
Abstract
Purpose:
Examine predictors of short- and long-term adherence to a tobacco-free policy prohibiting all tobacco use inside and outdoors on Executive Branch property in Kentucky.
Design:
Cross-sectional online surveys administered at 2 time points.
Setting:
Commonwealth of Kentucky.
Participants:
27 000 employees of the Kentucky Executive Branch were invited to participate in 2 online surveys: March 2015, 4 months postpolicy (N = 4854) and August 2015, 9 months postpolicy (N = 3522).
Intervention:
Executive order prohibiting tobacco use on Executive property implemented November 2014.
Measures:
Tobacco use, tobacco users’ adherence to the tobacco-free policy, and personal characteristics were assessed.
Analysis:
Two separate logistic regression models used to determine predictors of short- and long-term adherence to the policy.
Results:
In the short term, employees who had seen others violate the policy (P < .001) and had more tobacco-using friends (P = .020) were less likely to adhere to the policy. At 9 months after the policy, employees who were older (P = .038) and those who had seen others violate the policy (P < .001) were less likely to report adherence to the policy. Tobacco-using employees who worked in a county with a comprehensive smoke-free ordinance (P = .047) were more likely to adhere to the policy.
Conclusion:
This study indicates the need for strong policy compliance procedures, employer-based tobacco treatment programs accompanying tobacco-free policy change, and smoke-free workplace laws to promote prohealth norms.
Keywords
Smoke-free workplace policies encourage cessation, reduce tobacco consumption, and shift the protobacco norm. 1 -3 These policies have little impact on smoking rates or air quality if policy adherence is low. 4 Few studies examine adherence to smoke- and tobacco-free policies, particularly among employees. 5 Although the majority of employees support and comply with smoke-free legislation, 6,7 adherence is significantly better among workers who are aware and supportive of the policy and whose owners/managers are nonsmokers. 7 Other smoke- and tobacco-free policy research has examined adherence in bars/restaurants 4 and in the university setting. 8 -10 The majority of noncompliant smokers on university campuses reported knowingly violating the policy. 8,9 Less is known about employee adherence to tobacco-free workplace policies, specifically those implemented by governmental entities.
Purpose
In September 2014, the then Kentucky Governor signed an Executive Order prohibiting the use of cigarettes, cigars, electronic cigarettes, and all other tobacco products, indoors and outdoors, on all property owned, leased, or contracted by the Executive Branch. 11 Kentucky does not have a statewide smoke-free workplace law. 11,12 To evaluate adherence to the Executive Order, we surveyed employees of the Executive Branch covered by the policy at 2 different time points. The study purpose was to examine the short- and long-term predictors of policy adherence.
Methods
Design and Sample
Two cross-sectional online surveys were administered to all employees of the Executive Branch (N = 27 000). The first survey was distributed via e-mail in March 2015, 4 months postpolicy. A second survey was sent to all employees 9 months postpolicy in August 2015.
A total of 4854 individuals responded to the 4-month postsurvey (18% response rate); 3522 employees completed the 9-month postsurvey (13% response rate). Of these respondents, only current tobacco users who indicated whether or not they had adhered to the policy during the past 7 days were retained for the analysis. The effective sample sizes were 724 and 453 employees, respectively, for the March 2015 and August 2015 cohorts. Based on an adult smoking rate in the state of approximately 25.9%, 13 the effective response rates among smokers were estimated to be 10.4% and 6.5%, respectively.
Procedures
The e-mail invitation explained the purpose of the study, the importance of participating, and that completing and submitting the online survey implies consent to participate. In addition, an anonymous survey link was included in the e-mail. Based on the logistics of governmental procedures and human participants protection guidelines, the survey invitation was distributed by the Personnel Cabinet in partnership with the Kentucky Office of Health Policy. A reminder e-mail was sent to all employees 1 week later. The survey was administered using Qualtrics 2015, 14 a secure survey administration and database software. Qualtrics has SAS 70 Certification and meets the rigorous privacy standards imposed on health-care records by the Health Insurance Portability and Accountability Act. All Qualtrics accounts are hidden behind passwords, and all data are protected with real-time data replication. 14
Measures
Each survey assessed demographic characteristics, personal and perceived adherence to the tobacco-free policy, tobacco use, exposure to the policy, and social norms relative to tobacco use. Demographic characteristics included age (years), gender (“male,” “female,” “transgender”), race (“white,” “black/African American,” “Asian,” “Pacific Islander,” “American Indian, Alaskan Native,” “2 or more races,” “Other”), and ethnicity (“Hispanic” or “non-Hispanic”). Race and ethnicity were combined and coded as “white/non-Hispanic” or “Other” for analysis given that the majority of the employee population is white/non-Hispanic.
Policy adherence was measured via self-report. Respondents were asked whether they had seen someone else violating the policy in the past 7 days (separate items for cigarettes and other tobacco products; yes/no). These 2 items were combined into a single binary “adherence by others” variable (regardless of tobacco product). Respondents were asked the same 2 questions to determine personal adherence to the policy and combined to indicate “personal adherence” to the policy.
Tobacco use was assessed for cigarettes, hookah, little cigars, smokeless tobacco, e-cigarettes, and other tobacco products. For cigarettes, 2 questions were asked: “Have you smoked at least 100 cigarettes in your lifetime?” (yes/no) and “When was the last time you smoked a cigarette?” with responses ranging from “never,” “today,” “1 to 7 days ago,” “8 to 29 days ago,” “1 to 3 months ago,” “4 to 6 months ago,” “7 to 11 months ago,” “1 to 4 years ago,” or “5 years ago or more.” Those who said they had smoked at least 100 cigarettes in their lifetime and smoked a cigarette within the past 30 days were current cigarette users. 13 For each of the other tobacco products, only the “most recent use” question was asked. Those who had used the product in the past 30 days were considered current product users. Only current users of at least 1 tobacco product were retained for the study. For this analysis, tobacco use was categorized as “cigarette only,” “other tobacco product only,” or “both cigarettes and other tobacco products.”
To assess exposure to the tobacco-free policy, participants were asked whether they had read the workplace policy and if they had seen signs about the policy at their workplace (yes/no for each). To measure social norms, participants were asked, “How many of your 5 closest friends use any form of tobacco?” Responses ranged from “0” to “5.” Participants indicated the county where they worked. This information was used to create a binary variable to indicate whether or not they worked in a county with a comprehensive smoke-free workplace ordinance (covering all restaurants, bars, and workplaces with few to no exemptions) 12 as another indicator of social norms.
Analysis
Descriptive statistics, including means and standard deviations or frequency distributions, as appropriate, were used to summarize study variables for each cohort. Respondents who indicated they had smoked cigarettes or used other tobacco products in the past 7 days at work were coded as nonadherent to the policy. Bivariate comparisons were assessed using the 2-sample t test or χ2 test of association. Two separate logistic regression models were used to determine predictors of short- and long-term adherence to the tobacco-free policy. The Hosmer-Lemeshow test was used to assess goodness of fit for each logistic regression model, and variance inflation factors were used to gauge multicollinearity. For both models described here, the Hosmer-Lemeshow tests were not significant (P values = .95 and .96), suggesting the model fits the data well. The variance inflation factors for both models were all <2, suggesting the multicollinearity did not distort model parameters. Data analysis was conducted using SAS, version 9.4, with an α level of .05 throughout.
Results
Although the March 2015 cohort was younger than those who completed the survey in August 2015 (M = 45.4 and 47.0, respectively; P = .016), the 2 cohorts did not differ on gender, race/ethnicity, or tobacco use status (Table 1). Both samples were primarily female, white/non-Hispanic, and the largest percentage in both groups used only cigarettes.
Demographic and Personal Characteristics, Policy Exposure, Adherence, and Social Norms by Cohort.
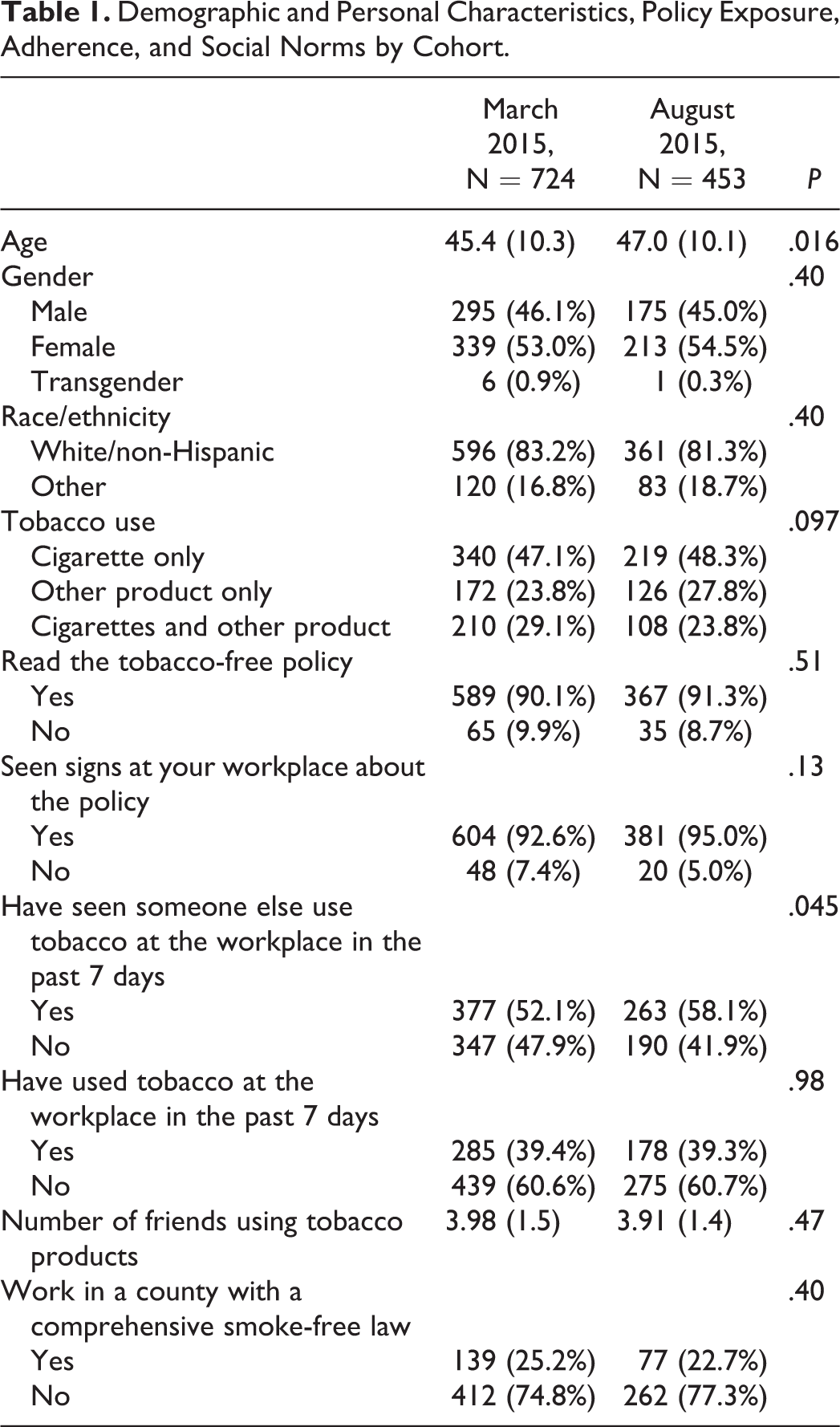
There was a difference in observed adherence between the short- and long-term assessments: 48% reported they had not seen anyone in violation of the policy 4 months postpolicy, but only 42% reported adherence of others 9 months after implementation (P = .045). Reported personal adherence did not differ between cohorts: 39% reported adhering to the tobacco-free policy during the past 7 days. At both time points, more than 90% of participants reported they had read the policy and seen signs about the policy at the workplace; there were no differences by cohort in exposure to the policy. The number of friends who used tobacco was similar between the 2 cohorts, with approximately 4 tobacco-using friends reported. Approximately one-fourth of the participants lived in a county with a smoke-free workplace ordinance, with no difference between cohorts.
Short- and Long-Term Predictors of Adherence to the Policy
The logistic model to determine short-term predictors of personal adherence 4 months postpolicy (March 2015) was significant overall (likelihood ratio χ2 = 204.4, P < .001). Significant predictors of short-term personal adherence included whether they had seen others violate the policy and number of friends who use tobacco products (Table 2). Those who had seen others use tobacco product(s) at work were 95% less likely to report adherence to the tobacco-free policy (P < .001). Similarly, for each additional friend who used tobacco, the participant was 17% less likely to report adherence to the policy (P = .020). Demographic variables and tobacco use group, exposure to the policy, and whether they worked in a county with a comprehensive smoke-free ordinance were not associated with personal adherence in the short term.
Logistic Regressions Modeling Short- and Long-Term Personal Adherence to the Tobacco-Free Executive Order.
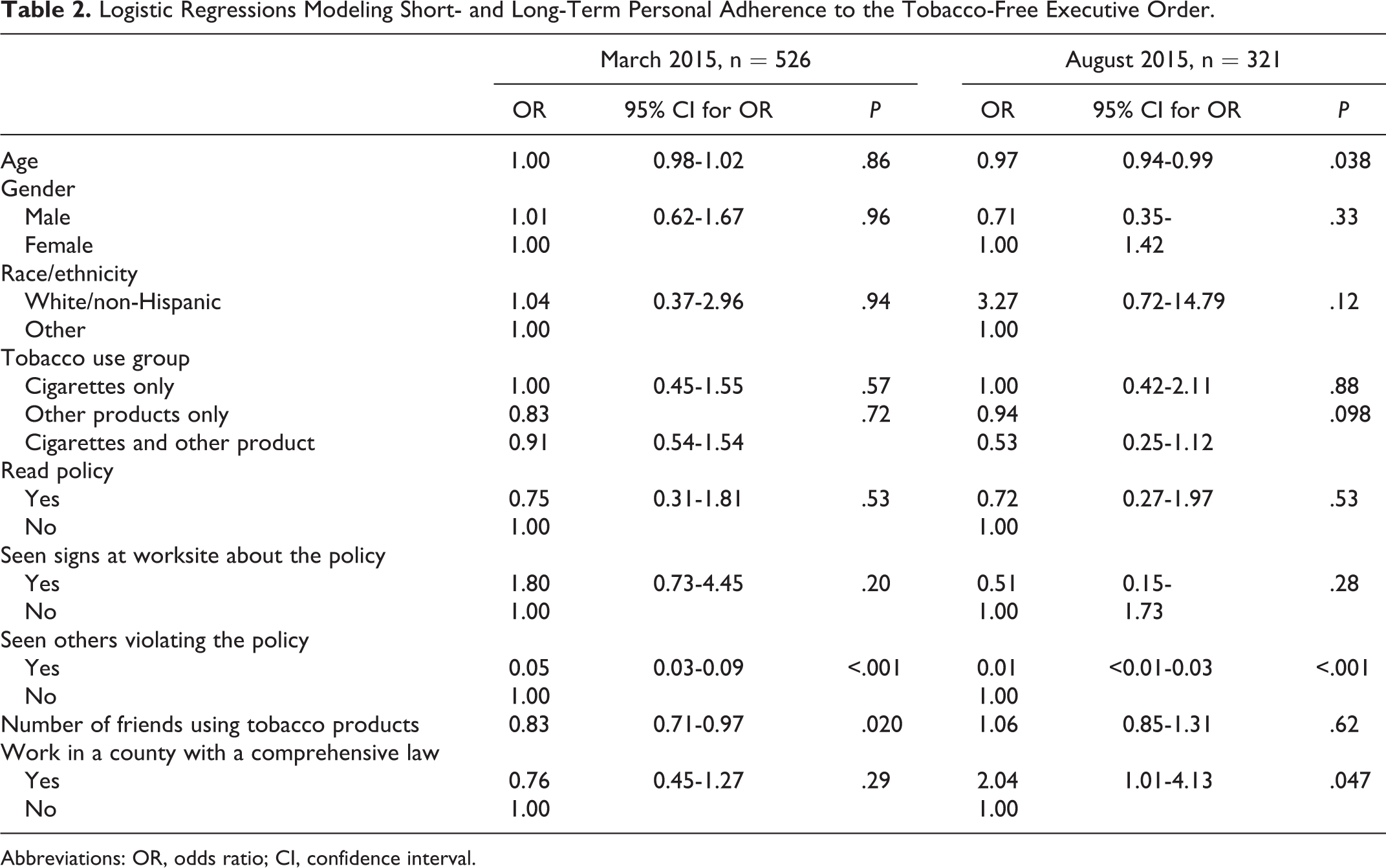
Abbreviations: OR, odds ratio; CI, confidence interval.
The logistic model for long-term predictors of personal adherence 9 months postpolicy (August 2015) was significant overall (likelihood ratio χ2 = 167.4, P < .001; Table 2). Significant long-term predictors of adherence were age, whether they had seen others violate the tobacco-free policy in the past 7 days, and whether they worked in a county with a comprehensive smoke-free ordinance. For each additional 10 years of age, a participant was 28% less likely to report adherence to the tobacco-free policy during the past 7 days (P = .038). Similar to the short-term model, those who reported seeing violators in the past 7 days were 99% less likely to report they had adhered to the policy (P < .001). Finally, those working in a county with a comprehensive smoke-free ordinance were 104% more likely to indicate they had adhered to the tobacco-free policy during the past week (P = .047). Long-term personal adherence was not associated with race/ethnicity, tobacco use group, exposure to the policy, or number of friends using tobacco products.
Discussion
In the short term (4 months postpolicy), employees of the Executive Branch were less likely to report personal adherence to the tobacco-free Executive Order within the past week if they saw others violate the policy and if they had more tobacco-using friends. Similarly, those who saw others violating the policy were less likely to adhere to the policy in the long term (9 months postpolicy). These findings highlight the potential impact of peer and social networks on adherence to tobacco-free policies. We used observation of others as a measure of perceived policy adherence in this study based on existing literature on the impact of social acceptability and peer influence on smoking behaviors. In a study predicting smokers’ adherence to smoke-free policies, 15 social acceptability of smoking significantly predicted nonadherence. Although numerous studies have shown the impact of peers and social contacts on smoking cessation, 16,17 further research is needed to understand workplace norms, including peer influences in the workplace and supervisory influences, in relation to policy adherence. This information can lend to the design and testing of peer support and social network-based interventions on adherence to tobacco-free policies at the worksite.
In the long term, employees in counties with a comprehensive smoke-free ordinance were more likely to adhere to the policy. Smoke-free laws change the social norms related to tobacco use. Those living in smoke-free communities come to expect smoke-free environments, which may translate to adherence to tobacco-free policies at work. 5,18 Further longitudinal research is warranted in this area.
Age was also a significant predictor of long-term adherence. Given that tobacco dependence is associated with nonadherence to smoke-free policies, 15 older employees who have used tobacco over a longer period may be more dependent on tobacco. This finding has implications for tobacco treatment at the worksite. Older, more dependent tobacco users need access to both affordable tobacco treatment medications and counseling as part of the workplace insurance benefits and employee assistance programs. Kentucky Executive Branch employees have access to tobacco treatment medications and counseling. There may be a need to further promote these resources.
Despite high exposure to the policy via signage and written sources in both cohorts, adherence to the policy was relatively low, further indicating the need to consider individual- and context-specific factors that could be related to poor policy adherence, including perceived favorability of the policy and tobacco use behavior of supervisors. 7 In light of the history of tobacco and prevalence of tobacco use in Kentucky, formal enforcement criteria along with clear-cut procedures, substantive penalties, and funding to sustain adherence strategies need to be delineated when drafting smoke- and tobacco-free policies. 4
Findings must be interpreted cautiously due to limitations in data collection and sample size. Although we were not able to analyze adherence behaviors over time, given the design of the study (2 cross-sectional surveys rather than a repeated measures strategy), this was not the focus of the study. Instead we evaluated predictors of personal adherence at each time point. The concern about lack of matching from one cohort to the second is mitigated by the observation that the 2 groups were largely similar demographically, with the exception that the earlier cohort was slightly younger overall. As a secondary limitation, although the response rates were as expected for e-mailed surveys, 19 this analysis was limited to only current tobacco users, so the effective sample sizes were diminished. Still, the cohort sizes of 724 and 453 tobacco-using employees, respectively, are relatively large and a strength of this study. It is important to acknowledge the possibility that current tobacco users and nonadherents to the policy may have been less inclined to participate in this survey, which may also be reflected in the response rate.
Our findings fill a significant gap in tobacco-free policy implementation research. Despite a dramatic increase in smoke- and tobacco-free policies, 5,20 findings indicate a need for continued emphasis on both policy adherence efforts and employer-based tobacco treatment programs. Social network analysis may be a useful research method for further understanding social norms related to tobacco-free policy adherence. Future research is needed to design and test peer support interventions to change protobacco norms at the worksite. Advocacy for smoke-free laws could be key in changing protobacco norms that have been engrained through the sociocultural and historical context particularly in tobacco-growing states.
So What?
What is already known on this topic?
Smoke- and tobacco-free policies have been successful in changing the cultural norms around tobacco use.
What does this article add?
Given limited research on adherence to tobacco-free policies, findings reveal that, in the short term, adherence to a tobacco-free property policy was influenced by protobacco norms; tobacco-using employees were less likely to adhere if they saw others violate the policy and if they had more tobacco-using friends. Nine months after the policy, older employees and those who saw others violating the policy were less likely to adhere; those who worked in a county with a comprehensive smoke-free ordinance were more likely to adhere.
What are the implications for health promotion practices or research?
Peer support-based platforms and other social norm methods need to be explored to promote tobacco-free policy adherence. Without policy adherence, these policies will not be successful and will not achieve the intended positive outcomes.
Footnotes
Acknowledgments
The authors wish to thank the Kentucky Personnel Cabinet and the Office of Health Policy for their assistance with survey distribution to state employees.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported through a contract between the Kentucky Department for Public Health and the University of Kentucky Research Foundation. Institutional review board approval number: 14-0914-X1B.