
Abstract
Purpose:
To assess the effectiveness of an intervention to promote influenza vaccination among members of an Affordable Care Act (ACA) insurance plan.
Design:
Randomized controlled trial.
Setting:
Messages were delivered by a community-based, nonprofit health insurance provider to its members in Central Texas.
Participants:
Adult subscribers for whom either a phone number or an e-mail address was available (n = 25 649).
Intervention:
Participants were randomly assigned to be sent (1) no messages, (2) messages encouraging influenza vaccination via e-mails and texts, and (3) messages encouraging influenza vaccination through e-mails, texts, and postal mail. Messages were sent between September 12, 2017 and November 17, 2017.
Measures:
Influenza vaccination was determined using medical and pharmacy claims.
Analysis:
Rate differences and 95% confidence intervals between each exposure condition were calculated for the overall population and by subgroups.
Results:
The vaccination rate by December 31, 2017 was 16.9%. Those sent both electronic messages and postal mail were significantly more likely to be vaccinated than those who were not sent messages (rate difference: 2.5%; 95% confidence interval [CI]: 1.4-3.6) and those who were sent electronic messages only (rate difference: 1.6%; 95% CI: 0.5-2.8).
Conclusion:
A combination of messages delivered via text, e-mail, and postal mail generated a modest but significant positive effect on influenza vaccine rates in an ACA plan population. The postal mail component was essential for achieving this effect.
Keywords
Purpose
A substantial gap exists between the influenza vaccination rate among adults aged 18 to 64 years—estimated at 38% for the 2016 to 2017 season 1 —and the Healthy People 2020 target of 70%. 2 The Community Preventive Services Task Force (Task Force), established by the US Department of Health and Human Services in 1996, utilizes findings from rigorous systematic reviews to identify effective health promotion and disease prevention intervention approaches. Two strategies recommended by the Task Force to increase vaccination rates are client vaccination reminder interventions and incentives to obtain vaccines. 3 The Task Force also identified a need for further research on effective implementation, sustainability, and expansion of reminder interventions and on the effectiveness of the use of emerging communication technologies, such as e-mail and text messages. 4
In 2017, Sendero Health Plans, Inc (Sendero), a community-based, nonprofit organization that provides health-care coverage in Central Texas, sought to increase influenza vaccination uptake among members of its Affordable Care Act (ACA) marketplace plan. Sendero provides a typical ACA plan that covers preventive services, including influenza vaccination, at no cost to its members. 5 This project provided an opportunity to assess the effectiveness of best practice recommendations in a population and context that has been understudied. Prior vaccine promotion studies have focused on high-risk populations (eg, older adults, those with chronic conditions such as diabetes, health-care workers, or pregnant women) and messages delivered from health-care providers to their own patients. 6 -8 To our knowledge, no studies focused on lower risk populations and implemented outside health-care delivery contexts have been described in the peer-reviewed literature.
The purpose of this study was to assess the effectiveness of an intervention to promote influenza vaccination among members of an ACA insurance plan. This study assessed the relative effectiveness of (1) messages encouraging influenza vaccination via e-mails and texts and (2) messages encouraging influenza vaccination through e-mails, texts, and postal mail, among adults enrolled in an ACA plan.
Methods
Design
This randomized controlled study with 3 arms targeted adult ACA plan subscribers enrolled through Sendero.
Sample
The target population included 25 702 adults aged 18 years or older living in an 8-county area in central Texas, which includes Austin. To prevent contamination between intervention and control participants in the same household, only the main policy holder was included. The institutional review board of the University of Texas Health Science Center at Tyler granted this study administrative approval as exempt research and a waiver of informed consent (IRB #17-016).
According to the US Census, in 2010, this 8-county area served by Sendero was home to approximately 1.8 million people, including 1.3 million aged 18 years old or older. Of the adults, 27% were 18 to 29 years old, 21% were 30 to 39 years old, 19% were 40 to 49 years old, and 33% were 50 years old or older. The racial/ethnic composition of the area was 31% Hispanic, 56% non-Hispanic white, and 7% non-Hispanic black. Approximately 21% spoke Spanish at home. Two of the 8 counties are Federally Designated Shortage Areas for primary care.
Measures
All measures were obtained from administrative records collected electronically as part of the routine practice of the health plan and its provider network. The outcome of interest was receipt of an influenza vaccination between September 12, 2017, and December 31, 2017, documented by claims data submitted to Sendero Health Plans by a doctor’s office or pharmacy. Sex, age, and high-risk status (ie, having one of the following: asthma, diabetes, heart disease, or chronic obstructive pulmonary disease) was sourced from enrollment records and medical claims.
Intervention
Participants were randomly assigned to 1 of 3 groups: (1) control—no direct messages sent; (2) electronic messages only—messages sent via texts and e-mails; and (3) electronic messages plus postal mail—messages sent via text, e-mails, and US postal service. Although all members were eligible to receive a $10 gift card to a local grocery store if they obtained an influenza vaccination before December 31, 2017, only those in groups 2 and 3 were sent information about the incentive. All messages were written in both English and Spanish and are available in the supplemental files.
Participants in group 2 (electronic messages only) and group 3 (electronic plus postal mail group) were sent a total of 4 electronic messages. A text message sent on September 12 and e-mail on October 9 encouraged members to get their free influenza vaccination and provided information about the $10 incentive. A second e-mail sent on November 13 and second text sent on November 17 reminded members to get their influenza vaccination before the end of the year to be eligible for the incentive.
Participants in group 3 (electronic messages plus postal mail group) were also sent influenza vaccine promotion messages via US postal service on September 19. Message content was developed based on the findings of a meta-analysis of influenza-related communications research by the US Centers for Disease Control and Prevention. 9 Participants who were identified as having a condition that put them at higher risk received a letter stating that “the flu can be more serious for people with” their specific chronic condition, with a brief explanation as to why. Remaining participants were sent an oversized postcard encouraging members to get their flu shot to protect both themselves and others in their community who are “more likely to get very sick from the flu.”
Analysis
Chi-square tests were used to determine whether differential representation existed across study groups in terms of sex, age-group, and risk status. The influenza vaccination rate during the study period was calculated by study group and within study groups by sex, age-groups, and risk status. Rate differences and 95% confidence intervals between each study group for the overall population and by sex, age-groups, and risk status were used to assess the effects and relative effects of the 3-level intervention. A multivariable logistic regression model was used to assess the effect of a 3-level exposure variable on influenza vaccination, adjusted for sex, age, and risk status. Statistical significance for all comparisons was set at P < .05. Analyses were based on intention to treat. Randomization and analyses were conducted using Stata 14 (College Station, Texas).
Results
After excluding those in the target population for whom both phone number and e-mail address were missing (n = 53, 0.2%), N = 25 649 were randomly assigned to the 3 study groups. Those who had received an influenza vaccination prior to messaging launch were excluded from the analysis (n = 378), resulting in a study population of 25 271. No significant differences were found across the 3 study groups by sex (P = .28) age-group (P = .73), or risk status (P = .99). Just over half of participants were female, the median age was 41 years, and 8.3% were classified as high risk (Table 1).
Demographic Characteristics and Risk Status of the Study Population by Study Group.
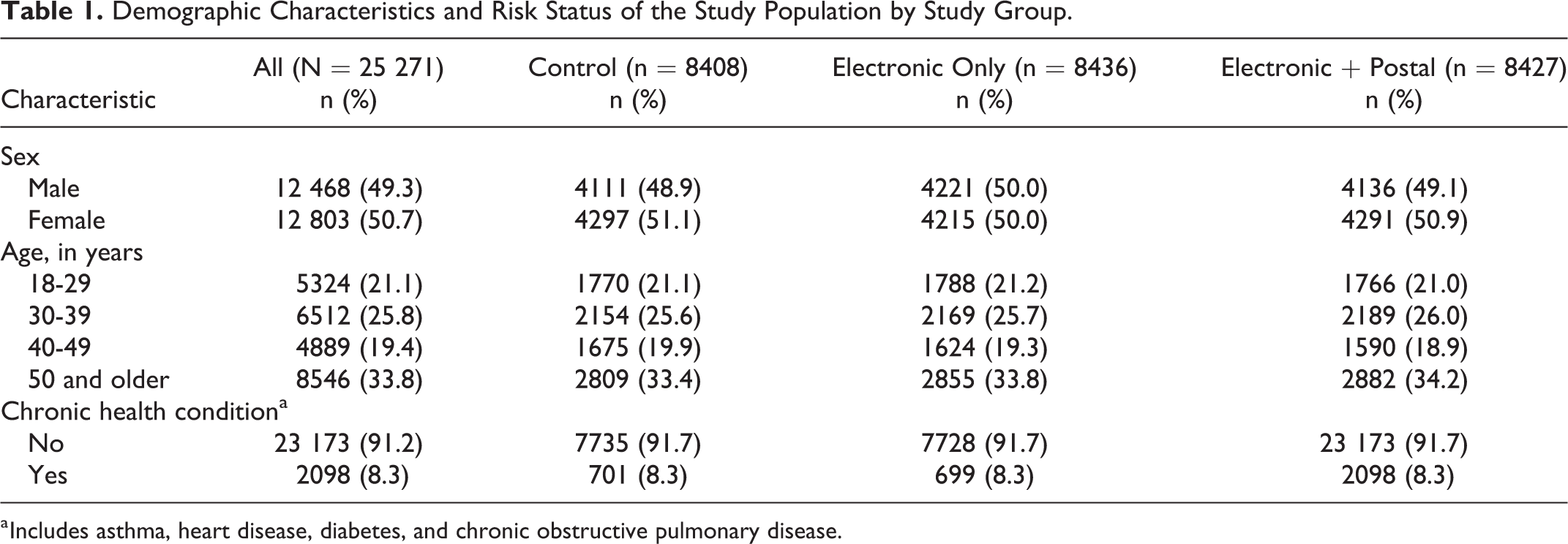
a Includes asthma, heart disease, diabetes, and chronic obstructive pulmonary disease.
Influenza vaccination rates and comparisons by group assignment and subpopulations are given in Table 2. By December 31, 2017, the influenza vaccination rate was 16.9% in the overall population, 15.8% in the control group, 16.6% in the electronic messages only group, and 18.3% in the electronic plus postal mail group. Vaccination rates were significantly higher in the electronic and postal mail group compared to both the control group (difference: 2.5%; 95% CI: 1.4-3.6; P < .001) and the electronic messages only group (difference: 1.6%; 95% CI: 0.5-2.8; P = .005). The vaccination rate among those in the electronic messages only group and those in the control group was not significantly different (difference 0.9%; 95% CI: −0.2 to 2.5; P = .13).
Influenza Vaccination Rates and Percentage Difference From Control and Between Intervention Groups by Sex, Age-Group, and Risk Status.
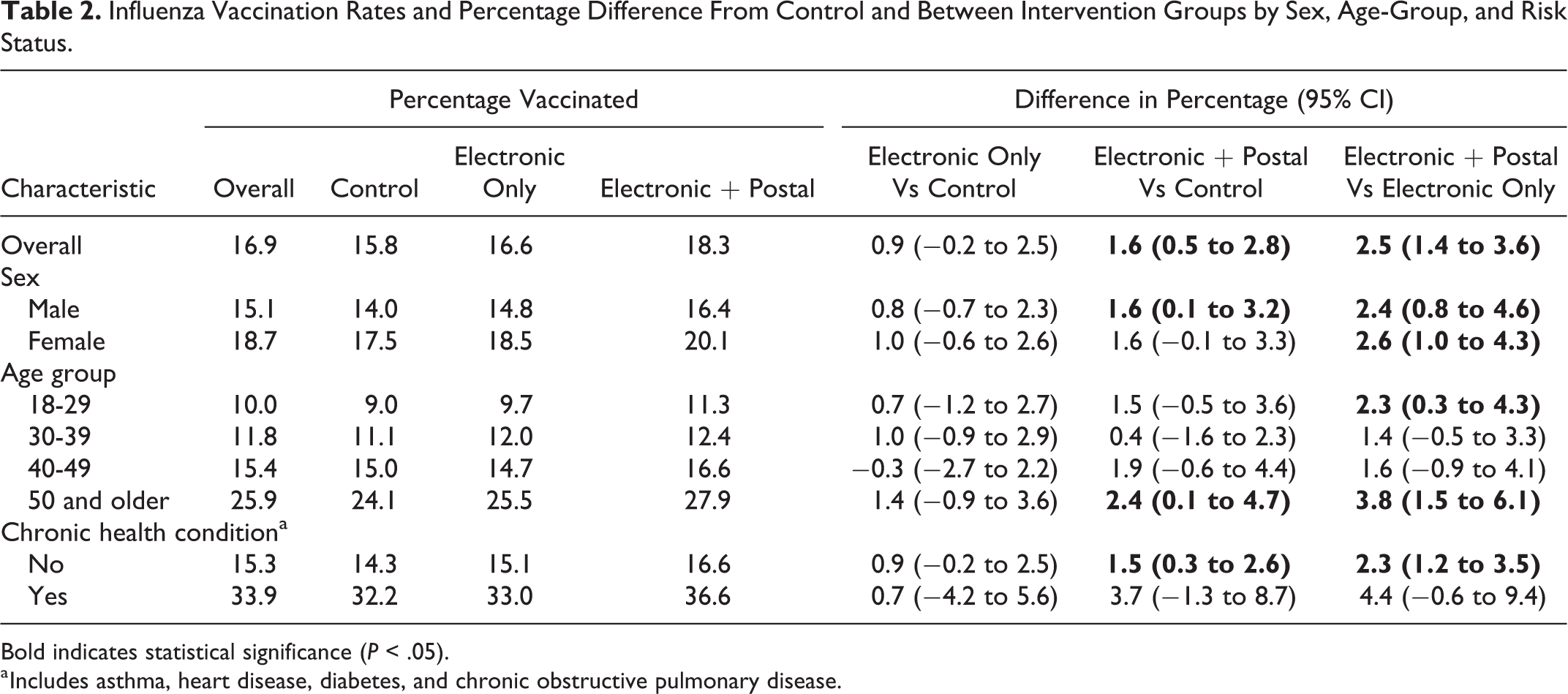
Bold indicates statistical significance (P < .05).
a Includes asthma, heart disease, diabetes, and chronic obstructive pulmonary disease.
Significant rate differences between electronic plus postal mail groups and control group were seen in the youngest age-group (18-29 years old; 11.3% vs 9.0%; difference: 2.3%; 95% CI: 0.3-4.3; P = .02) and the oldest age-group (50 years old or older; 27.9% vs 24.1%; difference: 3.8%; 95% CI: 1.5-6.1; P = .001) and among those without a chronic condition (16.6% vs 14.3%; difference: 2.3%; 95% CI: 1.2-3.5; P < .001; Table 2). The odds of receiving an influenza vaccine among those in the electronic plus postal mail group, adjusted for sex, age-group, and risk status was 1.20 (95% CI: 1.10-1.34) compared to the control group (Table 3).
Adjusted Odds Ratios and 95% Confidence Intervals for Receipt of Influenza Vaccination by December 31, 2017, by Study Condition, Demographics, and Risk Status.
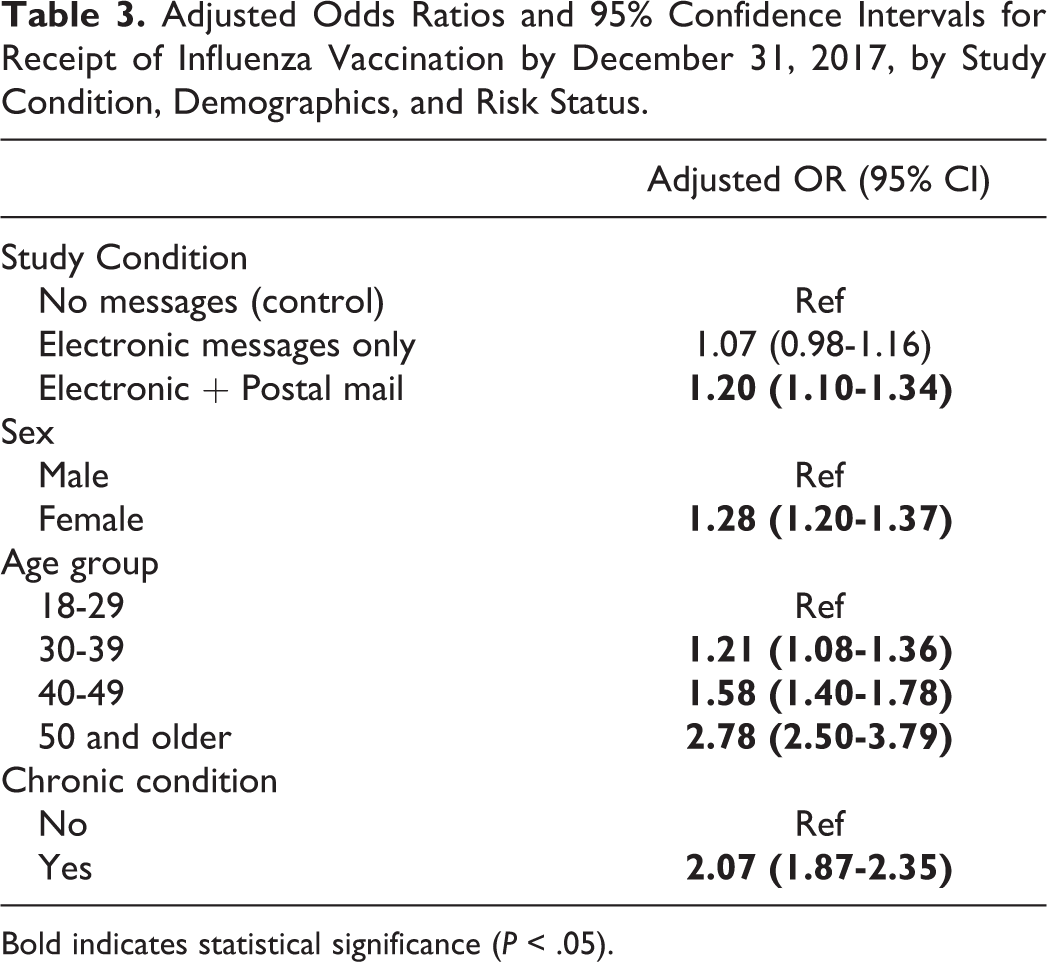
Bold indicates statistical significance (P < .05).
Discussion
Summary
This population-based, randomized controlled trial targeting an ACA plan population found that a combination of incentive plus messages delivered via text, e-mail, and postal mail generated a modest but significant positive effect on influenza vaccine rates. The postal mail component was essential to achieving this effect.
This study found an increase in influenza vaccination rates of 2.5 percentage points compared to the control condition. The studies included in the systematic reviews that support the Task Force recommendation of client reminder systems found that vaccination rates increased by a median of 11 percentage points among those who received reminders. 4 Several possible factors may have contributed to the smaller effect size in the current study.
One possible factor is the influence of the relatively low effectiveness of the 2017 to 2018 influenza vaccine, which was estimated to be 36%. 10 Many media outlets ran stories reporting low vaccine effectiveness, and early season reports found influenza vaccine coverage through November 2017 was down by 2.1% among all adults (3.7% among 18-49 year olds) compared to coverage estimates for the same time period in 2016. 11
It may also be the case that health-care advice sent by someone’s personal doctor is more likely to impact a person’s health behaviors than health-care advice from his or her health plan. However, given that younger populations are less likely to utilize health-care services than their older counterparts, 12 and therefore are less likely to receive messages delivered by health-care providers, utilizing channels other than health-care providers may be important to reach a younger population.
The smaller effect size in the current study relative to prior studies may also be explained in part by the overall low-risk status of the target population. People in a high-risk group may be more responsive to influenza vaccine messages than those who perceive themselves as healthy and not susceptible to influenza or serious complications from influenza. Two-thirds of the study population was younger than age 50 and over 90% did not have documentation of a chronic health condition that would put them at higher risk for influenza-related complications. Given this low-risk status, the group may not have felt particularly vulnerable to influenza, and therefore were less inclined to get vaccinated. Indeed, the overall vaccination rate in the study population by December 31, 2017, was just 16.9%.
The subpopulation analysis by age-group found that the intervention was effective among the oldest and the youngest age-groups, while no significant effect was seen in the 30 to 49-year-olds. It may be that the mechanism influencing the decision to obtain an influenza vaccination differed for the youngest group and the oldest age-group. The latter may have a greater perceived need to be vaccinated and therefore messages may have served as a nudge toward a behavior to which they were already inclined. By contrast, the younger group may have been the group most influenced by the existence of the $10 incentive. This explanation is speculative; no prior research on whether incentive effectiveness varied by age was found.
Limitations
Study limitations include the unavailability of sociodemographic data, the inability to assess the effect of the incentive on vaccine rates independent of the messages, and the lack of information on returned mail or bounced electronic messages. The inability to identify influenza vaccinations not billed to Sendero, such as those delivered at workplace or school influenza vaccine clinics and not submitted to health insurance, may have led to an undercount of the true vaccination rate. Finally, the small size of the geographic area within which participants lived limits generalizability beyond the central Texas area.
So What?
What is already known on this topic?
Vaccination reminder interventions have been shown to be effective at increasing vaccination rates in high-risk populations, and when delivered by health-care providers to their own patients.
What does this article add?
This study found that a combination of influenza vaccination promotion messages delivered via text, e-mail, and postal mail to a general population enrolled in an ACA plan generated a modest but significant positive effect on influenza vaccine rates. We also found that the postal mail component was essential for achieving this effect.
What are the implications for health promotion practice or research?
Existing evidence-based messaging strategies for influenza vaccination promotion have been tested primarily with higher risk populations. This study shows that these approaches can have measurable effects in a lower risk population. However, to reach the Healthy People 2020 influenza vaccination target of 70%, more research is needed to identify effective interventions for a general adult population.
Significance
Although the effect size found in this study was modest, an improvement in the population-level vaccination rate of 2.5% in a primarily low-risk, low-influenza vaccination population is of value. However, this study suggests that the existing evidence-based practices that have been successful in increasing influenza vaccination rates among higher risk groups may not be as effective in low-risk populations who are underrepresented in previous studies. To reach Healthy People 2020 goals, more research is needed to develop effective influenza vaccination promotion interventions for a general adult audience.
Supplemental Material
Supplemental Material, flu-vax-electronic-msgs_(3) - Promoting Influenza Vaccination Among an ACA Health Plan Subscriber Population: A Randomized Trial
Supplemental Material, flu-vax-electronic-msgs_(3) for Promoting Influenza Vaccination Among an ACA Health Plan Subscriber Population: A Randomized Trial by Eileen K. Nehme, Michelle Delphia, Eun Me Cha, Milton Thomas and David Lakey in American Journal of Health Promotion
Footnotes
Authors’ Note
The content is solely the responsibility of the authors and does not necessarily represent the official views of The University of Texas Health Science Center at Tyler or Sendero Health Plans.
Acknowledgments
The authors thank the leadership and staff at Sendero Health Plans who contributed time and effort for this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by Contract Number 2016-UT from Sendero Health Plans, a nonprofit community health plan in Central Texas.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.