
Abstract
Purpose:
To examine the association between weight loss and type 2 diabetes remission among vulnerable populations living in medically underserved areas of the Mid-Southern United States.
Design:
Quantitative, retrospective cohort study.
Setting:
114 ambulatory sites and 5 adults’ hospitals in the Mid-South participating in a regional diabetes registry.
Participants:
9,900 adult patients with type 2 diabetes, stratified by remission status, with 1 year of baseline electronic medical record data, and 1 year of follow-up data for the 2015-2018 study period.
Measures:
The outcomes were diabetes remissions, categorized as any remission, partial remission, and complete remission based on the guidelines of the American Diabetes Association. The exposure was weight loss, calculated by the change in the Body Mass Index (BMI) as a proxy measure.
Analysis:
χ2 tests, Fisher’s exact tests, and the Mann-Whitney U-test were used to examine the differences in patient characteristics by remission status across the 3 remission categories, as appropriate. Multiple multivariable logistic regressions adjusting for confounders were performed to estimate the adjusted odds ratios (aORs) for the associations between weight loss and diabetes remission.
Results:
Among 9,900 patients identified, a reduction of 0.3 kg/m2 (standard deviation: 2.5) in the average BMI from the baseline to the follow-up was observed. 10.8% achieved any type of remission, with 9.8% for partial and 1.0% for complete remissions. Greater weight loss was significantly associated with an increased likelihood of any (aOR = 1.07, 95% confidence interval (CI), 1.06-1.08), partial (aOR 1.06, 95% CI, 1.04-1.07), and complete diabetes remission (aOR 1.10, 95% CI, 1.07-1.13).
Conclusions:
Weight loss is significantly associated with diabetes remission among patients living in medically underserved areas, but complete remission is rare.
Purpose
Type 2 diabetes is a chronic disease, resulting in high morbidity, mortality, and healthcare expenditure, especially among low-income people and those residing in medically underserved areas.1,2 Suboptimal self-management of type 2 diabetes and poor glycemic control increase the risk of diabetes complications.3-6 Researchers have long known that weight gain and obesity are the main drivers of type 2 diabetes and poor glycemic control.7-10 Strong evidence demonstrates that obesity management is critical in diabetes treatment. Many studies have shown that modest and sustained weight loss is effective in improving glycemic control and reducing the need for pharmacotherapy in patients with type 2 diabetes and obesity.11-13 The American Diabetes Association recommends diet, exercise, and behavioral therapy to achieve at least 5% weight loss for overweight and obese patients with type 2 diabetes. 14 The United States Preventive Services Task Force (USPSTF) recently concluded that adults with obesity benefit most from behavioral weight loss interventions that are intensive and multicomponent.15-17
Recent evidence has demonstrated that intensive multicomponent weight loss interventions can also lead to diabetes remission, defined as achieving sustained glycemic control below the diabetic range without active pharmacologic therapy. 18 Specifically, large randomized control trials (RCTs), such as Look Action for Health in Diabetes trial (Look AHEAD) and Diabetes Remission Clinical Trial (DiRECT) suggest that intensive, primary care-led weight loss and lifestyle interventions can frequently result in type 2 diabetes remission.19-21 Although these clinical trials have found that exposure to primary care-led weight loss interventions was associated with improved average blood sugar (HbA1c) control and diabetes remission, little evidence is available regarding rates of remission and the association of weight loss with diabetes remission in community settings, especially among medically underserved populations at risk for health disparities.
However, little progress has been made addressing obesity in primary and specialty care settings. Low-income and African American patients are generally less likely to get recommended care for type 2 diabetes and other obesity related chronic conditions, 22 and as a result are much more likely to experience diabetes-related amputations, kidney failure, and premature death.23,24 Outpatient visit appointment adherence is generally associated with better diabetes management and control.25-27 But evidence suggests that during outpatient visits for diabetes care, patients are infrequently counseled about healthy eating, physical activity, and weight loss.15,16 And little is known whether more frequent outpatient visits are associated with increased diabetes remission in vulnerable underserved populations.
This study examines the incidence of and factors associated with remission among patients with type 2 diabetes from medically underserved areas of the American Mid-South. Furthermore, we examine how often low-income patients achieve varying levels of remission. In particular, we sought to determine whether weight loss is associated with diabetes remission in a cohort of community-dwelling patients with type 2 diabetes. The secondary objective is to examine whether higher outpatient visit frequency is associated with type 2 diabetes remission.
Methods
Design
This population-based, retrospective cohort study used data for 2015-2018 from a regional diabetes registry known as the Diabetes Wellness and Prevention Coalition (DWPC) Practice-based Research Network.28,29 The DWPC Practice-based Research Network includes electronic medical record data from 6 regional health systems, 5 adult hospitals within a non-profit integrated healthcare delivery system, a large multi-site federally qualified health center, and a total of 114 ambulatory sites. These health systems serve a large, majority medically underserved population located in the Memphis metropolitan statistical area of the Mid-South region of the United States (US).28,29 The data contains information on patient demographics, clinic and hospital encounters, diagnostic information, vital signs, and laboratory data.
Sample
Patients were identified during an index visit, defined as the first outpatient or hospital encounter in the period between January 2016-December 2017. Patients were included in the study if they met the following criteria during the index visit: 1) age ≥ 18 years, 2) HbA1c ≥ 6.5%, and 3) an eligible body mass index (BMI) (16 ≤ BMI ≤ 100).30-32 A one-year look-back window prior to the index date was used as a baseline period for each individual in order to completely assess baseline comorbidities and outpatient visits, and individuals were followed for 1 year from their index visit to assess diabetes remission (Figure 1). Additional inclusion criteria were: 1) 1 or more HbA1c test in the one-year follow-up period, and 2) and an eligible HbA1c (3.0% ≤ HbA1c ≤ 25.0%) value30-32 in the follow-up period. Patients were excluded from the study if they were diagnosed with type 1 diabetes in either baseline period or on the index date. Patients who underwent bariatric surgery at any time during the study period were also excluded. 33 The detailed diagnostic and procedure codes employed in cohort selection can be found in Online Appendix 1.
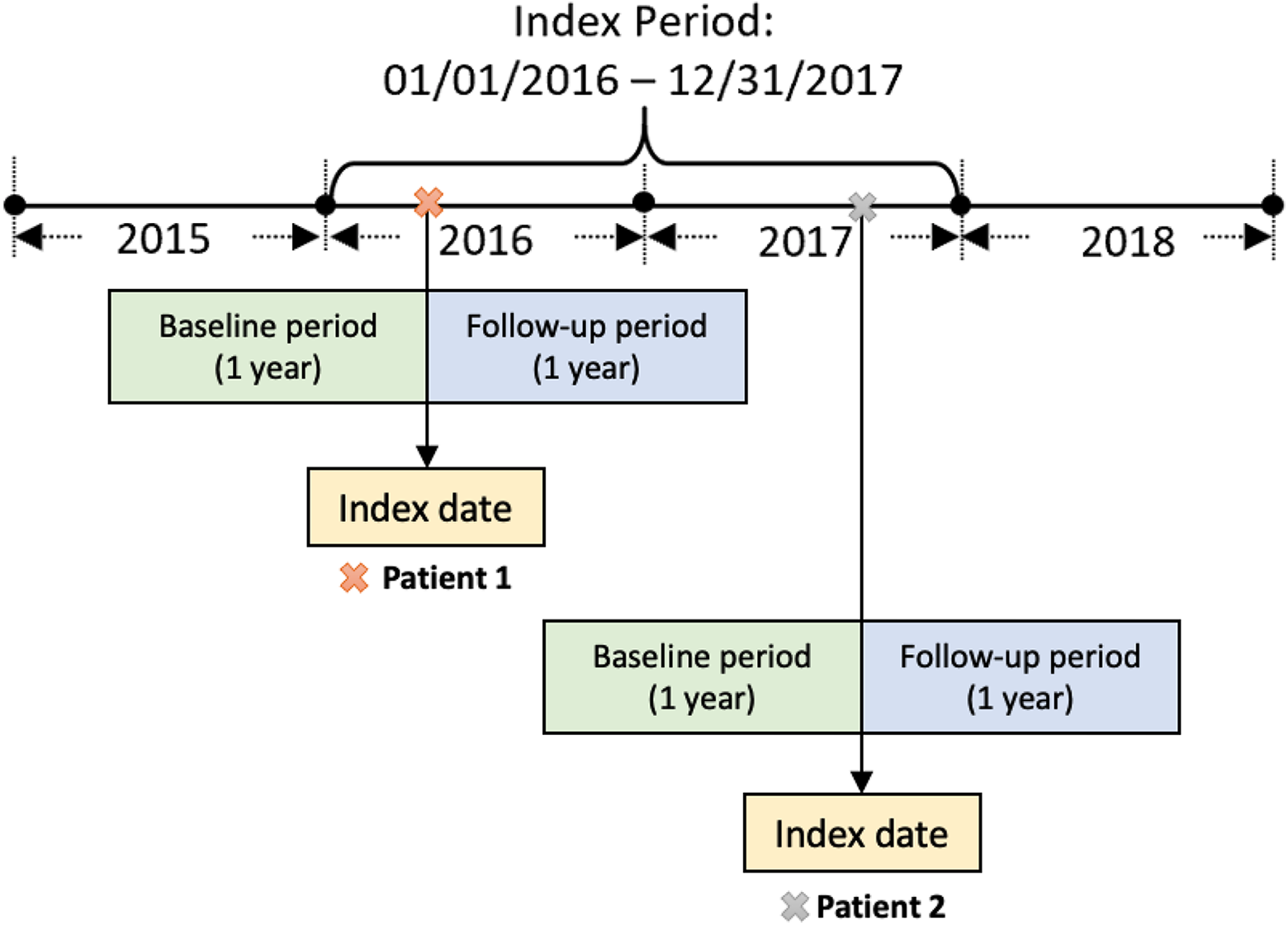
Retrospective cohort study design diagram with one-year baseline period and one-year follow-up period.
Measures
Diabetes remission
The primary outcome of interest was diabetes remission, which was defined based on the consensus statement from 2009 American Diabetes Association. 18 Patients were categorized into partial, complete, and any remission cohorts based on different ranges of HbA1c values in the follow-up period. 34 Partial remission of diabetes was defined as having any HbA1cvalue between 5.7% and 6.4% in the follow-up period. Complete remission was defined as having all HbA1c values < 5.7%. Any remission was defined as having either partial or complete remission (i.e., any HbA1c value < 6.5% in the follow-up period). 35 The date in the follow-up period upon which the patient met criteria for either partial or complete remission was defined as diabetes remission date.
Weight loss
The main independent variable was weight loss. We used BMI as a proxy measure for weight and defined weight loss as the change in BMI in kg/m2 measured as a percentage. BMI change was calculated by subtracting the follow-up BMI on the remission date from the index BMI and dividing this difference by the index BMI ((BMIindex-BMIfollow-up)/BMIindex * 100%). An increase in the percentage of BMI change indicated a reduction in BMI from index to follow-up. For patients who achieved remission, the BMI on the date of diabetes remission indicated as BMIfollow-up was used to calculate BMI change. Whereas for patients who did not achieve remission, the last eligible BMI in the follow-up period was chosen to assess the BMI change. In addition, outpatient visit frequency was assessed as the number of ambulatory encounters in the one-year baseline period.
Covariates
All covariates were measured at baseline either on the index date or for the one-year baseline period and included patient demographics and clinical factors. Patient demographics measured at the index date included age, gender, race, and residence in health profession shortage area (HPSA) and/or low-income area. Residence in HPSA and/or low-income area was identified by linking patient residence ZIP codes with the CMS database of HPSA and low-income ZIP codes, 35 with 4 categories as shown in Table 1.The areas with neither a HPSA nor a low-income designation were further used as reference group in the association assessment. Charlson Comorbidity Index (CCI) was calculated using ICD-9-CM and ICD-10-CM diagnostic codes (Online Appendix 1) for the one-year baseline period including index date. 36 CCI generates a total weighted score of the comorbidities and is an indicator for the comorbidity burden. The higher the score, the higher the comorbidity burden is. Detailed scores for each comorbidity are available in Online Appendix 1. The number of outpatient visits was measured both in the one-year baseline period and one-year follow-up period. We included the baseline outpatient visits in the adjusted model to assess whether outpatient visits assessed at baseline would be associated with diabetes remission in a one-year follow-up period.
Characteristics of Type 2 Diabetes Patients With and Without Remission (2015-2018).

Abbreviations: CCI, Charlson Comorbidity Index; HPSA, health professional shortage area; HbA1c, Glycated hemoglobin; SD, Standard deviation.
*Number of missingness in the variables: 1 (Gender), 2 (CCI).
† To visualize the direction and reduction status of HbA1c change which is indicated by the negative symbols, HbA1c change was calculated by subtracting the index HbA1c from the follow-up HbA1c on the remission date, that is, HbA1c change = HbA1c follow-up-HbA1cindex. The percentage of HbA1c change is by dividing HbA1c change over the index HbA1c. That is, percentage of HbA1c change = (HbA1c follow-up-HbA1cindex)/ HbA1cindex *100%.
‡Consistent with the calculation on HbA1c change, in this table, BMI change = BMIfollow-up-BMIindex. Percentage of BMI change was calculated by subtracting the index BMI in kg/m2 from the follow-up BMI in kg/m2 on the remission date and dividing this difference by the index BMI. That is, percentage of BMI change = (BMIfollow-up-BMIindex)/ BMIindex *100%.
Analysis
Baseline demographic and clinical characteristics of patients with type 2 diabetes who achieved remission (any, partial, and complete) versus those who did not achieve remission are presented in Table 1. Specifically, we compared baseline demographic and clinical characteristics of patients with type 2 diabetes who achieved: 1) any remission versus not, 2) partial remission versus not, and 3) complete remission versus not. For each remission group, differences by remission status (Yes/ No) in patient characteristics defined as categorical variables were assessed using χ2 tests or the Fisher exact test, as appropriate. Given that all continuous variables were non-normally distributed, differences in the continuous variables by remission status were tested using the Mann-Whitney U-test. Multiple multivariable logistic regression models with logit link and binomial distribution were performed to estimate the associations between BMI change, number of outpatient visits, and type 2 diabetes remissions (any, partial, and complete remissions, respectively) after adjusting for covariates described above. Separate regression models were constructed for each remission group. Adjusted odds ratios (aOR) and 95% confidence intervals (CIs) were reported. To test the robustness of findings, sensitivity analyses using a subpopulation with stricter inclusion criteria (i.e., requiring 2 or more HbA1c values in the follow-up period) were performed for each remission group. We used same definition for overall, partial, and complete remission that was used for our main analysis. Descriptive statistics and adjusted associations of the sensitivity analysis were reported (Online Appendix 2 and 3). All tests were 2-tailed, and a P value < 0.05 was considered statistically significant. All statistical analyzes were performed using SAS® 9.4 (SAS Institute, Cary, NC).
Results
A total of 9,900 adult patients were identified with type 2 diabetes who met full inclusion and exclusion criteria for the study period. Baseline characteristics of the study population are shown in Table 1 by diabetes remission cohort categories. Overall, the mean age for study subjects was 60.5 years (Standard deviation (SD): 13.0), 54.0% were female, and 51.9% were Black. Moreover, 50.0% of eligible patients resided in both an HPSA and a low-income area, 5.3% resided in a HPSA only, and 14.6% resided in a low-income area only. Wide variations in levels of comorbidity were noted, with CCI values ranging from 0 to 18 with a mean score of 2.6 (SD: 2.1). Baseline average outpatient visit frequency was 2.0 (SD: 1.2). Average index HbA1c was 8.2% (SD: 1.9%), and average BMI at index was 34.1kg/m2(SD: 8.1 kg/m2).
Among these patients (N = 9,900), 10.8% achieved any diabetes remission in their follow-up year, including 9.8% experiencing partial remission and 1.0% experiencing complete remission (Table 1). Overall, most of patients who achieved any remission were residents in the low-income, health professional shortage areas (48.2%) and had an average CCI of 2.3 ± 2.1 (mean ± SD).
Table 1 shows significantly lower index HbA1c values for the any and partial diabetes remission cohorts when compared to patients without remission (P < 0.0001). Compared to patients without remission, patients with type 2 diabetes remission experienced more reduction in HbA1c from index date to follow-up, and these findings were significantly consistent across 3 remission cohorts (P < 0.0001 for all comparisons). Likewise, greater weight loss, assessed as both BMI change and as percentage BMI change from index date to follow-up, was observed in patients who achieved remission compared with those who did not achieve remission (P < 0.0001 for all comparisons). Furthermore, outpatient visit frequency was significantly lower in all 3 remission cohorts compared to those without remission (P < 0.05 for all comparisons).
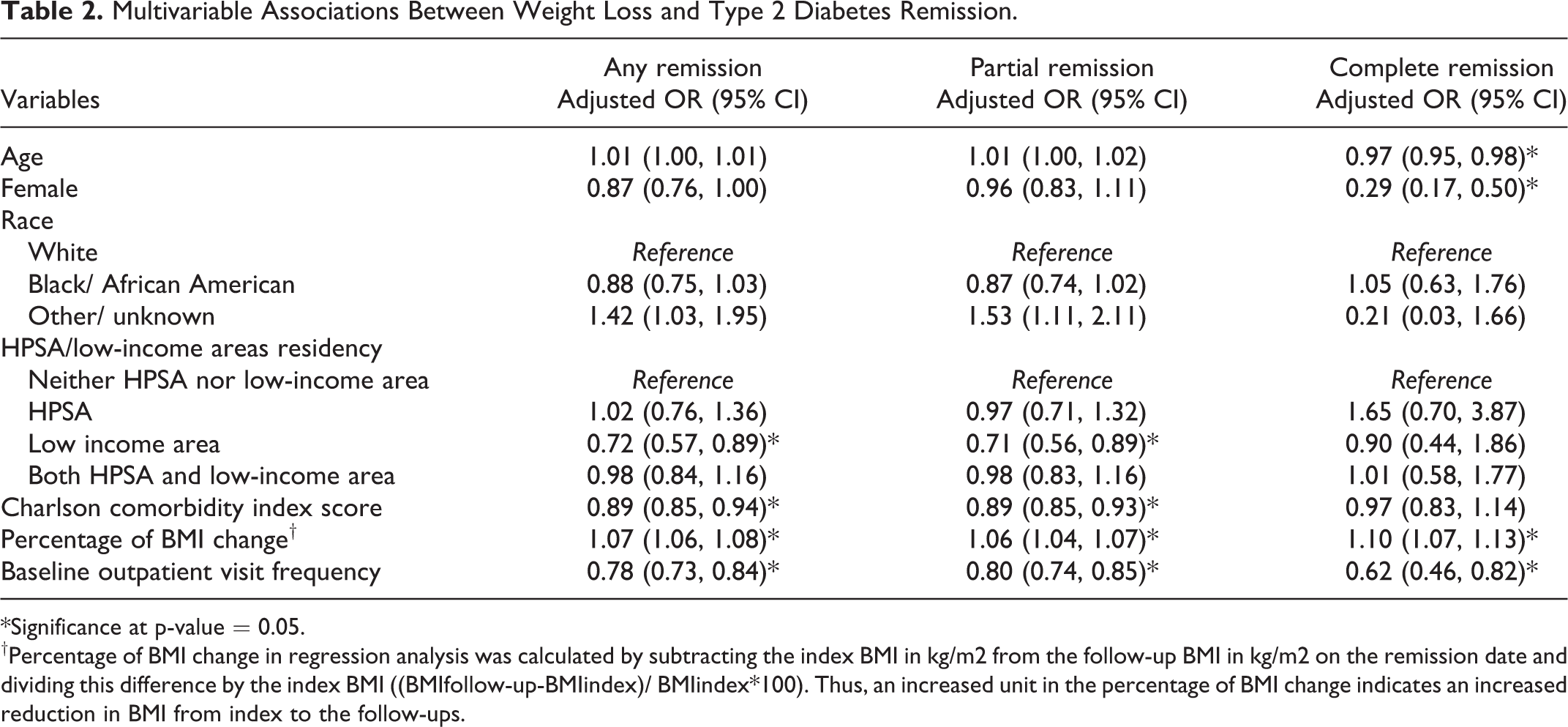
In Table 2, multivariable analysis demonstrated strong and consistent associations between weight loss and type 2 diabetes remission. BMI change and baseline outpatient visit frequency were the only significant factors association with diabetes remission across 3 remission groups. After adjustment for confounding factors, a BMI change of 1% reduction was associated with a 7% increase in the likelihood of any diabetes remission (aOR 1.07, 95%CI 1.06-1.08). Similar directions and magnitudes of associations of weight loss with remission were found in the partial and complete remission cohorts. In addition, less frequent outpatient visits were associated with increased likelihood of diabetes remission in all 3 remission groups.
Multivariable Associations Between Weight Loss and Type 2 Diabetes Remission.
*Significance at p-value = 0.05.
†Percentage of BMI change in regression analysis was calculated by subtracting the index BMI in kg/m2 from the follow-up BMI in kg/m2 on the remission date and dividing this difference by the index BMI ((BMIfollow-up-BMIindex)/ BMIindex*100). Thus, an increased unit in the percentage of BMI change indicates an increased reduction in BMI from index to the follow-ups.
Among patients who achieved either any or partial remission, residing in low-income areas was associated with decreased likelihoods of remission for both any (aOR 0.72, 95%CI 0.57-0.89) and partial remission (aOR 0.71, 95%CI 0.56-0.89) cohorts. Higher CCI scores were also associated with decreased likelihoods of remission for both any (aOR 0.89, 95%CI 0.85-0.94) and partial remission (aOR 0.89, 95%CI 0.85-0.93) cohorts.
In sensitivity analysis, the final analytic sample consisted of 4,765 adults with type 2 diabetes, including 344 with any type of remission, 318 with partial remission, and 26 with complete remission. Similar directions and magnitudes of the associations found in the main analysis were observed from the sensitivity analysis (Online Appendix 3).
Discussion
To our knowledge, the present study is among the first to provide a population-based assessment of the association between weight loss and diabetes remission among medically underserved patients. The use of a comprehensive regional diabetes registry and practice-based research network data28,29 ensures adequate study power and representativeness of our findings. Moreover, the findings of the current study replicate the findings of previous randomized clinical trials15,19-21,37 in a real-world setting. Specifically, we found that greater weight loss significantly increased the likelihood of type 2 diabetes remission in a predominantly African American, medically underserved, population in the Southern US. Our results provide additional evidence supporting the effectiveness of type 2 diabetes self-management through nonsurgical weight loss for vulnerable patients in medically underserved areas.
The current study provides further evidence to support a true causal effect of weight loss on diabetes remission with practical implications. A strong dose-response effect of weight loss on diabetes remission was demonstrated; significantly greater weight loss was seen in those with complete remission group versus those with partial remission. Dose-dependent effects of weight loss on remission have similarly been demonstrated in randomized clinical trials of both lifestyle and surgical weight loss interventions.20,37,38 Results from RCTs suggests that diabetes remission is much more likely to occur in participants with type 2 diabetes who were exposed to short-term intensive lifestyle interventions, and the likelihood of achieving remission with lifestyle intervention was higher than with pharmacotherapies.20,37 Furthermore, secondary analysis of RCTs provides supportive evidence that both level of weight loss and the likelihood of type 2 diabetes remission are dependent on the dose or intensity of lifestyle intervention. 38 Thus, the extent of weight loss may be a surrogate to indicate the intensity of lifestyle intervention, which is also an intermediate outcome between lifestyle intervention and diabetes remission. Using real-world data, the current study demonstrated similar dose-dependent effects of weight loss on diabetes control and diabetes remission among vulnerable patients in medically underserved areas of the Southern US. Although complete remission was rare in the medically underserved population examined in current study, it did occur and was highly associated with weight loss. Our study provides additional evidence pointing to the need of further pragmatic trials on the effectiveness of lifestyle intervention on weight loss and diabetes remission in this vulnerable population.
This association is biologically plausible, and we do not believe it is explained by alternative mechanisms. For example, it is possible that the cases of complete remission seen in the study population may have been caused by weight loss due to increased comorbidity, severity of illness, or cancer, since severe weight loss due to illnesses such as cancer has been commonly seen in practice. 39 However, this appears unlikely since the complete remission group experienced levels of both comorbidity and outpatient visit utilization that were similar to those of the partial remission group. Moreover, by comparing the extent of weight loss among patients with type 2 diabetes remission, we found those with complete remission had more weight loss than those with partial remission over similar time periods, indicating that the rate of weight loss was higher for those with complete remission. The finding of higher amounts and rates (i.e., intensity) of weight loss in patients with complete remission than in those with partial remission may also be attributed to a higher average baseline BMI and HbA1c level for the complete remission cohort. This finding is consistent with the results of the Italian Diabetes and Exercise Study, which demonstrated that the extent of HbA1c reduction achieved through weight loss intervention was highly dependent on baseline HbA1c levels. 40 Although this is not an intervention study, both BMI and HbA1c level changes may be subject to the ceiling effects in terms of the dose or intensity of an intervention. Patients with lower baseline BMI and HbA1c levels are more insensitive to change and are more likely to experience ceiling effects compared with those with higher baseline BMI and HbA1c levels. Also, we suspect that patients with higher baseline HbA1c and BMI may have been more likely to experience greater weight loss because: 1) higher average levels of blood sugar are associated with more glucosuria and weight loss caused by loss of calories through the urine, and 2) patients with higher BMI and HbA1c are more likely to receive more intensive pharmacologic and behavioral (e.g., weight loss) therapies.4,5,7,15
We did not find a significant association between higher outpatient visit frequency and type 2 diabetes remission. To the contrary, those who achieved remission had fewer outpatient visits, suggesting that outpatient visits did not effectively assist patients in achieving diabetes remission by any mechanism, either through supporting weight loss self-management or through improvements in pharmacotherapy. This finding is likely in part due to confounding by indication secondary to decreased comorbidities and/or severity of illness among patients who achieved remission. Indeed, patients with remission were found to have lower levels of comorbidity as measured by CCI scores in the baseline year. However, even after adjustment for comorbidity, more frequent outpatient visits were not associated with type 2 diabetes remission. This observed lack of benefit is consistent with studies showing that weight loss counseling for obesity is uncommon in outpatient care settings. 13 While the prevalence of obesity in the US population has dramatically increased particularly among the underserved, the number of patients receiving counseling to encourage weight loss in primary care settings has declined substantially. Similarly, second line diabetes medications associated with weight loss are underutilized in both primary and specialty care settings. 13 Additionally, we found that the odds of achieving overall and partial diabetes remission after adjusting for confounders were 28% and 29% less likely to occur among patients living in low-income areas than those living in neither HPSA nor low-income areas. It was likely that patients living in low-income areas had limited access to primary care and/or low adherence to scheduled medical appointments, which would lead to poor diabetes metabolic control.25,26
Thus, our results suggest that outpatient providers in medically underserved areas are not routinely providing recommended intensive multicomponent weight loss interventions for patients with obesity.15-17 Previous studies have clearly demonstrated that for primary care-based lifestyle interventions to be effective in achieving weight loss, they must be intensive. The Look AHEAD and DiRECT randomized clinical trials and the Italian Diabetes and Exercise Study have shown that intensive lifestyle interventions are highly effective in controlling HbA1c level and improving the clinical outcomes of type 2 diabetes management.19-21,40 Recently, Yoshino and colleagues provided preliminary evidence that intensive diet and weight loss support was as effective as surgical weight loss and that the benefits associated with both approaches were related to weight loss itself. 41 Further pragmatic trials are needed to assess alternative primary care-based approaches for supporting intensive weight loss and whether the differences in weight loss intervention intensity, number of components, and/or duration result in significant differences in type 2 diabetes remission in underserved populations.
The strength of this study is that the study findings are generalizable to similar underserved populations. Unlike the study by Karter et al that required 2 consecutive HbA1c tests in the follow-up period, 42 our study required only 1 or more HbA1c test in the follow-up period to increase the generalizability of the study findings. In our study, a substantial proportion of eligible patients with type 2 diabetes only received 1 HbA1c test during the follow-up period. To have a consistent evaluation with the previous study, we conducted a sensitivity analysis by selecting a subpopulation of those with 2 or more HbA1c tests in the follow-up period. We found similar results in terms of direction and magnitude when compared to the main findings.
There are several limitations to this study. First, because our study used a diabetes registry data consisting of comprehensive electronic medical records, certain diagnosis may be miscoded, which may affect the accuracy in comorbidities assessment. However, our analysis indicated that about 97.2% of the study sample with type 2 diabetes defined using HbA1c also presented an ICD-9 and/or ICD-10 diagnosis codes of type 2 diabetes (Online Appendix 4). Second, given our study has a higher representation of adult patients with type 2 diabetes residing in HPSA and low-income areas in the Mid-South, the results may not be generalizable to other populations. Third, adults with type 2 diabetes may have time-varying exposure to antidiabetic and/or other medications. Without control for such effects, the association between weight loss and the remission of diabetes may be affected. However, previous RCTs have suggested the substantial effects of lifestyle interventions on diabetes self-management and their associations with decreased risk of diabetes complications. 19 Our study aimed to evaluate the effect of weight loss as an intervention of diabetes self-management regardless of the medication effects. It is partially due to the limited access to medication and potential low- and non- medication adherence in this vulnerable population,43,44 and lifestyle intervention tends to be a more effective approach for diabetes control. Finally, we only looked at diabetes remission in a one-year follow-up period. Future studies should assess sustained long-term diabetes remission by considering longer follow-up.
Conclusion
In conclusion, this study using real-world data found that weight loss is significantly associated with diabetes remission among medically underserved patients, but complete remission is rare. Furthermore, this study demonstrates that for community-dwelling people with diabetes, routine outpatient care exposure does little to increase likelihood of remission even though effective primary care approaches to support weight loss have been demonstrated. This suggests that primary and specialty care providers can do much more to improve diabetes outcomes by adopting evidence-based approaches to support weight loss and diabetes remission in populations at risk of disparities. Further studies are needed to evaluate alternative pragmatic outpatient care-based interventions to support weight loss and increase rates of diabetes remission among vulnerable populations.
SO WHAT?
What is already known on this topic?
Randomized controlled trials demonstrate that intensive weight loss can lead to type 2 diabetes remission, but little is known from real-world settings. Real-world evidence generated from large population-based studies on the association between weight loss and type 2 diabetes remission among vulnerable patients in medically underserved areas is limited.
What does this article add?
Using a population-based observational design and comprehensive electronic medical records from a regional diabetes registry, this study found that weight loss is significantly associated with type 2 diabetes remission among medically underserved patients, but complete remission is rare. Although there has been evidence on effective primary care approaches to support weight loss, the likelihood of remission is not much improved through routine outpatient care exposure in community-dwelling adults with type 2 diabetes who are vulnerable and in medically underserved areas.
What are the implications for health promotion practice or research?
The findings from this study suggest that vulnerable patients with type 2 diabetes in real world settings who lose weight are much more likely to achieve remission. Primary and specialty care providers may be able to do more to encourage weight loss in vulnerable populations as a primary therapy for type 2 diabetes. Evidence-based approaches such as clinic-based multi-component weight loss programs including lifestyle interventions and nutrition education and support can be considered as part of routine diabetes management. Future efforts to evaluate the effectiveness of alternative pragmatic outpatient care-based interventions on weight control and diabetes management among vulnerable populations are needed.
Supplemental Material
Supplemental Material, sj-pdf-1-ahp-10.1177_08901171211024426 - Association of Weight Loss With Type 2 Diabetes Remission Among Adults in Medically Underserved Areas: A Retrospective Cohort Study
Supplemental Material, sj-pdf-1-ahp-10.1177_08901171211024426 for Association of Weight Loss With Type 2 Diabetes Remission Among Adults in Medically Underserved Areas: A Retrospective Cohort Study by Ming Chen, Satya Surbhi and James E. Bailey in American Journal of Health Promotion
Footnotes
Authors’ Note
The Institutional Review Board of the University of Tennessee Health Science Center approved this study (No. 18-06224-XP).
Acknowledgments
The authors acknowledge Ms. Nicky Hitching at the University of Tennessee Health Science Center on her assistance in reviewing and editing the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: All authors are supported by a Patient-Centered Outcomes Research Institute (PCORI) Project Program Award. The views expressed here do not necessarily represent the views of the PCORI, its Board of Governors or Methodology Committee. Support for this work was provided in part by the University of Tennessee Health Science Center College of Medicine and College of Graduate Health Sciences.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.