
Abstract
Purpose:
To estimate changes in self-reported health and psychosocial factors associated with a 12-week sedentary behavior intervention for older adults.
Design:
Exploratory secondary analysis of pilot randomized controlled trial.
Setting:
Kaiser Permanente Washington
Subjects:
Sixty adults aged 60 to 89 with body mass index ≥30 kg/m2.
Intervention:
Participants were randomized to the I-STAND intervention or control group. I-STAND involved 6 coaching sessions, a study workbook, Jawbone UP activity tracker to prompt breaks from sitting, and activPAL feedback on objective sitting time.
Measures:
At baseline and 12-week follow-up, participants completed a survey with validated measures of self-reported health outcomes (depression, stress, memory/concentration, sleep, pain, ability to do daily activities, energy, and quality of life) and modified scales measuring psychosocial factors (perceived benefits/barriers, social support, self-efficacy, and sedentary habit strength) regarding sedentary behavior.
Analysis:
Generalized linear models assessed associations between group assignment and change in each self-reported health and psychosocial score, adjusting for baseline scores.
Results:
I-STAND participants demonstrated improvements in self-efficacy (β = 0.35, 95% confidence interval [CI]: 0.10 to 0.60) and reduced habit strength (β= −0.23, 95% CI: −0.42 to −0.04) compared to control participants. There were no significant differences in self-reported health outcomes, although power was limited in this exploratory analysis.
Conclusion:
A sedentary behavior reduction intervention for older adults resulted in improvements for some psychosocial factors. Health outcomes may require longer than 12 weeks to observe improvements.
Keywords
Purpose
Older adults represent the most sedentary age-group, sitting 8 to 11 h/d. 1 Sedentary behavior (SB) is defined as activities spent exerting minimal energy (<1.5 Metabolic equivalent tasks (METs)) while seated or lying down. 2 Sedentary behavior has emerged as a risk factor for health distinct from physical activity (PA) and associated with mortality and chronic conditions in older adults. 3 To address this risk, several pilot studies have demonstrated feasibility of reducing SB among older adults. 4 –10
However, it is unknown whether an SB intervention impacts indicators of self-reported health such as functional and mental health that are important to healthy aging. 11 Emerging evidence on sedentary older adults suggests that functional and mental health outcomes may vary. 12,13 Two systematic reviews found SB generally associated with poorer mental health; however, cognitively engaging sedentary activities such as reading and computer use were associated with better cognitive functioning. 12,13 The majority of these findings were observational, highlighting the need for SB interventions to evaluate changes in functional and mental health outcomes that are important to healthy aging. 11
Further, unlike PA interventions, 14 there is little information about potential mechanisms specifically for SB intervention effectiveness. No studies have examined whether potential psychosocial mediators such as self-efficacy, decisional balance, sedentary habit strength (automatic nature of ingrained sitting habits), and social support are impacted by an SB intervention and could be driving observed changes in SB patterns. Therefore, this study examined whether a pilot 12-week SB intervention changed self-reported health and psychosocial outcomes for sedentary older adults.
Methods
Design
This exploratory secondary analysis uses data from a pilot randomized controlled trial conducted at Kaiser Permanente Washington (KPWA) Health Research Institute, between February 2016 and February 2017. Research activities were approved by the institutional review board of KPWA. Detailed study methods can be found in the published protocol. 15
Sample
Older adults were recruited from KPWA membership panels to participate in a 12-week SB intervention. Using electronic health records, we identified potentially eligible participants (aged 60-89, baseline body mass index [BMI] 30-50 kg/m2, not residing in long-term care or skilled nursing, and no diagnosis of dementia or serious mental or potentially terminal illness). Participants were excluded if they reported during telephone screening that they were unable to stand, walk 1 block, were participating in another intervention study, sat <6 h/d, could not communicate by phone, or could not speak and read English. Written informed consent was collected at baseline, and participants were compensated $50 per visit at in-person baseline and follow-up assessments.
Interventions
I-STAND
The I-STAND intervention was informed by social–cognitive theory, 16 the ecological model, 17 and habit formation theory. 18 Participants randomized to I-STAND worked with health coaches to reduce SB by discussing the health benefits of reducing SB, setting personalized goals, problem-solving barriers, modifying home and work environments, and using reminder strategies to prompt sitting breaks. Participants received 2 in-person health coach visits and 4 biweekly calls over 12 weeks. Participants received study workbooks, Jawbone UP wristbands programmed to gently vibrate after 15 minutes of inactivity, and feedback charts summarizing activPAL data (objectively measures SB) collected at baseline and weeks 1, 2, and 6. 15
Healthy Living
Participants randomized to the control condition received a self-study program that included a workbook on age-appropriate topics (e.g., fall safety, urinary incontinence, managing medications), 1 in-person health coach session, and 5 biweekly mailings with self-directed goal sheets.
Measures
Sociodemographic characteristics, self-reported health outcomes, and psychosocial factors were measured using baseline and follow-up surveys. Validated scales assessed self-reported health outcomes. For the following measures, high scores indicate worse health: depressive symptoms (Patient Health Questionnaire-8), 19 perceived stress (Perceived Stress Scale), 20 lapses in memory and concentration (Cognitive Failures Questionnaire), 21 sleep disturbance (Patient-Reported Outcomes Measurement Information System [PROMIS]–short form), 22 and pain intensity (PROMIS). 23 For the following measures, high scores indicate better health: ability to do daily activities using lower extremity function (Late Life Function and Disability Instrument: Function Component), 24 energy (Short Form-36), 25 and global quality of life (PROMIS). 26 Scoring protocol was followed for all validated measures.
At the time of this study, no validated measures existed for assessing older adult psychosocial factors specifically for SB. Therefore, measures were adapted from validated PA measures of the same psychosocial constructs. For all measures, high scores indicate high levels of the measured construct: perceived benefits and barriers (Exercise Benefits/Barriers Scale 27 with sedentary-specific additions), social support (Social Support and Exercise Survey 28 ), self-efficacy (Patient-centered Assessment & Counseling for Exercise survey [PACE] 29 ), and sedentary habits (PACE 29 and Self-Report Habit Index 30 ). Response options for all psychosocial measures ranged from 1 to 5, and scores were averaged across items for interpretability. Item descriptions and internal consistencies (Cronbach α) 31 are provided in Supplemental Appendix A.
Analyses
Descriptive statistics summarize baseline characteristics overall and by randomization group. Complete case analysis resulted in different analytic sample sizes for each outcome. Generalized linear models assessed difference in mean change from baseline to 12 weeks between intervention and control groups for each outcome, adjusted for baseline scores of the dependent variable. To facilitate comparison of the magnitude of estimated intervention effects across the various outcomes that are measured on different scales, and for comparison with other studies, standardized effect sizes (Cohen d) were also calculated for each outcome. 32 Effect sizes were interpreted as small (≤0.20), moderate (0.21-0.79), and large (≥0.80). 32 Analyses were conducted using STATA 15. 33
Results
Sixty participants were randomized to I-STAND (n = 29) or Healthy Living (n = 31). Participants were 68% female, 87% white, with an average age of 68, and average BMI of 36 (Supplemental Appendix B). One participant failed to complete the baseline survey. Six participants dropped out of Healthy Living (2 wanted the intervention, 2 cited health problems, 1 was too busy, and 1 did not specify a reason). No participants dropped out of the I-STAND intervention group. The resulting analytic sample included 53 participants.
For self-reported health outcomes, there were no significant differences in mean change scores between the intervention and control groups (Table 1). For psychosocial outcomes, I-STAND increased self-efficacy scores an average 0.35 points on a 5-point scale (β = 0.35, 95% confidence interval [CI]: 0.10 to 0.60; d = .78) and decreased SB habit strength by an average 0.23 points on a 5-point scale (β= −0.23, 95% CI: −0.42 to −0.36]; d= −0.69) compared to Healthy Living. There were no significant differences in mean change scores for social support, perceived benefits, or perceived barriers to reducing SB.
Standardized Effects and Mean Change in Self-Reported Health and Psychosocial Outcomes Measured at Baseline and 12 Weeks for Control (n = 31) and Intervention (n = 29) Participants Enrolled in a Sedentary Behavior Intervention Study.
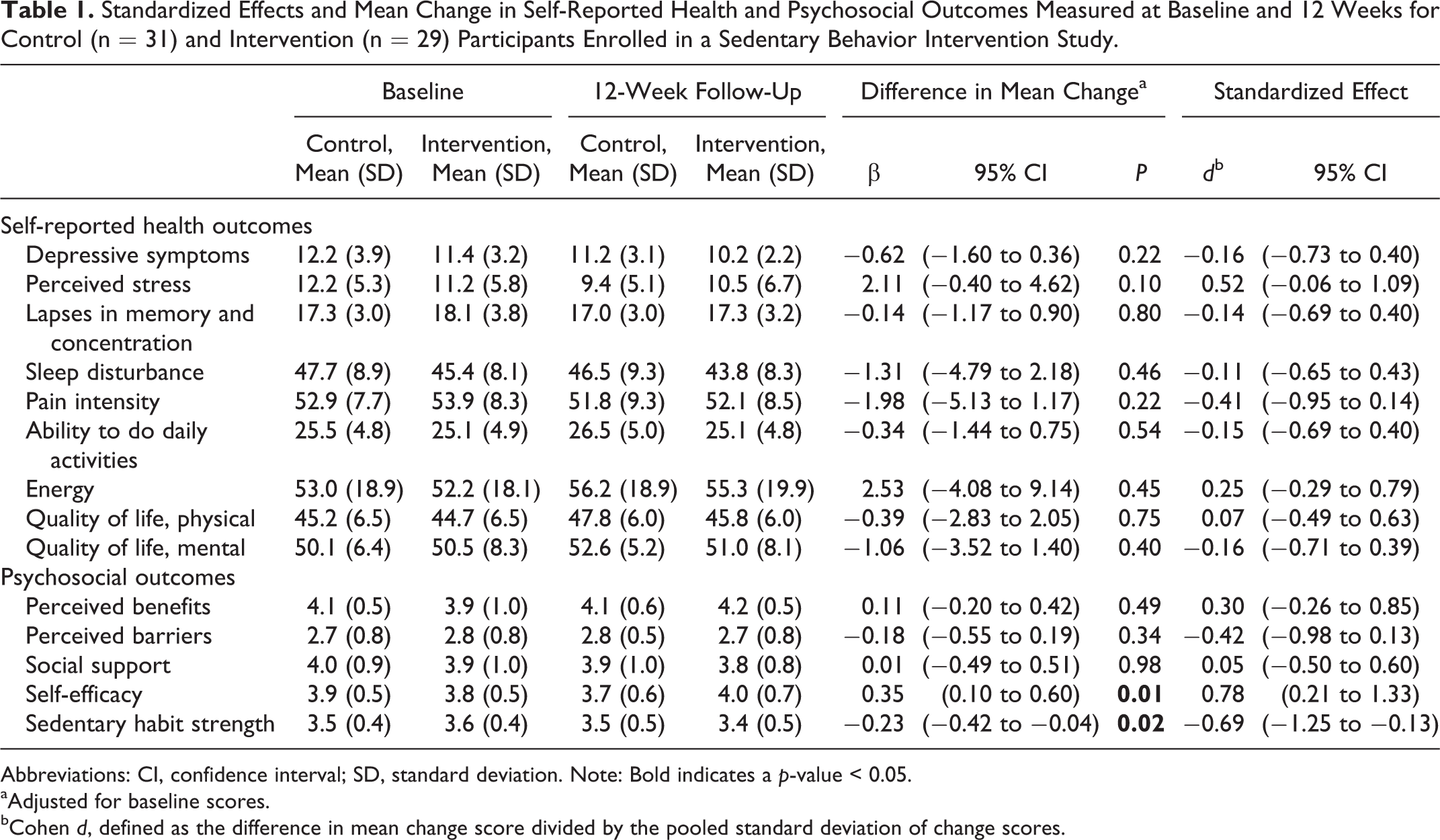
Abbreviations: CI, confidence interval; SD, standard deviation. Note: Bold indicates a p-value < 0.05.
aAdjusted for baseline scores.
bCohen d, defined as the difference in mean change score divided by the pooled standard deviation of change scores.
Discussion
A 12-week intervention to disrupt SB and reduce sitting time among older adults significantly improved self-efficacy to reduce sitting and reduced habit strength and automaticity of SB compared to a control group. However, there were no statistically significant changes for other psychosocial measures of social support, perceived benefits, or perceived barriers. Although the direction of change for most self-reported health outcomes suggests improvement in the I-STAND group, analyses found no significant change.
Among older adults with high BMI—for whom PA is very low 10 —confidence to reduce SB improved. In fact, I-STAND’s effect on change in self-efficacy (d = 0.78) was stronger than the average effect of PA interventions (d = 0.37) included in a systematic review of 24 intervention studies on PA self-efficacy. 14 Sedentary behavior reduction may be more feasible than PA for this population.
Findings suggest the importance of including intervention components that address strong sedentary habits. Because SB reduction needs to occur frequently, throughout the day, the automaticity of sitting must come under conscious decision-making processes to disrupt automatic habits. 18 This differs from approaches in PA interventions, whereby researchers typically promote single bouts of PA. I-STAND’s moderate effect on changes in habit strength (d = −0.69) suggests that having a variety of reminder strategies to prompt breaks from sitting can help older adults reduce sedentary habits.
More research is needed to understand the impact of an SB intervention on changes in subsequent functional and mental health outcomes. The finding of no significant changes in self-reported health is in contrast to cross-sectional studies that have found SB associated with poorer mental health and consistent with one longitudinal study that found no association with mental health. 13 Timing/temporality and a possible bidirectional relationship must be considered when studying the relationship between SB and mental health. Our findings suggest that sitting less does not have a potent or quick impact on self-perceived health status. It may be that standing more does not meaningfully impact self-reported health or that 12 weeks is insufficient for health improvements to occur. Changes in self-reported health may also depend on the magnitude of change or whether SB was replaced with light PA versus standing only.
This study has several limitations. First, as a pilot trial, the sample size was not selected to detect significant differences in secondary outcomes. However, estimated effects provide important information regarding potential intervention impact. Second, many outcomes were considered in this exploratory analysis, raising the possibility of type 1 errors and spurious findings. Third, validated instruments assessing psychosocial outcomes for SB do not currently exist, so psychosocial items were adapted from PA questionnaires. Fourth, there was differential dropout by group, which may have biased findings toward the null if those who dropped out of the control group were less healthy than those who did not drop out. Finally, participants were predominantly white, female, and well-educated older adults; thus, results may not generalize to other populations.
Study strengths include a highly sedentary population that has multiple chronic conditions. This is the first study to assess self-reported health and psychosocial outcomes related to an SB intervention in older adults from a randomized controlled trial.
Findings from this study make important contributions to the emerging field of SB research and have implications for sedentary older adults with high BMI. Future studies with larger samples are needed to confirm findings. Future studies should explore whether psychosocial factors mediate the relationship between an SB intervention and objectively measured SB.
So What
What is already known on this topic?
Older adults are the most sedentary age-group. Sedentary behavior (SB) interventions are feasible and effective at reducing SB for older adults, but little is known about mechanisms for intervention effectiveness and whether SB interventions impact functional and mental health important to healthy aging.
What does this article add?
An SB intervention improved confidence to reduce sitting time and reduced the strength and automaticity of sedentary habits. Improvements for health outcomes may require a longer follow-up period to observe changes.
What are the implications for health promotion practice or research?
Understanding effective mechanisms for reducing SB will be important for designing future trials. Larger studies that follow older adults over a longer period are needed to better understand impact of SB on health.
Supplemental Material
Supplemental Material, Supp_file_1_AJHP - Changes in Self-Reported Health and Psychosocial Outcomes in Older Adults Enrolled in Sedentary Behavior Intervention Study
Supplemental Material, Supp_file_1_AJHP for Changes in Self-Reported Health and Psychosocial Outcomes in Older Adults Enrolled in Sedentary Behavior Intervention Study by Theresa E. Matson, Melissa L. Anderson, Anne D. Renz, Mikael Anne Greenwood-Hickman, Jennifer B. McClure and Dori E. Rosenberg in American Journal of Health Promotion
Supplemental Material
Supplemental Material, Supp_file_2_AJHP - Changes in Self-Reported Health and Psychosocial Outcomes in Older Adults Enrolled in Sedentary Behavior Intervention Study
Supplemental Material, Supp_file_2_AJHP for Changes in Self-Reported Health and Psychosocial Outcomes in Older Adults Enrolled in Sedentary Behavior Intervention Study by Theresa E. Matson, Melissa L. Anderson, Anne D. Renz, Mikael Anne Greenwood-Hickman, Jennifer B. McClure and Dori E. Rosenberg in American Journal of Health Promotion
Footnotes
Acknowledgments
The authors gratefully acknowledge the participants of the I-STAND study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the National Institutes of Health (R21 AG043853; Rosenberg, PI).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.