
Abstract
Purpose:
Individuals with mental illnesses have higher morbidity rates and reduced life expectancy compared to the general population. Understanding how patients and providers perceive the need for prevention, as well as the barriers and beliefs that may contribute to insufficient care, are important for improving service delivery tailored to this population.
Design:
Cross-sectional; mixed methods.
Setting:
An integrated health system and a network of federally qualified health centers and safety net clinics.
Participants:
Interviews (n = 30) and surveys (n = 249) with primary care providers. Interviews (n = 158) and surveys (n = 160) with patients diagnosed with schizophrenia, bipolar, anxiety, or major depressive disorders.
Measures:
Semi-structured interviews and surveys.
Analysis:
Thematic analysis for qualitative data; frequencies for quantitative data.
Results:
More than half (n = 131, 53%) of clinicians believed patients with mental illnesses care less about preventive care than the general population, yet 88% (n = 139) of patients reported interest in improving health. Most providers (n = 216, 88%) lacked confidence that patients with mental illnesses would follow preventive recommendations; 82% (n = 129) of patients reported they would try to change lifestyles if their doctor recommended. Clinicians explained that their perception of patients’ chaotic lives and lack of interest in preventive care contributed to their fatalistic attitudes on care delivery to this population. Clinicians and patients agreed on substantial need for additional support for behavior changes. Clinicians reported providing informational support by keeping messages simple; patients reported a desire for more detailed information on reasons to complete preventive care. Patients also detailed the need for assistive and tangible support to manage behavioral health changes.
Conclusions:
Our results suggest a few clinical changes could help patients complete preventive care recommendations and improve health behaviors: improving clinician–patient collaboration on realistic goal setting, increasing visit time or utilizing behavioral health consultants that bridge primary and specialty mental health care, and increasing educational and tangible patient support services.
Keywords
Introduction
Individuals with mental illness diagnoses, particularly serious mental illnesses such as schizophrenia and bipolar disorder, have higher rates of preventable chronic conditions and higher rates of premature death than the general population, even after excluding suicide and other unnatural causes. 1 -5 One explanation for excess morbidity among people with serious mental illnesses is insufficient use of preventive care. 6 -8 Lack of awareness about preventive care, poor medical compliance, a high degree of life instability, 9,10 avoidance due to fear of finding they have a chronic condition, 11 and poor-quality relationships with clinicians or lack of continuity of care with providers 12 have all been suggested or identified as potential barriers to preventive service completion among this population.
In contrast to expectations, we recently reported that individuals with mental illness diagnoses were as or more likely than individuals without these diagnoses to receive guideline-concordant preventive screenings. 13 Despite these findings; however, screening rates were suboptimal given the higher risk of chronic disease and premature death in this population, raising the question of how primary care clinicians might better address both preventive and routine care to improve long-term health outcomes for patients with mental illnesses. Quality preventive care delivery begins with the relationship between primary care providers (PCPs) and patients, 14 -16 and this may be especially true for individuals with serious mental illnesses who see the relationship with their PCP as critical to their health. 17
The current analyses were part of a larger mixed-methods study designed to assess the rates of preventive care use among patients with mental illnesses in different health settings and explore clinician and patient perspectives on preventive health-care delivery. We used a sequential, developmental mixed-methods design. 18 In this design, qualitative results are used to develop or inform quantitative data collection. In the present study, formative qualitative interviews with PCPs informed the development of a web-based clinician survey, as interviewing a large sample of PCPs was infeasible. Formative patient interviews were likewise used to develop a parallel interview guide and survey for use with patients with mental illnesses. Interviews were designed to provide contextual detail that would allow us to understand clinician- and patient-reported beliefs, clinician-reported practice behaviors, and patient-reported preventive health behaviors. Survey data provided a sense of the magnitude of concordance between provider and patient perspectives on preventive health care. By directly comparing clinician and patient viewpoints, we sought to identify barriers and facilitators salient to both groups, as well as discordant views that could indicate areas where beliefs and practices could be modified to improve care.
Methods
Setting
Participants were recruited from PCP and patient populations at Kaiser Permanente Northwest (KPNW) and from federally qualified health centers and safety net community health clinics (CHC) belonging to the OCHIN network. KPNW is a not-for-profit, private integrated health plan that, during the study period, provided care for about 500 000 members in Oregon and southwest Washington, including individuals with Medicare and Medicaid coverage. OCHIN provides a common electronic health record (EHR) platform for its members, more than 400 federally qualified health centers in 18 states. Primary care clinicians from 34 OCHIN member organizations in 5 states met study eligibility criteria (ie, clinic provided primary care to adult patients and had an established EHR system by May 1, 2012). Of those, 27 organizations representing 107 clinics in California, North Carolina, Ohio, Oregon and Wisconsin agreed to participate. The KPNW Human Subjects Protection Office approved and monitored all research activities. Informed consent was obtained during patient interviews; clinician consent was by survey response.
Primary Care Providers
Formative clinician interviews
Primary goals of the interviews were to understand attitudes and beliefs about providing preventive care to patients with mental illnesses and to use the resulting insights to construct a brief clinician survey to be administered to a larger group of PCPs. We identified clinicians at KPNW and participating CHCs who had ≥100 patients on their panel. To increase our likelihood of interviewing clinicians with varying experience treating patients with serious mental illnesses, we stratified samples by the proportion of individuals with schizophrenia spectrum disorder or bipolar disorder diagnoses on each clinician’s panel and by clinician gender. Because the intent was to conduct interviews in-person, we restricted recruitment to clinicians in the Portland, Oregon metropolitan area, although subsequent surveys were conducted in all participating sites. We randomly selected 62 clinicians (n = 31 at each system) for recruitment. Semi-structured interviews took an average of 15 minutes. We completed 30 interviews, 15 at each setting (17 female, 13 male) from March to July 2013; inability to contact and schedule clinicians was the most common reason for not completing an interview.
Clinician Survey
The web-based survey focused on attitudes, beliefs, and practices related to providing preventive care to patients with mental illnesses. All PCPs with ≥100 total patients on their panel and ≥10 empaneled patients with mental illness diagnoses (n = 489) were invited to complete the survey. Primary care providers were sent a letter (including a chocolate bar as a token of appreciation), followed by an e-mail including a link to the survey. We telephoned nonresponders 1 to 2 weeks following the e-mailed invitation. The survey was available from December 2013 through February 2014 and took approximately 25 minutes to complete. We received 249 completed surveys, a 51% response rate. This response rate is higher than those reported by others conducting online clinician surveys, 19 and double the rate received by a group conducting topically similar work in a comparable population. 20 We could not conduct nonresponder analyses due to the lack of information about individuals who did not complete the survey. Additional details on PCP characteristics and survey content are available elsewhere. 21
Patients with Mental Illnesses
Formative patient interviews
Instruments to measure reasons for use or avoidance of preventive services among this population did not exist. Therefore, between September and December 2013, we conducted formative interviews with patients (n = 30) to ascertain patient interest in, and barriers and facilitators of, preventive health-care engagement, and to understand how patients thought about and talked about prevention, to improve construct and content validity of the survey.
Patient interviews and surveys
Using formative interview results, we constructed an interview guide and survey for use with a larger sample of patients. Patients were eligible to participate if they were ≥19 years old and had one of the following disorders: schizophrenia spectrum, bipolar/affective psychosis, major depressive, or anxiety. Individuals were excluded from participation if they had diagnoses associated with a serious cognitive or developmental disability, or if master’s level–trained interviewers with extensive experience working with individuals with mental illnesses determined they were unable to provide informed consent. Because interviews were conducted in person, we only recruited patients who resided in the Portland, Oregon metropolitan area (all KPNW members and OCHIN patients at 8 community health centers).
We targeted our enrollment to include a variety of different patterns of engagement in preventive care, across psychiatric diagnoses and balanced on gender. This type of sampling is purposeful 22 -24 in that it samples intentionally from within defined clusters based on predefined characteristics, in this case preventive care patterns, patient psychiatric diagnoses, and gender. Preventive care patterns were derived from the EMR based on 7 common preventive services or screenings (body mass index, cholesterol level, blood pressure, flu shot, pap smear, mammogram, colorectal cancer screening), and individuals were grouped by the number of gaps on these screenings (0,1,2,3+). After purposefully creating the sampling clusters we used a randomization procedure included in SAS (v.9.3; Cary, North Carolina) to randomly select individuals from each cluster in each setting for interviews. All individuals with schizophrenia spectrum disorders in both settings were included in the sample pool as there were relatively few from which to sample. Of 1130 recruitment letters mailed to potential participants, 231 were undeliverable or associated with disconnected phone numbers, leaving 899 available for recruitment. We telephoned potential participants up to 6 times over the following month and were unable to contact 429 (48%) individuals. Of the 470 with whom we had contact, 227 refused; typical refusal reasons were “not interested” or “too busy.” We enrolled 163 individuals for an overall response rate of 18%. Among those with whom we had contact (n = 470), the participation rate was 35%. Individuals we recruited did not meaningfully differ from those who chose not to participate or whom we could not contact. However, as we purposefully set out to achieve certain recruitment goals (eg, gender parity, see above), we adjusted our recruitment strategy to successfully meet our targets and thus some potential participants received more/fewer recruitment contacts. See Supplemental Table 1 for additional patient nonresponder analyses. Interviews and surveys were completed between July 2014 and August 2015.
Self-administered surveys were sent to participants’ homes to complete prior to interview appointments. Surveys took approximately 45 minutes to complete and focused on health-related practices, interest in changing health behaviors, quality of care, and barriers and facilitators to preventive care. Participants brought completed surveys to the interview, or completed them at the appointment if they needed assistance or were not finished (3 were returned uncompleted or were never returned).
At the interview appointment, we used a structured interview guide with semi-structured and open-ended follow-up questions to elicit context and detail. We compensated participants for their time with a $50 gift card to a local shopping chain. Five participants never completed interviews despite several attempts to reschedule. Questionnaires and interview guides are available upon request.
Data Analysis
Quantitative analysis
We report descriptive statistics using SPSS v.22 (IBM).
Qualitative analysis
Provider and patient interviews were recorded using encryption-enabled devices, and transcribed verbatim. The qualitative analysis team met weekly while reading initial interview transcripts to develop descriptive code lists. Starting with open coding techniques to identify broad concepts being expressed by participants, 25 coders continued to meet weekly until no new codes emerged, then met monthly for the remainder of the project to discuss emerging themes. The team used Atlas.ti software queries to identify examples and counter examples of codes applied to transcripts. 26 Thirty-six (23%) of 158 patient transcripts were randomly selected and double-coded; agreement was 85% between coders.
We used thematic analysis 27,28 to characterize patients’ and clinicians’ descriptions of stated beliefs and actions related to preventive service delivery and preventive service use themes. We actively sought disconfirming quotes and modified themes to accurately represent the descriptive range expressed by participants.
Results
Sample Characteristics
Primary care providers who returned surveys had a mean age of 47 years (standard deviation [SD] = 10; range: 28-76), and had been practicing medicine, posttraining, for an average of 14 years (SD = 10; range <1-42). Provider respondents were 57% female (n = 135) and 85% white (n = 195). Patients’ mean age was 47 years (SD = 14; range: 19-87); 53% were female (n = 87) and 68% were white (n = 99). Patients had diagnoses of bipolar (n = 54, 33%), schizophrenia spectrum (n = 44, 27%), major depressive (n = 40, 25%), and anxiety (n = 25, 15%) disorders. Patients reported suboptimal health, with more than 4 in 10 patients reporting that their health was fair (n = 50, 31%) or poor (n = 17, 11%). Table 1 presents additional demographic characteristics for providers and patients.
Provider and Patient Participant Demographic Characteristics.

Abbreviation: KPNW, Kaiser Permanente Northwest; CHC, community health/safety-net clinics; SD, standard deviation.
We organized survey responses and interview data from patients and clinicians into 3 overarching themes that emerged during analysis: Patient interest in preventive health care, likelihood of patients following preventive health-care recommendations, and support needed for patients to change health behaviors.
Patient Interest in Preventive Health Care
Clinicians believe patients with mental illnesses are not interested in preventive care
Answers to several survey questions indicated that clinicians felt that patients with mental illnesses were not as interested in preventive health as patients without mental illnesses. Fifty-three percent (n = 131) reported they believed patients with mental illnesses cared about preventive health slightly to a great deal less than the rest of their patient population. Sixty-eight percent (n = 163) reported that “lack of patient interest in prevention” had moderately or greatly affected their ability to deliver preventive care to individuals with mental illnesses. Even more (80%, n = 191) reported their ability to deliver preventive care was moderately or greatly affected by the fact that “patients come in with acute problems.” Additional clinician-reported barriers to preventive care delivery are presented in Table 2.
Perceived Barriers to Preventive Care Completion among Providers and Patients.a
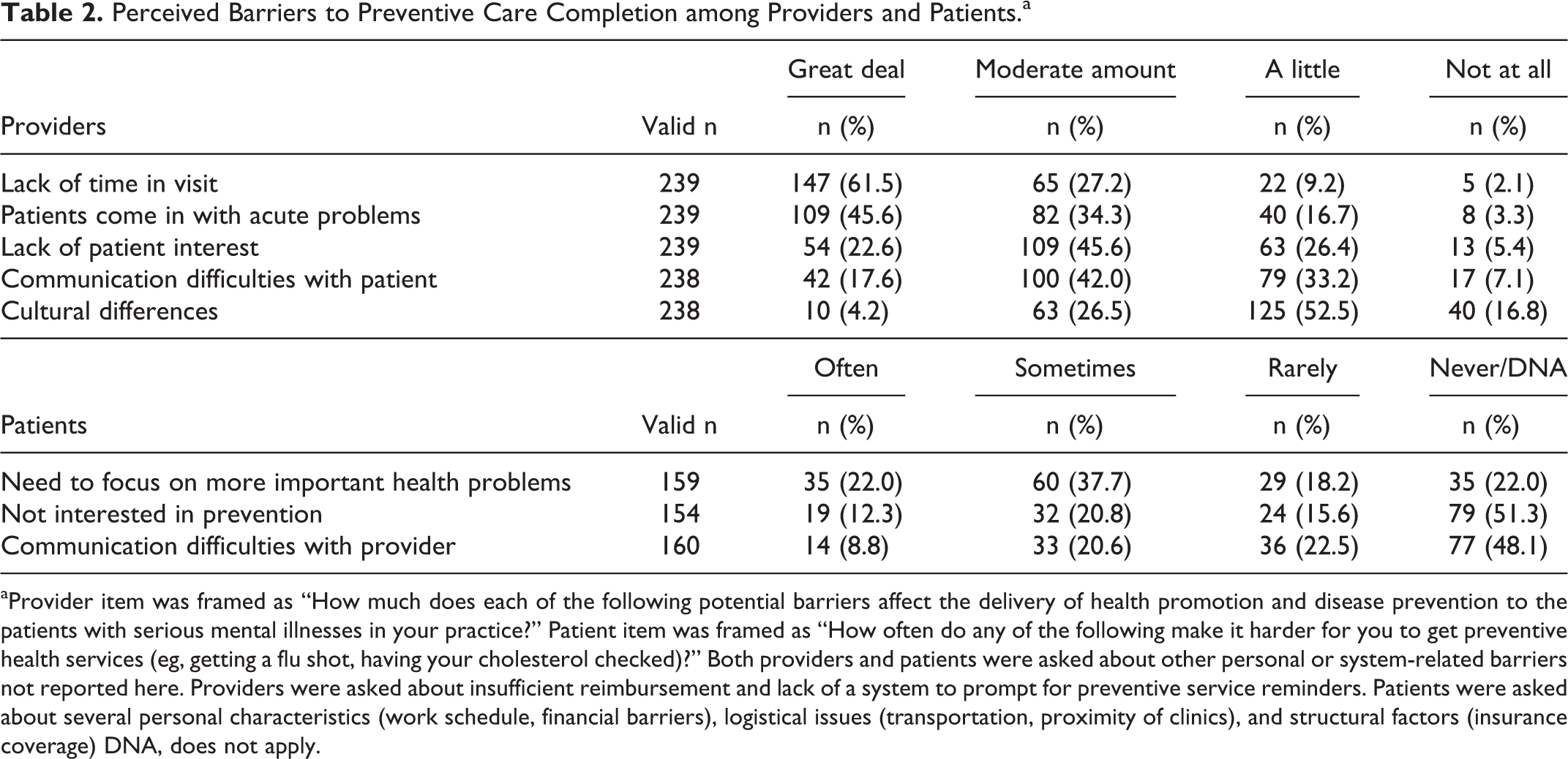
aProvider item was framed as “How much does each of the following potential barriers affect the delivery of health promotion and disease prevention to the patients with serious mental illnesses in your practice?” Patient item was framed as “How often do any of the following make it harder for you to get preventive health services (eg, getting a flu shot, having your cholesterol checked)?” Both providers and patients were asked about other personal or system-related barriers not reported here. Providers were asked about insufficient reimbursement and lack of a system to prompt for preventive service reminders. Patients were asked about several personal characteristics (work schedule, financial barriers), logistical issues (transportation, proximity of clinics), and structural factors (insurance coverage) DNA, does not apply.
In interviews, clinicians elaborated on how, from their perspective, patients’ needs to focus on acute health concerns, whether related to mental health or physical health, interfered with discussions about prevention. As one explained: When they do come in they tend to focus on what really bothers them. They’re not really concerned as much as other patients with.…preventive care.…if they’re having mental health issues that seems to be the major thing that causes a lot of difficulties. Like they’re having problems with depression, or they’re not feeling good, or if they’re.…you know, schizophrenic.…So trying to get through that to just regular routine things is sometimes hard. (male physician) These are patients that do live very chaotic lives and maybe are less aware of their physical body, and so it’s just less of a priority. Until something very acute happens. Which then they often end up in the emergency department. (female physician)
Patients report they are interested in preventive care
In contrast to clinician impressions, patients reported a high level of interest in “improving health-related practices such as diet, exercising, smoking, drinking:” 53% (n = 84) reported that they were “very interested,” and an additional 35% (n = 55) reported that they were “somewhat interested.” Further, 77% of patients (n = 121) disagreed or strongly disagreed with the statement “I don’t really want to focus on preventive care when I see my doctor.” Additional patient-reported barriers to preventive care are presented in Table 2.
Some patients specifically noted a lack of communication about preventive care during primary care visits: And she [doctor] does what she can do to help make things better. I am kind of concerned though.…about the lack of dialogue between me and doctors about preventive medicine. It seems like I’m always going there because of something and they treat what that is, but they don’t say, well, let’s talk about how we can avoid going back to this. Maybe, you know, changing your diet or maybe taking some vitamins, or whatever warrants the situation. (female, major depressive disorder) I think it’s the most important thing.…That’s what healthcare is for.…the whole idea to me is trying not to get sick. Not going and getting help once you’re already sick.…I eat very, very healthy. I try to get exercise. And pay attention to things. (female, bipolar disorder)
Likelihood of Patients Following through with Preventive Health Care Recommendations
Clinicians lack confidence that patients with mental illnesses will follow preventive care recommendations
Eighty-eight percent (n = 216) of clinicians reported they were “slightly” or “not at all” confident patients with mental illnesses would follow through on making behavior changes needed to improve their health, while only 42% (n = 102) reported similar low levels of confidence for patients without mental illnesses. In interviews, this belief was closely related to the belief that patients with mental illnesses do not prioritize their long-term health: Well, compliance is pretty poor in general within that group. And, self-care is lousy: extra chemicals, tobacco, following healthy diets and exercising is probably nonexistent in the seriously mentally ill.…I probably put preventive care way down on the list because of their mental illness.…I probably have a prejudice against even going into preventive care. Because I think that mostly we’re putting out fires about short term things.…I probably bring a fatalistic prejudice to the encounters. (male physician) I don’t think it’s [preventive care] going to make much of a difference.…this patient is going to die at an earlier age just from social unrest or living on the streets or the drugs they’re abusing.…I don’t see it necessarily being in the same longitudinal benefit as there would be for, you know, middle income Americans. Which I think is unfortunate and clearly, you know, it’s a bias on my part. And it’s one that probably contributes to poorer health care for that population.…(male physician) So when people are treated, and are stable on medication.…who are very well controlled, they do very well.…They follow-up. They want preventive services. I find that people who are not treating their psychosis as well as they should, and bipolar and schizophrenia, do not then follow through with any preventive measures. (female physician) I feel like I want them to quit but a lot of times they have no interest at all in quitting. And so, oftentimes my counseling kind of ends at that point. If someone has no interest in quitting, then I’ve brought it up and talked about why I think they should quit, and encourage them to do so. But if they have no interest then going farther is kind of a waste of both of our time. And so I feel like it gets lost right there for folks a lot of times because they just have no interest. (female physician)
Patient confidence about following through with preventive care recommendations was mixed
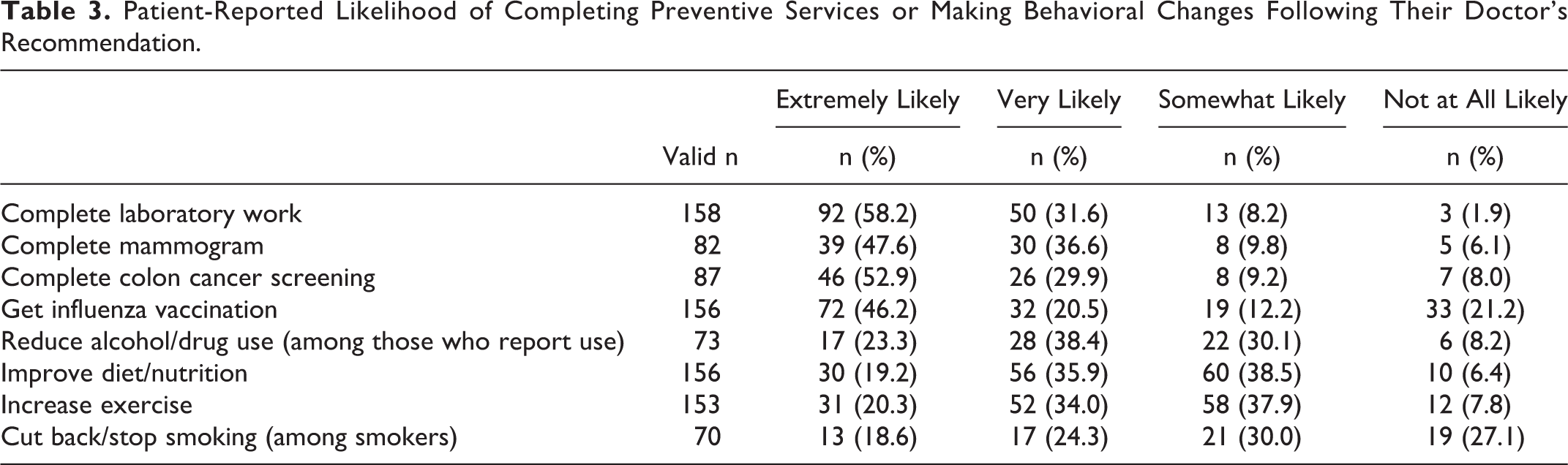
When considering lifestyle changes generally, 82% of patients (n = 129) agreed or strongly agreed with the statement “If my doctor advises me to change my lifestyle, I will try to do it.” When asked to report on the likelihood of following through on specific provider recommendations for preventive tests or behavioral changes, patients reported being considerably more likely to complete preventive services (eg, labarotary work, screenings) than they were to make behavioral changes (eg, stop drinking or smoking). Nearly 90% (n = 142) reported that they would be “extremely” or “very likely” to complete recommended laboratory work; 43% (n = 30) of current smokers said they would be “extremely” or “very likely” to cut back or stop smoking if recommended by their doctors. Nonetheless, for all behaviors except for smoking, over 50% of patients reported that they were “very” or “extremely likely” to make changes following a doctor’s recommendation. See Table 3 for additional details.
Patient-Reported Likelihood of Completing Preventive Services or Making Behavioral Changes Following Their Doctor’s Recommendation.
Although patients were somewhat more optimistic than clinicians, both were largely in agreement about the difficulty of making behavioral changes, particularly around smoking behavior. As one patient noted: He’s [doctor] told me more than once now, probably multiple times [to quit smoking]. And I even.…was introduced to the [quit] program, or he set me up to be introduced. Somebody called me and talked to me and I denied [declined to join]. You know, I went into denial and basically told him that.…I didn’t need help or something. I didn’t follow through with it because I don’t believe I can achieve it. I don’t have faith in myself. I use it as a recreational thing to take and help break my stress points at times. (male, anxiety disorder) It’s just hard to lose weight and change your diet, just [finger snap] cold turkey like that.…I try to change my diet sometimes, you know, eat more salad or those nutrition bars, nutrition drinks and whatever, but, just it’s hard to resist sweets and all that stuff [Laughs.] (male, schizophrenia spectrum disorder)
Support Needed for Patients to Change Health Behaviors
Clinicians believe patients with mental illnesses need additional preventive care support, but time is a major barrier
The most common barrier to preventive care identified by providers was lack of time: 89% (n = 212) of providers felt time constraints moderately or greatly affected their ability to deliver preventive care. In interviews, providers noted time was especially limited in visits with patients with mental illnesses because of the need to address psychiatric issues: The entire appointment is used to try to counsel the patient on actually taking medication for their psychosis. So then room to actually have a robust conversation about prevention is often left to the notes in the after visit summary. (female physician) The people that don’t have mental illness, the majority of them readily accept screening tests and they readily accept most vaccinations.…but I think that people who are mentally ill require a lot more hand holding. They require a lot more reassurance and a lot more explaining of what the tests are about. And it’s more challenging for them.…Sometimes it does make the visit longer.…(female physician) I try to simplify it [prevention message]. So I don’t talk about simple carbs versus complex carbs or the Mediterranean Diet. I usually just say, do you drink soda? Don’t drink soda. Do you drink juice? Don’t drink juice. Do you smoke? Don’t smoke. And just realize if I can make small steps to make a bigger difference. (male physician)
Patients would like more time with providers to develop a trusting relationship and additional support to follow preventive care recommendations
Like providers, patients frequently mentioned lack of time during visits as a barrier to care. From the patient perspective, hurried providers often failed to understand their concerns or took time to develop trusting relationships. Although patients appreciated when they felt doctors and medical staff took extra time with them, they also understood that doctors were busy and noted that small changes in behavior and demeanor could make them feel more respected and listened to: Well, I don’t have a problem with quick service. But anyone can do quick service, and still be polite and acknowledge that you’re a human being and not just a little part of the job they have to come in and do really quick. (male, major depressive disorder) And every time she [doctor] would see me, the first thing she would come into the room and sit and just sit and talk with me. No paper, no chart, no computer screen. Nothing. Just, how are you today? What’s going on? Do you like the weather? Wasn’t necessary [and it only] took about a minute of her time. (female, schizophrenia spectrum disorder) Depend[s] on what it [the recommendation] applies to. If I think it’s not necessary to do it, I just don’t think it’s necessary, I just don’t see the point.…, like if they told me, ‘okay, get this vaccine because it’s for the best, but we don’t know.…Like I want to know the statistics and research on it before I do it. Like how accurate is it? (female, major depressive disorder) If it’s coming back specifically to changing my diet, I would need a lot of help to get a lot of specifics because I can follow directions and instructions, but just saying, ‘You should eat nutritional’ is not going to help me. So ‘Increase these things in your diet’, that’s like ‘Whoa’! What does that mean? I need.…practical. You know, if you give me some recipes, I can follow a recipe, yeah, throw in.…’You should eat this’, or ‘You should eat this’. (male, bipolar disorder) [E]ver since the diagnosis of prediabetes, there’s a one hour, Kaiser online class or something that you can watch about this. That’s it?? You know.…I’m not uneducated on prediabetes and diabetes in general, so I’m like, I feel like what I need is more support with, again, this is where my diet’s at, and this is where it should be. How can we, you know, move that along? Yeah, you know, looking up glycemic index and glycemic load.…it’s what I can find on the internet. Which is a great resource, but I would much prefer.…to be able to see some nutritionist or dietician.…(male, major depressive disorder)
Discussion
Our findings suggest clinically relevant differences in perspectives between clinicians and patients about the importance of delivering and following through on preventive care. One important discrepancy was the finding that a majority of patients report interest in making behavioral health changes, despite some clinicians’ beliefs to the contrary. Previous research focused specifically on cardiovascular screening found similar discrepancies between providers and their patients with mental illnesses. 29 In our findings, providers were especially discouraged about their perception that patients with mental illnesses were uninterested in smoking cessation, yet 43% of patients with mental illnesses who smoked reported a willingness to engage in cessation efforts should their doctor recommend them. This substantial proportion is consistent with previous findings in this population, 30,31 and presents an important opportunity for clinicians to motivate and support cessation efforts. Primary care providers do not appear to recognize the potential positive influence they have on these patients, and beliefs that patients with mental illnesses are uninterested in preventive care, won’t attend visits, or are unwilling to make health changes may be negatively affecting quality of care. 32 -35
Patients expressed a desire for further information about why preventive services are important and additional, concrete, support for enacting behavioral changes. Clinicians struggled to find time and sometimes had low expectations that patients would follow through with recommendations, thus avoiding taking the time to make them. Given the fatalistic orientation expressed by some clinicians in our study and others, 34,36 clinicians may be falsely interpreting patients’ desire for more assistance or information as resistance to recommendations. Sometimes clinicians interpreted the need for more information as distrust or suspicion. However, rather than elaborate, explore barriers, and build trust, clinicians responded by reducing or simplifying messaging, the opposite of what patients were looking for. Communication difficulty between providers and patients with mental illnesses, including those resulting from mental illness symptoms or lack of patient self-advocacy, have been noted. 9 Yet patient desire for improved communication and positive relationships with clinicians 37,38 and a collaborative clinician–patient relationship to enhance patient-directed health management 39 have also been noted. Improving communication and shared decision-making may aid in assessing and developing realistic health goals and implementing practical behavioral change strategies. 40,41 When developmental delays, lower reading level or lower educational attainment, or comprehension challenges due to psychotropic or illicit drug use create provider–patient communication difficulties, alternative approaches to shared decision-making, goal setting, and health behavior coaching may be necessary. Health systems could support the health management of individuals with mental illness diagnoses by flagging upcoming appointments and expanding visit time to allow for more robust communication and support between clinicians and patients; whether this improves health outcomes should be evaluated in future research. Given time constraints noted by clinicians, and physicians’ low confidence in patients’ abilities to make health changes, additional ancillary, nonphysician support for behavior change seems warranted. Increased engagement with and support from clinical staff including nurses, 42,43 care managers, 44 or peers 45 has been shown to be effective in managing health and health-related practices. Behavioral health specialists embedded in primary care clinics are also a potential solution. 46 Availability of these counselors allows an immediate, warm hand-off to a skilled clinician with time to explore the lack of interest or self-efficacy, use motivational interviewing techniques, engage patients in supported, tailored behavioral change interventions or triage them to existing resources (eg, quit-lines), and follow-up beyond the primary care visit to coordinate ongoing care and address social determinants of health. 47 Future research should assess the effectiveness of such a model of care.
Initiating and maintaining behavioral changes are a complex, nonlinear process 48,49 that is challenging for individuals with 29 and without 50,51 mental illnesses. Consistent with this, our patient participants recognized these difficulties and reported needs for additional, individually tailored support. Many patients with mental illnesses realize that behavioral change is a process that involves periods of greater or lesser focus on specific goals; mental health recovery is a parallel process for many people as it also involves strides forward cycling with setbacks. Contrary to negative clinician expectations, meaningful health-related behavioral change outcomes are possible 52 when patients have access to tailored programs such as for weight loss 53 -55 and smoking cessation 56 that take into account their unique needs related to mental health. Making such interventions available, and providing adequate support to patients to facilitate intervention attendance and adherence, could result in significant improvements in health outcomes.
A few limitations should be noted. First, attitudes and beliefs of nonresponders to our clinician survey may differ from those who responded. Second, our patient participation rate was somewhat low. Although individuals who joined our study did not differ demographically from individuals who we could not recruit, we cannot be certain that their beliefs about preventive health would not have differed. We were also unable to compare nonresponders with study participants on variables that were not derived from the EHR (eg, homelessness). Finally, our results may be not be generalizable outside integrated care and federally qualified health center settings.
Conclusions
Clinicians working with patients with mental illnesses ascribed a lack of interest in preventive care to their patients that patients themselves did not report. Implications of these beliefs, combined with time constraints, include the possibility that clinicians focus mostly on providing straightforward preventive care that does not require much time (eg, laboratory tests) rather than more time-consuming care (eg, smoking or nutritional counseling). Inattention to supporting more important behavioral changes may result in missed opportunities to address the very changes that could reduce early morbidity and mortality.
So What?
What is Already known on this Topic?
Individuals with mental illnesses are a vulnerable population with higher than average morbidity and earlier mortality rates. Reasons for this disparity include the effects of antipsychotic medications and lifestyle behaviors that may be amenable to behavioral change efforts.
What does this Article Add?
Despite fatalistic beliefs from providers on the ability of their patients with mental illnesses to engage in and change health-related behaviors, we found that individuals with mental illnesses are very interested in improving their health and changing their health-related behaviors.
What are the Implications for Health Promotion Practice or Research?
Along with PCPs, ancillary providers—including nurses, behavioral health specialists, care managers, and peers—could play a larger role in working with patients with mental illnesses on achieving behavioral health goals.
Supplemental Material
Supplemental Material, Suppl_table1 - Perspectives on Providing And Receiving Preventive Health Care From Primary Care Providers and Their Patients With Mental Illnesses
Supplemental Material, Suppl_table1 for Perspectives on Providing And Receiving Preventive Health Care From Primary Care Providers and Their Patients With Mental Illnesses by Scott P. Stumbo, Bobbi Jo H. Yarborough, Micah T. Yarborough, and Carla A. Green in American Journal of Health Promotion
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the National Institute of Mental Health (R01 MH096795). The funding agency played no role in the design or conduct of the study, the preparation of this manuscript, nor the decision to submit the report for publication. The authors would like to thank Julie Cavese and Alison Firemark for their work in conducting the patient interviews.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.