
Abstract
Purpose:
Home food environment, including home food availability and parental food preparation practices, plays a significant role in child diet patterns. Recent evidence suggests that parental psychological stress is related to parental food preparation practices; however, there is limited information about the relationship between parental psychological stress and home food availability. The purpose of the study is to examine the relationships between parental stress, home food availability, child diet patterns, and body mass index (BMI) in families with young children.
Design:
A secondary data analysis from a mixed-methods design study.
Setting:
The parent study was conducted in both local and online communities using a web-based survey.
Participants:
Participants were 256 parents of children aged 2 to 5 years (53.4% white; 41.5% of overweight or obese children).
Measures:
Parents completed well-validated self-report questionnaires.
Analysis:
We used latent structural equation modeling using Bayesian analysis.
Results:
There was a negative relationship between parents’ general stress and healthy food availability at home (β* = −.20, P < .001 for fruits; β* = −.23, P < .001 for vegetables; and β* = −.24, P < .001 for healthy beverage) and a positive relationship between parenting stress and healthy snack and healthy beverage availability (β = .13, P = .03; β = .14, P = .02, respectively). There was no relationship between parental stress and unhealthy food availability at home while unhealthy food availability was significantly associated with child’s unhealthy eating pattern (β* = .86, P < .01 for unhealthy snack; β* = .51, P < .01 for unhealthy beverage). There was no moderating effect of children’s health insurance on the relationships between parental stress and home food availability. Furthermore, child diet patterns were not associated with child BMI.
Conclusion:
Parental psychological stress is a potentially important intervention target point for improving home food environment and child diet patterns.
Keywords
Introduction
Childhood obesity is an ongoing epidemic: According to the Centers for Disease Control and Prevention, 22.8% of preschool children and 34.2% of school-aged children are at least overweight in the United States. 1 This health crisis underscores the need to understand how health behaviors including eating behaviors are established early in life, which may influence health throughout the life span. 2 Children begin to develop their diet patterns and food preferences when they are toddlers, at which time they are introduced to the foods that are available in their home environment 3 and they observe their parents’ preparation of foods and selection of foods. This influence of the home food environment on children’s eating habits creates similar patterns of food intake within families and shapes diet patterns and food preferences that may persist into adulthood. 4,5 Therefore, the home food environment is a critical determinant of child diet patterns and body mass index (BMI). 6
Home food environment often includes the physical environment (eg, food availability) and sociocultural environment (eg, parenting styles, practices, and rules). 7 Couch et al 7 found that children were less likely to eat fruits and vegetables if there was a low availability of those foods in their home. Similarly, sociocultural aspects of the home food environment (eg, parental feeding and food preparation practices) can influence a child’s diet behavior and nutritional intake. 8 Parents represent the principal and most proximal social interact during a child’s early development, 9 and in most US families, parents or adult caregivers are primarily in charge of purchasing food, preparing food, and serving food in the home environment, all of which influences children’s diet patterns. Furthermore, individual parents’ food-related practices influence home food environment and may be associated with parental psychological stress. 10
Stress is a response to the stressors of both perceived and actual threats. 11 It can affect the body physically, mentally, and emotionally, essentially acting as a threat to the body’s homeostasis. 12 Importantly, stress may influence an individual parent’s behaviors as stress responses or coping strategies. It is known that individuals with stress may experience more emotional eating, as a response to stress, that seek higher fat and carbohydrate foods. 13 Individuals who have high levels of stress may also be more likely to choose unhealthy food options such as comfort foods and thereby gain weight. 14 By affecting the parent’s own eating habits, parental stress may influence the food options at home that a parent shares with and provides to their children.
Emerging evidence suggests that parental stress is positively associated with unhealthy sociocultural aspect of home food environment. 15,16 Parents’ general stress and more specific stressors (eg, parenting stress) may be related to parental unhealthy feeding practices (eg, higher control over child eating and pressure to eat), which could lead children’s unhealthy eating behaviors. The effects of parental stress on what the parents choose to provide in terms of food availability may also affect how the children develop their own diet patterns. Parents who experience stress may also have unhealthy food preparation practice such as buying unhealthy foods and store those foods at home as stress coping responses 14 or because they do not have the energy to take on the responsibilities of making a healthy food option. 17 In addition, when parents are stressed, they may choose high-fat and high-carbohydrate foods but may not choose fresh fruits or vegetables. Parental stress, therefore, could influence the availability of foods at home. However, there is a paucity of information on whether parental stress is related to home food availability. In one study, Bauer et al 18 found that parents who had higher stress levels tended to have fewer family meals together, less vegetable and fruit intake, and meals with shorter preparation time. A better understanding of the relationship between parents’ psychological stress and the physical home food environment (ie, home food availability) would help develop more comprehensive and effective approaches for improving childhood obesity. Therefore, we aimed to examine the relationships between the community food environment, parental stress (ie, general stress and parenting stress), home food environment, and child diet patterns in families with young children aged 2 to 5 years. On the basis of prior findings, we developed a hypothesized model (Figure 1).
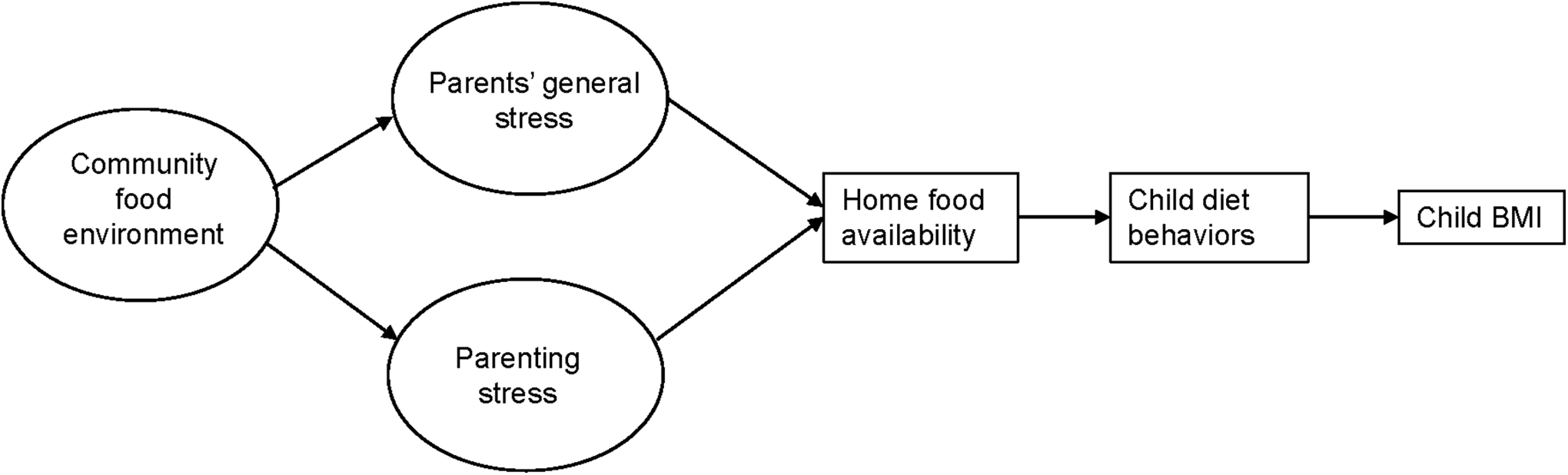
Hypothesized model.
Methods
Study Design
We conducted a secondary data analysis using quantitative data from a mixed-methods study of the relationships of parental psychological distress, parental feeding practices, child dietary patterns, and child BMI. Additional information on the design of the parent study is available in Jang et al. 16 A university institutional review board reviewed and approved the study.
Setting and Participants
The parent study enrolled diverse racial or ethnic families with children aged 2 to 5 years with the following inclusion criteria: (1) the parent or guardian able to speak and read English and (2) child without any chronic condition or taking any medications that could affect his or her diet or BMI. Each participant was asked whether he or she was responsible for most of the childcare and food preparation. The study was conducted in local communities and online communities. To enhance racial or ethnic diversity, oversampling strategies were utilized for racial or ethnic minority families targeting ethnic-specific communities.
Measures and Analysis
The data were collected using a validated self-report questionnaire.
Demographics
We assessed family demographic characteristics using the self-reported data on child age and gender, age of the primary caregiver (study participant), number of children and adults in the household, and race or ethnicity of both parent and child.
Parental Stress
Two different types of parental stress were assessed: parents’ general stress using the Perceived Stress Scale 19 and parenting stress using the Parental Stress Scale. 20 The Perceived Stress Scale (10 items on Likert scale; scores ranging from 0 to 40, with higher scores indicating more perceived general stress) has good reliability with high internal consistency (Cronbach α = .84) and test–retest reliability (intraclass correlation coefficient [ICC] = 0.85). 19 Cronbach α for the study sample was .62. The Parental Stress Scale (18 items on Likert-scale items; scores ranging from 18 to 90, with higher scores indicating greater stress) demonstrated satisfactory levels of internal reliability (Cronbach α = .83) and test–retest reliability (ICC = 0.81). 20 Cronbach α for the study sample was .87.
Community Food Environment
Community food environment was assessed using the Perceived Community Food Environment, which has been validated (Cronbach α = .78 for internal consistency; test–retest reliability ICC = 0.69). 21 The questionnaire included descriptive questions and 3 items asking about fruit availability, fruit quality, and low-fat food availability with a 5-point Likert (1 = strongly agree to 5 = strongly disagree), with lower scores indicating higher community food environment. We used these 3 items for the model development.
Home Food Availability
Home food availability was assessed using the Home Food Inventory. Home Food Inventory assesses 13 major food categories and 2 categories assessing ready access to foods in a checklist-type format with yes/no (1/0) response options. The instrument has good reliability (κ = .61-.83). 22 For data analysis, we categorized the major food items into healthy food options, including fruits, vegetables, reduced sugar snacks, and unsweetened beverages and unhealthy food options, including sugar snacks and sweetened beverages.
Child Dietary Patterns
Children’s diet patterns were measured with the Harvard Service Food Frequency Questionnaire (HFFQ), which is validated for use in children aged 1 to 5 years to assess dietary behaviors and patterns. 23 The Pearson correlation coefficient between the questionnaire and 24-hour recall ranged from 0.26 to 0.62. 23 The questions of the HFFQ included frequency of consumption of 84 specific food items during the previous month. We developed proxies of healthy and unhealthy diet patterns by summing each of healthy or unhealthy food items. Healthy food items included fruits and vegetables, unsweetened drinks, and low sugar snacks, and unhealthy food items included regular drinks, sweetened beverage, sugar snacks, and processed meats.
Data Analysis
We conducted descriptive data analysis using SPSS, version 14. We profiled each variable using frequencies for categorical variables and measures of central tendency for continuous variables. The proportion of missing data for child healthy diet and child unhealthy diet patterns was 14%, child BMI was 8%, and parenting stress was 7%. We reviewed the type of missingness for each variable and determined the missingness was at random based on the order of the survey in which the child eating pattern questions were placed at the end of the survey. Based on the proportion of the missing values, we did not impute the missing values.
Using Mplus, version 8.0, we ran a latent structural equation modeling (LSEM) analysis using empirical Bayesian (EB) modeling. Empirical Bayesian modeling allowed us to minimize standardized errors due to small sample size and skewed distributions of the variables. 24 To reduce a measurement error in the model, we constructed latent variables of parents’ general stress, parental stress, and community food environment. We developed 2 models by categorizing home food availability into healthy food options and unhealthy food options. For child diet patterns in the model, we based the score for healthy food items and unhealthy food items for each model. The variable of child unhealthy food items was not normally distributed, so we log-transformed the variable to adjust the distribution. Next, we utilized the EB modeling with confirmatory modeling based on robust maximum likelihood estimation to develop measurement models at the latent variable level as well as a direct effect model and indirect effect model among variables.
Mediation testing was based on the methods discussed by MacKinnon, 25 which guided the statistical analysis, and used significant indirect effects to demonstrate mediation. Bayesian methods are a useful alternative to maximum likelihood estimation in mediation models, particularly with smaller samples. 26 To obtain the small sample benefits of Bayesian methods, a prior distribution must be informative. 27 We estimated the direct effect, indirect effect (total and specific), and total effects using EB Markov chain Monte Carlo estimates, using data-derived estimates from our data set as our EB informative priors. 26,28,29 The Bayesian estimates and the analysis of the LSEM were constructed model fit for the Bayesian mediational structure was assessed using the Bayesian posterior predictive P value (PPP), where low PPP indicates poor fit, and the latent variable R 2.
To test whether the participants’ socioeconomic status (SES) level influences these relationships between community food environment, parental stress, home food availability, child diet patterns, and child BMI, a multiple-group structural model (a moderated mediation model with 2 outcome measurements) was constructed. The moderator (ie, children’s health insurance) was treated as a categorical variable by dividing into private versus public health insurance, which is an attractive method for studying moderated mediation as multiple-group structural modeling. 30 We divided participants into 2 groups based on insurance options as a proxy of SES and examined the relationships between and within the groups, which was equivalent to assessing SES as a moderating variable.
Results
Sample Characteristics
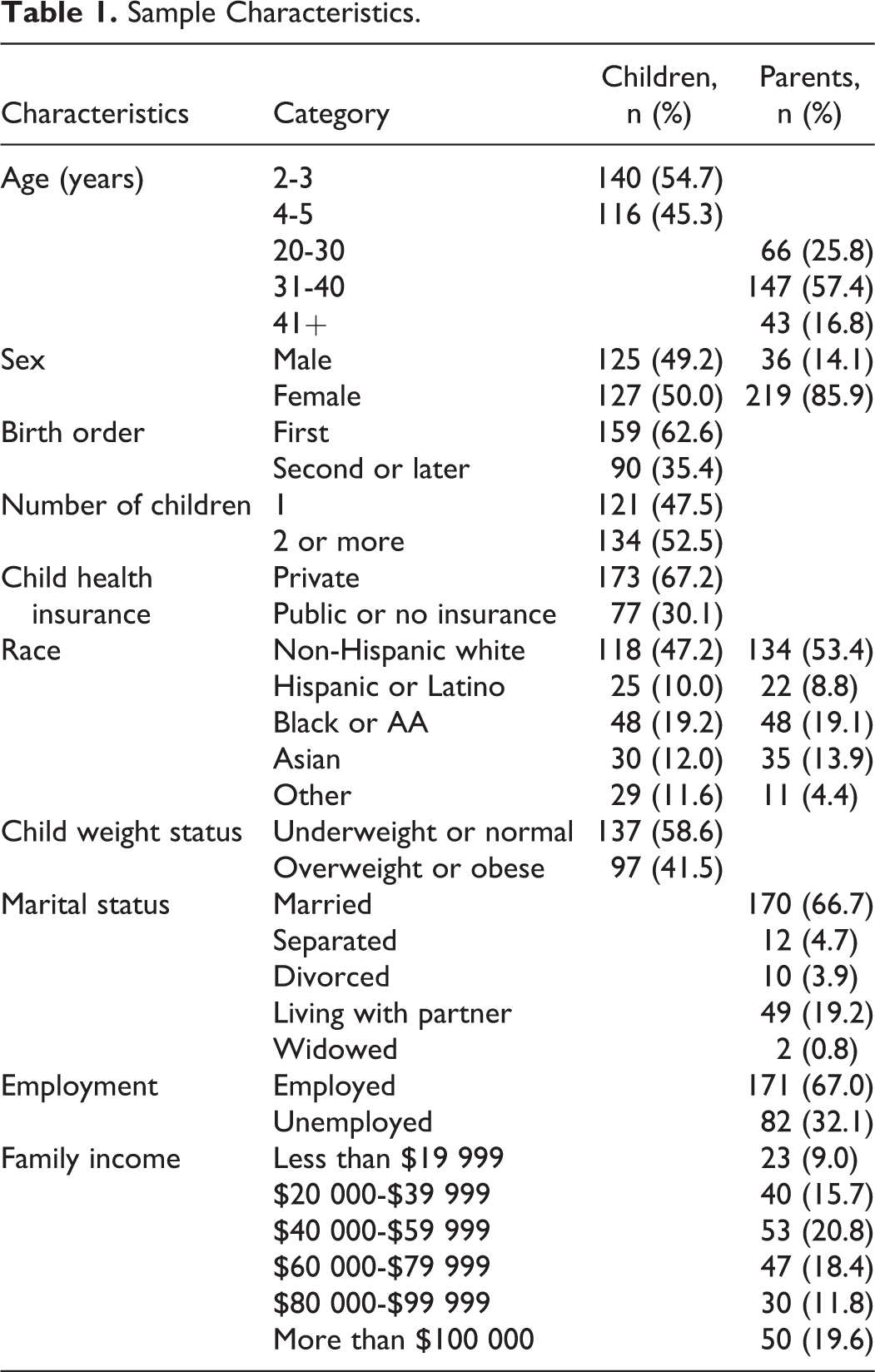
Two hundred and fifty-six parents participated in the study. The sample characteristics of the study participants appear in Table 1. The mean age of children was 3.8 (standard deviation [SD] = 1.0) years. Half (50.0%) of children were girls, and 30.1% of children were on public health insurance or had no health insurance. Less than half of parents were non-Hispanic white (47.2%), but Hispanic or Latino children constituted a relatively small proportion of the sample (10.0%) compared with other minorities (19.2% black and 12.0% Asian). The mean BMI for children was 17.8 kg/m2 (SD 5.9) and 31.1% of the children were obese. With respect to parents and family characteristics, 85.9% of parents were married or lived with partner. Family income was relatively evenly distributed from low- to high-income levels.
Sample Characteristics.
Bivariate Correlations Between Variables
The bivariate correlations between variables are presented in Table 2. Parents’ general stress and parenting stress were significantly correlated (r = 0.40, P < .05). Parents’ general stress was significantly inversely associated with fruit availability (r = −0.1, P < .05), vegetable availability (r = −0.14, P < .05), and healthy beverage availability (r = −0.17, P < .05). The healthy food items availability at home was significantly correlated with child healthy diet patterns (fruits: r = 0.95, P < .05; vegetables: r = 0.86, P < .05; healthy snacks: r = 0.71, P < .05; and healthy beverage: r = 0.57, P < .05). Healthy food availability items were positively correlated with unhealthy food availability items (r = 0.31-.73, P < .05), and all home food availability items were positively correlated with child diet patterns (r = 0.28-0.95, P < .05). However, any of the variables was not correlated with child BMI.
Bivariate Correlations Between Variables.

Abbreviations: BMI, body mass index; Comhealth, perceived community food environment; fruits, fruit availability; healthy BE, healthy beverage availability; healthy SN, healthy snack availability; parenting, parenting stress; PSS, Perceived Stress Scale (parents’ general stress); unhealthy BE, unhealthy beverage availability; unhealthy SN, unhealthy snack availability; vegetable, vegetable availability.
a P < .05.
Relationships of the Factors in the SEM Model
For the measurement model estimates, parents’ general stress was loaded with every item of the instrument ( λ*= .44-1.43, P < .001; data not shown). Parenting stress was also loaded with each item of the instrument (λ*= 1.00-4.33, P < .001; data not shown). Community food environment was loaded with 3 items about perceived fruit and vegetable availability and quality and low-fat food availability (λ*= .92-1.00, P < .001; data not shown).
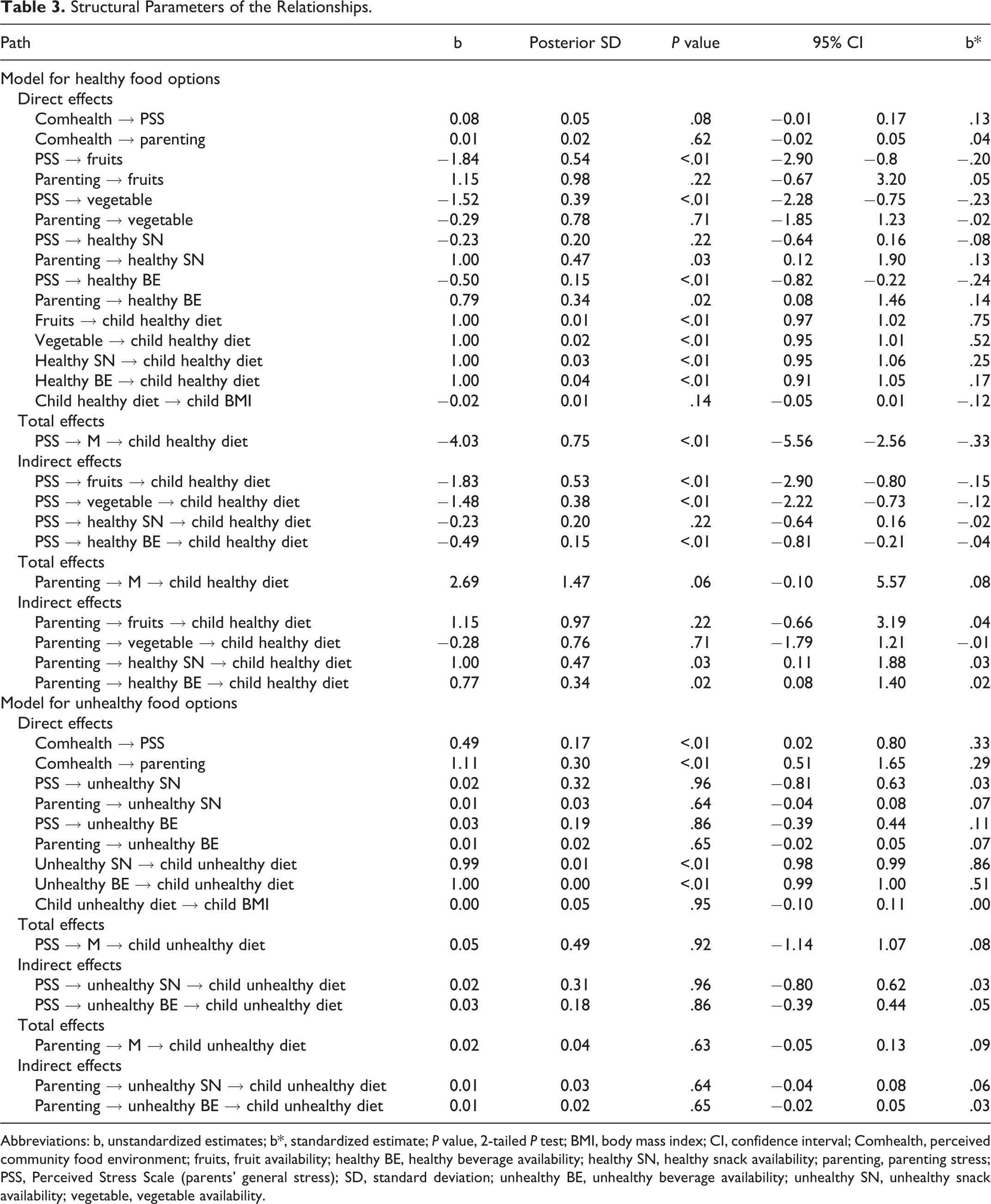
The relationships between community food environment, parental stress, home food environment, child diet patterns, and child BMI appear in Table 3. With regard to healthy food options, the relationship of parents’ general stress and parenting stress with home food availability took different directions. For direct effect, community health environment was not associated with both parental stress. However, parents’ general stress was inversely associated with fruit, vegetable, and healthy beverage availability at home (β* = −.20, P < .001; β* = −.23, P < .001; and β = −.24, P < .001, respectively). Parenting stress was positively associated with healthy snack and healthy beverage availability at home (β* = .13, P = .03; β* = .14, P = .02, respectively). In turn, all indicators of home healthy food availability were associated with child healthy diet pattern (β* = .17-0.75, P < .01), but child healthy diet pattern was not associate with child BMI.
Structural Parameters of the Relationships.
Abbreviations: b, unstandardized estimates; b*, standardized estimate; P value, 2-tailed P test; BMI, body mass index; CI, confidence interval; Comhealth, perceived community food environment; fruits, fruit availability; healthy BE, healthy beverage availability; healthy SN, healthy snack availability; parenting, parenting stress; PSS, Perceived Stress Scale (parents’ general stress); SD, standard deviation; unhealthy BE, unhealthy beverage availability; unhealthy SN, unhealthy snack availability; vegetable, vegetable availability.
With regard to the total effect, there was a significant inverse relationship between parents’ general stress and child healthy diet pattern (β* = −.33, P < .001), but no significant relationship between parenting stress and child healthy diet pattern. The indirect relationships were consistent with the direct and total effects in that healthy food availability at home (including fruit, vegetable, and healthy beverage availabilities) mediated the inverse relationship between parents’ general stress and child healthy diet pattern (β* = −.15 to −.04, P < .01). For parenting stress, the path relationship from parenting stress to healthy snack and beverage availabilities and child healthy diet pattern was significant (β* = .03, P = .03; β* = .02, P = .02, respectively).
With regard to unhealthy food options, there were some relationships among variables. Unhealthy community food environment was positively associated with both of parental stress (β* = .33, P < .01 for parents’ general stress; β* = .29, P < .01 for parenting stress). Both of parental stress were not associated with unhealthy food availability at home. In turn, all indicators of unhealthy food availability at home were associated with child unhealthy diet pattern (β* = .86, P < .01 for unhealthy snack; β* = .51, P < .01 for unhealthy beverage). With regard to the total effect and indirect effect, there was no significant relationship between parental stress and child unhealthy diet pattern.
Health Insurance Moderation
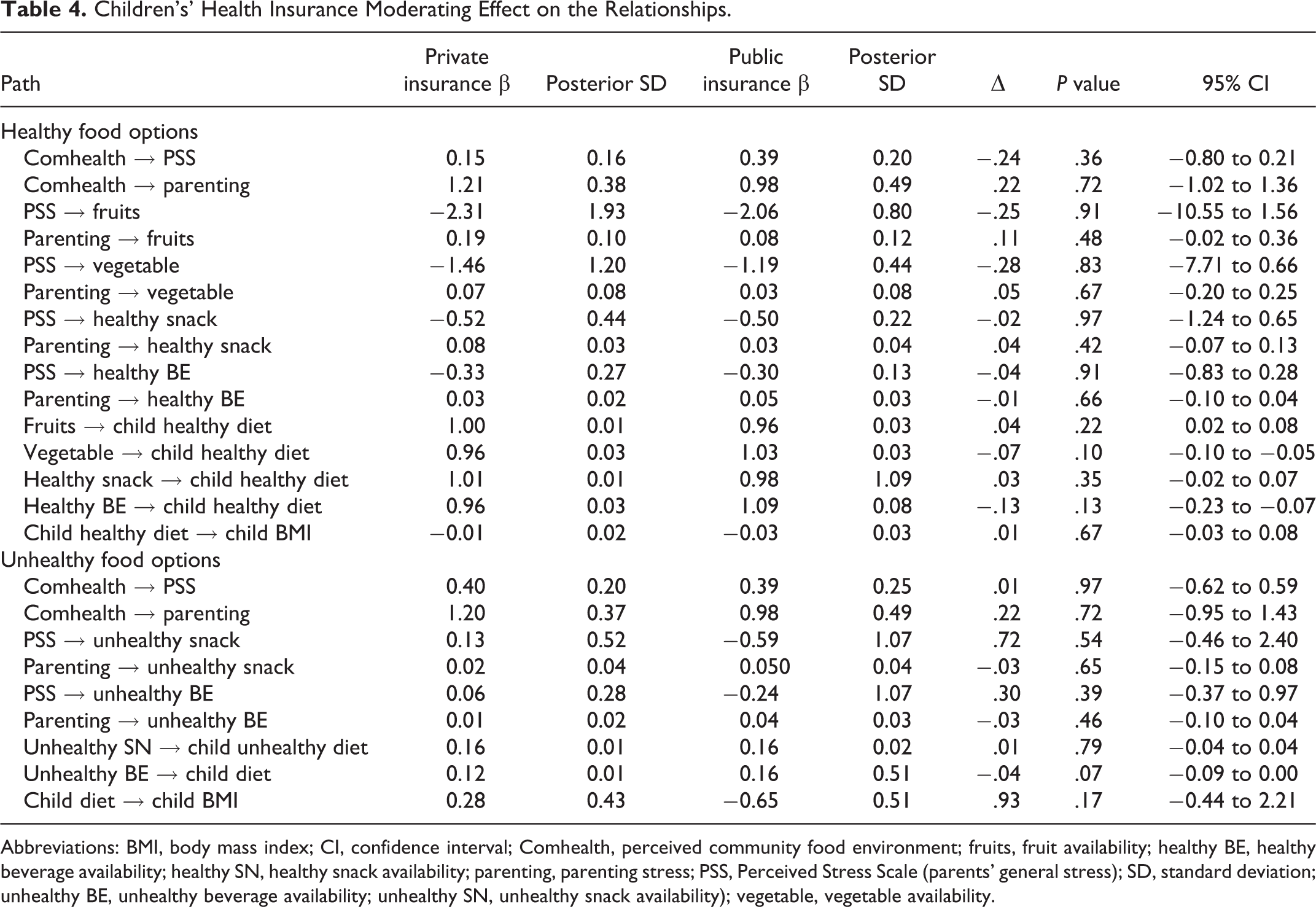
With regard to healthy food options, parents’ general stress was negatively associated with healthy food availability at home in families of children with public health insurance (β* = −2.06, P < .01 for fruits; β* = −1.19, P < .01 for vegetable; β* = −.50, P = .03 for healthy snack; β* = −.23, P < .02 for healthy beverage; data not shown). In families of children with private health insurance, parenting stress was positively associated with healthy snack availability (β* = .08, P < .05; data not shown). With regard to unhealthy food options, unhealthy community food environment was positively associated with parents’ general stress and parenting stress in both insurance groups (private insurance families: β* = .27, P = .02; β* = .32, P < .01, respectively; public insurance families: β* = .34, P = .02; β* = .29, P = .03, respectively, data not shown). In the moderation model, no statistically significant differences in parameters between private and public health insurance suggest the lack of a moderating effect of child’s health insurance on the structure (Table 4).
Children’s’ Health Insurance Moderating Effect on the Relationships.
Abbreviations: BMI, body mass index; CI, confidence interval; Comhealth, perceived community food environment; fruits, fruit availability; healthy BE, healthy beverage availability; healthy SN, healthy snack availability; parenting, parenting stress; PSS, Perceived Stress Scale (parents’ general stress); SD, standard deviation; unhealthy BE, unhealthy beverage availability; unhealthy SN, unhealthy snack availability); vegetable, vegetable availability.
Discussion
To date, there is no prior report regarding the mediating role of home food environment in the relationship between parental stress and child diet patterns. We advanced our understanding of the relationship between parental stress and child diet patterns by examining the mediating effect of home food availability on the relationship between parental stress and child eating patterns. Furthermore, we classified parental stress into parents’ general stress and parenting stress and examined whether different types of parental stress are mediated by home food environment for the relationship with child diet patterns. We used LSEM to delineate the complex relationships.
We found that home food environment acts as a possible mediating factor for the relationship between parental stress and child diet patterns. Our finding indicated that there is a negative relationship between parental stress and healthy food availability at home; yet, there was no relationship between parental stress and unhealthy food availability at home. Prior reports suggested that the stress of individuals may be associated with a greater preference for energy-dense foods, which are high in sugar and fat. 13,31 Our findings were partially aligned with the prior reports in that parents with higher stress may be less likely to purchase and store fruits, vegetables, and healthy snacks and beverages at home, but not necessarily sugar snacks and sweetened beverages. Furthermore, our finding supports prior research suggesting that the physical home food environment (ie, home food availability) is a significant factor for diet patterns of children. 32,33 Thus, our findings provide evidence of a potential mediating role of home food environment in the relationship between parental stress and childhood obesity.
Our findings also indicated that there were different directions for the relationships of parents’ general stress and parenting stress with the home food environment. Parents’ general stress was inversely associated with healthy food availability, while parenting stress was positively associated with healthy food availability. The differences in the relationship may depend on the different etiology of the stress sources as well as parents’ coping strategies for different types of stress. General stress reflects an individual’s overall perception of stress at a given duration of time. 34,35 Parenting stress, conversely, is the individual’s perception of stress resulting from the role of being a parent, experienced as daily hassles regarding children’s behaviors. 36 Parenting stress includes not only parent characteristics and child characteristics but also any family dynamics that may affect the parent–child relationship. 37 These different sources of stress may lead to the divergent relationships that we observed for general stress and parenting stress. The different types of stress may also influence parents’ coping strategies. Parents’ general stress may be more related to their own behavioral changes, such that their behaviors are relevant to their own stress coping strategies, which would be consistent with our hypothesis. Meanwhile, parenting stress is more associated with the bidirectional relationship between parent and child; thus, parents with parenting stress may try to improve their relations with their children to resolve the conflict or tension with their children. Prior research examining the relationship between parenting stress and childhood obesity was focused on the mediating role of parental practices in the relationship. Parents with higher parenting stress were less likely to limit their children’s TV viewing. 38 Likewise, different stress etiologies and different coping strategies according to stressors may support our finding of the differences in the relationship of general parental stress and parenting stress with home food availability.
There were differences in the relationships of community food environment, parental stress, and home food availability between SES groups (ie, families of children with private health insurance vs public or no health insurance). Children’s health insurance as a socioeconomic indicator is an influencing factor for home food environment. 39 Low SES families have limited resources for healthy food choices, which in turn influences children’s eating patterns and food options. 40 We found that there was negative relationship between parents’ general stress and their healthy food choices, including fruits, vegetables, healthy snacks, and healthy beverage, in low SES families. Furthermore, our finding of the significant relationship between unhealthy community food environment and parental stress in families of children with public health insurance indicated that parental stress is definitely related to community food resources. A community with limited resources is more likely have unhealthy food options such as fast-food restaurants and convenient stores that provide energy-dense food at lower prices. 41 Limited community resources could create conflicts in the parents’ healthy practice for their own and children’ diet patterns resulting from limited community resources, which may lead higher parental stress. Furthermore, children in such a community with limited healthy food options are more likely to be obese than children living in a community with more resources. 42 Nonetheless, the statistically insignificant moderation effect of children’s health insurance warrants a cautious interpretation of any possible influence of children’s health insurance on the relationship between parental stress and home food environment.
Study Limitations
Our study has some limitations. We used an existing data set obtained by convenience sampling; thus, the data had limited flexibility for answering the current study questions. Moreover, the cross-sectional study design did not allow us to determine causal relationships. Although the parent study included a diverse sample with oversampling methods to obtain sufficient comparative data from multiple racial and ethnic groups, the study outcomes may not be applicable to all families. Also, because parents reported information about their child’s diet, height, and weight, the accuracy of the assessment of child dietary patterns and BMI could be biased. Finally, the assessment of community food environment is somewhat limited by the use of only 3 items to obtain parents’ perception of food availability and quality. Therefore, there was limited information of accessibility of community food environment such as fast-food restaurants that could have a great influence on parents’ stress and home food availability.
Conclusions
We examined the relationships between parental stress and community food environment, home food environment, and child eating patterns. We found that the home food environment acts as a mediator in the relationship between parental stress and child diet patterns, which advances our efforts to improve childhood obesity. Future researchers may wish to further explore the specific etiology of different directional relationships for parental stress and home food environment. Interventions that target parental stress management may help to improve child eating patterns and behaviors.
So What? (Implications for Health Promotion Practitioners and Researchers)
What is already known on this topic?
Parental psychological stress is positively associated with parental unhealthy feeding practices, which is a known risk factor for childhood obesity.
What does this article add?
We found the mediating role of home food environment in the relationship between two different types of parental stress and child diet patterns.
What are the implications for health promotion practice or research?
Future research will consider subgroup differences for racial or ethnic minority families (in which childhood obesity is more prevalent) and for socioeconomically disadvantaged families. Additionally, future research needs to explore the etiology of different types of stress and coping strategies, so how these stresses are related to child health behaviors and weight. Finally, developing intervention programs need to be considered to improve home food environment by promoting parental stress management, thus improving children’s diet patterns and reducing childhood obesity.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported by American Nurses Foundation.