
Abstract
Purpose:
To examine the potential impact of paraprofessional home visitors in promoting breastfeeding initiation and continuation among a high-risk population.
Design:
A secondary analysis of program data from a statewide home visitation program.
Setting:
Thirty-six Healthy Families New York sites across New York State.
Subjects:
A total of 3521 pregnant mothers at risk of poor child health and developmental outcomes.
Intervention:
Home visitors deliver a multifaceted intervention that includes educating high-risk mothers on benefits of breastfeeding, encouraging them to breastfeed and supporting their efforts during prenatal and postnatal periods.
Measures:
Home visitor-reported content and frequency of home visits, participant-reported breastfeeding initiation and duration, and covariates (Kempe Family Stress Index, race and ethnicity, region, nativity, marital status, age, and education).
Analysis:
Logistic regression.
Results:
Breastfeeding initiation increased by 1.5% for each 1-point increase in the percentage of prenatal home visits that included breastfeeding discussions. Breastfeeding continuation during the first 6 months also increased with the percentage of earlier home visits that included breastfeeding discussions. Additionally, if a participant receives 1 more home visit during the third month, her likelihood of breastfeeding at 6 months increases by 11%. Effect sizes varied by months postpartum.
Conclusions:
Delivering a breastfeeding message consistently during regular home visits is important for increasing breastfeeding rates. Given that home visiting programs target new mothers least likely to breastfeed, a more consistent focus on breastfeeding in this supportive context may reduce breastfeeding disparities.
Keywords
Introduction and Aims
The benefits of breastfeeding are well-documented for both mothers and children. Breastfed infants are at lower risk for sudden infant death syndrome, 1 more likely to be protected against infections during infancy, 2 less likely to be obese, 3,4 and more likely to have higher IQs. 5 Mothers who breastfeed have a decreased risk of breast and ovarian cancers, better birth spacing, and reduced risk of type 2 diabetes. 2,6 Research suggests that breastfeeding may also be a protective factor against child maltreatment. 7
Given these benefits for mothers and children, Healthy People 2020 has set a national goal for breastfeeding initiation at 81.9% and for continued breastfeeding for 6 months at 60.6%. 8 Multifaceted efforts to encourage breastfeeding have yielded a steady increase in breastfeeding rates in the United States. In 2011, 79% of all newborns were breastfed after birth and 49% were still breastfed at 6 months. 9 However, significant disparities in breastfeeding initiation and continuation remain based upon mothers’ demographic and socioeconomic status. 10 –13 Young, low-income, black, unmarried, and less educated mothers have lower rates of breastfeeding. For example, while 84% of mothers aged 30 or older initiated breastfeeding, only 59% of mothers younger than 20 did. 13 Disparities in continuation rates by race and maternal education indicated even steeper gaps: 70% of mothers with college degrees breastfed their baby at 6 months, but only 40% of mothers with high school degrees or less did so. When their baby was 6 months old, only 35% of black mothers continued to breastfeed. 13
Socially and economically disadvantaged mothers face multiple barriers to breastfeeding. They may lack information about the benefits of breastfeeding, receive limited or inadequate support from their social support system, lack jobs with maternal leave policies, or have psychological difficulty due to childhood sexual abuse or a cultural context that discourages breastfeeding. 14 –16 The Baby Friendly Hospital Initiative, peer and professional support, educating mothers and media campaigns are interventions that work for all mothers. 17 –19 However, no single intervention has successfully addressed the multiple breastfeeding challenges faced by mothers who are least likely to breastfeed. 20 Thus, it is worthwhile to examine how current research-based intervention programs might be utilized or extended to address these disparities.
Early home visiting programs are grounded in an ecological model that incorporates relationship- and strength-based strategies and serves socially disadvantaged families with an increased risk of poor child health and development outcomes. 21 –23 Focusing on prevention of adverse outcomes, evidence-based home visiting programs work to reduce risk and promote protective factors in maternal behaviors during pregnancy and in parenting during early childhood. 23 –27 Healthy Families America (HFA) is one such model that is widely implemented across the United States. 22,28 The HFA programs target unmarried, young, and poor mothers who tend to have lower rates of breastfeeding. Encouraging mothers to initiate and continue breastfeeding is an ancillary goal or one of the explicit targets of many HFA programs.
Research on the impact of home visiting programs on breastfeeding is limited, but findings from available studies are generally positive. 29 –32 Successful intervention strategies include educating expectant mothers on the benefits of breastfeeding and supporting their effort to breastfeed by building a trusting relationship during pregnancy and after birth in multilevel interventions. 21,31,33 Having someone regularly provide support to mothers, regardless of whether the home visitor is a nurse, a doula, a social worker, or a paraprofessional worker, seems to improve breastfeeding outcomes for mothers. 29 Although the consistency of outcomes across various home visiting programs is very promising, we know little about the aspects of home visits that contribute to improved breastfeeding outcomes and whether breastfeeding is specifically and consistently promoted during home visits. These implementation questions are critical in identifying strategies for evidence-based home visiting models because such programs are well positioned to work with the populations who are least likely to initiate and continue breastfeeding.
Healthy Families New York (HFNY), an HFA-accredited home visiting program, is a statewide program to achieve optimal child health and development and prevent child maltreatment in at-risk families. 25 –27,34 Participants in HFNY tend to be young, unmarried, Latina or black, poor, or with a childhood sexual abuse history. Given the challenges of improving breastfeeding among these populations (except for Latinas, who already have high rates of breastfeeding), HFNY promotes breastfeeding and includes breastfeeding as a performance target. This study is part of ongoing efforts to improve the program through continuous quality assurance. Specifically, we examine the proportion of home visits that includes discussion of breastfeeding and whether breastfeeding discussion is associated with the initiation and continuation of breastfeeding.
Methods
Study Setting: HFNY Programs
The HFNY is a statewide home visitation program targeted to highly stressed families residing in communities with high rates of teen pregnancy, babies with low birth weights, infant mortality, Medicaid births, and mothers with late or no prenatal care. The program is open to families who are pregnant or have an infant of less than 3 months old, and about two-thirds enroll prenatally.
Community-based agencies under contract with the state agency recruit prospective participants who are screened for risk factors such as single parenthood, teen pregnancy, poverty, and late or no prenatal care. Prospective families who screen in are given a more detailed assessment (the Kempe Family Stress Inventory) in order to determine their eligibility for the program. Sixty-six percent of those who are eligible subsequently enroll—a rate that is fairly similar across demographic groups. Currently there are 35 HFNY programs dispersed throughout New York State in both rural and urban areas, including New York City. 34
Once an expectant or new mother agrees to participate in HFNY, she is assigned to a family support worker (FSW) who initiates contact and schedules home visits. The FSW, who is almost always female, often shares the same language and cultural background as program participants. During the prenatal period, FSWs are expected to make biweekly visits. Immediately following a child’s birth, visits are increased to weekly until the child is 6 months of age, after which they decrease in intensity as the family needs change. Visits generally take place at home, but FSWs may accompany participants to other services, if needed.
The FSWs first work with mothers to establish a trusting relationship while discussing their psychological preparedness for parenthood and strategies to decrease stress. During pregnancy, FSWs encourage mothers to develop healthy prenatal behaviors by providing information about fetal development, promoting healthy habits, discouraging risky behaviors, and encouraging compliance with prenatal appointments and medical advice. Included in these conversations are discussions about the overall benefits of breastfeeding on the parent/child relationship and children’s development. The FSWs also facilitate mothers’ linkage to medical providers, Women, Infants and Children (WIC), and other support services, such as La Leche League.
Study Design and Data Sources
This study uses longitudinal data extracted from HFNY’s centralized management information system (MIS). A standard set of data are collected from families at assessment for risks, program intake, the birth of the child, and when the child is 6 months old. Furthermore, the content of each home visit, including discussion topics and referrals made, is documented in a home visit log.
The university’s institutional review board approved the data collection for HFNY and the evaluation of HFNY. At the time of program enrollment, mothers signed a written consent form for their data to be used for research purposes.
Sample
The study sample includes mothers who enrolled prenatally, had their first home visit between January 1, 2010, and July 17, 2014, and had valid 6-month follow-up data in the HFNY MIS. These selection criteria resulted in a sample of 3521 mothers. The sample is described in more detail in Table 1.
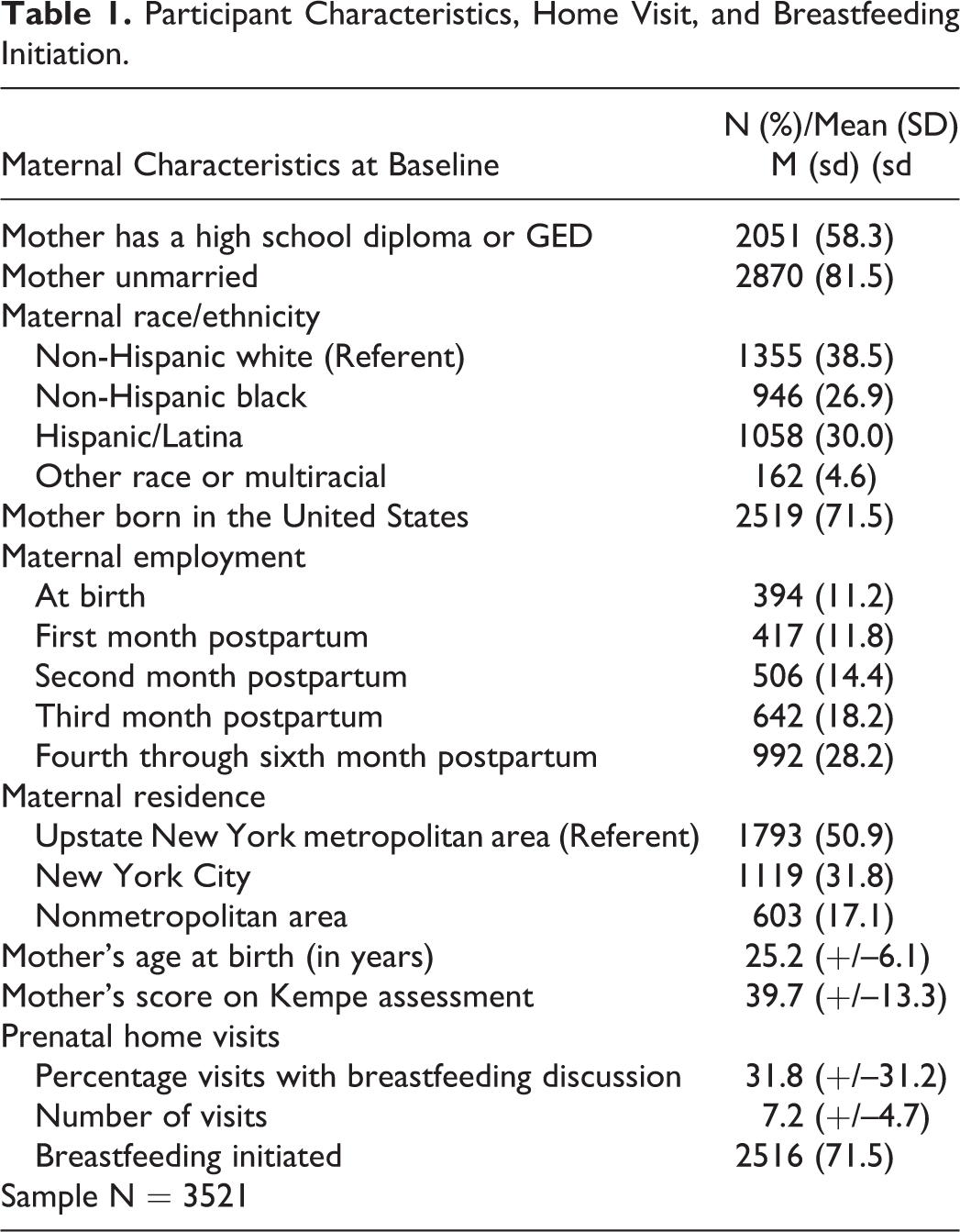
Participant Characteristics, Home Visit, and Breastfeeding Initiation.
Measures
The study used 2 measures of breastfeeding outcomes: breastfeeding initiation and continuation. Breastfeeding initiation was defined as the mother reporting having ever breastfed her infant. This information was extracted from a series of questions on infant feeding methods immediately after birth and at the 6-month follow-up. The first question asked whether mothers ever breastfed their child. Breastfeeding continuation measures how long the child was breastfed (with no distinction for exclusive vs nonexclusive breastfeeding). The second question addressed breastfeeding length or continuation. Mothers who breastfed at least once were asked how long the child was breastfed (less than a month, 1 month up to 2 months, 2 months up to 3 months, or 3 months up to 6 months) at the 6-month follow-up interview.
Our main predictor measure is breastfeeding discussion, defined as providing breastfeeding support and information during a home visit. Family support workers are trained to provide information on the benefits of breastfeeding and address any breastfeeding concerns during home visits. There is no standardized curriculum that FSWs use with their clients around breastfeeding; instead, home visitors tailor all conversations to the identified needs and interests of the families. While increasing rates of breastfeeding is considered a program goal, there are no guidelines in place for how often FSWs are expected to have these discussions. Once the conversation takes place, the FSW completes the home visit log, which includes the date and length of the visit, 71 different activities potentially engaged in during the visit (including breastfeeding information and support), and who participated in the visit. 34 Home visit logs are typically completed immediately after a home visit. A tally of breastfeeding discussions and percentage of visits in which they occurred was calculated for each of the 3521 families in our sample.
The study includes the following covariates known to be associated with breastfeeding outcomes: mother’s age at intake, marital status, race/ethnicity (black, Hispanic, non-Hispanic white, or other race), nativity, having a high school diploma or equivalent, and residence in a nonmetro area or in New York City, as opposed to other metropolitan areas in the state. We also controlled for mother’s employment during the measurement period (employment status at the child’s birth and during the postnatal period). Finally, we included a risk assessment score known as the Kempe Family Stress Inventory (KFSI). 35 The KFSI has been used in HFA programs to predict parents’ future risk of maltreating their children as well as other family functioning outcomes. The KFSI is a 10-item index that assesses risk through a psychosocial screening interview focused on maternal history and experiences. The scale covers a variety of domains, including psychiatric history, criminal and substance abuse history, childhood history of care, emotional functioning, attitudes toward and perception of child, discipline of child, and level of stress in the parent’s life. Each item is scored 0 for “no risk,” 5 for “risk” and 10 for “high risk,” and a total KFSI score is created by summing all 10 items.
Statistical Analyses
All statistical tests were 2 tailed, using an α of 0.05. Data were extracted from the HFNY MIS and analyzed using SPSS version 21 software. We used a series of binary logistic regression models to calculate the unadjusted odds of initiating breastfeeding (vs never breastfeeding); among those women who initiated breastfeeding, the odds of continuing for at least a month; among those breastfeeding at least 1 month, the odds of continuing for at least 2 months; among those breastfeeding for at least 2 months, the odds of continuing for at least 3 months; and among those breastfeeding for at least 3 months, the odds of continuing for at least 6 months.
The percentage of home visits involving breastfeeding discussions was the independent variable of interest, but in each regression, this variable was calculated for the period immediately preceding the period where breastfeeding behavior was measured (eg, breastfeeding until at least 2 months was predicted using breastfeeding discussions in the first month). When looking at breastfeeding discussions and breastfeeding behavior in the same period, there is a potential for reverse causation. Introducing the lag between BF discussions in period T and BF behavior in period T + 1 allows us to measure the true effect of breastfeeding discussion on breastfeeding behavior in the subsequent period.
Results
Breastfeeding Rates
The HFNY includes an overrepresentation of women who have characteristics associated with lower rates of breastfeeding initiation and continuation (see Table 1). Slightly more than half of the women (58.3%) had a high school diploma or GED; 15.1% were younger than the age of 19 at the child’s birth; 81.5% were unmarried; and 26.9% were non-Hispanic black. The average maternal KFSI score was 39.7 (with a score of >25 indicating a high risk of poor childhood outcomes). The rate of maternal employment gradually increased during the early postnatal period. While only 11.2% of new mothers were employed at birth, 28.2% were working outside the home at 6 months.
On average, mothers in the study sample received 7.2 home visits prior to the child’s birth, and of these visits 31.8% included a discussion of breastfeeding. During the first 3 months postpartum, families received an average of 3.5 home visits per month, and approximately one-third of the visits each month included a breastfeeding discussion.
After the birth of the child, 71.5% (2516) of mothers initiated breastfeeding, exclusively or with other types of feeding. This is lower than the 2011 national rate of 79% presented in the annual National Immunization Survey (NIS) but is not unexpected, given HFNY mothers’ multiple risk factors. 13 Hispanic mothers in the study had high rates of initiation (84%), while those younger than 18, those without a high school diploma, and unmarried mothers had low rates (61%, 66%, and 69%, respectively). Initiation rates among HFNY subgroups were similar to the rates for the same groups reported in the NIS. 13
Approximately 65% (n = 2283) of the study sample reported breastfeeding for at least the first month following the child’s birth (Figure 1). While no breastfeeding data were available for 4th or 5th month postpartum, gradual drop-offs were expected in the number of the participants who breastfed. By the sixth month, less than a quarter of the sample (21.6%) reported that that they were still breastfeeding, which is far lower than the national average of 49.4% and is lower than the rates of similar subgroups. 13 Among those who initiated breastfeeding (2516 out of 3521), however, continuation rates were 90.7% between initiation and the first month, 83.6% between the first month and the second month, 85.4% between the second month and the third month, and 46.6% between the third and sixth month.
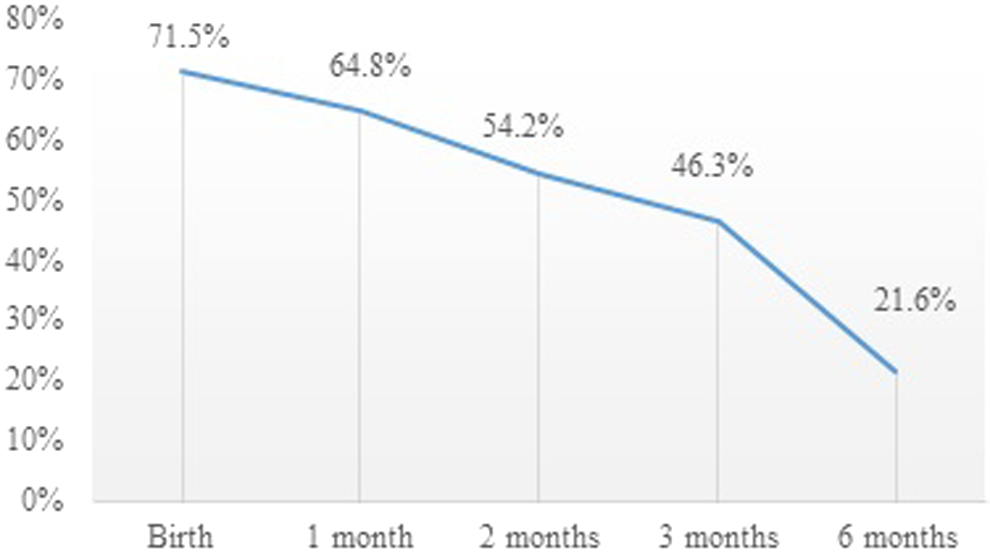
Rates of breastfeeding among HFNY mothers, birth to 6 months postpartum.
Effects of Breastfeeding Discussion on Breastfeeding Initiation and Continuation
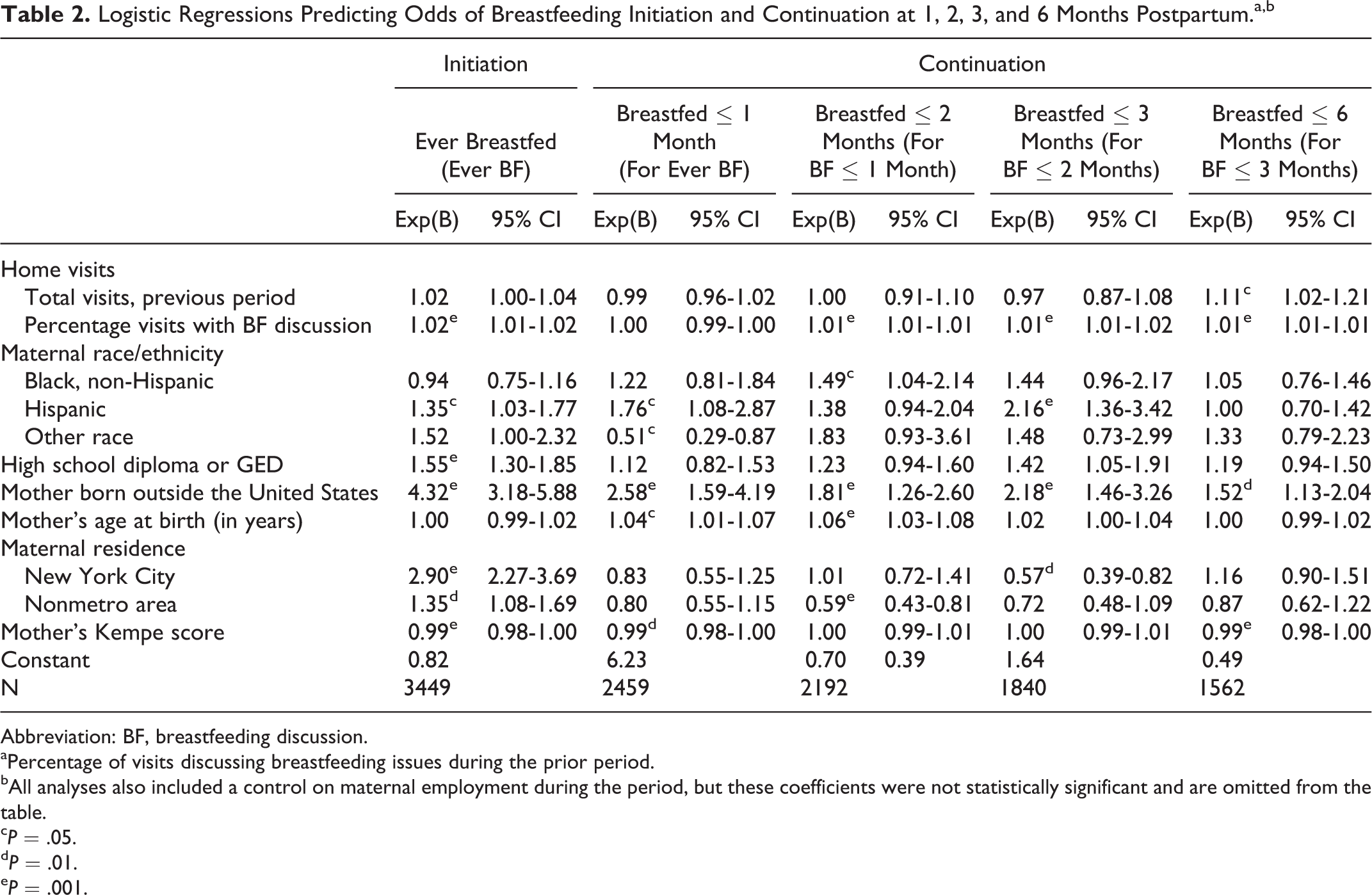
As shown in Table 2, the inclusion of breastfeeding discussion in home visits was significantly and positively associated with both the initiation and continuation of breastfeeding. This effect was independent of other factors known to influence breastfeeding, such as the mother’s age, education, race/ethnicity, and KFSI score.
Logistic Regressions Predicting Odds of Breastfeeding Initiation and Continuation at 1, 2, 3, and 6 Months Postpartum.a,b
Abbreviation: BF, breastfeeding discussion.
aPercentage of visits discussing breastfeeding issues during the prior period.
bAll analyses also included a control on maternal employment during the period, but these coefficients were not statistically significant and are omitted from the table.
cP = .05.
dP = .01.
eP = .001.
The likelihood of breastfeeding initiation increased by 1.5% for each 1-point increase in the percentage of prenatal home visits that included breastfeeding discussions. If the mean number of visits with breastfeeding discussion increases by 10%, it would increase the likelihood of breastfeeding initiation by 15%. The timing of the first prenatal breastfeeding discussion (not shown) was not related to the likelihood of initiation. While there was not a significant effect of breastfeeding discussions on breastfeeding continuation between birth and 1 month, the likelihood of breastfeeding continuation between 1 and 2 months increased by 0.8% for every 1-point increase in the percentage of home visits during the first month that included breastfeeding discussions. Similarly, the likelihood of breastfeeding continuation between 2 and 3 months increased by 1.1% for every 1-point increase in the percentage of home visits in the second month that included breastfeeding discussions, and the likelihood of breastfeeding continuation between 3 and 6 months also increased by 1.1% for every increase in the percentage of home visits in the third month that included breastfeeding discussions.
The number of home visits in the third month postpartum also had a significant positive effect on the likelihood of breastfeeding until 6 months. If a participant receives 1 more home visit during the third month, her likelihood of breastfeeding at 6 months increases by 11%. This effect was independent of the percentage of visits in which breastfeeding discussions took place.
A number of sociodemographic factors also affected breastfeeding initiation. The likelihood that HFNY participants would begin to breastfeed varied by their birthplace, ethnicity, risk-level, age, and education. We also found that geographical location was associated with breastfeeding, with the highest initiation and continuation rates occurring in New York City, even after controlling for characteristics such as maternal race and ethnicity.
Discussion
This study makes an important contribution to the current literature on strategies to reach the national public health goal to raise breastfeeding rates and reduce disparities among high-risk populations. Including breastfeeding discussions in home visits to high-risk mothers predicts higher breastfeeding initiation and continuation rates. Early home visitation programs serve expectant mothers who are disproportionately young, nonwhite or Hispanic, unmarried, and of low socioeconomic status. Therefore, these programs offer great opportunities to assist these mothers in overcoming challenges in breastfeeding initiation and continuation through education and support.
In HFNY programs, one-third of home visits included breastfeeding discussion between home visitors and expectant and new mothers. Since no comparable data exist, we cannot determine whether different patterns of discussion and visits would lead to different results. It is encouraging, however, that the proportion of home visits that included a discussion about breastfeeding was positively related to the mother’s initial and subsequent breastfeeding behavior. This occurred independent of other characteristics that generally predict breastfeeding outcomes such as race/ethnicity, education, age, and stress score. The effect of these characteristics on patterns of breastfeeding initiation and continuation among mothers in this study are similar to what we know about breastfeeding rates in the general population (see Table 2). Therefore, we can reasonably argue that more discussion about breastfeeding could lead to enhanced breastfeeding outcomes.
The findings are conceptually linked to the strength-based approach and content training of home visitors. Home visitors tailor their conversations to the specific strengths and needs of the family. Through their training, home visitors learn the importance of eliciting family strengths, described as “accentuating the positives.” 23,25 –27,31,32 This practice helps them to build trust, motivate, and ultimately engage parents in achieving self-identified goals as well as addressing and removing any obstacles. Home visitors rely on these skills when discussing the importance of breastfeeding. By tapping into parents’ own motivations and ambivalence, home visitors create a safe space where parents can openly discuss any fears or concerns regarding breastfeeding.
The study has several limitations. Thoroughness in completion of the home visit log varied among FSWs. Additionally, no standard definition for “provide breastfeeding information and support” was used. Since there were no specific guidelines as to what comprises a breastfeeding discussion, some workers may only check this topic if they have given concrete information such as pamphlets or if they made a referral. Others may do so if any discussion of breastfeeding took place, even briefly. Another limitation is that, while monitored by the state, program delivery might have varied across sites since they operate independently within different locations and varying agency structures.
Next steps should include targeted, in-depth studies to specifically identify activities and information that workers use to encourage breastfeeding among their clients. More research is also needed to identify the approaches that appear to have the most impact, and whether this impact varies based on the characteristics of the mothers. Additionally, it will be important to examine the role played by other strategies that home visitors use to achieve their goals (eg, improving families’ social support and linking families to other services in the community).
Implications
The study highlights the potential for using existing programs to deliver public health messages such as the importance of breastfeeding in a supportive educational context like that provided through home visiting. The picture that emerges underscores the importance of reinforcing the breastfeeding message through ongoing discussions between home visitors and at risk mothers during their routine home visits.
While breastfeeding is an explicit goal of the HFNY program, with associated performance targets that program sites strive to meet, program implementation is highly dependent upon the focus and training of home visitors. Therefore, we suggest that programs send a consistent message to their home visitors to avoid “drift” from this goal. This may include developing a specific menu of breastfeeding promotion activities that home visitors can complete with families at different developmental stages, though these efforts must, by necessity, be tempered by the need to support families in their particular context. In addition, programs may consider evaluating home visitors’ breastfeeding support skills using a validated instrument, so all home visitors attain a desired level of competency. 36 Finally, programs may consider collecting data that are tied to specific objectives for improving breastfeeding.
We also suggest strengthening breastfeeding support during the postnatal period in home visiting programs in order to prevent breastfeeding drop-off. Providing information about how growth spurts may change infant feeding patterns can alleviate maternal concerns about not producing enough milk, while others may need encouragement and support for continued breastfeeding including lactation counseling. 37 Addressing cultural issues and concerns about nursing in public also needs to be included in discussions during the early postnatal period. Additional visits between 3 and 6 months postpartum may benefit mothers who may have to return to work, who are stressed by continued breastfeeding, or who are unsure about continuation.
SO WHAT? Implications for Health Promotion Practitioners and Researchers
What is already known on this topic?
Interventions designed to reduce sugar-sweetened beverages (SSBs) have been effective at reducing weight gain. The use of media messages in promoting health behaviors can be effective, but experts recommend that messages be carefully tailored to the target audience’s concerns.
What does this article add?
A series of rolling cross-sectional surveys showed that the longer the Get Healthy Philly campaign public service advertisement (PSA) was in the field, the greater parents’ intention to reduce SSB consumption. Exposure to the PSA was associated with the beliefs that reducing SSBs will help prevent weight gain and diabetes, which were the main themes of the PSA.
What are the implications for health promotion practice or research?
Campaign duration (at least 9 months) and a consistent message developed through theory-based formative research with the target audience are important factors for successful health communication.
Conclusion
Increasing breastfeeding rates among mothers with many risk factors for poor child health and development outcomes is a big challenge in meeting Healthy People 2020 goals. Evidence-based home visiting programs serve expectant and new mothers with multiple risk factors, and thus are ideal settings to promote breastfeeding. Home visits where home visitors engage mothers in discussion about breastfeeding is likely to promote breastfeeding initiation and continuation among mothers in HFNY programs. The results of this study suggest a simple yet powerful strategy: having discussions about breastfeeding early and often can help families start their children off on the path to a healthy future.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this research was provided by the NYS Legislature.