
Abstract
Purpose:
To evaluate an intervention promoting adoption of occupational sun protection policies by employers in a randomized trial.
Design:
A randomized pretest–posttest controlled design with 2-year follow-up was conducted in 2010 to 2013.
Setting:
Local government organizations in Colorado who had outdoor workers in public works, public safety, and/or parks and recreation.
Participants:
Ninety-eight local government organizations (n = 51 municipalities, 10 counties, and 37 special districts).
Intervention:
Organizations were randomly assigned to receive a policy and education intervention comprised of personal contacts and theory-based training and materials or to an attention control group.
Measures:
Occupational policy documents were coded for sun safety content by a trained research assistant blind to condition.
Analysis:
Policy scores were analyzed with logistic and Poisson regression models using imputation.
Results:
At posttest, more organizations in the intervention group had a sun protection policy than in the control group (odds ratio [OR] = 4.91, P < .05; intent to treat: OR = 5.95, P < .05) and policies were more extensive (χ2 = 31.29, P < .01; intent to treat: χ2 =73.79, P < .01) and stronger (χ2 = 24.50, P < .01; intent to treat: χ2 = 51.95, P < .01). Policy adoption was higher when the number of contacts and trainings increased (P < .05).
Conclusion:
The intervention had a large effect on adoption of formal sun protection policies, perhaps because of its fit with legal requirements to maintain safe workplaces. Personal contacts with managers were influential on adoption of occupational policy even in this age of communication technology and social media.
Purpose
The workplace is a promising venue for programs to prevent chronic disease and acute injury. While health education promoting individual behaviors has been successful in worksite wellness, 1 so have changes in workplace policies that can significantly impact safety, 2,3 disease management, 4 and disease prevention. 5 Most workplace interventions have focused on prevention education, 6 but fewer have used the combination of education and policy, even though such approaches have achieved long-term well-being 4,6 (eg, reductions in blood pressure and cholesterol levels, 7 chemical dependence, 8 hospital visits, and the need for mental health services 9 ). Policies can clarify personal and organizational responsibilities, formally direct employees to take precautions, and overcome workers’ low perceived risk, personal preferences, and other barriers to practicing prevention.
Skin cancer is among the most common cancer worldwide. The World Health Organization estimates that up to 3 million cases of nonmelanoma skin cancers (NMSCs) and approximately 132 000 cases of melanoma are diagnosed annually. 10 Outdoor workers are exposed over many years to high levels of solar ultraviolet (UV) radiation 11 and are at risk for skin cancer, 12 especially NMSC. An elevated risk of melanoma with outdoor occupations has also been observed, 12,13 and melanoma mortality produced US$66.9 billion in productivity losses from 1990 to 2008 in the United States. 14 The NMSC prevention is a priority due to its high prevalence, 15 recurrence, and treatment and lost productivity costs. 16
Sun safety aligns with workplace initiatives to prevent injury, improve well-being, and address concerns over heat stress and climate change. 17 Sun protection should be promoted at work because many outdoor workers fail to practice sun safety. 11,18,19 Studies have shown that workplace education can improve workers’ sun protection. 20 –26 A comprehensive approach that motivates employers to adopt policies for routine sun safety training, to enact environmental controls and administrative procedures, and to place sun safety on organizational and individual agendas may reduce exposure to UV and skin cancer more than education alone. However, few employers currently have sun safety policies, and these policies mainly promote personal protection, rarely address environmental controls or administrative procedures, and usually only encourage personal protection but not require it (requiring protection has improved workers’ sun safety 18,27 ). In a survey in the United States, sun protection policies increased lifeguards’ sun protection habits and decreased their sunburning, 25 but a study in New Zealand found no effect of policy on outdoor workers’ sun protection. 28 Only 1 investigation, an intervention in 3 units within an Israeli water company, has examined education and policy (free sunscreen and obligatory use of sun protection gear) together. 29
In this article, policy-focused results of a randomized field trial evaluating an intervention that promoted adoption of sun safety policy by employers and provided education to employees are presented. It was hypothesized that employers who received the combined workplace policy and personal protection education intervention would adopt more occupational sun safety policies than employers in an attention control condition (ie, basic sun safety communication only).
Methods
Design
The experimental design consisted of a randomized pretest–posttest controlled trial. Local government organizations were recruited over 6 months (March to August 2011). Copies of policy documents were obtained by e-mail or by visiting nonresponding organizations. Senior managers completed a baseline survey either online or by mail, after reading and acknowledging an informed consent statement. Each month during the recruitment period, local government organizations completing pretesting were randomized to either the Sun Safe Workplaces (SSW) intervention or an attention control condition (ie, basic sun safety communication) by the project biostatistician using a customized computer program. The program drew a random number from the uniform distribution in SAS, and if the number was less than 0.05, the organization was assigned to the control group, thereby ensuring that the next organization would be assigned to the intervention group to balance the number of controls and intervention organizations over time. The intervention was conducted over a 2-year period. At the conclusion of the intervention, project staff collected the most current policy documents by e-mail or in person; the senior managers who completed the baseline survey (or their replacement if they had left the position or employer) were surveyed online or by mail. Policy documents were coded for content related to sun safety by trained research assistants blind to condition. All protocols were approved by the Western Institutional Review Board and Colorado Multiple Institutional Review Board.
Sample
A sample of 98 local government organizations in Colorado, that is, municipalities, counties, and special districts (public organizations providing water, sanitation, parks and recreation, and fire protection), were recruited in 2011 by project staff who contacted the senior most manager (eg, city or county manager or district executive director) who consented for the organization to participate. Sample size was set a priori to achieve statistical power of 80% for a difference of 21% in organizations with an extensive policy. The primary eligibility requirement was being a local government organization with employees who worked outdoors in at least one of the following service areas—public works, public safety, and parks and recreation. Additionally, organizations had to provide copies of documents containing formal written policies on employee safety and have 5 or more senior managers complete a baseline survey. Results pertaining to adoption of worksite policy are reported here; the recruitment and senior managers’ characteristics have been reported elsewhere. 30
Measures
Policy measures
Project staff worked with the contact managers to obtain copies of written policy documents pertaining to employee safety (ie, safety and risk management manuals, employee handbooks, standard operating procedures, personnel manuals, safety binders, administrative and training policies, safety compliance guidelines and policies, and procedure manuals). The policy coding protocol 31 was modified from procedures used by the first author to measure sun protection policies in public school districts. 32 It covered 15 “content categories” in 3 domains—(1) environmental controls (provision of shade, schedule of outdoor work), (2) administrative procedures (risk assessment, training of employees and of managers/supervisors, policy review/monitoring, resource allocation, communication with clients/patrons, compliance by contractors/subcontractors, and posting of UV index), and (3) personal protection practices (use of UV-protective clothing [including long-sleeved shirt and long pants/skirt], hats, protective eyewear, and sunscreen [including sunscreen lip balm], and regular skin cancer screening [self-examination or clinical examination]). For each policy category, research assistants recorded the presence (0 = not addressed, 1 = addressed), strength (−1 = not allowed, 0 = not specified, 1 = allow/recommend, 2 = require), and intent (0 = indirectly addresses sun protection, 1 = directly addresses sun safety) of the policy; responsibility for policy implementation (0 = not specified, 1 = employee, 2 = employer); and date adopted/revised. Additionally, specific “directives” within certain policies were recorded to assess best-practice sun safety as recommended by the Centers for Disease Control and Prevention and the National Institute on Occupational Safety and Health 33,34 (ie, work schedules that avoided midday hours outdoors [or not]; supervisor delivered sun safety training [or self-directed training]; sunscreen with SPF 15 or higher [or not]; wide-brimmed hat [or any brim or no length specified]; long sleeves and long pants [or any sleeves/pants or length not specified]; UV-protective eyewear [or not]; clinical skin examination [or self-examination]; and interval of examination [annual, monthly, any interval, no interval specified]). Research assistants, blind to condition, were trained to use the coding protocol. They first practiced on policies from organizations not in the project until they had intercoder reliabilities of 0.70 or higher. Research assistants independently coded policies, but to avoid coder drift, they coded a group of policies together at the outset, at the midway, and at the end and resolved disagreements. This maintained high intercoder reliability (r = 0.52-1.00 at posttest), except for the employee/supervisor training category (r ≤ 0.30; disagreements were resolved by discussion among coders).
Policy implementation measures
At posttest, managers reported on policy implementation, along with job and demographic characteristics and attitudes toward workplace health and sun safety policy. They indicated if they were aware of a formal written sun protection policy (yes, no/don’t know), how well managers/employees were following the policy (1 = very poorly, 5 = very well), and whether the organization provided employees with sun protection equipment (ie, sunscreen, wide-brimmed hats, sunglasses, long-sleeved shirts, long pants, or outdoor shade) or adjusted work schedules to reduce employees’ time outdoors at midday (yes, not/don’t know). Managers rated their frequency of wearing sunscreen with SPF 15+, protective clothing, hats with any brim or wide brim, or sunglasses; limiting time in the midday sun; or staying mostly in the shade when outdoors at work (1 = never, 5 = always).
Intervention
Sun Safe Workplaces intervention
The SSW promoted adoption of workplace sun safety policies and provided training in personal sun protection for outdoor workers. It operationalized principles from diffusion of innovations theory (DIT) 35 and 2 relationship development models—social penetration theory 36 and stages of relational development. 37 Based on DIT, the intervention aimed to convince senior managers to adopt sun safety policies and agree to the sun safety training by increasing the perceived need for workplace sun safety and fit of policy/education with workplaces’ safety mission/procedures, helping them plan for policy implementation and education, and identifying ways to alter the policies/education and/or the workplace to improve fit and to clarify such changes to other managers and employees. 38 Project staff worked as outside change agents and “bundled” occupational sun protection with worksite safety goals (eg, hydration and personal protection equipment). 38 Based on the relationship theories, project staff maintained open channels of communication and developed relationships with the managers and engaged in involved communication about policies and education on worksite sun safety. In face-to-face meetings with managers, project staff worked to reduce their uncertainty 39 about sun safety, highlight occupational sun safety advice from national health authorities (eg, CDC and NIOSH) to build credibility/trust, and obtain public commitment to adopt and implement policies/education. 40
The intervention began by sending a Program Announcement Packet to the contact manager at each workplace (ie, manager tasked with working with project staff) and requesting the first face-to-face meeting. At the first meeting, project staff covered: (1) introduction to SSW, (2) sun safety practices in the workplace, (3) sun safety policy for outdoor workers, (4) sun safety policy adoption, and (5) sun safety policy reinforcement and maintenance. They also presented the SSW website, which described skin cancer and UV, risk factors, personal risk assessment, and workplace prevention strategies (ie, sunscreen, sunglasses, hats, shade, scheduling, and clothing). The website also contained a sun safety toolbox with a worksite audit, policy-writing tool, and fact sheets on sun safety and barriers to policy implementation. Following the first meeting, the contact manager scheduled sun safety training by project staff with various employee groups. The training fit into workplace safety/wellness and covered (1) the US skin cancer problem; (2) the sun, UV rays, and skin cancer; (3) assessing personal risk; and (4) practicing sun safety and obtaining regular skin examinations. Workplace sun safety materials based on DIT principles were sent in 4 sets (twice a year over 2 years) to the contact manager for distribution to employees, including 10 posters, 6 tip cards, a sticker, a sunscreen discount coupon, and a CD on total skin self-examination. In monthly follow-up contacts, project staff nourished their relationships with managers, supported managers’ decisions to write policies and train employees, and problem-solved barriers such as working through policy approcal processes.
Attention control intervention
Project staff sent printed materials on occupational sun safety to local government organizations in the attention control condition (1 package per year). These included posters with personal protection messages and skin cancer incidence rates, risk assessment brochures, worksite guides, total skin self-examination CD, the American Academy of Dermatology SPOT bookmark showing the ABCDEs of melanoma and skin self-examination, and a sun safety tip card from OSHA. Project staff made presentations on general sun safety topics (not policy) at state professional conferences that may have been attended by control and intervention organizations.
Analysis
Three policy measures were analyzed. First, presence of an occupational sun protection policy (or not) was indicated by an organization having any content category present. Policy categories had to be coded as having direct sun protection intent to be considered present. Extent of policy was the sum of the number of content categories in the organizations’ policy (total possible extent score = 0 to 15). Strength of policy was measured by summing the strength scores for each category (possible range = −15 to 30). Two versions of these 3 measures were created—general policy scores and best-practice policy scores. The latter was created by applying the directives to create conservative versions of the policy measure that conformed to best-practice sun safety (ie, work schedule avoids midday hours outdoors, sunscreen with SPF 15 or higher, wide-brimmed hat, long sleeves and long pants, UV-protective eyewear, clinical skin examination at annual intervals). An analysis of the sun safety policies at baseline was published previously. 31
Policy scores were analyzed with generalized linear models using SAS 9.3, with α set at .05 (2-tailed). The biostatistician was not blind to random assignment; however, analyses were done by using codes for this assignment to keep it from being known for any individual organization and performed by a data analyst remote from the biostatistician (the biostatistician provided direction on data analysis techniques). For the dichotomous presence score, a Firth logistic regression was used to produce penalized maximum likelihood estimation because the pre–post increases were all from the intervention organizations. For the ordinal extent of policy score and strength of policy score, Poisson regression models were conducted. Analyses were initially adjusted only for baseline values of the policy score. Next, analyses were adjusted for covariates using stepwise selection selected from characteristics of the local government organizations (see Table 1) that included cosmopoliteness (ie, connectedness or worldliness, operationalized as distance from the urban Front Range 35 ), party affiliation based on county voting records for 2010 Gubernatorial election and 2008 and 2010 Senatorial election, the type of government organization, the percentage of senior managers, household income, the percentage of bachelor’s degrees by county, number of employees, and national and local political culture regions (national: individualist, traditionalist, moralist 41 ; local: Denver metro, other Front Range, Eastern Colorado, Western and Southern Colorado 42 ). Covariates meeting the criterial of P < .15 were retained in each model. Analyses accounted for nonresponse to follow-up in 3 ways—intent to treat (n = 98; all organizations included, assuming no change for nonresponders, ie, baseline value imputed for missing posttest), responder (n = 84; organizations providing policy documents or stating that no changes had occurred at posttest, ie, baseline value assigned for “no changes” posttest), and completer (n = 46; all organizations providing policy documents at posttest) samples.
Comparison of Policy Scores and Characteristics of the Local Government Organizations Sample at Baseline Between Experimental Condition and by Posttest Response Status.
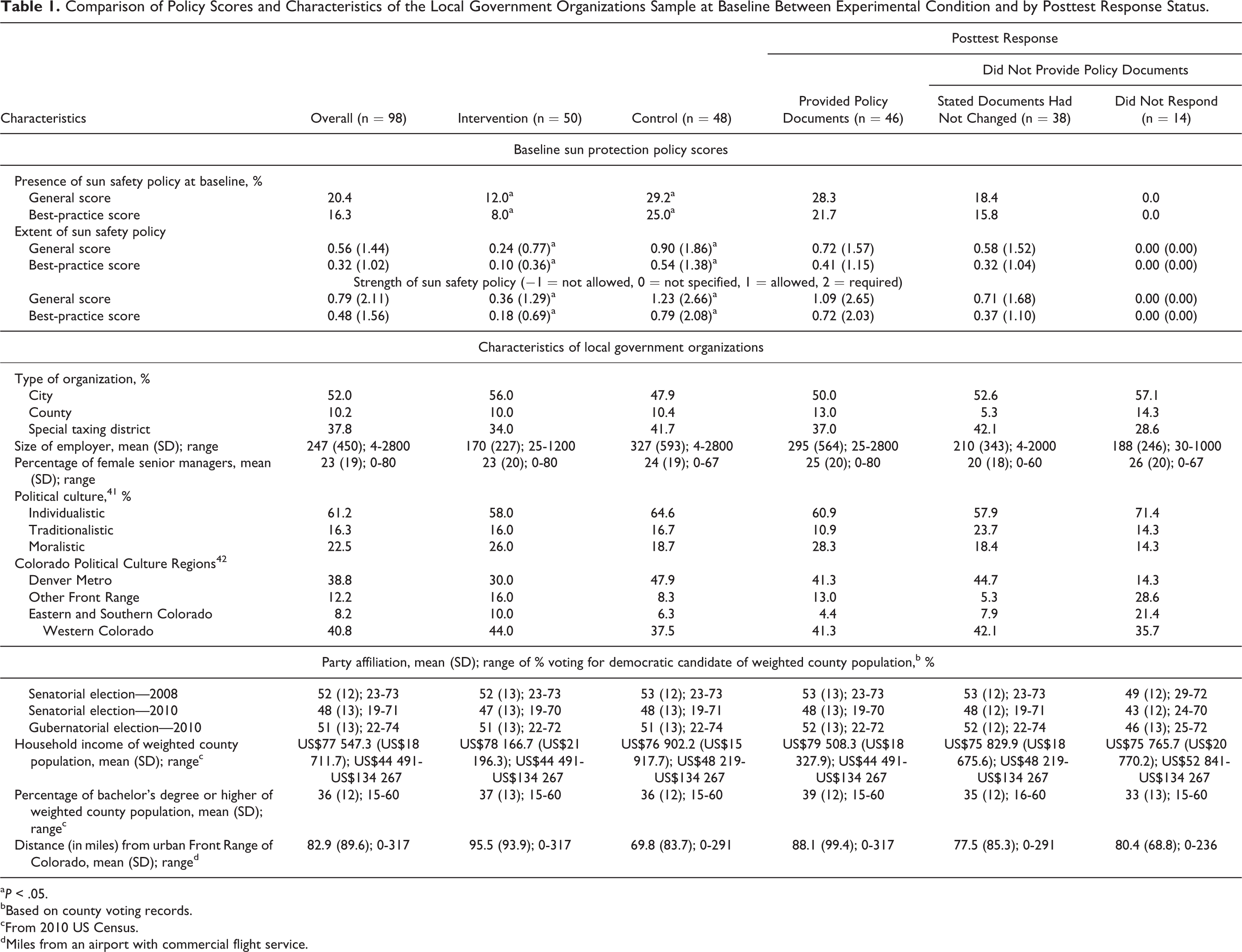
aP < .05.
bBased on county voting records.
cFrom 2010 US Census.
dMiles from an airport with commercial flight service.
Results
Profile of the Local Government Organizations and Senior Managers
The sample contained 98 local government organizations (n = 51 municipalities, 10 counties, and 37 special districts). Five hundred seventy-one organizations were invited; of which 385 were determined to be eligible, 137 (36% of eligible) agreed to participate (30% actively refused and 34% did not respond), and 98 (26% of eligible) provided the required policy documents and baseline surveys to be enrolled (see CONSORT diagram in Figure 1). Table 1 presents the characteristics of the sample. Randomization successfully balanced the organizational characteristics (Table 1), but at baseline, organizations assigned to the control condition had more sun protection policies (and more extensive and stronger policies) than organizations assigned to the intervention group. At posttest, 46 (47%) of the 98 organizations submitted copies of written policy documents. Another 38 (39%) reported that they had not changed any policies since baseline and declined to submit new copies. Only 14 (14%) organizations did not respond at posttest. Policies were subsequently obtained from 2 organizations that reported no change and coding confirmed that no changes existed.
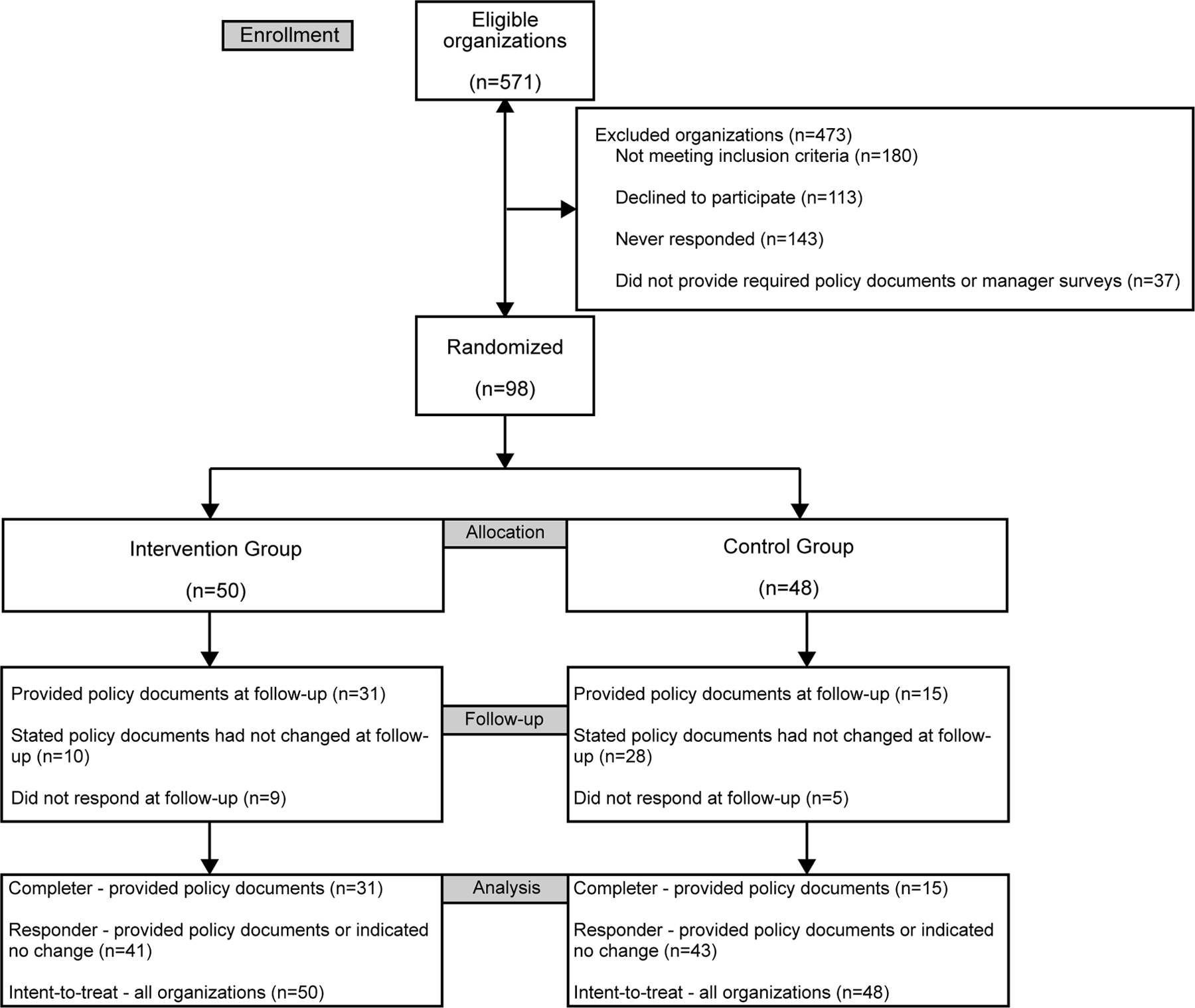
CONSORT Diagram on Participants for Randomized Trial.
Also, 523 senior managers completed the posttest and reported on policy implementation. They averaged 14.0 years (standard deviation [SD] = 10.3) working for the organization; 96% were involved at least some of the time in making decisions about workplace policy, procedures, and training related to the safety and health of employees; and 51% worked at least part of the time outdoors. The mean age of managers was 47.2 years (SD = 9.6); 10% had a high school education, 34% had education beyond college, and 56% had 4-year college or postgraduate degree; 4% were Hispanic and 2% were nonwhite; and 24% were female. Additionally, 32% had skin types that sunburned easily and 13% had been diagnosed with skin cancer.
Implementation of the SSW Intervention
Project staff met with 46 (92%) of the 50 local government organizations in the intervention group and performed the SSW policy intervention (n = 1673 e-mail, 182 phone, 162 in-person, and 114 mail contacts). Project staff conducted the in-person sun safety training at 40 intervention organizations (80%; mean = 2 trainings per organization). Managers at 4 organizations did not respond to requests to meet with project staff and those at 6 additional organizations declined to schedule the sun safety training. Thus, 40 organizations received the policy intervention and sun safety training, 6 received the policy intervention only, and 4 received neither. In the attention control condition, project staff mailed printed materials to all organizations and made presentations to 9 professional associations (eg, American Public Works Association—Colorado Chapter, Special Districts Association of Colorado, Colorado Parks and Recreation Association) during the intervention period.
Differences in Sun Protection Policy at Posttest by Experimental Group
At posttest, more organizations in the intervention group had a sun protection policy than in the control group (Table 2). Looking first at the general policy scores among the 46 completers (ie, organizations providing policy documents at posttest), more intervention organizations than controls had any sun safety policy and policies were more extensive and stronger (Table 2). This same positive intervention effect emerged in the analysis of the 84 responding organizations (ie, those who either provided their policy or reported no change at posttest) and the intent-to-treat analyses with all 98 organizations (Table 2). Likewise, when looking at the best-practice policies, more intervention organizations had any sun protection policy and their policies were more extensive and stronger than control organizations (Table 2).
Results of Statistical Comparison of Occupational Sun Protection Policy Scores Between Experimental Conditions at Follow-Up.
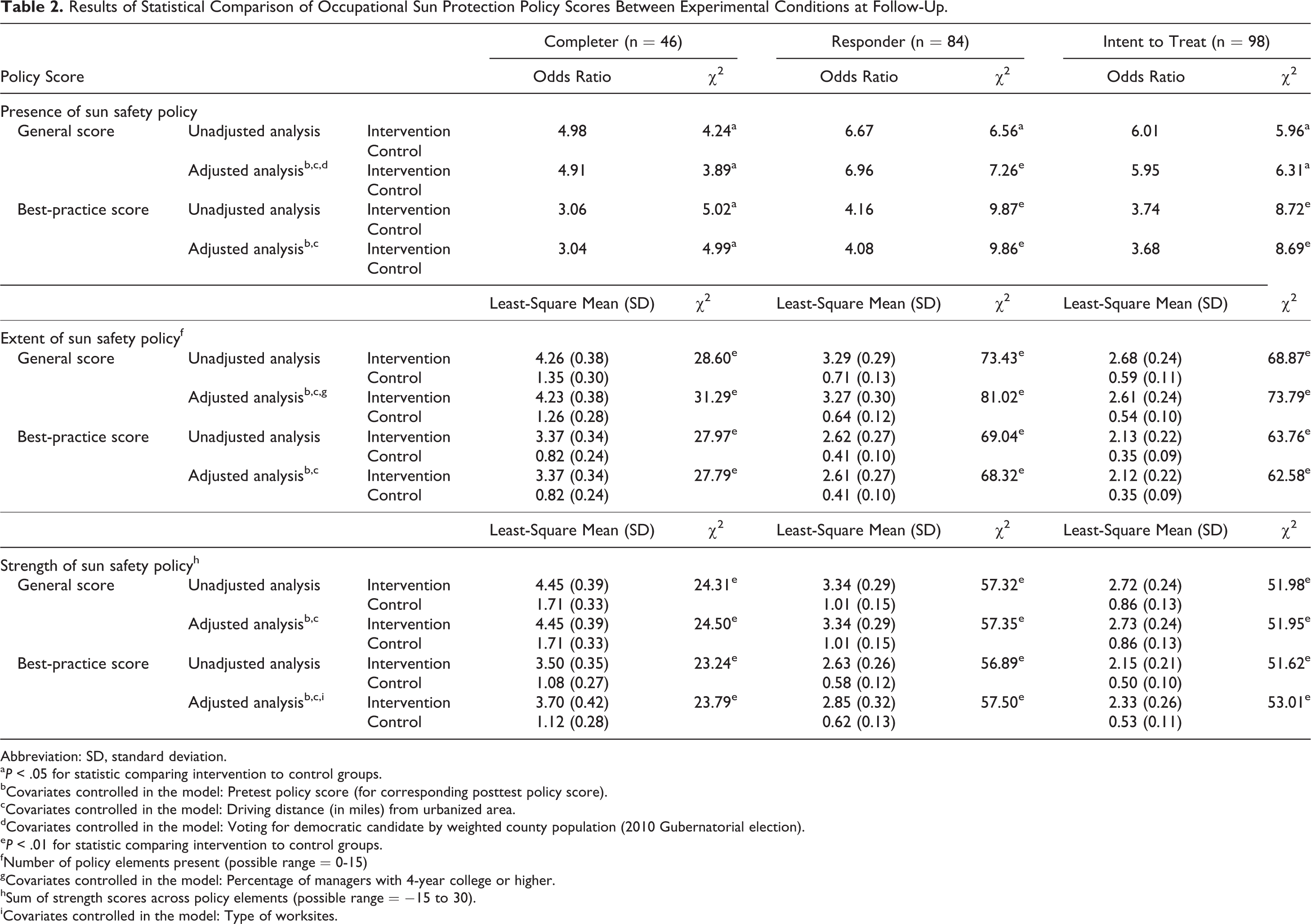
Abbreviation: SD, standard deviation.
aP < .05 for statistic comparing intervention to control groups.
bCovariates controlled in the model: Pretest policy score (for corresponding posttest policy score).
cCovariates controlled in the model: Driving distance (in miles) from urbanized area.
dCovariates controlled in the model: Voting for democratic candidate by weighted county population (2010 Gubernatorial election).
eP < .01 for statistic comparing intervention to control groups.
fNumber of policy elements present (possible range = 0-15)
gCovariates controlled in the model: Percentage of managers with 4-year college or higher.
hSum of strength scores across policy elements (possible range = −15 to 30).
iCovariates controlled in the model: Type of worksites.
Differences in Policy Implementation by Experimental Group
There was some evidence that the intervention increased implementation of personal protection policy with employees and senior managers. Compared to control organizations, more managers at intervention organizations were aware that there was a formal written sun protection policy (control = 33.7%, intervention = 58.1%, F = 8.44, P < .01 adjusted for pretest, awareness of other organizations with sun protection policies, and gender), reported that their organization provided wide-brimmed hats to employees free or at reduced costs (control = 33.5%, intervention = 48.0%, F = 4.37, P < .05 adjusted for pretest, years working for organization, age, and gender), and said they more frequently wore protective clothing (ie, long-sleeved shirts and long pants) when working outdoors in the sun (control M = 3.08, intervention M = 3.34, F = 10.06, P < .01 adjusted for pretest, belief that taxes should be kept low rather than provide additional services, age, skin type, gender, and tanning image). However, there were no differences between the intervention and control conditions in managers’ perceptions of how well the formal policies were being implemented.
Relationship of Intervention Intensity and Policy Adoption
Table 3 shows that greater intervention intensity, measured by the number of contacts with senior managers and number of sun safety trainings for employees by project staff, was associated with adoption of more extensive and stronger occupational sun protection policies in the intervention organizations. These relationships emerged in the completer and intent-to-treat analyses.
Relationship Between Occupational Sun Protection Policy Scores and Number of Contacts With Senior Managers and Number of Sun Safety Trainings at Intervention Organizations.
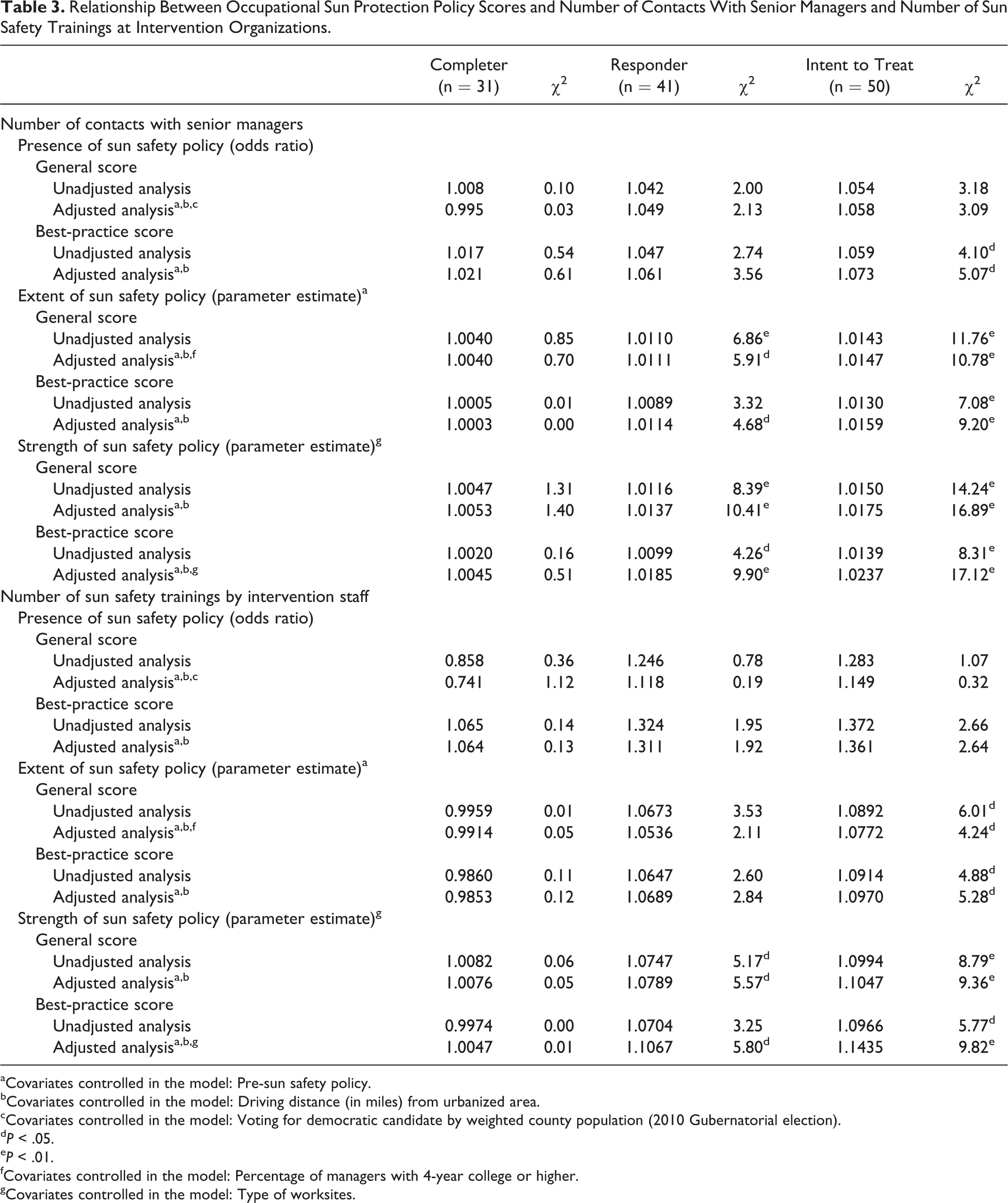
aCovariates controlled in the model: Pre-sun safety policy.
bCovariates controlled in the model: Driving distance (in miles) from urbanized area.
cCovariates controlled in the model: Voting for democratic candidate by weighted county population (2010 Gubernatorial election).
dP < .05.
eP < .01.
fCovariates controlled in the model: Percentage of managers with 4-year college or higher.
gCovariates controlled in the model: Type of worksites.
Discussion
The SSW intervention showed considerable success at convincing managers at local government organizations to adopt formal written sun protection policies and deliver sun protection training to employees. The effect on policy adoption was very robust, emerging in conservative intent-to-treat analyses and measures of best-practice policies. Effecting policy changes is highly desirable because they signal a strong organizational commitment to sun safety, direct all employees to take precautions, and may result in workplace resources being devoted to sun safety (eg, providing employees with low or no cost wide-brimmed hats). Policy also carries permanence and may combat the degradation of effects owing to management turnover witnessed in a previous study. 43
Education in personal sun protection of employees was popular, with 80% of organizations scheduling the in-person sun safety training. Education may shift responsibility for sun safety to the employee and avoid the need for managers to allocate workplace resources to sun safety (eg, building shade structures). The intervention occurred in 2011 to 2013, following an economic recession which may have compounded reluctance to make changes that required resources. Still, some workplaces adopted policy and educated employees, but concerns over resources also may underlie the choice of several workplaces to “encourage” but not “require” sun safety in written policies (ie, low policy strength).
Adoption rates for policies among the local government organizations were far higher in this study than in a project that promoted sun protection policies for students to public school districts, 44 but the proportion delivering education was only slightly higher than witnessed in the private North American ski industry. 45 The legal requirements to maintain a safe workplace may motivate managers to take steps to mitigate the risk posed by solar UV. By contrast, school district administrators may feel that student sun safety is not mandatory, given they are only outdoors part of the time. Many of the employers were already taking steps to reduce workplace risks (eg, hard hats and safety glasses,), so sun protection may have better fit in work environments than schools. Workplaces may be a fruitful community avenue for improving skin cancer prevention.
The benefits of workplace sun safety policy and education will only be realized if managers implement the policies and employees practice adequate protection. Evidence of this is provided by equipment changes, that is, managers at the intervention workplaces reported providing wide-brimmed hats to employees. Such hats can protect the face and neck from UV exposure and reduce skin cancer risk. 46 It may take more time, resources, and possibly external support to help managers broadly implement policy. Some categories may be easier or less expensive to implement (eg, hats) than others (eg, shade and adjusting work schedules).
Limitations
There are limitations to consider. The trial was conducted in a western, high-altitude state where UV can be high, which may have increased relevance of sun safety. The findings may generalize best to other local government organizations, which, compared to private employers, do not have a profit motive and may place a premium on employee benefits. However, US employers, public and private, legally must provide a safe workplace. We earlier demonstrated that a large private outdoor recreation industry was willing to widely adopt sun safety education. 45 The SSW program has the potential to be effective with private and public employers. Actions taken to implement policies were self-reported by managers, which is open to demand and social desirability biases, but the policy scores were based on objective coding of actual written documents, not subject to these biases. The failure of some organizations to provide copies of these documents at posttest may have caused us to miss some policy change, although SSW’s effect emerged in conservative intent-to-treat analyses.
Conclusion
The US Surgeon General has identified occupational sun protection as a priority in community-based skin cancer prevention efforts. 16 Policy may elevate the priority and sustainability of occupational sun safety for both employers and employees. It is also possible that convincing workplaces to take actions on skin cancer prevention may influence other organizations and individuals in their communities to do so as well. Personal contacts with managers and in-person training were especially influential on adoption of sun protection policies. Many prevention interventions have been guided by theoretical frameworks applied to how messages should be designed to persuade the at-risk population. 47,48 However, DIT 35 and the 2 relationship theories, that is, social penetration theory 36 and stages of relational development, 37 suggested that the messenger and the message are important. Spending time working with managers, educating employees in person, keeping lines of communication open, and nourishing these relationships may be very important for achieving organizational change, even in this age of communication technology and social media. Recent research suggests that individuals are supported and persuaded most by those with whom they have off-line interpersonal contact. 49
SO WHAT? Implications for Health Promotion Practitioners and Researchers
What is already known on this topic?
The large population of outdoor workers is exposed over many years to high levels of solar ultraviolet radiation and is at risk for skin cancer. Most workplace interventions have focused on prevention education, including efforts to improve personal sun protection behavior by employees. However, fewer interventions have aimed to convince managers to adopt formal workplace policies, in this case that alter workplace environments and administrative procedures and promote personal protection for workers.
What does the article add?
The article reports the results of an evaluation of an intervention using personal contact and print/online materials intended to increase adoption of occupational sun protection policies by public employers in a randomized controlled trial. At posttest, more employers receiving the intervention had formal occupational sun protection policies, and these policies were more extensive and stronger than among employers in the control condition. Policies were more extensive and stronger when intervention staff had more contact with managers and delivered more sun safety trainings.
What are the implications for health promotion practice or research?
Policies on sun protection can be successfully promoted through personal contacts with worksite managers and in-person training of employers, based on principles of the diffusion of innovations theory. Adoption of occupational sun protection policies is a national goal in the US Surgeon General’s Call to Action to Prevent Skin Cancer in 2014, because they should increase the priority and sustainability of sun protection and reduction in skin cancer among the outdoor workforce.
Footnotes
Authors’ Note
Trial Registration: ![]() identifier—NCT021824289. The design, data collection, analysis and interpretation of the data, and preparation of and decision to submit this manuscript were solely the responsibility of the authors; the National Cancer Institute had no involvement in these aspects of the project.
identifier—NCT021824289. The design, data collection, analysis and interpretation of the data, and preparation of and decision to submit this manuscript were solely the responsibility of the authors; the National Cancer Institute had no involvement in these aspects of the project.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by a grant from the National Cancer Institute at the National Institutes of Health (CA134705). Dr Buller reports grants from National Institutes of Health, National Cancer Institute during the conduct of the study and salary from Klein Buendel, Inc. Dr Walkosz reports grants from National Institutes of Health, National Cancer Institute during the conduct of the study and salary from Klein Buendel, Inc. Ms Buller is an owner of Klein Buendel, Inc and reports grants from National Institutes of Health, National Cancer Institute during the conduct of the study and salary from Klein Buendel, Inc. Dr Wallis reports grants from National Institutes of Health, National Cancer Institute during the conduct of the study and salary from University of Colorado Denver. Dr Andersen reports grants from National Institutes of Health, National Cancer Institute during the conduct of the study, salary from San Diego State University, and personal fees from Sage Publications, Waveland Press, and Pearson Publishing. Dr Scott reports grants from National Institutes of Health, National Cancer Institute during the conduct of the study and personal fees from Mikonics, Inc and McGraw-Hill Education. Ms Eye reports grants from National Institutes of Health, National Cancer Institute during the conduct of the study and salary from Klein Buendel, Inc. Ms Liu reports grants from National Institutes of Health, National Cancer Institute during the conduct of the study and salary from Klein Buendel, Inc. Dr Cutter reports grants from National Institutes of Health, National Cancer Institute during the conduct of the study and grants and personal fees from Klein Buendel, Inc, and personal fees and Board membership from Biogen Idec, Teva Neuroscience, EMD Serono, Novartis, Pfizer, Sanofi, Questcor, Genzyme, Medimmune, Receptos, Gilead, Neuren, Apotex/Modigenetec, Opko, NHLBI, NICHD, Ono/Merck, Genentech, GSK, Tranparency Life Sciences, Roche, Opexa, Jansen, Somahlution, Savara, Nivalis, Horizen Pharma, Reata Pharma, Munck Wilson, and PTC Therapeutics.