
Abstract
Purpose:
Assess relationship among health services received and patients’ digital health-care engagement.
Design:
Quantitative cross-sectional survey study.
Setting:
Community health centers in Washington state and DC.
Sample:
N = 164 adult safety-net patients.
Intervention:
Not applicable
Measures:
Outcomes were knowledge and use of health apps. Predictors were health service access (access to specialists and health information); health service delivery (healthy eating and physical activity counsel); health service satisfaction; and perceived service value.
Analysis:
Descriptive and multivariate regression analyses. Odds ratios (OR) reported for 95% confidence interval (CI).
Results:
Response rate was 35%. Of all, 71% were knowledgeable of smartphone use for wellness and 48% used health apps. Physical activity (PA) counseling predicted knowledge and health apps use. Respondents receiving PA counseling were 2.61 times more likely to be knowledgeable about using smartphones for health promotion (OR = 2.61; P = .047; 95% CI: 1.01-6.73). Respondents receiving PA counseling were 2.89 times more likely to use health apps (OR = 2.89; P = .022; 95% CI: 1.17-7.17). Health information access predicted health apps use; respondents with easy access to general health information were 0.29 times as likely to use health apps (OR = 0.29; P = .043; 95% CI: 0.09-0.96).
Conclusion:
Targeted preventive care support encourages digital health-care engagement. mHealth may supplement health-care needs outside clinics.
Keywords
Introduction
Obesity and reduced physical activity (PA) are risk factors for chronic diseases. 1,2 Safety-net patients (residents of communities who are of low-income or uninsured) report more chronic health conditions such as diabetes and have higher obesity rates relative to overall US population. 3
Clinicians can guide patients to adopt and maintain an active and healthy lifestyle through healthy eating and PA; however, evidence show low emphasis on preventive care behaviors by practitioners. 4 Limited time during patient–provider visits necessitates supportive resources for preventive care.
Mobile health technology (mHealth) uses mobile phones, monitoring devices, and other wireless technology for health-care support. 5 There is evidence of the effectiveness of mHealth to increase access to health information, 6 and research shows moderate effects in supporting PA 7 and weight loss. 8 However, little is known about how safety-net patients’ experiences with their health-care providers (HCPs) can promote digital health-care management. The current study assesses the relationship among health services—access, delivery, satisfaction, and value on patients’ digital health-care engagement. The approach was an exploratory analysis informed by the Andersen and Newman’s model of health services utilization which states that characteristics of health service system and individual characteristics predict health services utilization. 9
Methods
Study Population
We conducted a cross-sectional primary analysis of data collected from N = 164 patients from community health centers in Washington state and DC. In Washington, 103 respondents were randomly selected from a regional community-supported health system. In District of Columbia, patients comprised a convenience sample of n = 61 from human service centers. Data were analyzed for 159 respondents due to missing information from 5 patients.
Instruments and Data Collection
A 47-item questionnaire assessed mHealth knowledge, practices, and health-care services. Questions on the survey were adapted from existing patient satisfaction/consumer assessment of health surveys as well as an existing theory outlining users’ attitudes, acceptance, and use of technology. 10 Study protocols were approved by the institutional review boards of HealthPoint (Renton, Washington), Eastern Washington University, and Trinity Washington University (Washington, DC).
Investigators commenced survey administration on September 2014 and concluded in November 2015. In Washington state, investigators approached patients entering waiting areas of the health-care facility. A detailed breakdown of the recruitment schema is found elsewhere. 11 Criteria for inclusion were own a smartphone; age 18+ years; and at least 2 face-to-face contacts with HCPs within the past 12 months. Eligible patients completed written informed consent, questionnaire, and received $10 gift certificate.
Measured Variables
Outcome Variables
Knowledge: Assessment question was: “Some people use smartphones/mobile devices as part of patient wellness,” prevention, and treatment, were you aware that you can use your smartphones (this way)? This outcome was treated as a dichotomized measure (“yes” = 1; “no” = 0).
Practice: Defined as using health-based applications for preventive health care including tracking caloric intake. Assessment questions were, “Have you ever used a health-based mobile application?” “What type of health app do you have?” Respondents were identified as users of health apps if they answered affirmatively to the first question and/or indicated an app that they currently owned. This outcome was treated as a dichotomized measure (“yes” = 1; “no” = 0).
Predictor Variables
Health-care service access
Assessment questions were, “Would you say that you have easy access to the medical specialists that you need?” “Would you say that you have easy access to health information so that you can make decisions about your health and well-being?” Bivariate measures of “agree” and “disagree” captured responses.
Health-care service delivery
“Has an HCP at this center ever talked to you about eating healthy or provide information about eating healthy?” “Has an HCP at this center ever talked to you about engaging in at least 2.5 hours (150 minutes) of moderate-intensity PA every week?” (“yes/no” responses captured).
Health-care service satisfaction
“How would you rate the nurses, medical assistants or doctors on giving you information you can understand?” “How would you rate the nurses/doctors on considering your personal and family’s cultural/ethnic needs?” Responses dichotomized (“very good/good” = 1; “fair/poor” = 0).
Healthy lifestyle value assessment
“How important is it for you to receive information about making healthy lifestyle choices (eg, being physically active and eating health)?” Responses dichotomized (“very important/somewhat important” = 1; “neutral/not very important” = 0).
Statistical Analyses
Descriptive analyses characterized outcome and predictor variables. Multivariate regression models assessed relationships between each outcome (knowledge and practice factors) and health-care systems and patient perception factors. We report odd ratios (ORs) and 95% confidence intervals (CIs). Data were analyzed using STATA/SE (Stata/SE 14) statistical software.
Results
Patient Characteristics
Response rate for patients approached in CHCs in Washington state was 35%. A full breakdown of study recruitment for both sites is available elsewhere. 11 Mean age of all respondents was 36 years (standard deviation = 8). The sample comprised mostly women (68%), nonwhites (41.5%), and individuals with incomes below $20 000/year (63%). Among respondents, 71% were knowledgeable of smartphone use for wellness and 48% used health apps. Majority had access to specialists (78%) and health information (83%). No significant differences existed between the 2 sites except in the domains of race and income (Table 1).
Descriptive Statistics of Demographic Factors, Predictors, and Outcome Variables.
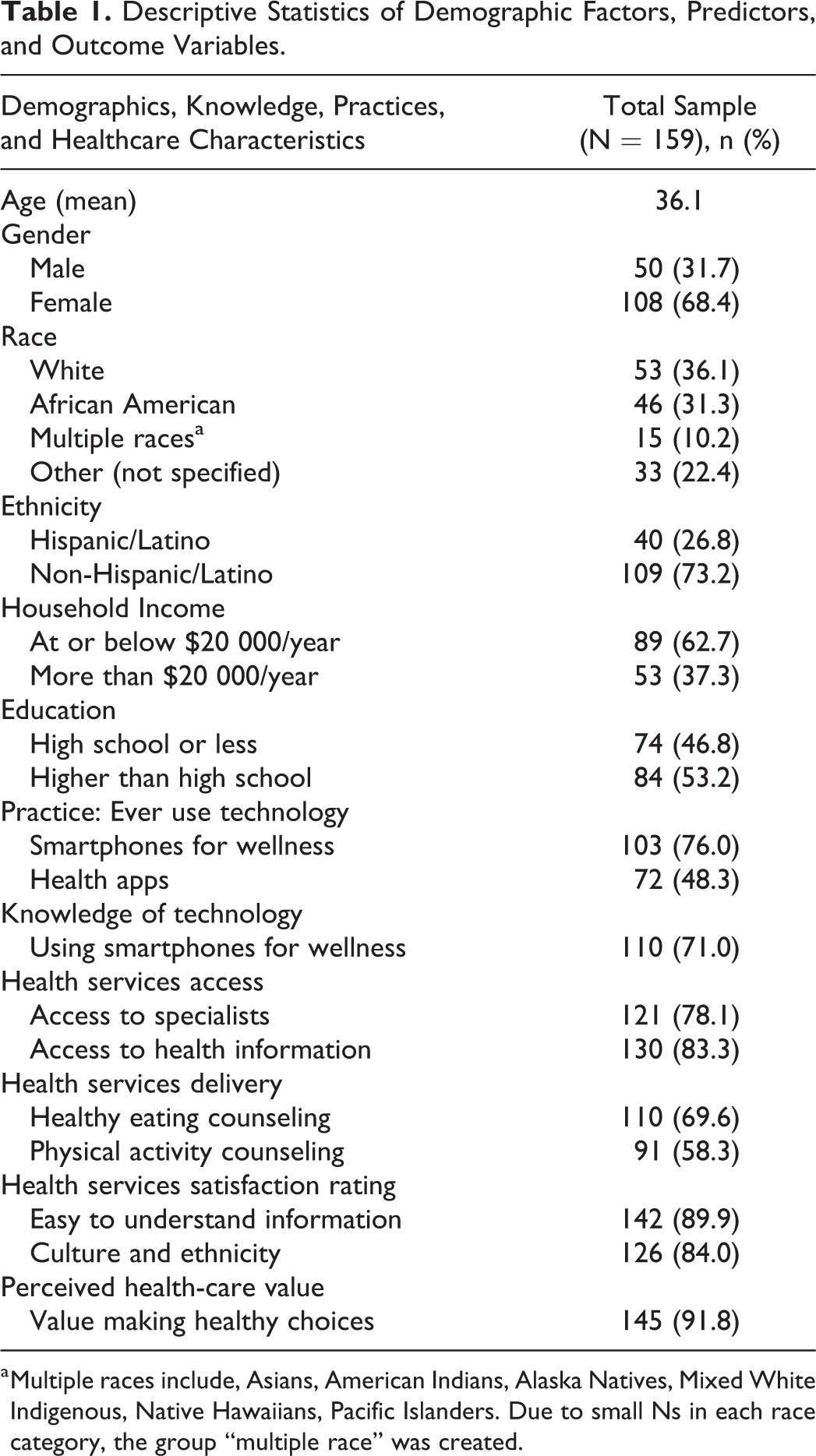
a Multiple races include, Asians, American Indians, Alaska Natives, Mixed White Indigenous, Native Hawaiians, Pacific Islanders. Due to small Ns in each race category, the group “multiple race” was created.
Availability of Preventive Care Support for Safety-Net Patients
Only 69% of respondents received healthy eating counsel, and fewer (58%) received PA support; however, a larger proportion (92%) indicated that they value information to help them make healthy lifestyle choices (Table 1).
Relationship Between Preventive Care Support and Use of Mobile Health Technologies
Physical activity made a unique contribution to predicting knowledge of using smartphones for wellness (OR = 2.61; P = .047; 95% CI: 1.01-6.73). Respondents counseled by an HCP to engage in recommended PA were 2.61 times more likely be knowledgeable about using smartphones for health promotion (Table 2). Our full regression model explains 34.1% of the variation in knowledge of using smartphones for wellness.
Logistic Regression: Health Services, Health Access, Service Satisfaction, and Perceived Value as Predictors of Mobile Health Technology Knowledge and Practice Factors.a

Abbreviations: CI, confidence interval; OR, odds ratio.
a Bold indicates significant at the P < .05 level. All models adjusted for age, gender, and race.
b R2= .341.
c Multiple races include, Asians, American Indians, Alaska Natives, Mixed White Indigenous, Native Hawaiians, Pacific Islanders. Due to small Ns in each race category, the group ‘multiple race’ was created. Other” race category not included in statistical models.
d R2 = .345.
For the model predicting use of health applications, respondents obtaining counsel to engage in weekly moderate PA were 2.89 times more likely to use health apps for status tracking (OR = 2.89; P = .022; 95% CI: 1.17-7.17). Also, respondents with access to general health information were 0.29 as likely to report use of health apps for wellness (OR = 0.29; P = .043; 95% CI: 0.09-0.96). For these results, the full regression model explains 34.5% of the variation in use of mobile health applications for status tracking. The health applications safety-net patients used or owned were calorie counting (38%), step counting (28%), and stress management applications (25%).
Discussion
Safety-net patients are knowledgeable about smartphones’ value to access wellness information, and they use health apps for preventive care. A gap in PA support exists, and this is significant because majorities of safety-net patients are motivated to engage in self-care management.
Patients who received specific PA counseling were likely to engage in digital health-care management, thus demonstrating that patient–provider connectedness can promote care continuity. Some physicians, however, are reluctant to recommend mHealth tools to supplement care, with only 10% of patients report learning about mHealth technologies from HCPs. 12 Reticence of HCPs is attributed to lack of clear strategy to evaluate health-based applications. 13 Research that identify mHealth tools yielding clinical significance on key health metrics 14 can support HCPs’ preventive care efforts.
To our knowledge, our study is the first to evaluate the relationship between support for preventive care and digital health-care practices of safety-net patients, and our findings generalize to this population. Association between digital health-care management and PA counseling has implications for public health practice because low-resourced patients are disproportionately impacted by chronic diseases associated with lifestyle practices. 15 Mobile health applications are ubiquitous, relatively inexpensive, and can support care in-between office visits.
Selection bias presented as a potential limitation due to convenience sampling in DC; however, no significant differences emerged between the 2 sites on several health services variables. A second limitation is the fact that data were collected and analyzed over a 2-year interval, and thus knowledge and use of mobile health devices by safety-net patients might have changed in the intervening years; we anticipate that with increasing penetration of digital health-care tools, behavioral practices may show a parallel increase during this time frame. A prominent strength is that respondents comprised a bicoastal sample from urban settings in DC and suburban/rural settings in Washington state, thus enhancing generalizability.
So What?
Clinical preventive services can improve health outcomes. 16 Our study demonstrates that limited physical activity counseling can encourage digital health-care engagement, and mHealth tools may effectively promote patient education and self-care management.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Some funding received from Eastern Washington University, Community Engagement Award.