
Abstract
Purpose:
To assess the efficacy of a food service implementation intervention designed to increase provision of foods consistent with nutrition guidelines on child consumption of fruit, vegetables, breads/cereals, meat/alternatives, dairy, and diet quality in care.
Design:
Exploratory cluster randomized controlled trial.
Setting:
Twenty-five childcare centers in New South Wales, Australia.
Sample:
Three hundred ninety-five children aged 2 to 5 years.
Intervention:
Centers were randomized to the intervention or control group. Intervention development was guided by the Theoretical Domains Framework and included securing executive support, provision of group training, resources, audit and feedback, and one-on-one support. The intervention was delivered across six months and the study was conducted between March and December 2016.
Measures:
Child diet was assessed by educators using a validated questionnaire modified for completion in childcare center.
Analysis:
Data were analyzed in SAS using generalized linear mixed models adjusted for clustering.
Results:
Children in the intervention group consumed significantly higher number of serves of vegetables (0.4 serves; P < .001), wholegrain cereals (0.7 serves; P = .02), and meat/alternatives (0.5 serves; P < .001), and had higher diet quality scores (10.3; P < .001).
Conclusions:
A food service intervention targeting the provision of food significantly improved child dietary intake in care. Such findings are relevant to health promotion practitioners responsible for supporting improvements in child diet.
Purpose
Dietary risk factors are one of the biggest contributors to premature death internationally. Among high income countries, low fruit and vegetable consumption and high sodium diets account for approximately 21% of deaths from ischemic heart disease and 11% of stroke. 1 Improving child dietary intake is recommended to reduce the burden associated with poor diet as child dietary pattern tracks into later life. 2 –4
Childcare centers are a recommended setting to deliver public health nutrition interventions to improve child diets as they provide access to the majority of young children. In Australia, 52% of children aged up to 6 years attend formal care at a preschool or long day care center for an average of 18 hours per week. 5,6 Approximately 30% of childcare centers in Australia provide food onsite, 7 where children can consume up to 67% of their daily dietary requirements. 5 For centers where food is provided onsite, menu planning and preparation of food and beverages are typically undertaken by an onsite cook. 8 Systematic reviews of trials undertaken in education and care settings including childcare centers and schools have found that modification of the food environment to increase availability of healthier food and beverages is associated with improvements to children’s dietary intake. 9,10 Such findings are consistent with the socioecological framework which posits that broader social and physical settings within the community can facilitate or promote healthy eating. 11
As such, in Australia, nutrition guidelines exist for childcare services and require that centers provide foods consistent with Australian dietary guidelines. 12 Despite this, cooks report a number of barriers to meeting these guidelines. Reported barriers include inadequate exposure to guidelines, concerns about child food preferences as well as challenges with modifying recipes to meet guidelines. 13 –16 Childcare cooks report that help with menu planning, providing appropriate recipes and making gradual changes to the menu would enable them to provide healthier food and beverages. 17
Given the potential benefits of improving provision of food in childcare, interventions that target cooks’ barriers to planning and preparing healthier meals represent a promising strategy for improving child diet. A previous nonrandomized trial in six childcare centers which included training workshops and monthly site visits to support cooks with preparing healthier foods reported that the intervention had a positive impact on consumption of saturated fat. 18 A recent systematic review of nutrition interventions in childcare centers however, identified no randomized controlled trials (RCTs) that have examined food service based implementation interventions. 9 Further, the impact of such an intervention on child dietary intake or quality has also not been explored in a RCT design. 9 We aimed to assess the efficacy of a theory-based multistrategy implementation intervention, targeting the food service of childcare centers, to improve child dietary intake and diet quality in care, compared to usual care.
Methods
Design
The study employed a repeat cross-sectional exploratory cluster RCT design and reports results from a subsample of 25 centers participating in a larger trial to improve implementation of nutrition guidelines. Nested studies represent an efficient way of assessing the impact of implementation of setting-based guidelines. 19,20 Repeat cross-sectional rather than cohort assessments were chosen as they are recommended to assess the impact of population level or settings-based interventions where the effect of the intervention is expected at the cluster level (in this study, child diet among children attending a childcare center exposed to the intervention) and where high attrition is expected (in this case, change of childcare rooms/centers). 21,22 Intervention and data collection procedures of the main trial are reported in detail in a published study protocol. 23 The primary outcome of the main trial was center menu compliance to nutrition guidelines for the sector and is reported in a separate publication. 24 Briefly, the main study found that services in the intervention were significantly more likely to have menus that provided serves of foods consistent with guidelines for fruit (odds ratio [OR]: 10.8, P = .0024), meat (OR: 8.3, P = .023), dairy foods (OR: 8.4 P = .006), and discretionary foods (OR: 17.8, P = .002). 24 Ethical approval was provided by the Hunter New England Human Research Ethics Committee (HREC; reference: 06/07/26/4.04) and the University of Newcastle HREC (reference H-2012-0321). The reporting of this study adheres to the Consolidated Standards of Reporting Trials guidelines for cluster trials. This trial was prospectively registered (ACTRN12615001032549).
Sample
In Australia, early childhood and education care consists of center-based (including long day care centers and preschools) and family-based care. Long day care centers usually operate more than 10 hours a day, while preschools typically have shorter operating hours (usually ranging from 9
Randomization and blinding
Overall, 54 childcare centers were recruited to the main trial. The randomization schedule for the main trial was prepared a priori by a statistician independent to conduct of the trial. Centers were randomized to the intervention or control group via block randomization (block size ranged between 2 and 6), using a central conceal random allocation process. Of these, 25 centers were approached in random order using a random number list generated in Microsoft Excel and invited to participate in the nested study. An information statement and consent form was mailed to centers approximately one week prior to a telephone invitation to participate in the trial. Centers consented to a one-day site visit and completion of pen and paper questionnaires by the nominated supervisors and cooks at baseline and follow-up. Centers participating in the nested evaluation also consented to completing child questionnaires reporting on child dietary intake and diet quality. The study was conducted as an open trial as it was not possible to blind the childcare center staff receiving the intervention. Outcome assessors were center educators and not blinded to intervention allocation. The study statistician undertaking the primary analyses was blinded to group allocation.
Intervention
Centers in the intervention group were offered a six month multistrategy implementation intervention to improve menu compliance with the NSW nutrition guidelines for childcare centers. These guidelines are outlined in the Caring for Children resource and requires childcare centers provide at least 50% of the recommended serves of the Australian Guide to Healthy Eating (AGHE) core food groups and no “discretionary” food to children each day. 26 Selection of trial strategies was informed by the Theoretical Domains Framework (TDF) 27 and based on extensive interviews with center cooks and managers regarding the barriers and facilitators to providing foods in line with guidelines. Specifically, implementation of the framework involved the following steps: (i) literature reviews; (ii) interviews using a validated TDF survey with childcare center staff, and (iii) observations of menu planning and food preparation processes. 23 Utilising this information, the identified barriers were mapped to TDF constructs, and implementation strategies recommended to address identified barriers were then selected. To be included, implementation strategies needed to be empirically supported as effective by systematic review evidence in childcare and other settings, and judged as feasible and acceptable to centers.
The selected strategies included: securing executive support at the commencement of the intervention via a face to face meeting with service managers and cooks, provision of group training, provision of resources, audit and feedback, and one-on-one implementation support provided by an experienced implementation support officer. The intervention was delivered in a staggered manner to all intervention centers from February 2016 to August 2016. An overview of the intervention content and delivery is provided in Table 1 and described in detail in the study protocol. 23
Summary of the Theoretical Domains Framework (TDF) Targeted Domains, Intervention Strategy and Detail.

aDefinitions were adapted from the Expert Recommendations for Implementing Change criteria.
Control
Centers allocated to the control group were mailed the Caring for Children resource which outlines the nutrition guidelines and received usual care from their local health district. Where support was requested, a feedback report outlining general menu compliance was provided to these centers.
Data collection procedures
Baseline data were collected following randomization (March 2016), with follow-up data collection undertaken approximately 6 to 8 months post baseline (October to December 2016). Center supervisor and cooks completed a brief pen and paper questionnaire at baseline and follow-up. Educators from the room with the majority of children aged 2 to 5 years, present on the day of the site visit, completed written questionnaires reporting on child age and sex and the usual dietary intake of the child attending care, over the past month. Educators were provided with 30 questionnaires per room and any educator present could complete these for children aged 2 to 5 years in the room on the agreed day of data collection. Previous trials undertaken by the research team have identified that approximately 23 children aged 2 to 5 years are present in a center room. As part of the data collection process, research assistants provided all participating educators with brief training on how to estimate serve sizes and complete the questionnaire and a supporting laminated pictorial resource outlining example serve sizes to help with estimating child food intake. Educators were asked to refer to the resource and also service menus to facilitate recall when completing the questionnaires. Educators were asked to return the questionnaires to research assistants present on the day or where not possible return the questionnaires to an allocated data collection box, via reply paid envelopes, or to a member of the research team at the end of the data collection period.
Measures
The outcomes for this nested study were the: (1) usual serves of AGHE core food groups consumed by children which includes: (i) vegetables and legumes/beans; (ii) fruit; (iii) wholegrain cereal and breads; (iv) lean meat and poultry, fish, eggs, tofu, seeds, and legumes; (v) milk, yoghurt, cheese, and alternatives, and (2) child diet quality, while in care.
All outcomes were assessed using a questionnaire developed for the purpose of this study. The questionnaire was adapted from a 38-item short food survey previously validated in a sample of Australian preschool aged children. 37 This original measure was identified in a recent systematic review of short dietary measures as a valid and reliable tool for assessing young children’s dietary intake. 38 The research team consulted with the developers of the original tool and minor modifications were made to support completion by childcare educators, increase clarity, and to address previous limitations. Reporting of child dietary intake by educators has previously been undertaken in a number of studies. 39,40 The modified tool consists of 47 items asking center educators to record the frequency and portion sizes of each AGHE food group, number of discretionary foods, the variety of foods, and the quality of foods (ie, wholemeal/wholegrain cereals, lean meats) consumed by an individual child during the duration of care. A post-hoc validation study of the modified food frequency questionnaire compared to direct observations by 2 to 3 research assistants per service across randomly selected days (gold standard for the setting) found between 53% (fruit) and 93% (vegetables) agreement for consumption of AGHE food groups in line with guidelines for the setting (manuscript in preparation).
Consumption of AGHE core food groups
Usual serves of AGHE core food groups were assessed using 28-items from the questionnaire assessing frequency (times per day/week or doesn’t eat) and portion size (1/2 portion, 1 portion, 2 portion, or doesn’t eat) consumed of each core food group. Food intake data were converted to usual servings of food groups per day consumed in care.
Diet quality
Diet quality was assessed using all 47-items in the questionnaire and comprised of the following nine components: usual serves of each of the five AGHE core food groups, number of extra/discretionary foods, healthy fats/oils, beverages, and diet variety. Similar to the original tool each component, except for extra/discretionary, was allocated 10 points, where a maximum score of 10 indicates optimal intake and a score of 0 indicates no intake of a particular food group. The extra/discretionary component was allocated 20 points with inverse scoring, where no serves of such foods represented optimal intake (20 points) and 0 represented excessive intake. Total diet quality was calculated by summing the scores from each component with a total score of 100, where a higher score represented better diet quality.
Center and cook characteristics
Center supervisors reported on their center operational characteristics including the total number of children enrolled; postcode; whether children of Aboriginal or Torres Strait Islander background are enrolled; and hours of operation. Childcare center cooks reported on their gender, age, years working in current position, years employed in the childcare setting, number of hours worked per week, and qualifications. Questionnaire items have been used in previous Australian surveys of center managers conducted by the research team. 41,42
Sample size calculation
Retrospective sample size calculations were undertaken and estimated that a sample of 12 centers per group, with approximately 20 children per cluster, allowing for 15% of centers loss to follow-up would provide 80% power to detect a difference of at least 50% of a standard deviation difference between the groups for all outcomes, with a 2-sided α of .025 allowing for multiple outcomes and assuming an intracluster correlation coefficient (ICC) of 0.1. 7 This would equate to between 0.2 to 0.6 serves of each of the core AGHE food groups; and a four point difference in total diet quality score. Such an effect size is similar to that identified in other intervention targeting preschool aged children. 43
Analysis
Statistical analyses was undertaken by a statistician independent to the project team (author C.L.) using SAS version 9·3 (SAS Institute, Cary, North Carolina) in August 2017. Center postcodes ranked in the bottom 50% of NSW according to Socioeconomic Indices for Areas were classified as being least advantaged. Only children who attended for 2 or more days a week (n = 476 [90%]) were included in the analysis as the outcome related to usual consumption in care. For the main outcomes of the current article (child dietary intake as reported via educator completed questionnaire), a complete case analyses was performed using all available data (without imputation). An intention to treat analysis using multiple imputation for missing data at baseline and follow-up was also undertaken using the MI procedure in SAS. Group differences for all outcome data were assessed through a group by time interaction using generalized linear mixed models, adjusting for clustering within centers. Statistical significance was defined as P-values less than .025 to account for multiplicity.
Results
Fifty-four centers (60% of eligible) were randomized into the larger study. Of these, 28 centers were randomly selected to participate in assessment of child diet (15 intervention, 13 control). At baseline, 13 intervention and 12 control centers (89% retention rate) completed questionnaires, resulting in 220 children in the intervention group and 175 children in the control group (see Figure 1). At follow-up, 13 intervention and 11 control centers completed questionnaires, which included 259 children in the intervention and 216 in the control group. A significant difference in child age was found among those children excluded from analysis compared to those included (t (932) = −2.35; P = .02), however there were no differences in child sex (χ2(919) = 0.04; P = .81). Comparison of children with and without at least one item missing on the questionnaire found no significant differences in child age (t (847) = 1.32; P = .19) or sex (χ2(832) = 0.006; P = .94). The operational characteristics of participating childcare centers, cooks, and children at baseline are specified in Table 2.

Participant flow through the trial and analyzed for the primary outcome. Data were analyzed using separate linear mixed models, adjusted for baseline values and clustering at the childcare level. Main findings are reported using intention to treat with multiple imputation analysis.
Demographic Characteristics of Childcare Centers, Cooks, and Children at Baseline (Data Collected January to February 2016).
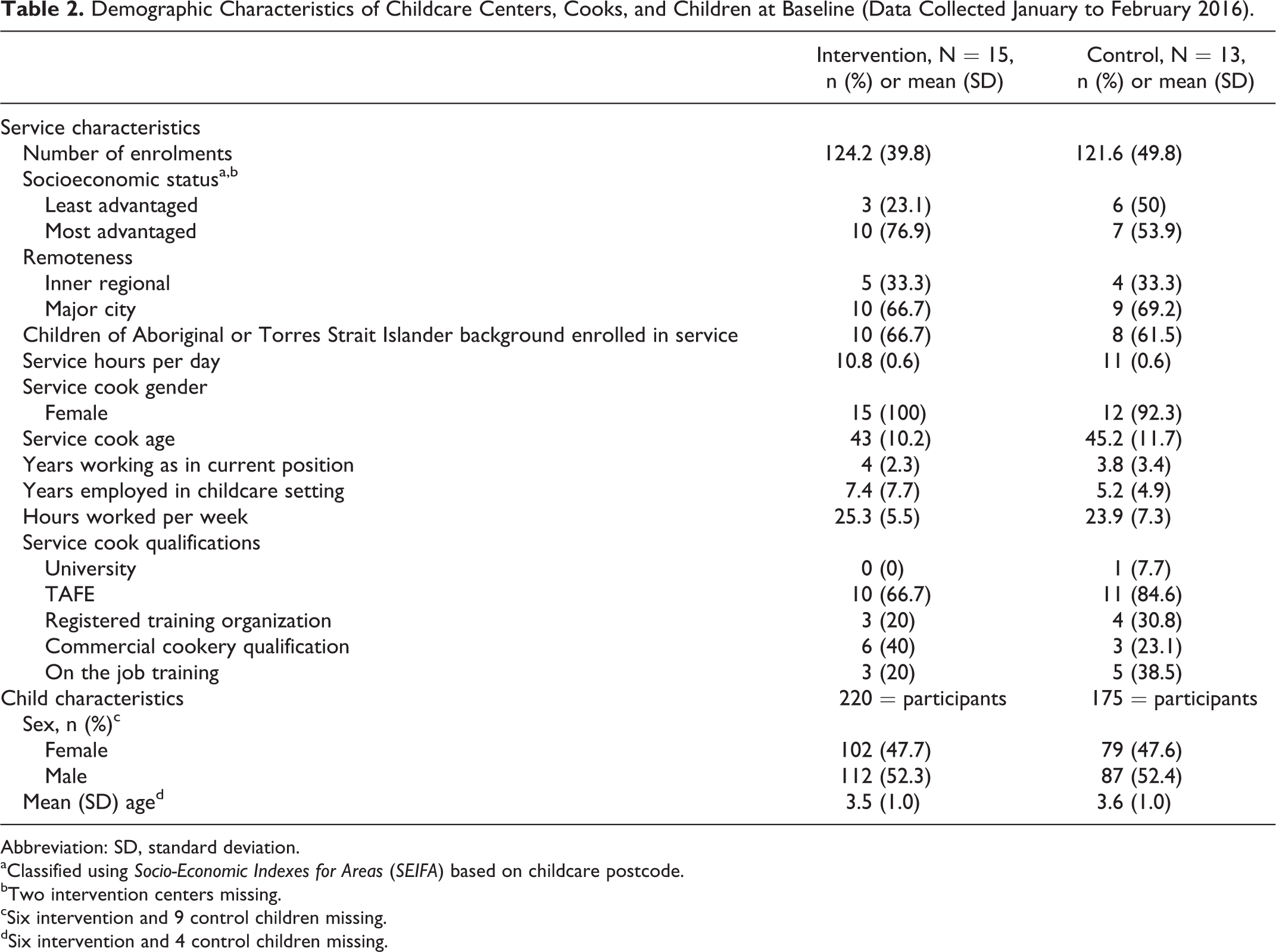
Abbreviation: SD, standard deviation.
aClassified using Socio-Economic Indexes for Areas (SEIFA) based on childcare postcode.
bTwo intervention centers missing.
cSix intervention and 9 control children missing.
dSix intervention and 4 control children missing.
Consumption of AGHE Food Groups
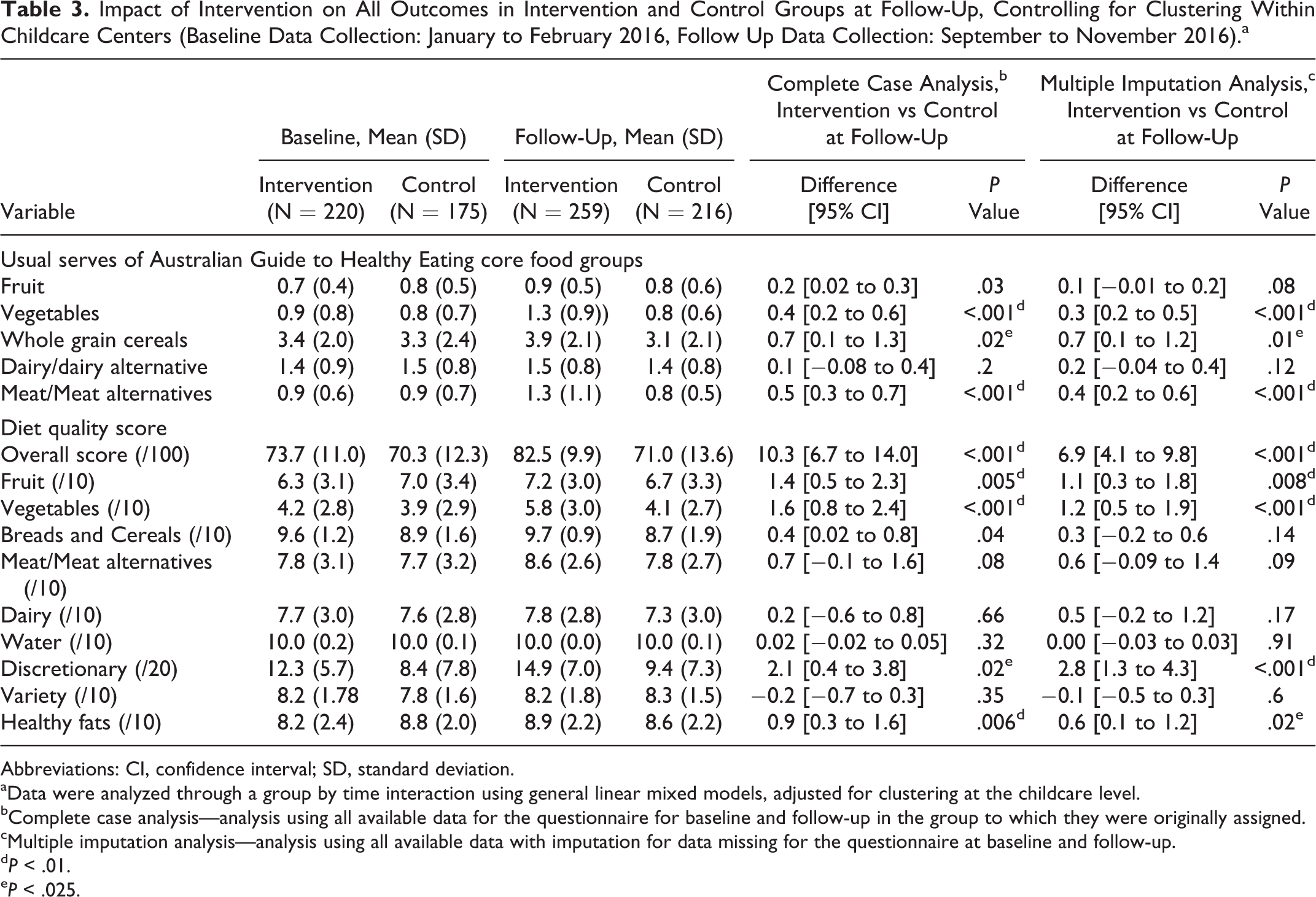
Children in intervention centers had significantly higher consumption of vegetables (mean difference: 0.4 [95% confidence interval [CI]: 0.2-0.6]; P < .001), wholegrain cereals (mean difference: 0.7 [95% CI: 0.1-1.3]; P = .02), and meat/meat alternatives (mean difference: 0.5 [95% CI: 0.3-0.7]; P < .001) while in care (see Table 3). There were no significant differences in serves of dairy and fruit items consumed.
Impact of Intervention on All Outcomes in Intervention and Control Groups at Follow-Up, Controlling for Clustering Within Childcare Centers (Baseline Data Collection: January to February 2016, Follow Up Data Collection: September to November 2016).a
Abbreviations: CI, confidence interval; SD, standard deviation.
aData were analyzed through a group by time interaction using general linear mixed models, adjusted for clustering at the childcare level.
bComplete case analysis—analysis using all available data for the questionnaire for baseline and follow-up in the group to which they were originally assigned.
cMultiple imputation analysis—analysis using all available data with imputation for data missing for the questionnaire at baseline and follow-up.
dP < .01.
eP < .025.
Diet Quality Scores
There was also a significant difference between groups in terms of total diet quality scores (mean difference: 10.3 [95% CI: 6.7-14.0]; P < .001) which could be attributed to improvement in scores for the following components: fruit (mean difference: 1.4 [95% CI: 0.5-2.3]; P = .005), vegetables (mean difference: 1.6 [95% CI: 0.8-2.4]; P < .001), discretionary foods (mean difference: 2.1 [95% CI: 0.4-3.8]; P < .02), and healthy fats (mean difference: 0.9 [95% CI: 0.3-1.6]; P = .006; see Table 3). There were no significant differences for the other domains. No changes in statistical significance were observed in the multiple imputation analysis for all outcomes.
Discussion
This study found that a theory-based multistrategy implementation intervention targeting the food service of childcare centers to improve nutrition guideline compliance resulted in significant improvements to child usual consumption of vegetables, cereals, and meat/meat alternatives in care at 6-months follow-up. Child diet quality was also significantly higher in the intervention group at follow-up. Findings from this trial suggest that interventions to support center provision of food in line with nutrition guidelines can improve child diet in care.
The size of the intervention effect on child consumption of vegetables is larger than that previously reported in other effective childcare-based studies employing multistrategy interventions (0.19-0.25 serves). 44,45 The intervention also had a positive impact on improving consumption of meat/meat alternatives and wholegrain cereals, providing a way of addressing previously reported deficits in preschool-aged children’s dietary intake that include low consumption of vegetables and meat/meat alternatives, 46 as well as low levels of dietary fibre. 47 The intervention also had a positive impact on child diet quality (10 point difference in scores between groups) an outcome which has not previously been explored in this setting. While we are unable to compare findings from this study with other studies, improvement in diet quality scores suggests that intervention also had a positive impact on variety and quality (unprocessed, wholegrains, healthy fats) of foods consumed. A systematic review of diet quality scores in children reported some association between overall diet quality and overweight and obesity and cardiovascular markers including blood pressure. 48 Findings from our main trial identified significant improvements in childcare center’s provision of foods in line with dietary guidelines. 24 Such findings together with that identified in the current study suggests that food-service based interventions to improve implementation of dietary guidelines in childcare centers could significantly improve the public health nutrition of children.
Findings from this study also support government investments in training and supporting food service staff to provide food in line with setting nutrition guidelines. While the intervention strategy employed in this study provides one potentially effective model of support, it was heavily reliant on face-to-face training of cooks and center managers and required ongoing in-person and telephone support contact to do so. Although effective, the provision of such support across an entire population of centers, including those in rural or remote locations could be cost prohibitive. Future studies utilising such multistrategy interventions should incorporate systematic methods to collect process data surrounding feasibility, and uptake to better understand the potential contribution of individual intervention components to outcome. Future interventions to investigate more scalable or lower resource means of improving provision of food, as well as investigations of cost effectiveness of such intervention are also warranted. For example a web-based training and decision support tool may provide a useful adjunct or alternative to face-to-face implementation support. 49 While providing evidence to support initial improvements in child dietary intake, future research investigating the longer term impact of this intervention is recommended given potential attenuation of long-term effects of interventions relying primarily on training and face-to-face support.
Study Limitations
These findings should be interpreted in light of a number of limitations. Firstly, the outcome assessors were center educators and not blinded to group allocation. While educators were not specifically targeted by the intervention, this could have resulted in detection bias where centers were more likely to report favorable outcomes due to receipt of the intervention. Second, this trial was undertaken in one jurisdiction in NSW, Australia, as such the generalizability of findings may be limited. Third, there was a significant amount of missing data for the questionnaire with approximately 21% of children at baseline or follow-up, missing at least one item on the record. However, no significant differences in child age or gender were found among children with and without missing data and multiple imputation and intention to treat analysis did not result in any changes to statistical significance of trial outcomes. Fourth, outcomes related to diet quality were not prospectively registered which could have resulted in some selective outcome reporting. Fifth, the measures were developed and validated for children attending care in NSW childcare centers, and as such is unlikely to be generalizable to other settings. Additionally, the self-reported dietary measure required childcare educators to recall child diet over the past month and as such is subject to recall bias. Further, initial findings from our validation study found lower level of agreements for food groups including fruit and dairy, and as such findings related to those food groups need to be interpreted with caution. Lastly, this study did not assess intervention uptake among childcare centers, limiting the ability to explore between-center variability, usefulness, and impact of the various components on outcomes.
The study provides initial evidence to support the efficacy of a multistrategy implementation intervention targeting childcare food service in improving child dietary intake. These findings suggest that greater investment to support childcare centers with improving food provided on their menu may be a promising strategy to improve child public health nutrition.
So What?
What is Already Known on This Topic?
Childcare services are a recommended setting to implement dietary guidelines to improve children’s diet. Data internationally suggest that cooks and childcare staff face a number of challenges with providing healthier foods consistent with guidelines. There have been few previous randomized controlled trials assessing the impact of the implementation of nutrition guidelines on child diet.
What Does This Article Add?
The article describes the efficacy of a childcare food-service based implementation intervention that was effective in improving children’s dietary intake. The intervention consists of securing executive support, training, audit and feedback, provision of resources and provision of implementation support.
What Are the Implications for Health Promotion Practice or Research?
This study provides health promotion staff with a support strategy that can be utilized when working with childcare staff and/or cooks responsible for planning menus.
Footnotes
Authors’ Note
This study was conducted according to the guidelines laid down in the Declaration of Helsinki and all procedures involving human subjects were approved by the Hunter New England Human Research Ethics Committee (HREC; reference: 06/07/26/4.04) and the University of Newcastle HREC (reference H-2012-0321). Written informed consent was obtained from all subjects. Trial registration: ACTRN12615001032549: (![]() ).
).
Acknowledgments
The authors wish to acknowledge Danielle Wilton, Nicole Pond, Emma Bone, and Maryann Falkiner for their support in data collection and intervention delivery.
Author Contributions
Substantial contributions to conception and design (S.Y., L.W., J.W., M.F.), data acquisition (T.W., M.F., K.S.), analysis and/or interpretation (S.Y., A.G., C.L.); drafting the article (S.Y., A.G.), revising it critically for important intellectual content (all authors); and final approval of the version to be published (all authors).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Hunter New England Population Health and University of Newcastle Australia provided in-kind support conduct to undertake the trial. Intervention delivery was undertaken as part of usual service provided within Hunter New England Population Health. Infrastructure support was also provided by Hunter Medical Research Institute. Dr Sze Lin Yoong receives salary support from an Australian Research Council Discovery Early Career Researcher Award (DE170100382). Dr Meghan Finch is a clinical research fellow funded by Hunter New England Population Health and the Health Research and Translation Centre, Partnerships, Innovation and Research, Hunter New England Local Health District. Associate Professor Luke Wolfenden receives salary support from a National Health and Medical Research Council (NHMRC) Career Development Fellowship (Grant ID: APP1128348) and Heart Foundation Future Leader Fellowship (Grant ID: 101175). The contents of this manuscript are the responsibility of the authors and Hunter New England Clinical Research Fellow and do not reflect the views of the NHMRC.