
Abstract



Sleep and work take up the largest proportion of an average day for US employees. 1 Sleep and work are also intricately related to one another. Specifically, insufficient sleep negatively impacts workplace outcomes (eg, employee productivity, absenteeism). 2 In addition, the nature of work (eg, workload, job demands) can result in insufficient sleep or sleep difficulties among employees. 3 Shift work is one such work characteristic that is known to adversely affect employee health.
Shift work is common in the United States. More than 21 million US workers (17.1% of the workforce) work on-call, overnight, and/or rotating shifts. 4 Shift work is associated with pressing health concerns, including metabolic syndrome, 5 diabetes, 6 cardiovascular disease, 7,8 hypertension, 9 and cancer. 10 Shift worker sleep often conflicts with the pattern of light and darkness in their environment, causing circadian misalignment that often compromises sleep health. 11,12 Consequently, shift workers report shorter sleep duration 13 and more drowsiness than do nonshift workers. 14,15 Sleep disorders are also common in this population; 36% of shift workers report having Obstructive Sleep Apnea (OSA), 14 a condition that exacerbates health risks and daytime sleepiness. 16
The American Heart Association, the National Institute for Occupational Safety and Health, and the CDC have issued recommendations for Workplace Health Promotion Programs (WHPPs). 17 –20 Meta-analysis conducted by Baicker and colleagues shows health-care spending per employee falls by approximately $3 for every $1 spent on WHPPs, and absenteeism and presenteeism costs fall approximately $2 for every $1 spent on WHPPs. 21 According to survey data, WHPPs are increasingly common as 90% of worksites in the United States featured such programs. 22 The most common WHPP targets in the studies analyzed by Baicker and colleagues 21 were weight loss and smoking cessation.
Promoting sleep health, broadly defined as insufficient sleep, poor quality sleep, and sleep disorders, should be a priority for employers particularly among worksites employing predominantly shift workers. Poor sleep health among shift workers carries an estimated economic impact of between $30 and $40 billion annually in the US in terms of direct and indirect health-care costs. 23,24 Also concerning, according to the American Academy of Sleep Medicine, the costs of health-care services received among individuals with untreated OSA are $4261 higher than those without OSA in terms of accidents, illness, lower productivity, and absenteeism. 25 In addition, another meta-analysis shows workers with OSA are at nearly 2 times greater risk for motor vehicle crashes than workers without OSA. 26 This article outlines sleep and health characteristics of shift workers in the transportation sector and articulates opportunities for WHPPs tailored to shift workers.
Examining Sleep and Health Characteristics of Shift Workers: Case History of the Transportation Sector
Surveys were administered to shift workers in the US Northeast (n = 110). The response rate was 76% in this sample. Thirty-five workers declined participation. All shift workers were employed in the transportation sector. Specifically, these workers were responsible for clearing, repairing, and maintaining roadways. During winter months, workers are staffed on extended and rotating shift schedules. Surveys were administered during a health fair in October 2017.
Surveys assessed participant demographics and chronic condition diagnoses, as well as sleep variables. Sleep was assessed using the Apnea Risk Evaluation System (ARES) questionnaire to examine OSA risk. 27 The questionnaire solicits demographic and anthropometric data, diseases associated with risk of OSA (eg, hypertension, diabetes, heart disease, or stroke), the Epworth Sleepiness Scale (ESS), 28 and frequency rating for snoring, waking up, choking, and having been told that patients stopped breathing during sleep. The ESS collects responses regarding the likelihood of dozing in a variety of circumstances (eg, lying down in the afternoon). The items on the ESS are then summed for a single measure of sleepiness so as to distinguish between less than normal sleepiness (0-5), higher than normal sleepiness (6-10), mild excessive sleepiness (11-12), moderate excessive sleepiness (13-15), and severe excessive sleepiness (>15). The ARES questionnaire was scored to indicate no risk (<4), low risk (4-5), high risk (6-10), and very high risk (>10). Descriptive analyses were computed using SPSS for Mac (Armonk, New York), and chi-square was computed to examine differences in ARES risk by self-reported OSA diagnosis.
Results indicate that high blood pressure was the most prevalent chronic condition in the sample (42.7%). Less than one-fifth of the sample reported diabetes (14.5%), depression (10.9%), or SA (16.4%). Regarding sleep characteristics, shift workers reported either “sometimes,” “often,” or “almost always” likelihood of dozing during various activities, including watching TV (83.6%) and as a passenger in a car (65.4%), but a surprisingly small number reported “sometimes,” “often,” or “almost always” likelihood of dozing while stopped in a car for a few minutes in traffic (16.4%). Few participants reported normal sleepiness (1.8%), whereas approximately one quarter were higher than normal in terms of sleepiness (22.7%), mildly excessively sleepy (13.6%), moderately excessively sleepy (27.7%), or severely sleepy (33.6%). Reports of snoring were particularly high in the current sample (83.7%), and the majority of the sample received a high risk score according to the ARES for OSA (48.2%) or very high risk (6.3%). Chi-square analysis revealed ARES risk did vary significantly by OSA diagnosis (P < .001). Among those individuals who scored low on ARES, 85.7% reported no OSA diagnosis; among those who scored high on ARES, 82.9% reported no OSA diagnosis. Yet among those with very high ARES scores, 71.4% reported an OSA diagnosis.
Implications for Future WHPPS Tailored to Shift Workers
This study points to a potential critical gap in the identification and treatment of OSA and excessive daytime sleepiness during many activities among transportation shift workers. Specifically, results show more than half of the sample at high to very high risk for OSA, although only 16.4% overall reported a diagnosis. Interestingly, the overwhelming majority of individuals at high risk for OSA did not report OSA diagnosis (82.9%). It is worth noting that there was a high prevalence of chronic diseases such as high blood pressure.
These findings suggest several opportunities for future WHPPs tailored to shift workers. Practitioners designing efforts to promote health among shift workers may consider the following recommendations:
Identify and reduce barriers to OSA symptom reporting. Unfortunately, research among vigilance-critical jobs, such as transportation, have found underreporting of sleep-related issues for fears of job loss.
29,30
Future research may endeavor to destigmatize OSA and sleep difficulties among these workers.
Tailored recommendations that incorporate circadian principles. Shift workers require sleep guidance based on their particular shift, requiring WHPPs that deliver personalized guidance on sleep hygiene, such as sleep timing and napping, that incorporate circadian principles.
31
For instance, research among maintenance workers on shift schedules found forward rotating shifts were optimal for sleep and health outcomes.
32
WHPPs tailored to shift workers hold promise for improving health and sleep among these workers at high risk for adverse outcomes and reducing risk for unintentional accidents such as motor vehicle crashes. Worksite interventions tailored to shift workers could take a number of forms, 18 yet are well-served incorporating OSA and circadian principles in their scope.
Chronic Condition Diagnoses Reported Among Shift Workers in the Transportation Sector.a
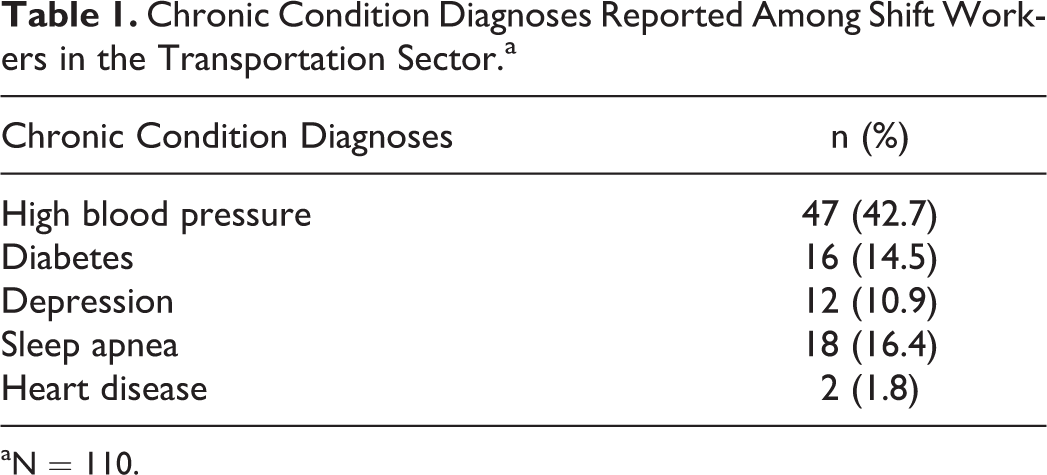
aN = 110.
Sleep Characteristics and OSA Risk Among Shift Workers in the Transportation Sector.a

Abbreviations: ARES, apnea risk evaluation system; OSA, obstructive sleep apnea.
aN = 110.
bParticipant who responded.
cParticipants who responded “sometimes,” “often,” or “almost always.”
dParticipant responses to the ARES questionnaire was scored to indicate no risk (<4), low risk (4-5), high risk (6-10), and very high risk (>10).