
Abstract
Evidence-based program repositories (EBPR) report intervention characteristics and how to implement the intervention. These EBPR are a dissemination strategy to address questions such as, “I have cancer, what programs can I join?” or “What evidence-based programs for weight loss are a good fit for my community?” However, these EBPR fall short of realizing their potential and are not seen as particularly interactive, robust, or relevant to stakeholders who may benefit from their content. We propose 2 solutions for existing EBPR to enhance dissemination of evidence-based information. Addressing this critical dissemination need is one strategy for health promotion.
Keywords
Introduction
Imagine the following scenario: In an upcoming community-research partnership meeting, community members will review potential gestational weight gain interventions to implement in their community. One of the members, Sarah, is a retired nurse who serves as a community stakeholder. To prepare for the meeting, Sarah looks for information from 4 repositories: the e-Library of Evidence for Nutrition Actions (eLENA; managed by the World Health Organization, 1 The Community Guide managed by the Centers for Disease Control and Prevention, 2 the National Implementation Research Network centered at UNC Chapel Hill, 3 and research-tested intervention programs (RTIPs) managed by the National Cancer Institute. 4
She makes a number of observations in her initial review of these 4 repositories. The layers of eLENA links and clear labeling make it highly accessible and usable; however, the global focus of the resources makes it challenging to find an intervention suitable for a rural county in a Southern state in the United States (and there is not a list of interventions for gestational weight gain). The National Implementation Research Network website has an impressive array of interactive and noninteractive resources including podcasts, videos, presentations, and workgroups, but the resources are about implementation not about the actual program content. Research-tested intervention programs has a rating system for quality and evidence of the listed interventions, but the search options are restrictive and do not lead her to a program to consider. Finally, while the Community Guide is searchable by 21 topics, the available topics do not relate to her target audience or behavior, and none of the results present a specific program.
Sarah’s frustration is unsurprising as numerous evidence-based program repositories (EBPR) exist but they are not used at the capacity to speed translation and impact public health. In fact, a review conducted by Burkhardt et al found that 20 repositories, including a range of 30 and 660 programs or interventions, have been in existence for an average of ten years. 5 While the purpose of EBPR was to support practitioners on how to select and deliver evidence-based programs, Burkhardt et al remarked that “much needs to be done to improve the ability of the registers to fully realize their purpose.” 5 Evidence-based program repositories have not fully realized their purpose because the content is not organized in a way community stakeholders need it, and there is lack of standardization on relevance and robustness of the interventions. The lack of standardization limits the ability to compare across programs, populations, and settings. Those who contribute to EBPR are likely aware and working to amend many of these issues, but they face several significant barriers: (1) many EBPR are a decade old with no funding to update the infrastructure; (2) many were developed with practitioners in mind rather than researchers, and simultaneously addressing the expectations of various audiences remains challenging; and (3) the lack of funding for EBPR restricts their ability to innovate and adapt. For example, funding was terminated for the National Registry of Evidence-based Programs and Practices, housed within the Health and Human Services Department’s Substance Abuse and Mental Health Services Administration. 6 This termination was perplexing given that there needs to be a “more scientifically rigorous approach to better inform the identification and implementation of evidence-based programs and practices.” 6
These repositories could benefit from reorganization and user-centered design. 7 Updated, organized repositories have the capability of speeding knowledge translation, improving capacity to deliver evidence-based information, and facilitate bidirectional communication to improve the relevance of the resources for practice partners. Here we highlight 2 possible solutions to advance EBPR. One illustrates the potential features and sustainability of a unified platform that is rigorously tested with the aim of assisting translation of EBPs. The other solution proposes application of social marketing strategies 8 to engage potential end-users in an efficient and speedy manner.
Solution 1: Platform for Evidence-Based Intervention Characteristics
One potential solution to improving EBPR is the development, dissemination, evaluation, and continued refinement of a state-of-the-art user-friendly portal that includes searchable intervention characteristics (eg, target audience, target behavior, costs), intervention materials, and implementation information related to adaptation, delivery, and evaluation. Each submitted intervention would undergo a rapid and standardized evaluation to determine rigor and relevance with definitions that are vetted and validated by both scientific and practice-based stakeholders. Individuals with a terminal degree can conduct review of EBP and serve as a research-practice liaison. Once an intervention and related materials had been reviewed, its description and packaged contents would be displayed on a unified portal. The portal would have a familiar modern look to consumer friendly websites such as Amazon or E-Bay. In this portal, researchers and practitioners could compare and contrast interventions in a “shopping cart” to determine which intervention best fits their needs. Intervention developers can disseminate interventions with others and tailor the information by the type of consumer (eg, fellow researchers, practitioners, etc). Other key features could include intervention reviews written by diverse individuals representing the “real-world” including researchers, participants, and community members who are applying the intervention in the field. This would also allow the intervention developer to track uptake, field feedback, and guide and assess adaptations. Essentially, this portal would generate a real-time Adaptome 9 to track adaptation type (setting, mode, delivery system), why the adaptation was made, and who suggested it (eg, their role in the intervention). 10 To improve sustainability, the portal can be funded in the similar model of journals (eg, society membership fees and open-access fees).
All the functions of the portal would follow human-computer interaction best practices, such as matching format to a target audience. 11 This includes strategic attention to interactivity, usefulness, engagement, ease of navigation, trust of the website content, and appeal. 12 -14 While these characteristics of the portal may seem minor, they are increasingly relevant as research evidence competes with social media influencers to commercial entities with strong marketing strategies. Evidence-based programs remain lost in translation when information is not clear, concise, and organized in user-friendly formats with explicit recommendations meeting the users’ needs. 15
One example is the frustration users may experience if the portal seems designed for researchers rather than community members. In the hypothetical scenario of Sarah (the community board member searching for a gestational weight control intervention), the complicated structure and theory-heavy content of the repositories seemed geared for D&I scientists, not community members who might be involved in participatory research. 7 Hence, there is a need to tailor sections of the portal to match target audience and match the information with the users. 16 A concise list of potential preliminary features and multi-level dissemination strategies are outlined in Table 1.
Desired Characteristics/Needs of Repositories.
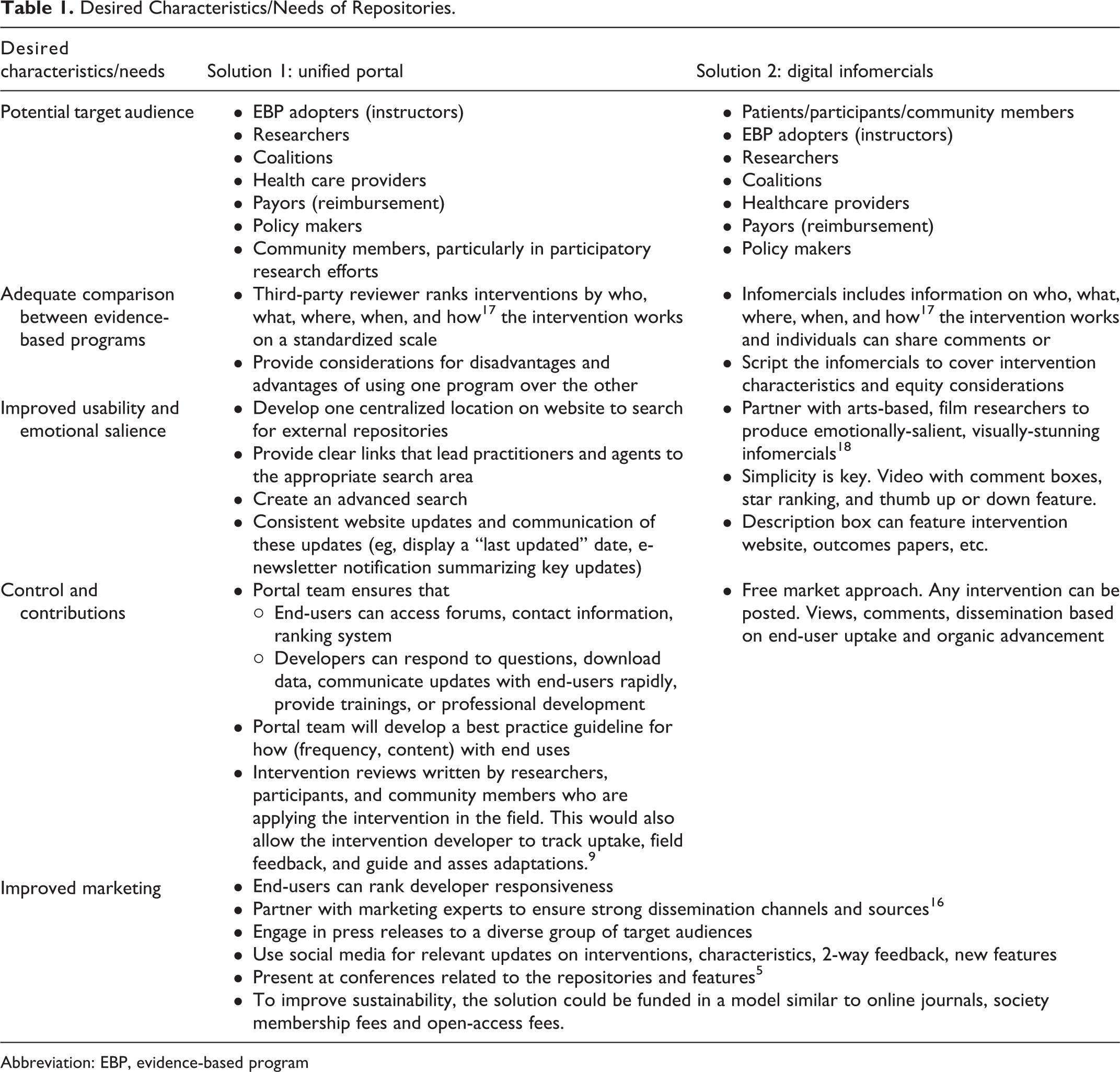
Abbreviation: EBP, evidence-based program
Notably, the usefulness of this portal is only as strong as its dissemination and successful implementation of EBIs, 16 which transdisciplinary work could advance. This transdisciplinary approach would involve many emergent fields such as engineering, human factors research, agile science, 19 public health, and health communication to advance the uptake of EBP and use of EBPR to facilitate awareness. However, this solution that relies on scientific fields (and values ascribed to those fields), not be as innovative, swift, or consumer-friendly as products and outputs in other fields.
Solution 2: Consumer-Friendly, Digitally Advanced “Marketing” Platform
While the scenario of the nurse stakeholder reviewing repositories aimed to be realistic, the more likely scenario in participatory research is that researchers glean the literature and present potential interventions for community members to consider. For example, community members on the Partnering for Obesity Planning and Sustainability-Community Advisory Board never searched the repositories; they chose a program for their community based on 3 options identified and presented by researchers. 20 Perhaps community members could have been involved in the initial steps of choosing a program if a consumer-friendly version of EBPR were available.
Therefore, Solution 2 involves developing a YouTube- or podcast-like channel on which interventions could be presented in short, descriptive videos similar to infomercials, explainer videos, or movie trailers—an EBP commercial. This platform could include standardized descriptions and a comment section to facilitate 2-way communication, crowdsourcing, and evaluation. Each infomercial would include detailed description of primary citations, costs, training needs, and other program logistics. This dissemination approach integrates communication science and social marketing to communicate intervention characteristics to diverse audiences, including nonacademic community members. Most importantly, this approach allows EBPR to harness the power of social media and keep up with the reality of communication in the digital age.
In the digital, fast-paced world, aesthetically pleasing, brief, and descriptive EBP commercials may be more impactful if they include key features of time, equipment, effect, measures, and testimonials. In this way, dissemination science matches communication science and marketing to commercialize intervention characteristics for delivery personnel, participants, community stakeholders, and researchers. 8,21,22 We suggest that these EBP “commercials” would be short, descriptive, and include a balance of quantitative and qualitative outcomes. For example, the video or podcast would include testimonials from individuals who have participated at different levels: delivery personnel describing the ease and enjoyment of delivering, participants sharing success stories, and researchers sharing the evidence base and adaptability of the intervention. Our suggestion for this approach stems from the rise and use of podcasts 23 -28 and YouTube 29,30 for health information. Essentially, people do a “simple internet search” 31 to find health information. We often forget that patients, health workers, researchers, physicians, and policymakers are people, too. Essentially, we need to meet the people where they are. This approach has the potential to pair EBP developers with experts from communication science, marketing, engineering, agile science, and even arts-based researchers, 18 truly elevating the influential side of dissemination science.
Despite the practical appeal of Solution 2, it may be challenging to galvanize researchers to make EBP infomercials/movie trailers and then keep up with the ongoing comment section. While the EBP commercial for the interventions may be a promising approach, there may also be a conflict between modern, effective dissemination tools (eg, YouTube) and scientific paradigms, incentives, worldviews, mental models of what constitutes success and skill sets. Finally, this free-market approach allows users to include and promote non-evidence-based programs, leaving the onus of discerning the level of evidence on the consumer, which could be problematic in this era of internet facilitate misinformation. Perhaps some type of crowdsourcing could be employed, as with Wikipedia to help users share experiences and collectively improve products.
How to Initiate these Bold Solutions
Passive diffusion of information through scientific outlets is insufficient to translate evidence-based information into the mainstream, and multiple strategies are suggested through a variety of sources and channels (eg, a dissemination strategy that includes reporting via social media, community forums, and peer reviewed literature). We propose that prototypes of both of these solutions be developed and evaluated. This could be funded through a Small Business in Research Grant from the National Institutes of Health or through leveraging other private/public partnerships. Each solution (Solution 1 = Unified Portal, Solution 2 = EBP Infomercials) could be evaluated through the RE-AIM framework (reach, effectiveness, adoption, implementation, maintenance). For example: Do people access it; how do they engage; can they identify a useful EBP; can they implement with fidelity and report adaptations? Evaluation would focus on the pragmatic “who, what, where, when, how” RE-AIM questions 17 to identify what populations were reached (and which not) and what impacts they have under different conditions of administration, at what cost, and so on. To capture this information, researchers could incorporate social media features such as clicks for “like” and “dislike.” Development and evaluation of each prototype would allow for exploration of potential mechanisms of dissemination that are triggered by each approach solution—contributing to theory within dissemination science.
Conclusion
We have presented 2 possible solutions to the problem of EBPR that may be helpful to clinical and community leaders. These could be combined—and are far from the only possible approaches—but they should start the conversation of ways to provide the “right information at the right time to the right person in the right modality in the right amount of detail.” 32 For example, an “on demand” EBPR librarian—either human or possibly even artificial intelligence—may be available to guide people and organizations on available EBP that may best suited for their needs and resources. This call to action can be a first step to inform funding announcements, partnerships, and opportunities. Any new platform would itself need to continue to evolve, keeping pace with the digital age, emerging rapid or real time data, incorporating new information related to ever-changing use and quality improvement, and fitting the dynamic needs of diverse users.
So What? (Implications for Health Promotion Practitioners and Researchers)
Evidence-based programs and evidence-based program repositories exist, but they are not reaching the intended audience or significantly increasing EBP uptake. Describing intervention characteristics to end-users is imperative to inform perceptions of fit, feasibility, adaptability, and sustainability in their intended settings.
We present a call to action for improved adoption and implementation through options including (1) an evidence-based, unified portal for intervention characteristics or (2) a digital, interactive marketing (or crowdsourcing) platform on intervention characteristics and implementation strategies.
These potential solutions spark discussions about the feasibility and impact of the two proposed solutions, and generate other alternatives to improve and evaluate the connectivity of intervention developers to their end-users.
Footnotes
Authors’ Note
SMH conceptualized with AS, and all co-authors contributed to the content and directions. All authors contributed to manuscript preparation and approval.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr. Estabrooks’ contribution was supported in part by the National Institute of General Medical Sciences, 1U54GM115458.