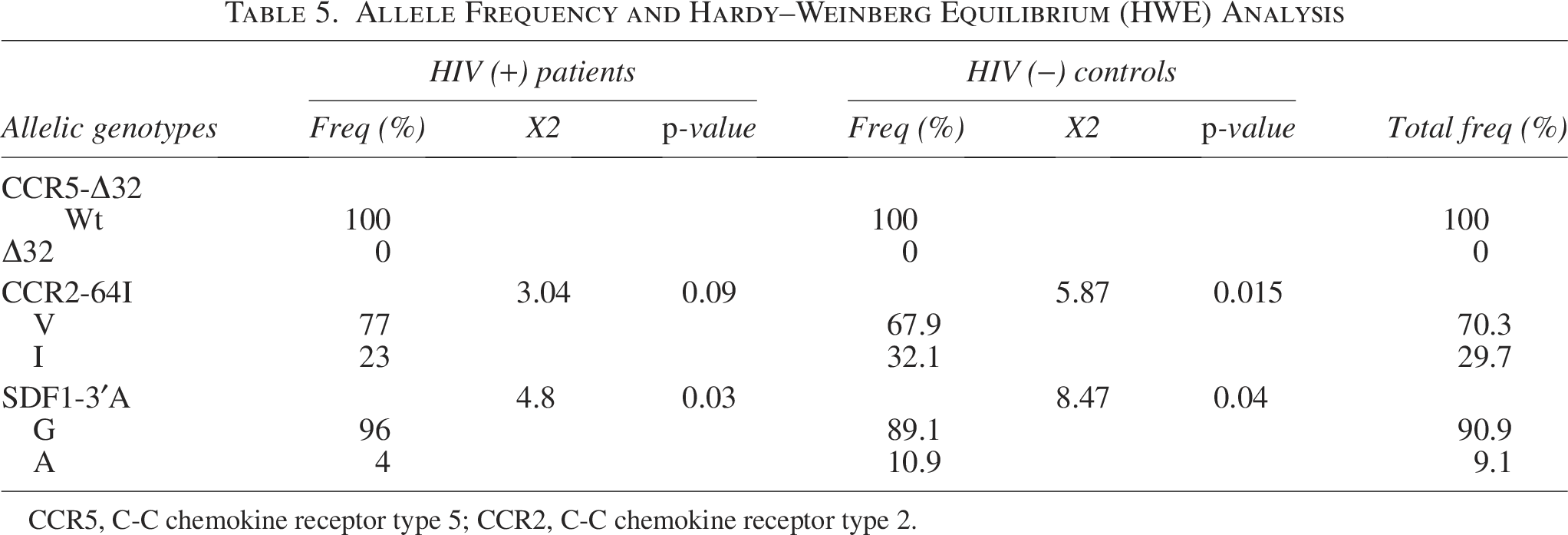
Allelic frequencies are shown in Table 5. The HWE analysis revealed that all genetic variants for CCR2 and SDF1 in the studied population were in equilibrium. (
Allele Frequency and Hardy–Weinberg Equilibrium (HWE) Analysis
CCR5, C-C chemokine receptor type 5; CCR2, C-C chemokine receptor type 2.
Discussion
HIV is a highly pathogenic virus compared with several other pathogens. Most unequivocal information is available on the impact of genetic variants of CCR5, CCR2, and the chemokine SDF 1 on the rate of HIV progression.25,26 Cohort studies showed that the presence of CCR5-Δ32, CCR2-64I, and SDF1-3′A polymorphisms can confer resistance to HIV1 infection or slow progression to AIDS. 27
This study describes the genotype and allele frequencies of the CCR5-Δ32, CCR2-64I, and SDF1-3′A in HIV-1 infected patients and healthy individuals in Khuzestan, Iran, and their effects on surrogate markers (HIV-1 RNA levels in plasma and CD4 + T cell counts) as indicators of HIV-disease progression. No individual was found to carry the CCR5-Δ32 mutation in this research. The frequency of CCR5 Wild/Δ32 mutant genotype in healthy and HIV-1 infected individuals vary from 0.7% to 3% in Northeast Iran by Tajbakhsh et al., Heydarifard et al., and Omrani et al. Consistent with our findings, Tajbakhsh and Heydarifard reported very low prevalence of CCR5Δ32/Δ32 mutant genotype (0%–0.25%).16,28,29 In several studies in accordance with the present study by Laying et al. (2005, Cameroon), Qijian Su et al. (2009, China), and Deepak Bharti et al. (2015, India), no mutation of CCR5 was observed.30,31 The frequency of CCR5Δ32 in some Asian and European countries is reported to be 0%–2% and 10%, respectively. 32 Overall, the results of the present study and other studies conducted in Iran showed that the Iranian population is more susceptible to HIV compared with other races, especially the European race. The frequency of the CCR5-Δ32 was high in Caucasians (15%), but low or even absent in Asians and Africans. 33 It is noteworthy that individuals who have this mutation hemizygously show higher resistance to HIV-1 infection. Patients with a heterozygous genotype will develop AIDS 2 to 3 years later than patients without the mutation. 9
The CCR2-64I polymorphism is associated with HIV resistance and reduced AIDS progression. Several studies have shown that the CCR2-64I allele is widespread in different countries with different populations. 34 The study conducted by Osman Köksal et al. (2021, Turkey) displayed that the frequency of the heterozygous CCR2-V64I genotype in people with HIV and healthy groups was 31% and 34%, respectively, which is almost the same as our study. The study of Gharagozloo et al. (2004, Iran) reported that the frequency of CCR2-V64, heterozygous, and homozygous mutants in normal papulation of Fars province were 78.1%, 19.4%, and 2.5%, respectively, which can be concluded that CCR2-64I mutation is common in Iranian population and may be associated with slower progression of HIV status in Iran. 35 Besides, in contrast to our study, Xiao-feng He et al. (2011, China) indicate that the CCR2 polymorphism may not have a protective effect against HIV-1 infection in Chinese participants and the population is susceptible to HIV-1 infection. 36
In the present study, the frequency of CCR2-64I allele was reported as 29.7% in all people and was not the same in HIV-1 seropositive and seronegative patients (Table 5). The high frequency of CCR2-64I was reported in sub-Saharan Africa and some Asian populations, such as Thailand, the Philippines, and Hong Kong, while the frequency is slightly lower in Turkish, Fars province of Iran, and Europeans. 37 Overall, the results show that CCR2-64I mutation is widespread enough in the Iranian population. Consequently, I allele is likely an allele that arose before the east and west migration of the Indo-European ancestors. 35
The CCR2-V64I mutation affects the function of the receptor on the surface of the cell. This may further impact disease acquisition and progression. 38 Analysis of race, sample size, and control population showed that the CCR2-64I genotype was associated with a reduced risk of HIV-1 infection in mixed-race populations. 39
Some projects reported a protective role of SDF1-3′A against HIV. 37 Similarly, Osman Köksal et al. (2021, Turkey) reported that the frequency of heterozygous and homozygous mutant genotypes was 38% and 8% in HIV-positive and 40.5% and 9.9% in healthy individuals, respectively. No significant difference in SDF1-3′A Polymorphism in the studied groups. 8 In the same way Xiao-Hua Tan et al. (2009, China) found the frequency of heterozygous mutant genotype was 51.8% in people with HIV and 51.7% in healthy individuals, while the frequency of homozygous mutant genotype in people with HIV and healthy individuals was 32.3% and 30.7%, respectively. Although the frequency of polymorphisms is higher than in our study, consider that no statistically significant difference was observed between the two groups. 23 In the study by Cline Nkenfou in the western region of Cameroon, heterozygous mutant was observed in people with HIV and healthy individuals, but homozygous mutant was not reported in either group. 34
In all participants examined, the allele A was 9.1%, which is not the same in people living with HIV and healthy individuals (Table 5), which is similar to Osman Köksal et al in Turkey. 8 In the study by Cline Nkenfou, the distribution of A and G alleles was 50% in both groups, which is not consistent with the present study. 34 This finding could subscribe to the chemokine blocking model in the prevention of HIV-1 infection. It is known that the SDF-1 chemokine down modulates CXCR4 expression on CD4+ T cells. 40
These polymorphisms alter the clinical course of the disease and affect the survival of patients. Our study indicated that the CCR2-64I and SDF1-3′ A polymorphism have protective effects on viral load or CD4+ cell counts of patients under ART (p < .5) (Data are not shown). The majority of HIV-1 isolates in Iran are of the subtype CRF-35AD. 41 It is possible that the relative genetic homogeneity of these clade isolates may have some implications for the resistance of SDF1-3′ A polymorphism involved in HIV-1 infection. 40 There is no evidence for a genetic subtype dependent on the inhibitory effect of CCR2 and SDF-1 on different clade isolates from Iran.
So far, several patients who are infected with the HIV virus have been definitively cured by receiving a bone marrow transplant from a donor with the CCR5-Δ32/Δ32 mutation, and the protection against AIDS provided by CCR5-Δ32 is continuous during the course of infection. 42 In contrast, the protection provided by CCR2-64I and SDF1-3′A is greatest early in the course of infection. Individuals with one or two copies of CCR2-64I and SDF1-3′A have lower risk of AIDS during the first 4 years. 18
Actually, we want to know about the genetic status of the society, and we needed to compare them with patients. If there is a positive and significant relationship between these polymorphisms and reduction of the risk of HIV infection in high-incidence population, these polymorphisms can be introduced as a protective role against HIV. The identification of CCR2-64I and SDF1-3A polymorphisms plays an important role in determining the prognosis and controlling the progress of HIV disease toward AIDS. These polymorphisms alter the clinical course of the disease and affect the survival of patients. 40
Overall, the results of this study and other studies showed that the difference in the distribution of CCR2-64I and SDF1-3′ A gene polymorphism is related to the difference in geographic region, race, control population, type of mutation detection technique, and sample size. Variation in HIV-1 transmission and/or disease progression has been associated with a combination of host genetic factors. 34 The benefit of these mutations can contribute to the resistance of human populations to infectious diseases; the mechanism leading to the accumulation of these changes remains unknown. Therapeutic strategies aimed at altering the receptor or blocking the interactions of HIV and co-receptors through chemokines or their synthetic analogues are effective in combating HIV status or delaying its progression. It is unknown yet, but perhaps as there are CCR5-inhibitors such as maraviroc, which are an important in anti-HIV-1 therapy, we may be able to produce SDF1 and CCR2-inhibitors, if the results are confirmed. We still do not know about their effect on the ART regime. 43 These findings provide baseline information that will help us in the future. 44 A large cohort of people with HIV-1 and monitoring their possible progression to AIDS would be suitable to further evaluate the significance of our findings.
Conclusion
This is the first study to report chemokine receptor variant frequencies in people living with HIV in southern Iran. The present data show that no polymorphism of CCR5 was detected. The distribution of CCR2-64I and SDF1-3′A was different between people with HIV and healthy individuals, suggesting that these mutations may have a protective effect against HIV, but among them the effect of CCR2-64I (genotype I/I) in protecting against HIV is more obvious. Further investigations into the frequency of these polymorphisms in Iran are important in order to clarify the susceptibility rate of individuals to HIV.
Authors’ Contributions
M.B.: Conducting research and investigation process, specifically performing experiments or data; S.J.: Design of methodology; S.H.: Application of statistics to analyze study data; M.B.: Development of methodology; R.N.: Analysis of clinical features of patients; A.A.: Ideas; formulation or evolution of overarching research goals and aims; writing of the article.
Footnotes
Acknowledgments
This article is extracted from final thesis of Mrs. Mina Bavi for her course of MSc Medical Virology with registration number OG-9922. The authors thank the individual volunteers who provided their samples for these studies.
Author Disclosure Statement
No conflict of interest relevant to this article was reported.
Funding Information
This study was supported by Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran. Registration number OG-9922.
Author Confirmation Statement
The authors are all from Ahvaz Jundishapur University of Medical Sciences (Ahvaz, Iran), where education and research are the primary functions.