
Abstract
With the widespread use of antiretroviral therapy, the clinical spectrum among people with HIV has evolved significantly. This study aims to investigate the dynamic changes in the primary indications and final diagnostic spectrum of bone marrow examinations in this population. We conducted a retrospective analysis of 154 hospitalized individuals with HIV who underwent bone marrow examination at Mengchao Hepatobiliary Hospital of Fujian Medical University, the largest designated HIV/AIDS care hospital in Southeast China, from September 2019 to December 2025. Demographic, laboratory, and pathological data were collected, and participants were stratified into tumor and nontumor groups based on final diagnosis for comparative analysis. Among the indications for bone marrow examination, the proportion of procedures performed due to cytopenia decreased from 55.55% in 2019 to 17.86% in 2025. Conversely, the proportion performed for suspected hematological malignancy or to assess tumor marrow infiltration increased significantly from 11.11% to 60.71%. Final diagnoses revealed that the proportion of malignant tumors increased from 11.11% to 53.57%, whereas the proportion of opportunistic infections showed a declining trend. The Cochran–Armitage trend test confirmed that the proportion of opportunistic infections decreased significantly (p = .002), while the proportion of malignancies increased significantly (p = .002). Compared to the nontumor group, individuals in the tumor group were older, had significantly higher proportions receiving antiretroviral therapy, higher rates of HIV RNA suppression, as well as significantly higher CD4+ T-cell counts, CD8+ T-cell counts, lymphocyte counts, platelet counts, and lactate dehydrogenase levels. Our findings demonstrate that the clinical indications for bone marrow examination in people with HIV have shifted from the evaluation of traditional opportunistic infections and unexplained cytopenia toward the diagnosis and staging of malignant tumors, particularly hematological malignancies. These results suggest that in the contemporary management of HIV, greater emphasis should be placed on screening for malignancies.
Introduction
Bone marrow examination is a critical procedure for evaluating the structure and function of the hematopoietic system. 1 The combined use of bone marrow aspiration and biopsy holds significant diagnostic and differential diagnostic value in people with human immunodeficiency virus (HIV). 2 Its core indications include evaluating unexplained pancytopenia, identifying the cause of fever of unknown origin (FUO), detecting etiologic agents of infection and assessing the tumor involvement of bone marrow.3,4
Over the past decades, with increased public awareness of HIV, expanded testing, and the widespread use of antiretroviral therapy (ART), the incidence of opportunistic infections among people with HIV has declined significantly.5,6 In contrast, the incidence of malignancies, including non-AIDS-defining cancers such as Hodgkin lymphoma, has gradually increased.7,8 In the early years of the HIV epidemic, the primary indications for bone marrow examination were often clinical manifestations such as opportunistic infections, FUO, and pancytopenia. However, clinical practice has evolved, and bone marrow examinations are increasingly focused on diagnosing hematological conditions and assessing tumor marrow involvement for disease staging.
Nevertheless, systematic research validating this clinical shift remains scarce. Few studies have tracked the temporal evolution of bone marrow examination indications in people with HIV over an extended period (≥6 years) in the ART era. Comparative analyses between those with and without malignancies are even more limited. These gaps hinder the optimization of diagnostic strategies. Therefore, we conducted a retrospective analysis of people with HIV who underwent bone marrow examination at our center. Our aim was to characterize the evolving indications and final diagnoses and to enhance clinicians’ understanding of the changing disease spectrum in the ART era.
Population and Methods
Study design and population
We performed a retrospective analysis of individuals with HIV aged over 18 years who underwent bone marrow examination during hospitalization at Mengchao Hepatobiliary Hospital of Fujian Medical University, the largest designated HIV/AIDS care hospital in Fujian, China, from September 2019 to December 2025. All participants had confirmed HIV infection by the Centers for Disease Control and Prevention. Those with incomplete medical records were excluded.
Data collection and definition
Data were retrospectively collected from the electronic medical record system, including sex, age, date of admission, CD4+ T-cell count, CD8+ T-cell count, HIV RNA level, complete blood count parameters (white blood cell count [WBC], platelet count [PLT], hemoglobin [Hb], red blood cell count [RBC], absolute neutrophil count [ANC], absolute lymphocyte count [ALC], etc.), serum lactate dehydrogenase (LDH) level, bone marrow aspiration smear findings, and bone marrow biopsy pathology results. Decisions to perform bone marrow examinations were made by physicians based on clinical judgment. Common triggers included persistent unexplained cytopenia, FUO, or suspicion of hematological malignancy.
FUO was defined as a fever >38°C persisting for more than 3 weeks, with no identified cause after routine investigations. Cytopenia was defined as WBC < 4 × 109/L, Hb < 120 g/L (in males)/110 g/L (in females), or PLT < 100 × 109/L.
Laboratory methods
CD4+ and CD8+ T-cell counts were measured by flow cytometry. Peripheral blood parameters, including WBC, RBC, Hb, ANC, ALC, and PLT, were determined using an automated hematology analyzer. Plasma HIV RNA load was quantified by real-time quantitative PCR.
All individuals underwent bone marrow aspiration at the posterior superior iliac spine. Approximately 0.2–0.5 mL of bone marrow fluid was aspirated and rapidly smeared onto slides. Two to three thin smears containing visible bone marrow particles were selected for Wright-Giemsa staining. Smears were examined under low-power and oil-immersion lenses, and 200 nucleated cells were classified and counted. Cellularity was graded as markedly hypocellular, hypocellular, normocellular, hypercellular, or markedly hypercellular.
Bone marrow trephine biopsy was performed 0.5–1.0 cm adjacent to the aspiration site. A biopsy needle was used to obtain one to two specimens of approximately 1.0 cm in length. The specimen was fixed in 4% formaldehyde, embedded in paraffin, sectioned, and sequentially stained with hematoxylin and eosin, Giemsa, periodic acid-Schiff, and silver staining, and then examined by microscopy. For cases suspected of lymphoma involvement, immunohistochemical staining was performed using the following antibodies: CD3, CD5, CD10, CD20, CD19, CD79a, Ki-67, CD45, CD43, TdT, MPO, CD34, CD15, CD23, CD25, CD30, CD138, BCL6, BCL2, and cyclin D1, according to different types of lymphoma. All bone marrow smears and biopsy specimens were independently reviewed by two pathologists.
Statistical analysis
Data were analyzed using SPSS software. Categorical data are expressed as numbers (n) and percentages (%). Differences between groups were compared using Pearson’s chi-squared test. Continuous variables are presented as median (range), and the Mann–Whitney U test was used for the comparison between groups. Temporal trend analysis of bone marrow examination indications and diagnostic outcomes using the Cochran–Armitage test. A p value of < .05 was considered statistically significant.
Results
A total of 154 individuals with HIV who underwent bone marrow examination were included. Of these, 132 were male (median age: 49 years; range: 19–83) and 22 were female (median age: 52 years; range: 26–73). The median ratio of CD4+ to CD8+ T-cell counts was 0.18 (range: 0.01–4.13). Approximately 23.38% had been on ART for more than 6 months, and 29.87% achieved HIV RNA suppression (Table 1).
Baseline Characteristics in Individuals with HIV Undergoing Bone Marrow Examination
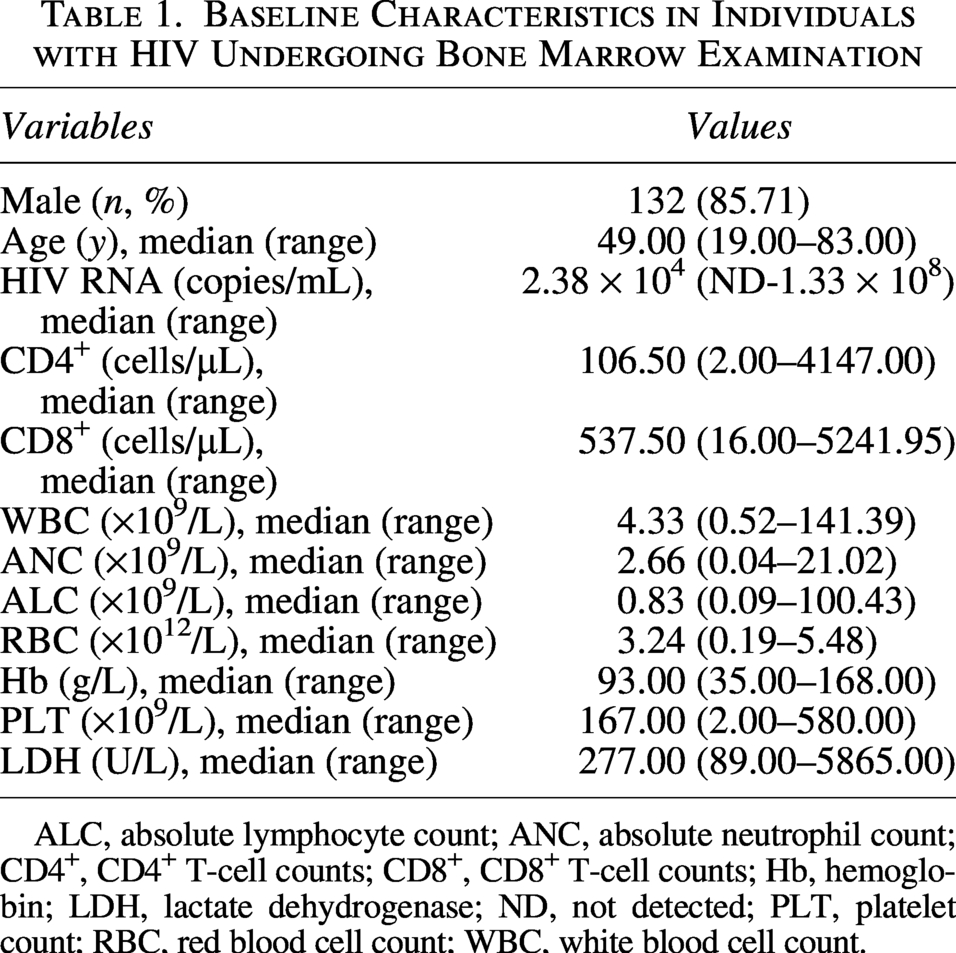
ALC, absolute lymphocyte count; ANC, absolute neutrophil count; CD4+, CD4+ T-cell counts; CD8+, CD8+ T-cell counts; Hb, hemoglobin; LDH, lactate dehydrogenase; ND, not detected; PLT, platelet count; RBC, red blood cell count; WBC, white blood cell count.
Among the 154 individuals, bone marrow examination was performed due to cytopenia in 57 cases (37.01%), FUO in 29 cases (18.83%), and for definitive diagnosis of suspected neoplastic hematological disorder or evaluation of marrow infiltration in confirmed hematological malignancies in 60 cases (38.96%). The remaining eight cases (5.19%) were attributed to other reasons (Table 2). The Cochran–Armitage trend test confirmed a significant decrease in the proportion of examinations performed for cytopenia (from 55.55% in 2019% to 17.86% in 2025, p = .002) and a significant increase in the proportion performed for suspected hematological malignancy (from 11.1% in 2019% to 60.7% in 2025, p = .002). In terms of cellularity, 81.17% exhibited normocellularity or higher, while 16.23% showed hypocellularity or lower (Table 3).
Analysis of Indications for Bone Marrow Examination
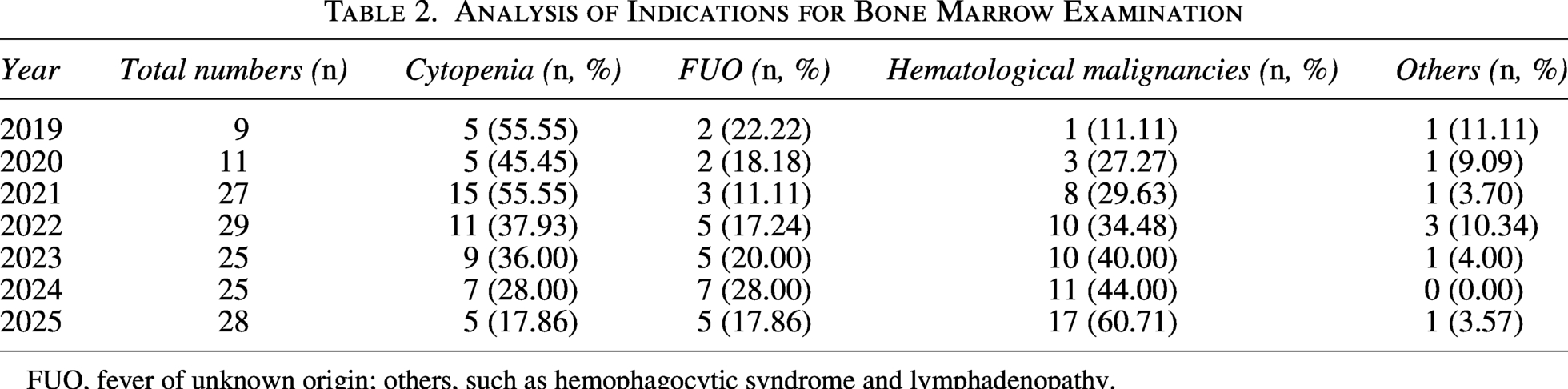
FUO, fever of unknown origin; others, such as hemophagocytic syndrome and lymphadenopathy.
Evaluation of Bone Marrow Hyperplasia Degree from 2019 to 2025 (n, %)

Others, puncture failure.
Ultimately, 58 individuals (37.66%) were diagnosed with malignant tumors, among which lymphoma was the most prevalent (44 cases), followed by leukemia (5 cases), Kaposi sarcoma (3 cases), and other malignancies (6 cases). Nonmalignant hematological diseases were identified in 27 individuals (17.53%), including megaloblastic anemia, autoimmune hemolytic anemia, aplastic anemia, primary immune thrombocytopenia, and secondary immune thrombocytopenia. Furthermore, 54 individuals (35.06%) were diagnosed with various opportunistic infections. The most common pathogens were Mycobacterium tuberculosis (21 cases) and Talaromyces marneffei (12 cases). In addition, 16 individuals (10.39%) had other conditions, such as immune reconstitution inflammatory syndrome and viral hepatitis-related cirrhosis. The Cochran–Armitage trend test revealed a significant shift over time: The proportion of opportunistic infections decreased significantly (from 33.33% in 2019% to 14.29% in 2025, p = .002), while the proportion of malignancies increased significantly (from 11.11%–53.57%, p = .002; Table 4).
Diagnostic Outcomes of Participants Undergoing Bone Marrow Examination
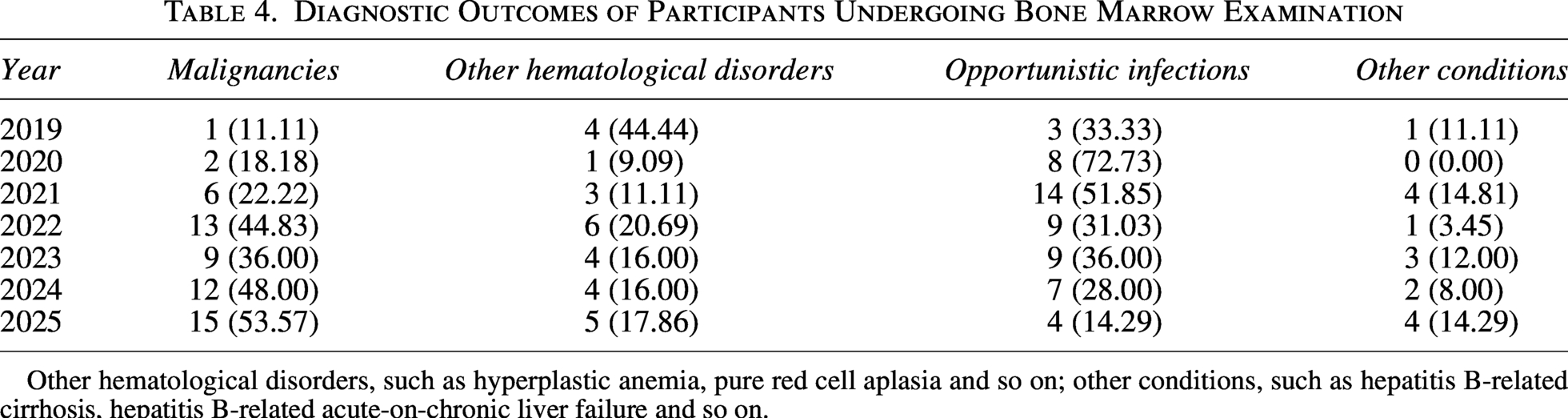
Other hematological disorders, such as hyperplastic anemia, pure red cell aplasia and so on; other conditions, such as hepatitis B-related cirrhosis, hepatitis B-related acute-on-chronic liver failure and so on.
The participants were divided into the tumor group (n = 58) and the nontumor group (n = 96). Compared with the nontumor group, those in the tumor group were older, had a higher proportion receiving ART, a higher HIV RNA undetectable rate, and significantly higher CD4+ T-cell count, CD8+ T-cell count, lymphocyte count, PLT, and LDH level. No significant differences were observed between the two groups in terms of sex, degree of bone marrow hyperplasia, WBC, ANC, Hb level, or red blood cell count (Table 5).
Comparison of Clinical Indicators in Tumor and Nontumor Groups
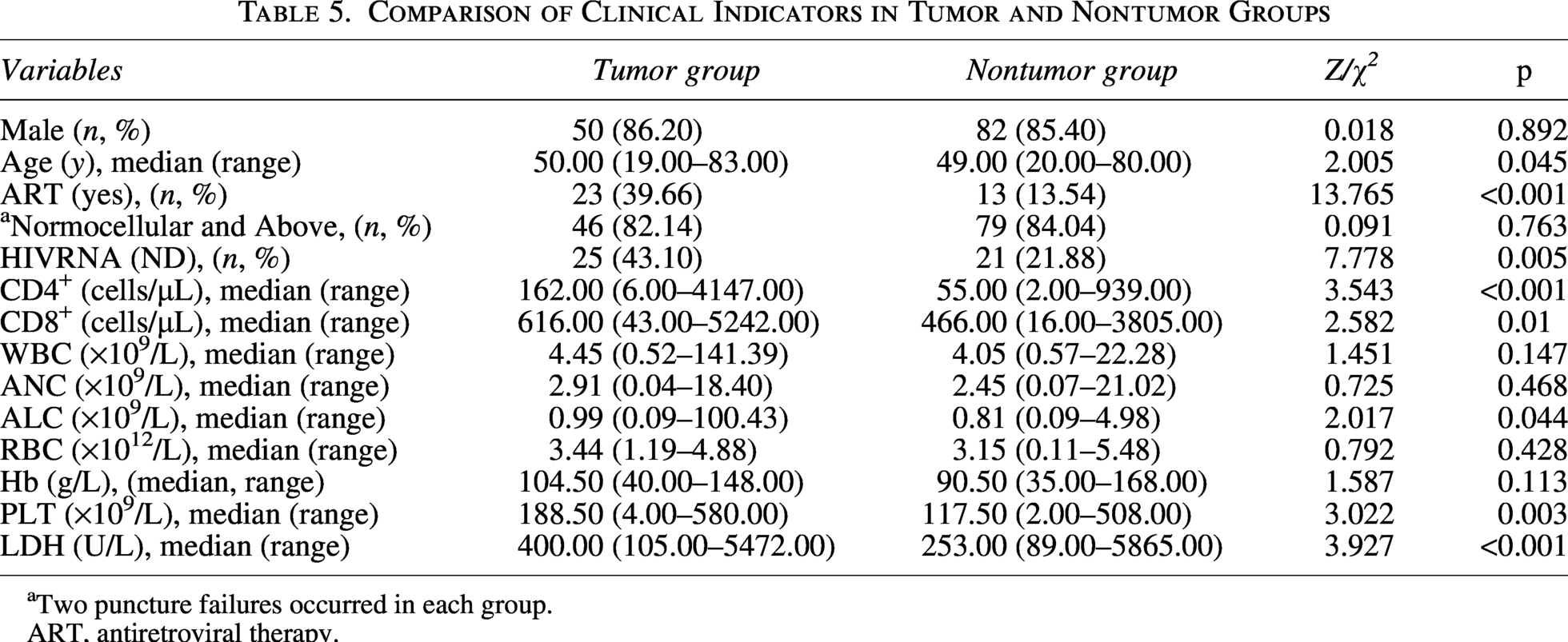
aTwo puncture failures occurred in each group.
ART, antiretroviral therapy.
Discussion
We conducted a retrospective analysis of 154 individuals with HIV who underwent bone marrow examination from September 2019 to December 2025. The results demonstrate a significant shift in the indications for bone marrow examination and the spectrum of final diagnoses against the backdrop of widespread ART. The primary indications for bone marrow examination have gradually shifted from traditional cytopenia and FUO to the diagnosis of suspected hematological malignancies and the assessment of tumor bone marrow infiltration. Correspondingly, the proportion of final diagnoses of malignant tumors has increased markedly, while the proportion of opportunistic infections has shown a declining trend. Notably, this observation is not unexpected and aligns with clinical knowledge in the ART era. Our study primarily serves to confirm and quantify these known epidemiological trends within our regional context, rather than to reveal a completely novel phenomenon. Nevertheless, this quantification provides a useful benchmark for clinical practice and highlights the ongoing shift in disease spectrum among people with HIV.
This study found that the proportion of bone marrow examinations performed for cytopenia decreased from 55.6% in 2019% to 17.86% in 2025, while the proportion performed for suspected hematological malignancy or tumor staging increased significantly from 11.1% to 60.71%. In parallel, the proportion of malignant tumor diagnoses rose from 11.1% to 53.6%. This trend aligns with multiple recent international observations. For instance, Xiong et al. noted that with the widespread use of ART, the proportion of infection-related causes of death among people with HIV has declined, while the proportion of non-AIDS-defining cancers (such as lung cancer and colorectal cancer) has increased. 9 Similarly, Chiao et al. reported that cancer incidence among people with HIV in the United States has increased, particularly for non-AIDS-defining cancers. 10 Wang et al. also indicated that with the prolonged survival of people with HIV, the number of participants with malignant tumors, especially hematolymphoid tumors, has been increasing as time goes on. 11 In a South African cohort, Abdullah et al. found that acute leukemia and lymphoma were the most common diagnoses among HIV-positive individuals undergoing bone marrow examination, while the diagnostic utility in individuals with isolated cytopenias was limited. 12 Similarly, Tshabalala et al. reported that hematological malignancies accounted for 50% of bone marrow biopsy diagnoses, with lymphoma being among the most frequent findings. 13 Our study further confirms that in clinical practice, the role of bone marrow examination is transitioning from an infection detection tool to a tumor diagnosis and staging tool.
This shift is the result of multiple interacting factors. First, the widespread use of ART has significantly reduced the incidence of opportunistic infections, making infection no longer the primary target of bone marrow examination. 5 Second, advances in pathogen detection technologies (e.g., metagenomic next-generation sequencing, high-sensitivity PCR) enable the diagnosis of many infections through less invasive methods such as blood or body fluid tests. Consequently, the reliance on invasive procedures such as bone marrow examination has reduced.14,15 Third, prolonged survival of individuals with HIV leads to the accumulation of age-related and immune-related cancer risks, making tumors increasingly prominent among this population.8,16 This study also found that the tumor group had significantly higher rates of ART use, HIV RNA suppression, and CD4+ T-cell counts compared with the nontumor group. The results are consistent with the findings by Borges et al. 17 Their research indicates that while those on effective ART have a lower risk of infections, their extended lifespan may be associated with a relative increase in the risk of certain tumors, particularly those related to immune activation or viral coinfections.
In this study, the tumor group showed higher CD4+ T-cell counts, CD8+ T-cell counts, lymphocyte, and PLTs. While these findings might seem contrary to the traditional understanding of immunosuppression promoting tumorigenesis, the underlying mechanisms remain unclear and warrant further investigation. In addition, the higher PLT in the tumor group may be related to certain hematological tumors (e.g., myeloproliferative neoplasms) or a tumor-associated inflammatory state. The significantly elevated LDH level in the tumor group is associated with high tumor burden and rapid cell turnover, serving as a common prognostic marker for malignancies such as lymphoma.
Unlike most international studies, which focus on AIDS-related lymphomas or specific tumor types, this study systematically describes the overall transition in the indications and diagnostic spectrum of bone marrow examination. It covers a broad range from infections to tumors and provides multiyear trend data. Similar domestic studies often concentrate on specific time periods or indications. In contrast, this study spans a longer period (2019–2025) and offers a clearer depiction of the dynamic evolution in the ART era. Furthermore, by comparing the clinical characteristics of the tumor and nontumor groups, this study provides new insights for understanding the immunological and hematological profiles of people with HIV with comorbid malignancies.
This study has several limitations. First, it is a single-center retrospective study from Southeast China. Tumor type distribution, especially the high proportion of lymphomas, may reflect local epidemiology such as EBV and HHV-8 prevalence. Our results may not apply to other populations with different ethnicities, ART coverage, or cancer patterns. Second, we only included people who actually had a bone marrow examination. This is a selected subgroup of people with HIV. We had no reference population, such as all hospitalized people with HIV or all individuals with cytopenia or FUO. Therefore, we cannot fully separate real changes in disease spectrum from changes in clinical practice, such as lower or higher thresholds for bone marrow testing. This limits our interpretation. Third, even with trend analysis, annual sample sizes were small and unbalanced. This may reduce statistical reliability.
Third, despite the use of trend testing, the yearly sample sizes are relatively small and uneven, which may affect statistical robustness. Fourth, bone marrow examination decisions were based on clinician judgment, not a standardized protocol. This may introduce variability in the indications. Fifth, we lack long-term follow-up data. So we cannot assess how bone marrow findings affect later health outcomes.
Clinical implications: Our findings suggest that in the ART era, clinicians should consider malignancy early in people with HIV presenting with cytopenia or FUO, especially lymphoma. Bone marrow examination remains useful. It should be used strategically, particularly when routine infection workup is negative and hematological disease or cancer is suspected.
Conclusion
In the current ART era, bone marrow examination in people with HIV has shifted from diagnosing opportunistic infections toward detecting and staging hematological and solid malignancies. This reflects improved viral control, prolonged survival, and rising cancer incidence in this population. Our findings underscore the evolving disease spectrum among people with HIV and highlight the growing importance of malignancy screening and evaluation in the long-term management of these individuals.
Authors’ Contributions
J.L.: Study design, data collation, statistical analysis, and article drafting. Y.C.: Study design, data verification, and article revision.
Ethical Considerations
The study was approved by the Medical Ethics Committee of Mengchao Hepatobiliary Hospital of Fujian Medical University (approval number: 2026-010-01).
Consent to Participate
Existing clinical information and laboratory data were anonymized and extracted from electronic medical records; thus, the requirement for written informed consent was waived.
Consent for Publication
Neither the entire paper nor any part of its content has been published elsewhere. While the article is undergoing the peer review phase, we will not submit the article to another journal without notifying the editor. If accepted, the paper will not be published elsewhere. The article has been read and approved by all the authors.
Footnotes
Acknowledgments
The authors thank all participants in this study.
Author Disclosure Statement
There are no conflicts of interest to disclose.
Funding Information
This study was funded by grants from the