
Abstract
Purpose:
To estimate the effects of stress on hypertension and high cholesterol with a focus on Million Hearts priority populations.
Design:
A population-based cross-sectional survey on cardiovascular health and its risk factors.
Setting:
Million Hearts cardiovascular community screenings
Sample:
Deidentified data were collected on a convenience sample of 59 798 participants.
Measures:
Self-reported stress score using the Perceived Stress Scale-4 (PSS-4), blood pressure, and total cholesterol.
Analysis:
Descriptive statistics were used to estimate the prevalence of high stress (PSS-4 score ≥ 9), prehypertension or hypertension, and elevated total cholesterol. Multiple logistic regression modeling was used to estimate the effect of stress on the risk of elevated blood pressure and total cholesterol.
Results:
Twenty-four percent of the participants had high stress. Younger participants had an increased prevalence of high stress than older participants (28% vs 20%, P < .001). African Americans had a high prevalence of stress (26.4%), prehypertension or hypertension (65.4%), and elevated total cholesterol (48.6%). Compared to those with low stress, high stress was associated with significant higher risks of having prehypertension/hypertension (odds ratio [OR] = 1.40, 95% confidence interval [CI] = 1.28-1.53) and elevated cholesterol (OR = 1.53, 95% CI = 1.41-1.66).
Conclusions:
Stress needs to be routinely identified and treated, especially in Million Hearts priority populations. More research is needed in designing culturally sensitive and effectively tailored interventions relative to both stress and disease management.
Purpose
Cardiovascular disease (CVD) is the leading cause of death for both men and women, yet it is largely preventable. Million Hearts is a national initiative with the goal of preventing 1 million heart attacks and strokes. 1 In 2018, Million Hearts identified a key focus area to improve outcomes in priority populations. These priority populations include Black/African Americans and 35- to 64-year-olds due to rising event rates. 1 The initiative has primarily focused on 4 evidence-based, cardiovascular prevention strategies called the “ABCS” of care: ‘A’ for appropriate aspirin therapy, ‘B’ for blood pressure control, ‘C’ for cholesterol management, and ‘S’ for smoking cessation. 1 Stress is not included as part of the “ABCS” of care in Million Hearts.
The objectives of this study were to estimate the prevalence of cardiovascular health risks and stress in a large sample of US adults and in 2 of Million Hearts priority populations, examine their relationships, and review clinical implications to improve cardiovascular population health assessment.
Methods
Design
The data collected for this study were part of the screenings conducted during the Million Hearts Fellowship program. 2 The fellows recorded deidentified data about the individuals they screened and input these data into an online survey. Deidentified data from the online, cross-sectional survey were collected and analyzed on 59 798 adult participants who completed a Million Hearts screening between February 2013 and February 2018.
Sample
The target population was the general adult population. Convenience sampling was the recruitment method. All participants were screened by Million Hearts Fellows. Participants provided verbal consent prior to participating in the screening. Approval from a full institutional board review (IRB) process was obtained. (Our University Behavioral and Social Sciences IRB; Approval Number 2015B0498)
Measures
Eight variables were collected on each participant during the Million Hearts screening, including age, sex, ethnicity/race, smoking status, body mass index (BMI), blood pressure, total cholesterol level, and perceived stress level. Blood pressure and total cholesterol were used as indicators of cardiovascular health. Blood pressure was categorized according to classification from the Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. 3 Total cholesterol was classified in 3 different levels: <200 mg/dL, 200 to 240 mg/dL, and >240 mg/dL.
The Perceived Stress Scale 4
The Perceived Stress Scale 4 (PSS-4) was the valid and reliable (α = .77 and r > .73) instrument used to determine the amount of perceived stress the participant reported during their screening. 4 The PSS-4 scale consisted of 4 questions. Scoring was rated on a Likert-type scale of 0 to 4. Higher scores indicated more stress. The tool was verbally administered to participants during screenings. Low stress was categorized as a score of 0 to 8, and high stress was categorized as a score of 9 to 16.
Analysis
Descriptive statistics were used to describe the sample characteristics, overall and stratified by sample characteristics. Multiple logistic regression modeling was used to estimate the effect of stress on the risk of having elevated blood pressure and total cholesterol. The odds ratio (OR) and 95% confidence interval (CI) estimates were presented. SAS 9.4 (SAS Institute, Cary, North Carolina) was used for all the analyses.
Results
Among a total of 59 798 participants, almost a half (45.9%) were of the age between 31 and 60 years and about 14% to 16% in each age-group of 31 to 40, 41 to 50, 51 to 60, and >60 years. The remaining 37.9% of the patients were 30 years or younger. A majority of the study participants were non-Hispanic white (70.3%). African Americans were the largest racial minority (15.8%), followed by Hispanics (6.6%), Asian Americans (4.9%), multiracial Americans (1.7%), and Native Americans (0.4%).
Overall, 24% of the participants had a PSS-4 score of 9 or higher (19.7% with PSS score of 9-12 and 4.1% with PSS-4 score of 13-16). Half of the participants had a normal blood pressure, with the rest having prehypertension (30.8%), stage-I hypertension (15.1%), or stage-II hypertension (3.6%). One-third of the sample had data on total cholesterol. Among them, 61.4% had total cholesterol lower than 200 mg/dL, 30.7% in the range of 200 to 240 mg/dL, and 7.9% higher than 240 mg/dL.
The prevalence of stress (PSS-4 score ≥9), prehypertension or hypertension, and elevated cholesterol (total cholesterol ≥200 mg/dL) was stratified by sample characteristics. The prevalence of stress was significantly associated with age (P < .001), the highest among those aged 31 to 60 (27.9% vs 20.0% for those younger than 30 years and 21.2% among those older than 60 years). African American and Hispanics had significantly higher stress (26.4% and 27.8%, respectively) than non-Hispanic whites (22.9%; P < .001).
Figure 1 showed the prevalence of prehypertension/hypertension and elevated total cholesterol was the highest among African Americans. Higher stress was associated with higher prevalence of prehypertension/hypertension (Figure 1A) and elevated total cholesterol (Figure 1B) among all race/ethnic groups. There was no significant stress by race/ethnicity interaction effects on having prehypertension/hypertension (P =.14) and having elevated total cholesterol (P = .66). Similarly, higher stress was associated with higher prevalence of prehypertension/hypertension (Figure 1C) and elevated total cholesterol (Figure 1D) among all age-groups. There was no significant stress by age interaction effects on having prehypertension/hypertension (P = .10) and having elevated total cholesterol (P = .25).
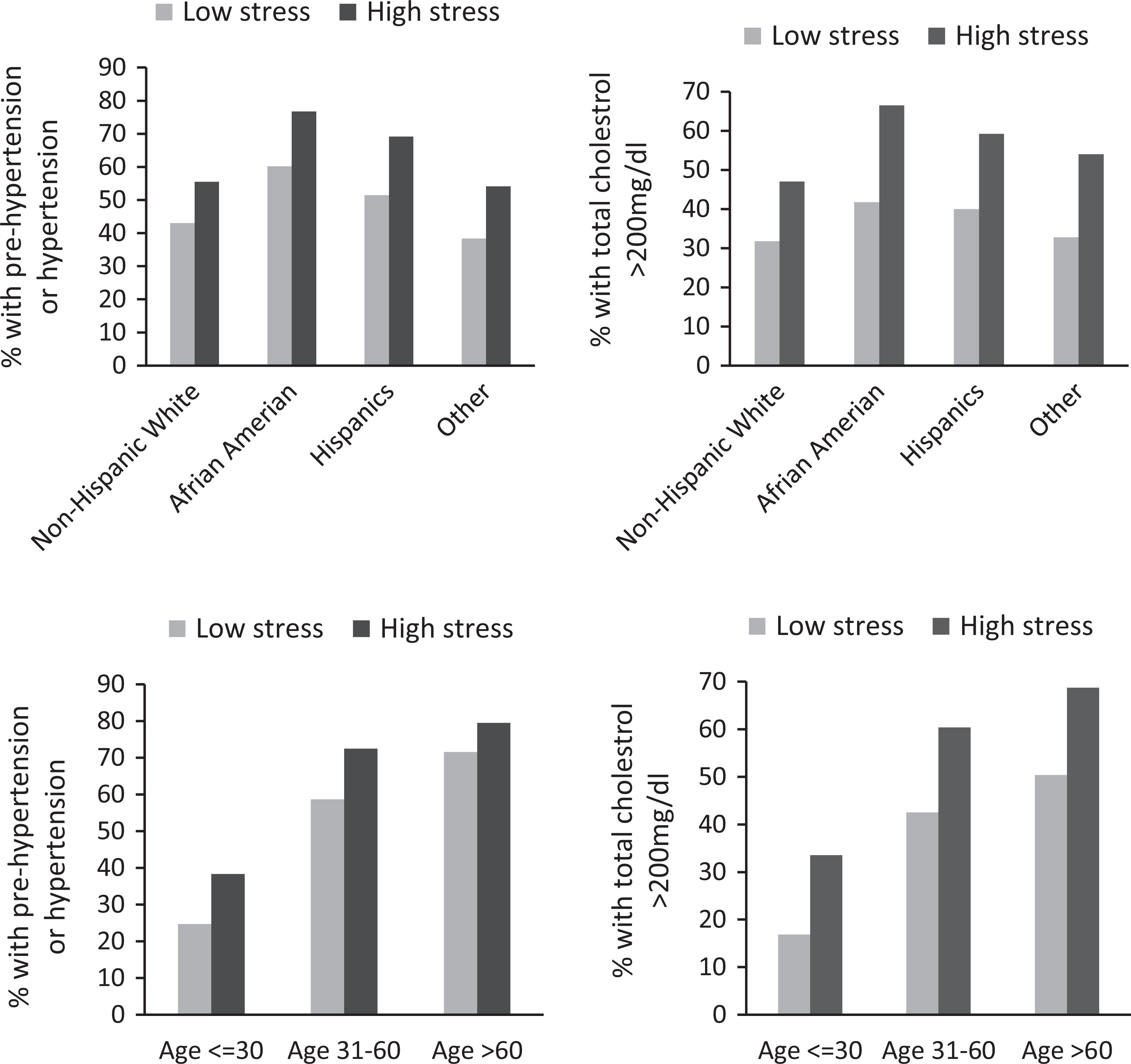
Proportion of patients with prehypertension/hypertension and proportion of patients with total cholesterol >200 mg/dL, by stress and race/ethnicity (A and B) and by stress and age (C and D).
Using logistic regression modeling, the effects of stress on cardiovascular health were estimated, adjusting for other confounders. Compared to those with low stress, high stress was associated with significant higher odds of having prehypertension/hypertension (OR = 1.40, CI = 1.28-1.53) and elevated cholesterol (OR = 1.53, 95% CI = 1.41-1.66). Adjusted confounders included age, sex, race/ethnicity, smoking status, BMI, total cholesterol (for the model on prehypertension/hypertension), and blood pressure (for the model on elevated cholesterol).
Discussion
This study is the first study to look at the prevalence of stress in 2 of Million Hearts’ priority populations (Black/African Americans and the younger age-group). Black/African Americans reported greater perceived stress when compared to non-Hispanic whites, and the younger age-group (30-59 years old) reported greater perceived stress when compared to the those >30 or ≤60.
Limitations
Reported stress was captured at the time of the screening. The stress screening instrument (PSS-4) utilized does not distinguish whether participants were experiencing acute stress or whether their stressors were chronic and ongoing. This study also does not assess or control for existing CVD and was derived from a convenience sample. The study population was mostly white, and the cross-sectional design precludes causal inference.
So What (Implications for Health Promotion Practitioners and Researchers)
What is Already Known on This Topic?
A growing body of research supports the significant association between stress and cardiovascular disease risk.
What Does This Article Add?
This is the first study to look at the prevalence of stress and its association to cardiovascular disease in 2 of Million Hearts’ priority populations (Black/African Americans and the younger age-group).
What are the Implications for Health Promotion Practice or Research?
Clinicians need to incorporate stress screenings into their cardiovascular assessments and prioritize stress screenings in high-risk groups, including African Americans and the younger aged population as they appear to be more vulnerable to the effects of stress.
More research is needed in designing culturally sensitive and effectively tailored interventions relative to stress and cardiovascular disease management.
Significance
Evidence has demonstrated that people with high levels of stress, anxiety, and depressive symptoms are at high risk of CVD and early death, calling into question whether modifiable cardiovascular risk factors can be effectively managed without first addressing emotional distress. 5,6 If the current trajectory of CVD is to be improved with a focus on primary prevention instead of its current “sick care” model, stress and mental health cannot continue to be ignored in current models of cardiovascular preventive care, especially in the Million Hearts priority populations. Stress management and coping skills need to be incorporated into current cardiovascular preventive standards of practice for these priority populations, especially in the African American population who are already at high risk of CVD and poor cardiovascular outcomes. More research is needed in designing culturally sensitive and effectively tailored interventions relative to both stress and disease management. These interventions need to be inclusive of both young and old populations as well as demonstrate effectiveness in diverse populations. Stress should also be added as an additional “S” to the Million Hearts initiative. Stress may be the missing link for improving cardiovascular population health and elevating cardiovascular preventive care to a higher standard.
Footnotes
Authors’ Note
All authors have made substantial contributions to either the conception and design, the analysis and interpretation of data, or both to the drafting/revision of the article, and gave their final approval of the final version to be published. All authors agree to be accountable for all aspects of the work.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.