
Abstract
Background:
The study examined the association between sedentary behavior and self-rated health-related quality of life (HRQoL) in a sample of patients with multimorbidity in Singapore recruited from a primary care clinic.
Methods:
Sedentary behavior and physical activity were assessed with the International Physical Activity Questionnaire short form (IPAQ-SF). HRQoL was assessed with EuroQol-5 Dimension (EQ-5D) utility index, visual analogue scale (EQ-VAS) and its 5 subscales (Mobility, Self-care, Usual Activities, Pain/Discomfort, and Anxiety/Depression). Depression was assessed via Patient Health Questionnaire (PHQ-9). Logistic and linear regression analyses adjusting for the effect of physical activity, depression, and sociodemographic variables (i.e., age, gender, ethnicity, education) were conducted.
Results:
932 patients participated in the study (mean age:64.5±8.5 years, range: 35-80) and 55% were men. Results indicated that women were less likely to have sedentary behavior (≥7 hrs/day) than men. Results indicated sedentary behavior was associated with lower EQ-5D index scores, but not EQ-VAS scores. Participants who were sedentary for ≥7 hrs/day were more likely to endorse having problems with mobility, self-care, and usual activities, but not with pain/discomfort, nor anxiety/depression.
Conclusion:
Sedentary behavior was associated with poorer HRQoL. There is a need for interventions and health promotions to reduce sedentary behavior in patients with multimorbidity.
Keywords
Background
Multimorbidity is defined as the coexistence of two or more chronic physical and mental conditions within the same individual. 1 It is distinct from comorbidity, as the primary chronic condition of an individual with multimorbidity need not be defined. 2 Multimorbidity is currently a major public health issue that poses a challenge to health care systems globally and is associated with complex care management, lower quality of life, 3 increased psychological distress 4 higher perceived stress levels 5 , as well as substantially higher economic and social care costs. 6 In a systematic review of 39 studies in 12 countries, the estimated prevalence of multimorbidity ranged from 12.9% in participants aged 18 years and older, to 95.1% in adults aged 65 and older. 7 Furthermore, studies indicate that the number of morbidities increases substantially with age, 8 with reports of prevalence ranging from 55% to 98% in older adults. 9 With the projection that the proportion of adults over 60 years in the world is expected to increase to a total of 2.1 billion (i.e., 1 in 5 people) in 2050, 10 it is essential for health-care systems to possess the necessary information to address multimorbidity in an aging population. Furthermore, systematic reviews have indicated that multimorbidity is associated with an increase in health-care utilization outcomes (physician use, medication, emergency care, and hospital admissions) and a near-exponential increase in health-care costs (medication, out-of-pocket, total health-care costs). 11,12 Additionally, there have been reports that the cost to older adults with multimorbidity are 2.1 to 5.5 times higher than for those without. 13,14 In essence, there is an urgency to examine and understand the characteristics of individuals suffering from multimorbidity as a means to identify any modifiable risk factors for resource allocation and interventions.
There has been considerable research expounding the benefits of physical activity on both physical and mental health, 15 as well as HRQoL. 16 Regular physical activity has been shown to act as both primary and secondary prevention for a vast range of chronic diseases. 17 On the other hand, physical inactivity, or sedentary behavior, is defined as activities that do not substantially increase energy expenditure above resting levels and involve a sitting, reclining, or lying down position. 18 It is important to note that sedentary behavior is not the absence or presence of physical activities, and is not the opposite of physical activity, as an individual may be classified as both active and sedentary (e.g., meets physical activity recommendations, but spends a substantial part of time sedentary). 18,19 Furthermore, an increasing pool of literature indicates that physical activity and sedentary behavior influence health via different physiological processes 20 and that the detrimental effect of sedentary behavior on health is independent of physical activity. 21 Research has demonstrated these negative effects of sedentary behavior on health, with increased risk of type 2 diabetes, 22 cardiovascular disease, 23,24 more than 10 types of cancer, 20 all-cause mortality, 25 and increased health-care costs. 18 However, findings on the relationship between sedentary behavior and HRQoL are contradictory. A meta-analysis by Boberska et al 26 indicated that lower levels of sedentary behaviors were associated with better physical component of HRQoL, but not with the mental component of HRQoL. Furthermore, a study by Loprinzi 27 found that there was no significant association between sedentary behavior and HRQoL. In contrast, a longitudinal study reported that sedentary behavior during leisure time was negatively associated with HRQoL. 28 With studies showing the association between sedentary behaviors, and increased odds of having multimorbidity, 27 it is important to understand the impact of sedentary behavior on health outcomes in patients with multimorbidity.
Singapore is a multi-ethnic Southeast Asian country with a rapidly aging population. Prevalence of multimorbidity in Singapore ranges from 16.3% 29 to 51.5%. 6 It is estimated that by 2050, 40.1% of Singapore’s population will be aged 60 and above, 10 and as such, the prevalence of multimorbidity is expected to increase significantly. Unfortunately, there is a dearth of studies examining the relationship between sedentary behavior and HRQoL, especially in patients suffering from multiple chronic diseases. Therefore, this study aims to investigate the association between sedentary behavior and HRQoL in a sample of patients with multimorbidity in Singapore, while accounting for the effects of physical activity levels and depression.
Methods
Sample
This cross-sectional study is part of a larger study aimed at examining different characteristics of patients with multimorbidity in a primary care setting and was conducted at a National Healthcare Group (NHG) primary care clinic between August 2014 and June 2016. Inclusion criteria for patients included: (i) aged 21 years and older, (ii) current coexistence of the 3 most prevalent chronic illnesses; hyperlipidemia, hypertension, and diabetes mellitus Type 1 or 2, (iii) ability to understand spoken English, Mandarin, Malay, or Tamil, and (iv) were seen at the NHG primary care clinic at least twice within 6 months prior to recruitment.
Various sample sizes were calculated in order to achieve the primary goal of the study, which is to examine multimorbidity in a primary care setting. The largest sample size was utilized in order to ensure adequate power to answer all research questions. Taking into account 5% missing data, a sample size of 892 was estimated. Assuming a 50% response rate, a sample size of 1800 was considered reasonable. Therefore, 1800 patients who met the inclusion criteria were randomly drawn from the patient population and tagged using the clinic list. As only one research assistant worked full time on the project, the sample was released in 4 replicates, ensuring a good outreach. Potential participants were identified from the electronic medical record system and referred to trained research assistants by clinicians and front-line staff before/during/after their scheduled appointments. In total, 1366 patients were approached for the study, out of whom 932 patients agreed to participate—resulting in an acceptable response rate of 68.2%. All participants included were clinically stable (not acutely ill) and were determined to be cognitively capable of providing informed consent. Trained research assistants conducted a 30-minute interview in the participants’ language of choice, and their answers to the study questionnaire were entered onto the QuickTapSurvey (www.quicktapsurvey.com) application on a tablet computer. Upon completion, participants were compensated SGD 30 as an inconvenience fee. Ethics approval for the study was obtained from the relevant ethics committee (Domain Specific Review Board, National Healthcare Group, Singapore), and all respondents provided written informed consent before participating in the study.
Measures
Health-related quality of life
The EQ-5D-3L 30 is an instrument that measures HRQoL which comprises a descriptive system and a Visual Analogue Scale (EQ-VAS). Rated on a 3-point scale (1 = no problems, 2 = some problems, 3 = extreme problems), the descriptive system comprises 5 items which represent 5 dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. A possibility of 243 health states can be obtained by combining one level from the respondents’ answers on each of the 5 dimensions. These different health states are then converted into a single utility index. The utility index for the present study was calculated based upon the algorithm derived from the time trade-off values within the general population of Singapore. 31 This calculation yields a perfect score of 1 for health state 11111, and ranges from 0.854 for state 11121, and -0.769 for state 33333. This method of calculating utility index scores has been well validated by studies within the general population of Singapore. 31,32 Higher scores on the utility index indicate better HRQoL. To identify whether respondents endorsed having issues with the 5 dimensions of the EQ-5D, participants’ response on each item were dichotomized (having no problems vs. having moderate/extreme problems). The EQ-VAS provides a single global rating of self-perceived health on a vertical scale 0 to 100 mm that ranges from “the worst imaginable health state” to “the best imaginable health state.”
Sedentary behavior
The International Physical Activity Questionnaire short form (IPAQ-SF) 33 is a 7-item instrument that measures an individual’s physical activity in the last 7 days. The first 6 items of the IPAQ-SF ask about 3 specific types of activity, namely: walking, moderate-intensity activities, and vigorous-intensity activities. Respondents are then asked about the specific number of days and amount of time in hours and minutes which they had spent doing each of these activities in the last 7 days. Physical activity levels and their correlates were examined in an earlier paper, 34 but its effects on HRQoL are accounted for in the present study. The last item on IPAQ-SF, “During the last 7 days, how much time did you spend sitting on a week day?” was utilized as the measure for sedentary behavior in this study. Respondents provided their answers in hours and minutes per day. A ≥7-hours/day cut-off was applied to differentiate between levels of self-reported sedentary behavior as recommended by a systematic review 35 and a meta-analysis. 36
Depression
Depression was measured by the Patient Health Questionnaire (PHQ-9), a 9-item self-administered instrument that is based upon the diagnostic criteria of major depressive episodes from the Diagnostic and Statistical Manual of Mental Disorders, fourth Edition. 37 The developers suggest that scores of 5, 10, 15, and 20 correspond to mild, moderate, moderately severe, and severe depression, respectively. 37 The PHQ-9 has been well validated within primary care patients in Singapore, with studies recommending an optimal cut-off score of ≥6 for the screening of depression. 38,39 Therefore, individuals who had PHQ-9 scores of <6 were classified as “Minimal or no depression,” while those with scores ≥6 were grouped as “At least mild depression.” The PHQ-9 had good internal consistency (Cronbach’s α = 0.72) within the present sample.
Sociodemographic Data
Sociodemographic information such as age, gender, ethnicity, marital status, education level, and monthly household income were obtained during the interview. To facilitate interpretation of the data, the ages of respondents were categorized as: “less than 55,” “55 to 64,” “65 to 74,” and “equal to or larger than 75.” Similarly, the ethnicity of participants was categorized as Chinese, Malay, Indian, and Others. Education was categorized into 4 groups: “no formal education,” “Primary,” “Secondary,” and “Post-secondary”; while Monthly household income was grouped into: “Less than SGD 2,000,” “SGD 2,000 to 3,999,” “SGD 4,000 to 5,999,” “SGD 6,000 to SGD 9,999” and “$10,000 and above.”
Statistical Analysis
All statistical analyses were conducted with SPSS version 23. Frequencies and percentages were calculated for categorical variables, while means and standard deviations were calculated for continuous variables. 25.54% (n = 238) of participants refused to provide information regarding their monthly household income and were thus treated as missing data. As such, the variable monthly household income was not included in regression models due to missing data. However, regression models with monthly household income are available upon request from the authors. Firstly, a logistic regression analysis was conducted to examine whether any sociodemographic variables (i.e. age, gender, ethnicity, and education) and depression were associated with sedentary behavior. Secondly, linear regression analyses controlling for the effect of physical activity, depression and sociodemographic variables (i.e. age, gender, ethnicity, education) were utilized to examine the association between sedentary behavior and EQ-5D utility index, and EQ-5D VAS scores. Five logistic regression analyses were then conducted on the binary outcomes of the EQ-5D subscales while adjusting for the effect of physical activity, depression and sociodemographic variables (i.e., age, gender, ethnicity, education). For regression models examining the outcomes of the utility index, EQ-5D VAS, and EQ-5D subscales, only estimates regarding the variable of interest, sedentary behavior will be displayed and discussed. Full model estimates are provided within Supplemental Appendices.
Results
There were 932 participants with multimorbidity (mean age: 64.5, standard deviation: 8.5, range:35-80. There were 115 participants (12.3%) who were less than 55 years of age, 330 (35.4%) were between 55 and 65, 360 (38.6%) were between 65 and 75, while the remaining 127 (13.6%) were aged 75 or older. The majority were male (55%, n = 513), and of Chinese ethnicity (82.5%, n = 769). The participants’ characteristics grouped according to sedentary behavior are presented in Table 1.
Characteristics of the Sample (n = 932) Grouped According to Sedentary Behavior.
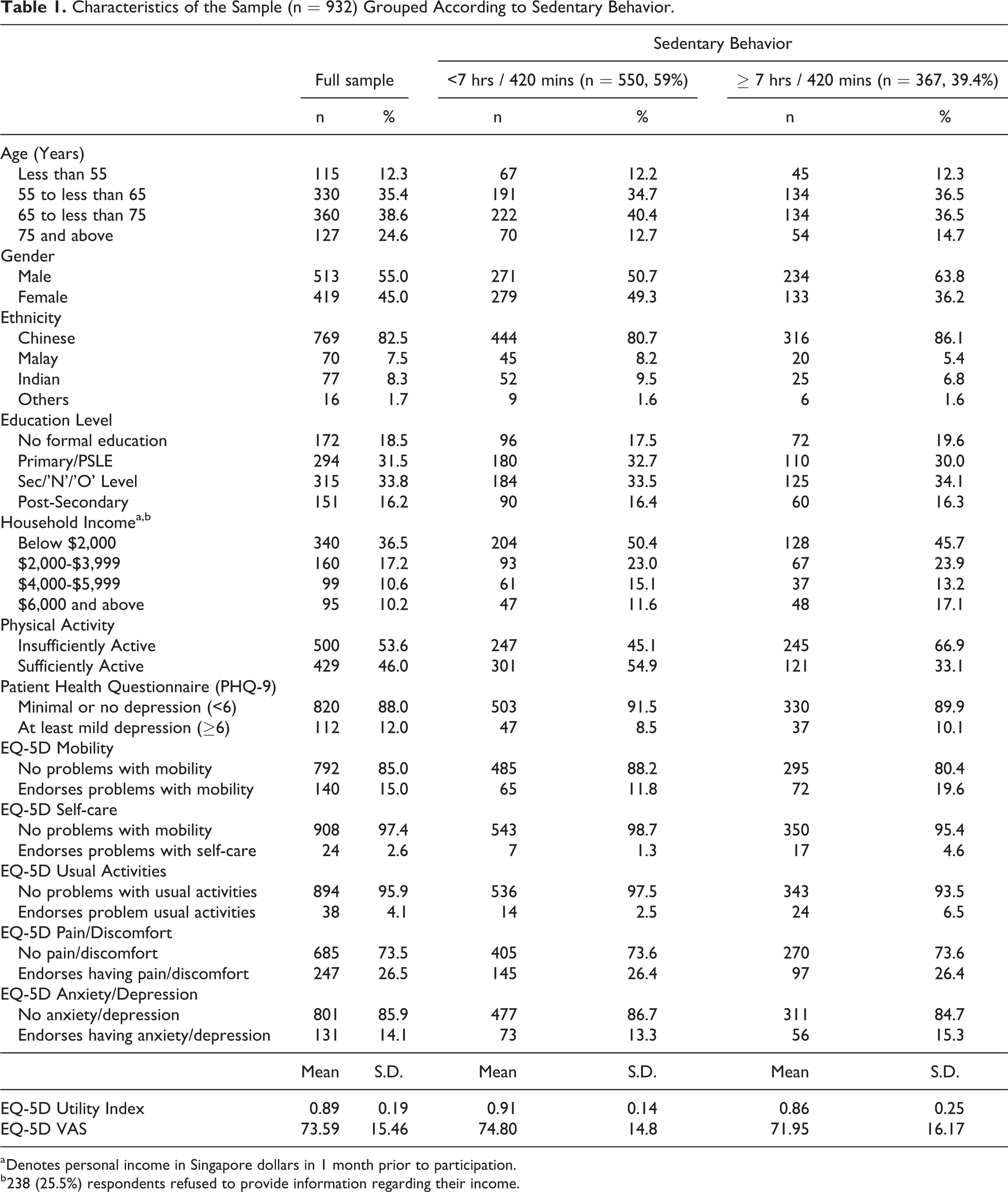
a Denotes personal income in Singapore dollars in 1 month prior to participation.
b 238 (25.5%) respondents refused to provide information regarding their income.
Correlates of Sedentary Behavior
Logistic regression analysis indicated that of the sociodemographic variables, only gender was significantly associated with sedentary behavior. Results of this model can be found within Table 2. Compared to males, females were less likely to have ≥ 7hours/day of sedentary behavior (OR: 0.53, 95% CI: 0.40 to 0.71, p < 0.001).
Results of a Logistic Regression Analysis Examining the Sociodemographic Correlates of Sedentary Behavior.
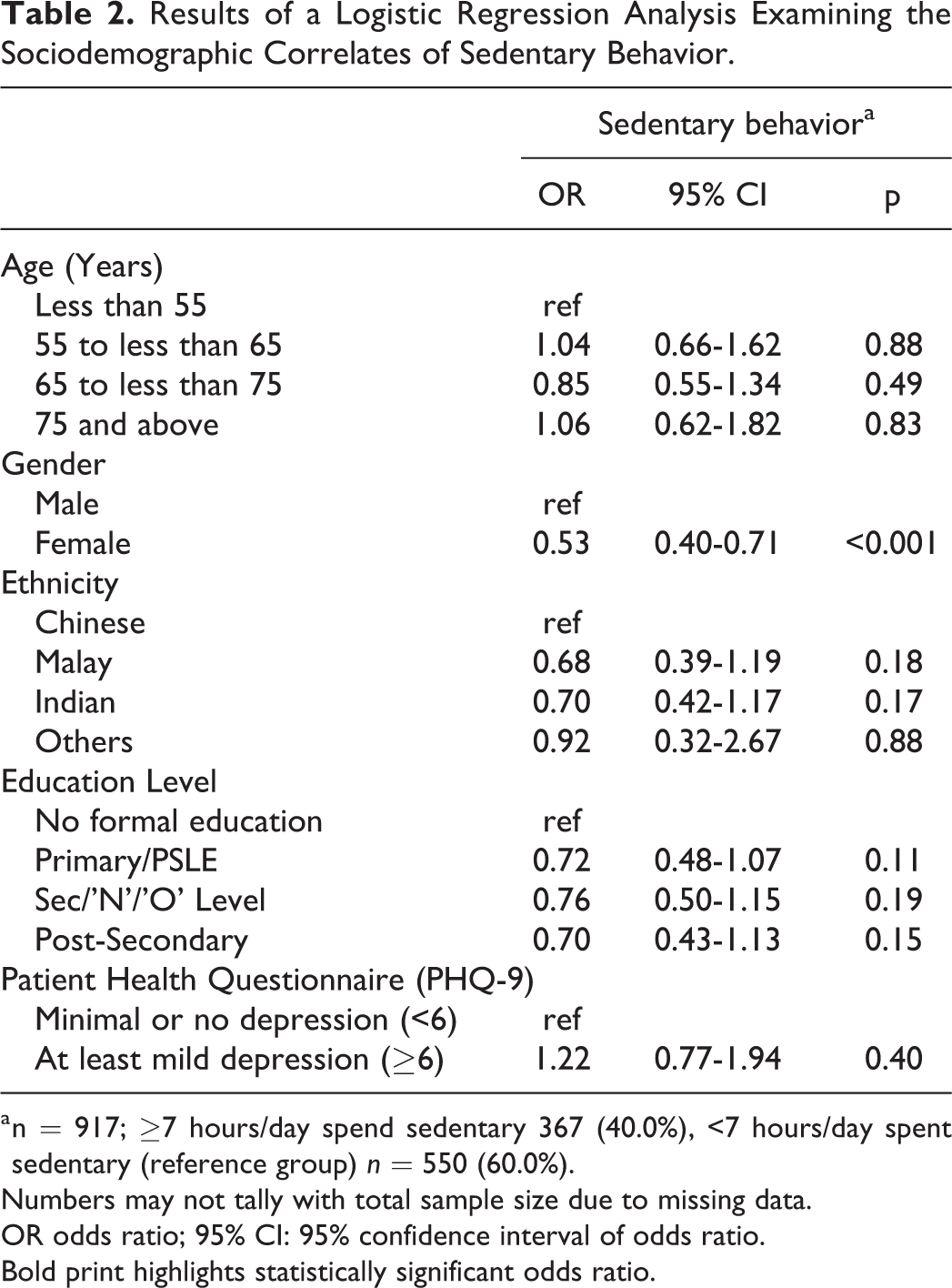
a n = 917; ≥7 hours/day spend sedentary 367 (40.0%), <7 hours/day spent sedentary (reference group) n = 550 (60.0%).
Numbers may not tally with total sample size due to missing data.
OR odds ratio; 95% CI: 95% confidence interval of odds ratio.
Bold print highlights statistically significant odds ratio.
Sedentary Behavior and HRQOL
Results of the linear regression analyses examining the association between sedentary behavior and EQ-5D as well as EQ-VAS, while controlling for the effects of physical activity, depression, and sociodemographic variables (age, gender, ethnicity, and education), are presented in Table 3. The full models examining the correlates of EQ-5D and EQ-VAS that displays all control variables can be found in Supplemental Appendix A. Results indicated that having ≥7 hrs of sedentary behavior was associated with lower EQ-5D index scores (i.e. poorer HRQOL) (B= -0.05, 95% CI: -0.07 to -0.02, p < 0.001). However, sedentary behavior was not significantly associated with the EQ-5D VAS (p = 0.09).
Linear Regression Results of Sedentary Behavior and Its Association With HRQOL (EQ-5D Index and EQ-5D VAS).
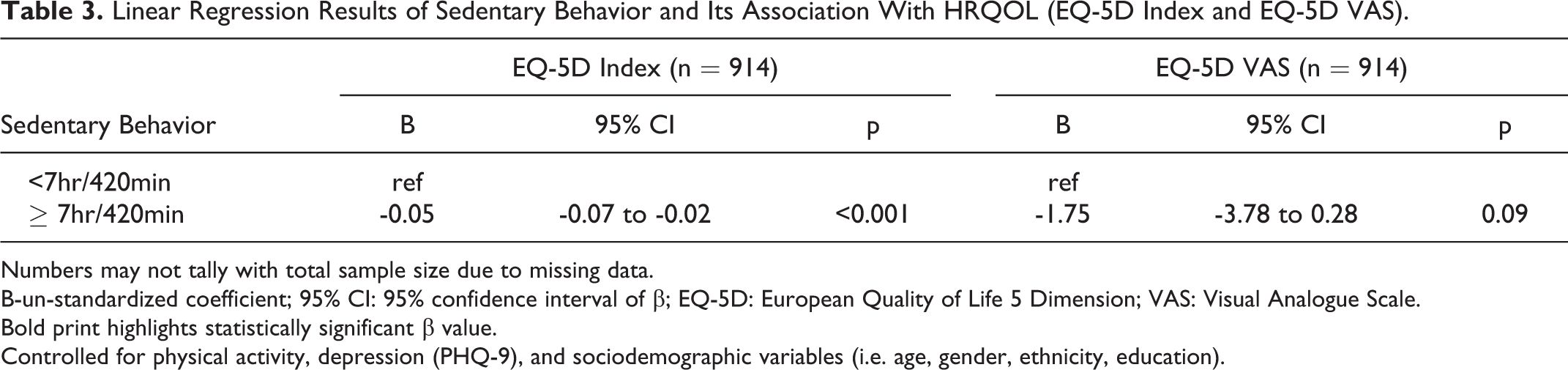
Numbers may not tally with total sample size due to missing data.
B-un-standardized coefficient; 95% CI: 95% confidence interval of β; EQ-5D: European Quality of Life 5 Dimension; VAS: Visual Analogue Scale.
Bold print highlights statistically significant β value.
Controlled for physical activity, depression (PHQ-9), and sociodemographic variables (i.e. age, gender, ethnicity, education).
Results of the logistic regression analyses assessing the association between sedentary behavior and the subscales of the EQ-5D while adjusting for physical activity, depression, and sociodemographic variables are presented in Table 4. The full models examining the correlates of the 5 EQ-5D subscales that displays all control variables can be found in Supplemental Appendix B. Those with ≥7 hrs of sedentary behavior had a higher likelihood of endorsing issues with mobility (OR: 1.70, 95% CI: 1.14-2.53, p = 0.01), self-care (OR: 2.97, 95% CI: 1.16-7.62, p = 0.02), and usual activities (OR: 2.50, 95% CI: 1.21-5.15, p = 0.01). However, there were no significant associations between sedentary behavior and endorsements of pain/discomfort (p = 0.93) or anxiety/depression (p = 0.73).
Logistic Regression Results of Sedentary Behavior and Its Association With HRQOL (EQ-5D Subscales).
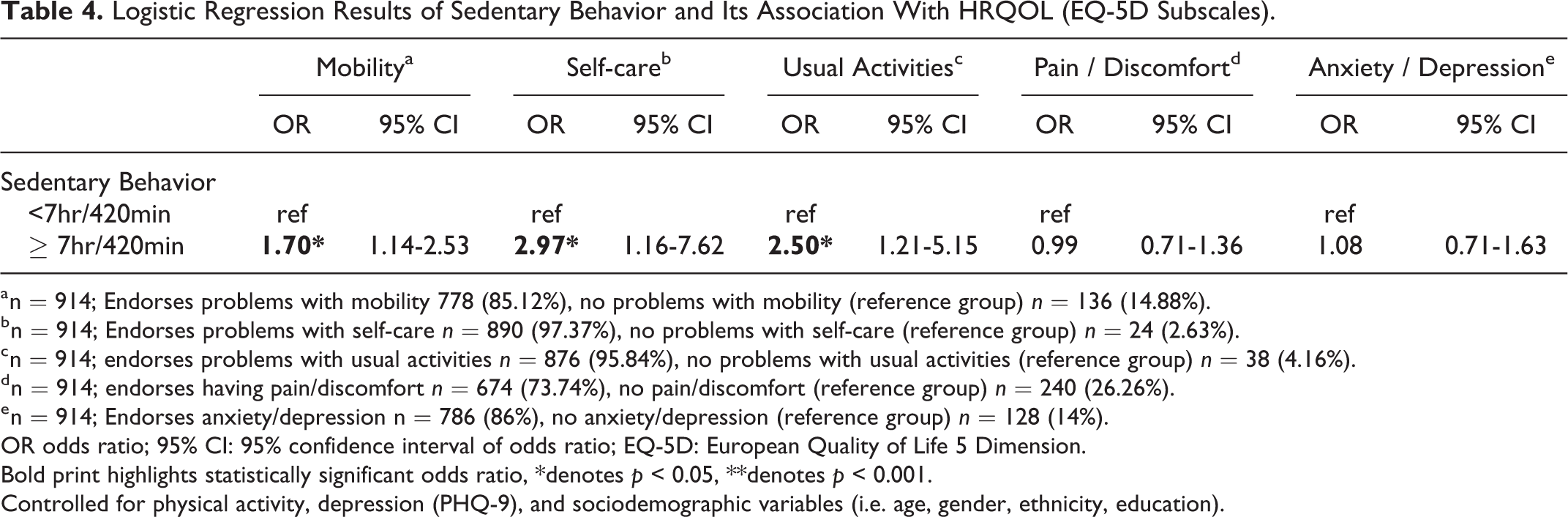
a n = 914; Endorses problems with mobility 778 (85.12%), no problems with mobility (reference group) n = 136 (14.88%).
b n = 914; Endorses problems with self-care n = 890 (97.37%), no problems with self-care (reference group) n = 24 (2.63%).
c n = 914; endorses problems with usual activities n = 876 (95.84%), no problems with usual activities (reference group) n = 38 (4.16%).
d n = 914; endorses having pain/discomfort n = 674 (73.74%), no pain/discomfort (reference group) n = 240 (26.26%).
e n = 914; Endorses anxiety/depression n = 786 (86%), no anxiety/depression (reference group) n = 128 (14%).
OR odds ratio; 95% CI: 95% confidence interval of odds ratio; EQ-5D: European Quality of Life 5 Dimension.
Bold print highlights statistically significant odds ratio, *denotes p < 0.05, **denotes p < 0.001.
Controlled for physical activity, depression (PHQ-9), and sociodemographic variables (i.e. age, gender, ethnicity, education).
Discussion
The present study examined sedentary behavior in a multi-ethnic sample of patients with multimorbidity. It has been recommended that an upper threshold of ≥7 hours/days should be utilized as a cutoff for sedentary behavior. 35,36 Considering this threshold, it appears that 39.4% of the sample have levels of sedentary behavior that puts them at increased risks for all-cause mortality. The present study also found that females were less likely to have sedentary behavior of ≥7 hrs than men. Two systematic reviews 40,41 regarding sedentary behavior among adults reported mixed findings on gender differences. While Rhodes et al 41 suggests that gender may not affect sedentary behaviors, O’Donoghue et al 40 reported that 10 out of 19 studies found that females had less sedentary behavior than men on total sitting, television/screen entertainment, and passive travel time. In a study utilizing accelerometer data, Bellettiere et al 42 found that among older adults, men were more sedentary than women in the morning, as women were likely to spend time on household activities/chores than men. However, it was not possible to delineate the gender differences in terms of specific domains (e.g. occupational, leisure, transport etc) as the IPAQ-SF only measures sedentary behavior in general. Nonetheless, this finding that male patients with multimorbidity have higher levels of sedentary behavior may highlight a need for further research to determine the domains in which this group differs from their female counterparts, so that recommendations can be made for a targeted intervention.
The present study lends further support to the evidence that sedentary behavior is negatively associated with self-reported HRQoL. Studies indicate that even when adults meet recommended guidelines for physical activity, being sedentary for prolonged periods may still compromise metabolic health (i.e., blood sugar, high density lipoprotein cholesterol, blood pressure, waist circumference), resulting in poorer overall health. 43 Moreover, the present study adjusted for the significant effects of possible confounders such as physical activity and depression in order to obtain a more accurate association of the effects of sedentary behavior on HRQoL, and the negative association between these two variables were still significant. Considering that adults spend the majority of their waking day sedentary. 44 this association between sedentary behavior and HRQoL is of utmost importance, especially since it is in a sample of patients with multimorbidity, who are already afflicted with multiplicative mortality risks. 45
The present study also revealed that sedentary behavior appears to be associated with having issues with mobility, but not with pain/discomfort. Vancampfort et al 46 found that in individuals with multimorbidity, both mobility difficulties and pain explained large variances in the association between chronic conditions and sedentary behavior, highlighting that these were important factors that may prevent patients from adopting or initiating an active lifestyle. The consensus on the association between sedentary lifestyle and pain (musculoskeletal pain or lower back pain) have been mixed, with some studies showing a positive relationship, 47,48 and others demonstrating a weak association, 49 and with a systematic review concluding no association. 50 Therefore, this study provides evidence that sedentary behavior may not be associated with pain/discomfort in patients with multimorbidity. In contrast, the association between sedentary behavior and impairments in mobility has been well documented in literature. For example, Santos et al 51 found that increased sedentary behavior negatively predicted physical functioning (scores on assessments such as chair stands, walking, and sit and reach). Therefore, reducing sedentary behavior could result in better functional mobility as well as health outcomes in patients with multimorbidity and improve their HRQoL.
The findings that sedentary behavior was associated with endorsements of having problems with usual activities and self-care are consistent with previous studies. A national study in the United States found that independent of moderate or vigorous physical activity, greater time spent in sedentary behavior was associated with the presence of disabilities in activities of daily living. 52 Furthermore, difficulties with basic and instrumental activities of daily living were common in individuals with multimorbidity, with studies showing that a greater number of chronic illnesses being linked to greater problems. 53
Two separate meta-analyses have revealed that higher sedentary behaviors were associated with greater risks of depression 54 and anxiety. 55 A study conducted in Myanmar and Vietnam among patients with chronic illnesses found that after adjusting for the effect of physical activity and relevant confounders, sedentary behavior was not associated with anxiety and depression. 56 In a similar vein, a study conducted in Japan also found no significant association between sedentary behavior and depression, and also that meeting physical activity requirements was associated with a lower risk of depressive symptoms, regardless of time spent sedentary. 57 Likewise, the current analyses adjusted for significant effects of depression as measured by the PHQ-9 and physical activity levels, and the results appear to suggest no significant association between sedentary behavior and depression/anxiety. Furthermore, sedentary behavior was not significantly associated with the PHQ-9 as well. The significant association between physical activity and depression/anxiety as reported previously by Subramaniam et al 34 may suggest that interventions advocating for increased physical activity levels, may be more suitable to reduce depression/anxiety in patients with multimorbidity. However, since the aforementioned studies also utilized self-report questionnaires for sedentary behavior, this non-significant association might warrant further investigation utilizing more objective measures of sedentary time. Furthermore, the depression/anxiety item of the EQ-5D in the present study may not have been sensitive enough to measure and elucidate the two complex constructs.
Limitations and Avenues for Future Research
Despite the significant findings of the present study, it possesses some limitations that might limit its validity. As mentioned briefly above, self-report measures of sedentary behavior are subjected to recall bias, 58 and therefore device-assessed measures such as accelerometers should be used. Ryan et al 59 compared accelerometer data with the IPAQ in a sample of older adults and found that the IPAQ showed weak reliability for total sedentary behavior, suggesting that the scale might not be suitable for assessing sedentary behavior. Furthermore, the IPAQ-SF only provides one general question on sedentary behavior, and does not measure sedentary time across different domains (e.g. occupational, leisure, transport), which would provide further opportunities to examine correlates of sedentary time within these domains, and identify areas for intervention. Despite these limitations, the findings do provide a starting point for future studies, which should utilize objective measures to elucidate further the relationship between sedentary behavior and HRQoL in patients with multimorbidity. Utilizing accelerometers as an objective measurement will allow future studies to examine sedentary bouts instead of an averaged daily sedentary time within patients with multimorbidity. This involves examining the number and length of periods an individual is sedentary without interruption throughout a day. Studies have revealed that the number of episodes and duration of sedentary behavior are associated with increased health risks. 60,61 Findings from such studies may provide better recommendations for patients with multimorbidity and help clinicians design interventions aimed at reducing sedentary behavior. The present study is also a cross-sectional study and thus, is unable to determine the cause-and-effect relationship between sedentary behavior and outcomes, especially since logic and extant literature indicate that mobility and sedentary behavior are highly linked with one another. Longitudinal studies are recommended to examine this relationship in further detail within patients with multimorbidity. The current study also did not account for the number of chronic illnesses and the length and severity of each illness. A meta-analysis and systematic review on multimorbidity has suggested that an increasing number of chronic conditions is associated with poorer HRQoL, and suggests that future studies should consider the length and severity of each disease to elucidate this association further. 62
Despite its limitations, the present study indicates a need for interventions aimed at reducing sedentary behavior. According to Owen et al, 43 sedentary behavior displaces time that may be spent in higher intensity physical activity, which therefore results in a reduction in overall physical energy expenditure. One potential method of dealing with this issue is via the isotemporal substitution paradigm, which estimates the effect of replacing one physical activity type with another physical activity type for the same amount of time (e.g., replacing TV watching with moderate physical activity). 63 It has been recommended that replacing sedentary behavior with an equivalent amount of low-intensity physical activity in adults may be more feasible than with moderate to vigorous physical activity, while still carrying a substantial benefit. 64 However, to date, no studies have examined isotemporal substitution in patients with multimorbidity. Since patients with multimorbidity require customized care that caters to the wide range of chronic conditions, not all patients may be able to replace sedentary behavior with physical activity due to physical conditions. Therefore, research on isotemporal substitution should identify and evaluate appropriate physical activities (e.g., less intense and safer activities such as household chores and climbing stairs) and examine whether these activities still provide substantial benefit for patients with multimorbidity.
Conclusion
In summary, the present study showed that sedentary behavior was an important health indicator among patients with multimorbidity in Singapore as it was associated with aspects of HRQoL, after adjusting for significant effects of physical activity levels and depression. Furthermore, the size of the sample as well as its sociodemographic characteristics, are representative of the Singaporean population. Given that the number of chronic conditions increase significantly with age, 8 health-care providers and policy makers should work toward reducing sedentary behavior in patients with multimorbidity to optimize their clinical outcomes, improve HRQoL and reduce health-care costs, especially since the population in Singapore is aging rapidly.
So What?
What Is Already Known on This Topic?
Multimorbidity is associated with poorer quality of life. Although regular physical activity has been shown to improve health-related quality of life (HRQoL), findings regarding sedentary behavior and HRQoL have been mixed.
What Does This Article Add?
This is the first paper within Singapore that examines the relationship between sedentary behavior and HRQoL within a sample of multi-ethnic patients with multimorbidity. The size and sociodemographic characteristics of the sample are representative of the Singaporean population. The analyses adjust for correlates of HRQoL such as physical activity and depression. Results indicate that females were less likely to have sedentary behavior (7≥hrs/day). Sedentary behavior was associated with poorer HRQoL, and increased likelihoods of endorsing problems with mobility, self-care, and usual activities.
What Are the Implications for Health Promotion Practice or Research?
The article indicates a need for health promotions to reduce sedentary behavior in patients with multimorbidity. Longitudinal studies that utilize objective measures for sedentary behavior, account for length, and severity of chronic illnesses are recommended.
Supplemental Material
Supplemental Material, sj-pdf-1-ahp-10.1177_08901171211001274 - Association Between Self-Reported Sedentary Behavior and Health-Related Quality of Life Among Multimorbidity Patients in Singapore
Supplemental Material, sj-pdf-1-ahp-10.1177_08901171211001274 for Association Between Self-Reported Sedentary Behavior and Health-Related Quality of Life Among Multimorbidity Patients in Singapore by Jue Hua Lau, Eng Sing Lee, Yunjue Zhang, Janhavi Ajit Vaingankar, Edimansyah Abdin, Siow Ann Chong and Mythily Subramaniam in American Journal of Health Promotion
Footnotes
Acknowledgments
MS, JAV, SAC, EA, and ELS conceptualized the design of the study, and ELS was the Principal Investigator of the grant. YZ provided input into the questionnaires used in the study, provided logistic support for patient selection and recruitment and led the data collection. EA and JHL provided statistical input for data analysis and interpretation. JHL conducted the literature review and wrote the first draft of the manuscript. All the authors provided intellectual input in the development of the article. All authors have read and approved the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research funding was provided by National Healthcare Group Small Innovative Fund, SIG/14030 J and the National Medical Research Centre Centre Grant-NMRC/CG/M002/2017 and NMRC/CG/C019B/2017. The funding bodies did not have any role in the design of the study and collection, analysis, and interpretation of data or in writing the manuscript.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.