
Abstract
Purpose:
This study assessed the impact of Mental Health First Aid (MHFA) in the United States with a theoretically based and psychometrically sound measure, the Mental Health Beliefs and Literacy Scale (MBLS).
Design:
Online MBLS surveys were administered pre-MHFA training, 3-weeks post-training, and 6-months posttraining.
Setting:
Mental Health First Aid trainings carried out across the United States.
Participants:
Six hundred sixty-two trainees were contacted, and 273 (41%) completed the presurvey. Of those, 63% filled out the postsurvey and 35% completed the 6-month survey. Seventy-six individuals completed all 3 surveys.
Intervention:
Mental Health First Aid is an 8-hour education program to help the general public identify, understand, and respond to signs of mental illness and substance abuse; to date, almost 1 million people have been trained.
Measure:
The MLBS, based on the Unified Theory of Behavior Change framework, consists of attitudinal, social-, and skill-based constructs affecting the intention to perform and achievement of MHFA actions and reports of their actual completion.
Analysis:
Change across time points was assessed using multivariate repeated measures analysis of variance.
Results:
Significant short- and longer term changes were found in internally consistent constructs tapping positive beliefs about MHFA actions, the confidence and intention to perform them as well as mental health literacy.
Conclusion:
The MBLS documented strong positive effects of MHFA training that were greater in individuals without prior mental health training, the intended targets of MHFA efforts.
Keywords
Purpose
Mental illness is a substantial public health problem, with as many as 1 in 3 adults and 1 in 5 children and/or youth meeting diagnostic criteria for a psychiatric disorder. 1 -3 However, many individuals with mental illness remain unidentified and untreated, 4 allowing mild problems to possibly progress into more severe and intractable disease. Identifying these individuals early in the course of their illness or those at risk of developing such problems and referring them to appropriate intervention can reduce the burden they may face. Mental health screenings (e.g., well-care visit screenings for depression 5 ) are a logical step toward increased early identification of mental health problems. However, because visits with health-care providers may be brief and infrequent, relying solely on these professionals is insufficient. To identify more individuals with mental health concerns and address these issues early in their course, a broader range of the community must be aware of the signs and symptoms of mental illness and be provided with basic knowledge and skills to assist appropriately.
Mental Health First Aid (MHFA) 6,7 developed in Australia is a public education program that helps nonmental health professionals identify, understand, and respond to people showing signs of mental illness and substance use disorders, with separate curricula focusing on adults and youth. In 2008, the National Council for Behavioral Health (herein termed the Council) led the adaptation of the Adult MHFA curriculum and, in concert with the Georgetown University Center for Child and Human Development (GUCCHD), the Youth MHFA curriculum for use in the United States. The Adult MHFA curriculum introduces participants to risk factors and warning signs of mental health problems, builds an understanding of the prevalence and impact of various mental illness, provides an overview of common treatments, and teaches ways to help an individual with mental health problems connect to appropriate and evidence-based professional, peer, social, and self-help resources. The Youth MHFA curriculum places particular emphasis on the unique risk factors and warning signs of mental health problems in adolescents, the importance of early intervention, and strategies for helping a youth in crisis or experiencing a mental health or substance use problem.
Adoption of MHFA in the United States has grown exponentially. As of 2018, more than 1, 000, 000 people across all 50 states have been trained as First Aiders. 8 Since 2014, the Substance Abuse and Mental Health Services Administration has granted over $15 million to state education agencies and local education agencies to deliver MHFA to adults who interact with school-aged youth to help increase mental health awareness and service capacity for school-aged youth.
The significant resources devoted to disseminating MHFA nationally underscore the need for rigorous evaluation of this program in the United States. Internationally, the impact of MHFA has been supported by a number of studies. Hadlaczky and colleagues 9 completed a meta-analysis of 15 studies from Australia, Sweden, and Canada, including 6 controlled trials and 9 studies conducted in specific subpopulations, revealing that trainees experienced increases in knowledge about mental health, reductions in perceived social distance from people with mental health problems, and increases in supportive behaviors toward individuals with mental health problems.
In the United States, several studies have demonstrated that MHFA trainees have more knowledge about mental health and feel confident and comfortable aiding people with mental illness immediately following their training sessions. 10 -13 However, to our knowledge, measures used to study these outcomes were not psychometrically evaluated, and there have been no evaluations of the longer term impacts. In 2013, the Council partnered with the GUCCHD to develop an instrument to evaluate the immediate and longer term impact of MHFA training on participants’ attitudes and behaviors. This instrument, the Mental Health Beliefs and Literacy Scale (MBLS), is being employed in a number of large-scale, national evaluations of MHFA. Here, we present the first report of its use to assess the impact of MHFA in the United States posttraining and at 6-month follow-up. Further, although the target audience for MHFA is the general population, the program has drawn trainees with a wide range of mental health experience. The impact of MHFA may vary depending on the extent of this experience; therefore, we compare outcomes between those with and without previous mental health training.
Methods
Design
Three surveys were developed for online administration via a SurveyMonkey platform. 14 These included a version completed prior to training (pre), a version completed within 3 weeks following training (post) as well as a 6-month follow-up (6 month). Only the postsurvey included items tapping opinions about the training format and usefulness. The changes in trainees’ awareness of mental health signs and symptoms, comfort level in talking with someone showing signs and symptoms of a mental health problem, and the use of MHFA information to help those in need were included in the 6-month survey. All questionnaires were identical for evaluation of Youth and Adult trainings. The MHFA trainings surveyed were conducted by certified MHFA instructors who are subject to random quality assurance checks to ensure that trainings are conducted with fidelity.
Sample
The Council provided the e-mail addresses of 741 individuals who registered for either the Adult MHFA or the Youth MHFA training across the United States between June and August 2014, 662 of who had valid e-mail addresses. Each trainee received an e-mail requesting his or her participation with a link to the appropriate survey. When participants logged onto the survey, they were prompted to read the informed consent script for a confidential survey and provide their electronic consent if they wished to participate. Only trainees older than 18 years of age were permitted to participate in the survey, and only those participants who completed the presurvey were asked to complete the post and 6-month surveys. Figure 1 provides details of the recruitment flow. Of the 662 trainees who were successfully contacted, 41% (273/662) completed the presurvey. Of those who completed the presurvey and were able to be contacted again, 63% (170/268) filled out the postsurvey, the pre–post sample, and 35% (90/256) completed the 6-month survey. The 76 individuals who completed all 3 surveys comprised the 6-month follow-up sample. This study was reviewed, approved, and monitored by the Institutional Review Board of Georgetown University.
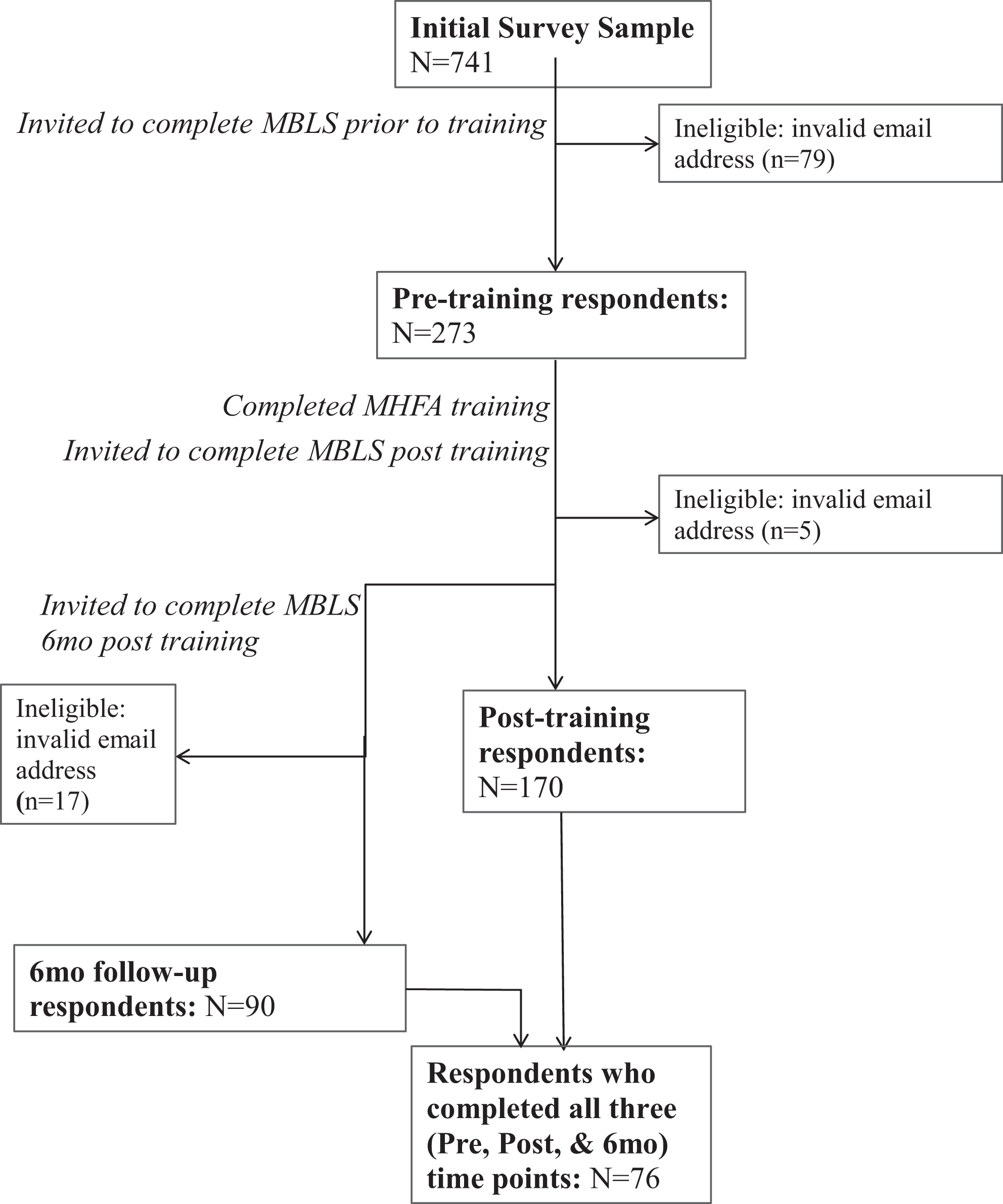
Consort flow diagram of respondents. The MBLS administration process and response rates are presented for 3 time points: pretraining, posttraining; and 6-month follow-up.
To determine a sufficient sample size, we employed the mean effect size of .58 reported in the Hadlaczky et al 9 meta-analysis of MHFA studies for measures of knowledge in a G*Power analysis for paired sample t tests using a α of .05 and a power of .8. Based on these assumptions, 44 participants would be necessary to detect significant change. Using the same assumptions as above, we conducted post hoc power analyses for MBLS constructs with adequate internal consistency. Effect sizes ranged from 0.26 to 1.04 for the pre–postanalyses, and the sample size (n = 170) was sufficient to detect change for all construct scores. For the 6-month follow-up sample repeated measures analyses, we used the partial η2as an estimate effect size (range from .047-.474). The sample size of these analyses (n = 76) was sufficient to detect change for all but 1 (usefulness) of the constructs.
Table 1 summarizes the very similar trainee characteristics for both the pre–post and the 6-month follow-up samples. Trainees were predominantly female and white and of middle age. Most trainees in each group had at least a bachelor’s degree and over 40% had a postgraduate degree. More than half of each sample reported that they had received some form of previous mental health training.
Frequency (Percentage) of Demographic Characteristics for Each Sample of Trainees.

a For this item, respondents were instructed to mark “all that apply” resulting in percentages that do not total 100.
Measures
The MBLS was developed based on the Unified Theory of Behavior Change (UTB). 15 -18 The UTB, depicted in Figure 2, posits 1 set of attitudinal and social constructs that affects the intention to engage in a behavior, and a second set of constructs (eg, knowledge and skills, cues to action) impacts the translation of intention into actual behavior. The more favorable the constructs in each set, the more likely a person will complete the target behavior. Thus, to examine the impact of MHFA, the MBLS was designed to measure changes in trainees’ intentions to perform proscribed behaviors and their reports of performing the behaviors and determinants of both intention and actual behaviors. All items were developed to correspond with the targets of MHFA training.

Framework for evaluation of mental health first aid based on the Unified Theory of Behavior Change (UTB).
Survey items were developed in an iterative manner. Employing item structure developed for UTB-based surveys, 19 -21 an initial set of items was created based on existing research and evaluations used in Australia. 22 Council staff reviewed the items to ensure that they aligned with MHFA training and goals. The immediate impact of training was assessed through pre- to post-training change in trainees’ attitudes, beliefs, and knowledge about mental health and MHFA ALGEE actions (Assess for risk of suicide or harm, Listen nonjudgmentally, Give reassurance and information, Encourage appropriate professional help, and Encourage self-help and other support strategies) and trainees intentions to and confidence in performing ALGEE. Longer term impact, measured 6 months following training, also included self-reported recognition of cues to perform MHFA-related actions and actual performance of MHFA actions. Table 2 provides a description of the constructs included in the final version of the surveys.
Summary of Constructs and their Descriptions Based on the Unified Theory of Behavior Change.

Analysis
Cronbach α values were calculated to assess the internal consistency estimates of reliability for each of the 12 a priori constructs described earlier. Also, factor analysis was conducted for each construct to examine whether items reflect the intended separate components 23 through assessment of the scree plots, component loadings, cross loadings, and correlations between components on the pattern, structure, and correlation matrices 24 . For those constructs with adequate reliability, the mean of relevant items, ignoring missing data, was calculated and used to represent that construct in all analyses. Items were reverse-coded as needed. The knowledge score was calculated by counting the number of correct responses to each item.
Descriptive statistics examined the quality of the MHFA trainings provided. Multivariate repeated measures analysis of variances (ANOVA) with post hoc Bonferroni correction were used to analyze change scores for the pre–post sample (N = 170) and the 6-month follow-up sample (n = 76). In these analyses, having previous mental health training (yes or no) was used as a between-subjects factor.
Results
Construct Consistency
Cronbach α was calculated for data collected at each of the 3 time points to assess the internal consistency of the 12 UTB-derived constructs. Most of the constructs (10 of 12) showed acceptable (0.8 > α ≥ 0.7), good (0.9 > α ≥ 0.8), or excellent (α ≥ 0.9) internal consistency. 25,26 Three of the 5 constructs within the subjective norms category had lower levels of consistency and related to issues of stigma. Two of 3 of these constructs tap beliefs about individuals with mental health problems (e.g., are they seeking attention, easy to talk with, dangerous, unpredictable), both personal and those of significant others. A third construct consists of items querying views about mental health problems (e.g., issues of disclosure). Only those constructs with acceptable consistency were used in the analyses.
Quality of MHFA Training
On a 1 to 5 scale, where 5 was extremely useful, participants indicated that the training was highly useful, regardless of whether individuals had received previous mental health instruction or not, with mean(SD) scores of 4.53(.84) and 4.70(.59), respectively. Mean usefulness ratings all exceeded 4.0 for different aspects of the training. Participants also rated the extent of their agreement with statements tapping other aspects of training quality on a 1 to 5 scale. Mean scores were over 4.0 for items tapping instructor effectiveness in teaching the material, presentation clarity, adequacy of responses to questions, adequate practice in using the MHFA actions, and safety in sharing their opinions. There was only 1 significant difference between those with and without previous mental health training; although both groups agreed that they gained new knowledge, those without mental health training reported stronger agreement.
Pre- to Post-training Changes
For the 10 UTB-derived constructs with adequate consistency, as well as the knowledge construct, we conducted multivariate repeated measures analyses to examine changes from pre- to post-training. The overall multivariate tests revealed significant effects of time (pre-post), F11,101 = 23.13, P < .000; mental health experience (yes-no), F11,101 = 2.35, P < .013; and the interaction of time and mental health experience, F11,101 = 2.95, P < .002. Nine of the 11 constructs demonstrated significant change posttraining as depicted in Table 3.
Pre–Post Changes in UTB-Derived Constructs With Adequate Internal Consistency (α > .60).

Abbreviations: MHFA, Mental Health First Aid; SD, standard deviation; UTB, Unified Theory of Behavior Change.
Trainees considered performing MHFA behaviors, or actions, to be more rewarding, less difficult, and more likely to positively impact people with mental health problems after training and were more likely to believe they should perform these behaviors. They also had greater self-confidence that they could perform behaviors to help people with mental health problems and that they would have the self-control to take action to help people with mental health problems, given the necessary knowledge. Trainees explicitly endorsed a greater intention to actually perform MHFA-related behaviors after completing the training. Also, they were more likely to agree that people important to them have more positive thoughts of those with mental health problems. Only trainees’ beliefs in the usefulness of performing MHFA behaviors and in whether people important to them thought they should use MHFA actions did not significantly change after training.
In addition to the changes in scores of attitudes related to mental health, participants showed significant improvements in knowledge about signs, symptoms, and risk factors for mental health problems from pre- (Mean = 11.82, standard deviation = 2.70) to posttraining (Mean = 13.97, standard deviation = 1.84), F1,111 = 56.39, P < .00, d = 0.931.
Pre- to Posttraining Changes: Previous Mental Health Training
Figure 3 shows that, regardless of the extent of prior mental health training, trainees showed significant positive changes from pre- to post-MHFA training for almost all of the 11 MBLS constructs. However, those trainees with no previous mental health training showed larger positive changes following MHFA training than those with previous mental health training. The interaction of time and mental health training was significant for the following constructs: Difficulty in performing MHFA activities, F1,111 = 6.30, P < .013; beliefs in the positive effects of MHFA activities, F1,111 = 6.65, P < .001; and self-confidence, F1,111 = 18.74, P < .000; and knowledge, F1,111 = 7.33, P < .008.

Cohen’s d effect size for mean change scores from pre- to posttraining for 11 constructs, stratified by those with Prior Mental Health (MH) training versus those without. Asterisk ’*’ indicates a significant positive change (P < .05) in mean scores on a construct between pre- and posttraining. Dagger “†” indicates a significantly larger positive change for individuals without prior mental health training versus those with where P < .05.
Of note, at pre-training, trainees with prior mental health training showed higher scores than those without MHFA training on 4 of the constructs; they felt that implementing MHFA would be less difficult, t155 = −2.996, P = .003; they possessed more self-confidence in their ability to carry out MHFA activities, t153 = 4.930, P = .000; they reported greater intention to carry out these activities, t155 = 2.222, P = .028; and they possessed more knowledge about general mental health, t162 = 4.308, P = .000. At post-training, there were no significant group differences for any of the constructs. For example, for knowledge, those with prior MH training scored 2.0 points higher, on average, than those without prior mental health training at pre-training. At post-training, the same group difference was only 0.3 and not significant, suggesting MHFA helped those without prior mental health training catch up in their knowledge to peers with prior training.
Follow-Up Changes: 6-Month Follow-Up Sample
Using repeated measures ANOVAs, we assessed the longitudinal changes in 11 constructs—9 of which are thought to influence behavioral intent as well as intent itself in the group of trainees who completed pre, post, and 6-month follow-up surveys. The results are portrayed in Figure 4. Similar to the results seen in the total pre–post sample, participants of the longitudinal sample showed significant changes between pre- and post-training for most of the UTB constructs thought to influence behavioral intent.
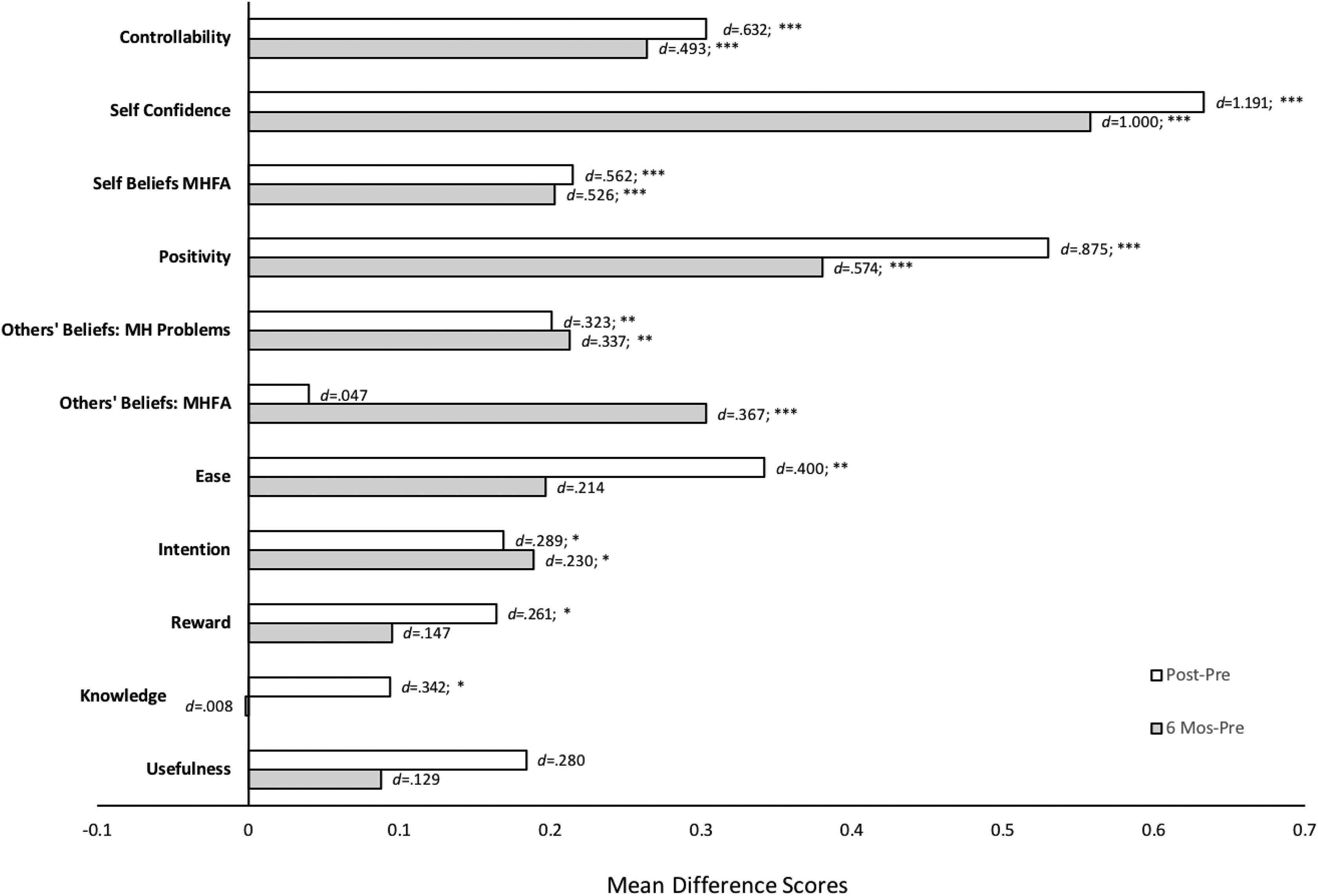
Change in MBLS construct scores for the 6-month follow-up sample. Mean differences, post minus pre and 6-month follow-up minus pre, for each of the 11 constructs. Cohen’s d indicates the effect size for change in each construct. Asterisks indicate a significant positive change in mean difference scores: *P < .05. **P < .01, ***P < .001.
Further, 6 constructs continued to remain significantly elevated over pre-levels at 6 months: self-control to perform MHFA behaviors, self confidence in performing MHFA behaviors, personal beliefs about the value of MHFA behaviors, belief that MHFA behaviors are positive, perception of others’ beliefs about people with mental health problems, and self-reported behavioral intent. Additionally, the perception of others’ beliefs about the value of MHFA behaviors, which did not change from pre to post, did show a significant increase between pre and 6 months. Figure 4 also shows changes in mental health knowledge/skills. From pre to post, knowledge significantly increased but did not remain significant from pre to 6 months. No significant interaction effects were observed between previous mental health training (yes/no) and time (pre/post/6 months) for any of the constructs.
Mental Health First Aid Actions
Table 4 shows the percentage of trainees, with and without prior mental health training, who encountered individuals with signs and symptoms of mental health difficulties and who performed MHFA actions as reported on the pre-survey.
Percentage of Trainees With Previous Mental Health (MH) Training and Percentage of Trainees without Previous MH Training Encountering Different Mental Health Cues to Action in Others and Performing Different MHFA Actions for the Total Sample at Pretraining.a

a N = 170.
b Significant difference between the percentage of trainees with and without mental health training.
Individuals displaying indicators of low mood and anxiety were most commonly recognized by trainees, followed by those showing difficulties in usual settings (e.g., school). Not surprisingly, individuals with signs of more intense problems (e.g., extreme distress and cognitive distortions) were encountered less often. The smallest percentage of trainees reported being aware of individuals with thoughts of self-harm. The same patterns described above held for the 6-month follow-up sample.
Consistently, the most frequently deployed actions were offering emotional support, listening, and helping someone calm down. Trainees frequently reported aiding in the process of identifying possible sources of help and encouraging individuals to contact professionals. However, the least common actions performed were those that involved directly intervening to get someone’s services (e.g., calling a crisis hotline and making someone an appointment) or talking directly to others about their mental health challenges (e.g., giving information about problems and inquiring about suicidal thoughts). A high percentage of trainees reported making referrals for services and supports. Most frequently, these referrals were to individual mental health providers and community mental health centers (approximately 50%). The fewest number of people said they made referrals to crisis hotlines (approximately 20%).
As Table 4 shows, on the pre-survey, using the z-test for differences in proportions of independent samples, those with mental health training were significantly more likely to have encountered each of the cues to action except for extreme distress and witness or experience trauma. In terms of MHFA actions, those with mental health training were more likely to report carrying out actions that involved more instrumental actions (e.g., calling a crisis hotline and talking with someone about suicidal thoughts, assessing for the presence of a crisis). There was no significant difference by training for more supportive actions (e.g., spent time listening, encouraged someone to seek help, and suggested options for help).
The patterns of differences in the frequency of trainees encountering cues to action and implementing actual actions reported in the total sample was similar for the 6-month follow-up sample at both the pre and the follow-up survey points. Although the same questions were asked on each survey, comparison of percentages across time points to assess the impact of training is not possible because the time frames trainees were asked to consider in responding to these items differed on the pre-survey (1 year) and the 6-month follow-up (6 months).
Discussion
The hope of MHFA is that the curriculum can increase mental health literacy and reduce stigma in the general population and spur them to carry out helpful actions for individuals in need. This study not only shows that the (MBLS) can measure key constructs relevant to MHFA training with good internal consistency reliability but also provides initial evidence in the United States that MHFA training can produce positive changes in attitudes, mental health literacy, and the intention to and confidence in carrying out ALGEE behaviors in the short and longer term.
Trainees’ intention to actually perform MHFA-related behaviors increased substantially after completing the training, and significant short-term (ie, pre–post) improvements were present in 9 of the 11 constructs thought to influence that resolve. Specifically, after training, participants felt more strongly that these MHFA actions could be implemented and would have positive effects. They reported increased confidence to perform the ALGEE behaviors and felt that doing so would be more personally gratifying. In keeping with other US studies, 10 -13 mental health literacy also increased; trainees demonstrated greater knowledge of prevalence rates, cardinal symptoms/characteristics, and effective treatments of common diagnoses. Of note, trainees perceived that people important to them had decreased stigmatizing thoughts about mental health problems after training.
Analyses of the 6-month follow-up sample showed that improvements in 6 of the 9 constructs that were significant at post-training were also significant at 6-month follow-up, providing some of the first support for longer term MHFA training effects. Although trainees’ scores on the mental health knowledge showed a significant increase from pre- to post-training, improvements were not maintained at 6-month follow-up. This supports the value of instituting MHFA “booster” sessions to help trainees maintain skills covered in their initial training.
This study provides one of the few accounts of the types of mental health issues that the general public reports identifying in their environments. At each time point, emotional symptoms (depressed mood, irritability, and anxiety) were recognized by the greatest percentage of trainees. Anxiety and mood disorders are 2 of the most prevalent mental illnesses in the United States 3 ; thus, it is not surprising that trainees reported encountering emotional cues to action related to these mental health problems most frequently. Furthermore, anxiety and mood disorders are more frequently experienced by women, 3 and a significant majority of MHFA trainees (78.9%) were women. It is possible that this influences the recognition of emotional symptoms (defined as depressive mood, irritability, and anxiety) by MHFA trainees such that those who have experienced these signs and symptoms can more readily identify them in others.
There was also a consistent pattern of which actions were deployed across time; MHFA trainees before and after training most often offered emotional support, listened to someone else, and helped someone calm down. The least common actions performed were those that involved directly intervening to get someone services (e.g., calling a crisis hotline and making someone an appointment) or talking directly to others about their mental health challenges (e.g., giving information about problems and inquiring about suicidal thoughts). These latter behaviors are less commonly carried out by those in the general population. Indeed, at baseline, those trainees without previous mental health training were less likely to call attention to concerning behavioral and emotional problems or the presence of a crisis situation in others and link individuals to indicated services, such as recommending self-help strategies and giving someone information about his or her problems or local services. These findings have important implications for MHFA training; the focus should be on these more difficult actions with less emphasis on empathic support and listening skills.
Importantly, this study found larger positive effects for individuals without prior MH training, affirming that MHFA training is having its intended effects. Importantly, the difference at baseline between those with and without MH training was only significant for one construct (difficulty), reducing the possibility that the effect was due to a ceiling effect. As articulated on their website, MHFA is intended for “people and organizations that make up the fabric of a community,” such as chambers of commerce, professional associations, hospitals, nursing homes, rotary clubs, parent organizations, social clubs, and other groups and individuals who regularly interact with a lot of people (e.g., first responders, service organization personnel, and school staff). Surprisingly, as in the current study, many who take the course have significant levels of mental health background and experience. It would not be expected that MHFA training would have as profound an effect on these individuals; thus, a full understanding of any MHFA evaluation necessitates the consideration of the extent of prior mental health training. Of note, however, findings suggest that those without MH training may “catch-up” to those with more MH training as a result of MHFA; differences observed between those with and without previous MH training at pre-training became nonsignificant at post-training for 3 constructs: knowledge, self-confidence, and difficulty performing.
Limitations
Several limitations exist when considering these findings. First, we were not able to assess changes in the percentage of trainees who recognized mental health-related signs and symptoms and carried out MHFA actions. The time period was 1 year for the pre-survey and 6 months for the 6-month follow-up survey. Second, study samples were somewhat skewed toward trainees with some previous MH training, female trainees, and restricted geographical areas. However, this skewness reflects the population generally for MHFA training. Third, a control group was not included that limits interpretation of the impact of the training. Future research will focus on testing the impact of MHFA in a randomized controlled trial with a larger sample size. Finally, the MBLS depends solely on trainee self-report. Impact findings will be strengthened if they are supplemented by data related to actual behaviors performed, such as true rates of referral to mental health services within a community and to whether individuals provided assistance and support by MHFA trainees benefit from the contact.
“SO WHAT?” Implications for Health Promotion Practitioners and Researchers
What is already known on this topic?
Mental Health First Aid is a public education program that helps non-mental health professionals identify, understand, and respond to signs of mental illness. There has been a rapid growth of MHFA training in the United States and there is evidence, mostly from studies outside the United States, MHFA training increases knowledge about mental health, reduces perceived social distance from people with mental health problems, and shows improvements in helping behaviors. 9
What does this article add?
This study evaluates the short- and longer term impact of MHFA training in the United States using a conceptually based psychometrically sound instrument called the Mental Health Beliefs and Literacy Scale. The results reveal new evidence that MHFA training in the United States not only has immediate positive impacts on trainees but also longer term impacts; trainees showed significant positive changes from baseline to 6 months posttraining in regard to their knowledge, attitudes, and beliefs about mental health and their self-confidence and behavioral intent to perform MHFA actions. A few evaluations of longer term impacts have been conducted outside the United States. 27 -29
What are the implications for health promotion practice or research?
Mental illness is a substantial health issue and public misunderstanding, prejudice, and discrimination can rob people of important life opportunities and achieving meaningful supports. That MHFA training has such clear positive long-term effects on trainees, particularly on those who have had no previous mental health training, provides support for the continued expansion of this education program across public and private systems to increase community understanding and support for individuals struggling with mental illness. Deliberate efforts should be made to disseminate Mental Health First Aid training to the public at large. Adaptation of MHFA should focus on helping trainees provide support to individuals that leads to needed changes. Future evaluation efforts should expand the measurement frame to understand MHFA’s community impact and its impact on the individuals it aims to benefit.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported in part by a Cooperative Agreement with the Substance Abuse and Mental Health Services Administration (SM056495) and was conducted in partnership with the National Council of Behavioral Health.