
Abstract
Purpose
To examine factors that facilitate an understanding of the relationship between two important, and often interchangeably used, concepts in diabetes management: compliance and adherence.
Design
A cross-sectional survey.
Setting
Online data collection.
Subjects
365 respondents at least 18 years of age and currently in treatment for diabetes.
Measures
We measured patients’ compliance, adherence, mindfulness, and perceptions about physician-patient communication, as well as their demographic characteristics.
Analysis
A moderated mediation analysis was conducted to examine the conditioned indirect effect of compliance on adherence.
Results
The direct effect of compliance on adherence was positive and significant (β = .378, SE = .073, P < .05, BootCI [.234, .521]), but the compliance-adherence association was also partially mediated by patient’s potential for mindful non-adherence. A higher level of compliance increased potential for mindful non-adherence (β = .716, SE = .082, P < .05, BootCI [.555, .876]), and, in turn, the increased potential for mindful non-adherence reduced adherence (β = −.107, SE = .045, P < .05, BootCI [–.196, −.018]). This detrimental mediating effect of potential for mindful non-adherence was contingent on the perceived quality of physician-patient communication (index = .076, SE = .038, 95% BootCI [.003, .153]), indicating that the positive perception significantly reduced the negative mediating effect of potential for mindful non-adherence on adherence.
Conclusion
Given that patients with diabetes are involved in a complex self-care, an established partnership and collaboration between patient and doctor is essential to promoting adherence; when the treatment coincides with the patient’s beliefs and needs, mindful non-adherence is less likely to occur.
Keywords
Purpose
Diabetes is one of the leading causes of blindness, amputation, end-stage renal disease, cardiovascular disease, and other acute complications. 1 It is also the seventh leading cause of death in the United States, affecting over 30 million people of all ages. 2 Research shows that 415 million people worldwide live with diabetes, and this number will continue to rise. 3 While Type 1 and Type 2 diabetes vary in their etiological, pathophysiological, epidemiological features,4,5 adherence to doctor-recommended treatments is critical to both Type 1 and Type 2 diabetes patients managing their diabetes and avoiding health complications. 1 Unfortunately, studies have shown that a large number of patients have difficulty with adherence to doctor-recommended treatments, 6 and non-adherence to recommended treatment regimens has been reported as a major barrier in the management of diabetes patients.7,8
In light of the importance of this issue, a substantial body of research has been conducted to examine compliance and adherence to medical instructions for patients with a variety of chronic illnesses, 9 including type 1 and type 2 diabetes.10-13 However, while the accumulated findings provide some consistent information on specific factors hindering the ability of patients to follow their doctors’ diabetes care recommendations,14,15 conceptualization of patient adherence used in the literature has been ambiguous or inconsistent. In particular, two closely connected but distinct terms—“compliance” and “adherence”—have been used interchangeably. 16 Although scholars have pointed out that they are different concepts,17-21 to our knowledge, no research has empirically tested how adherence differs from and/or is connected to compliance and what the implications of differentiating the 2 concepts are for improving patient adherence. The present study aims to address this gap. We first review the conceptual difference between adherence and compliance as two valuable but separate components in the course of diabetes care. Then, we examine the role of 2 other variables, patient’s potential for mindful non-adherence and physician-patient communication, to identify important factors in understanding the path from compliance to adherence.
Compliance and Adherence
Overall, the terms compliance and adherence have been used interchangeably in the literature, despite their conceptual differences.16,18,22 According to the Oxford English Dictionary, compliance is defined as “the acting in accordance with, or the yielding to a desire, request, condition, direction, etc.” This definition implies an asymmetric power relationship between 2 involved parties, such as the expectation that patients will passively follow orders in a medical context. A conventional definition of compliance—“the extent to which a person’s behavior in terms of taking medications, following diets, or executing lifestyle changes) coincides with medical or health advice” 23 —demonstrates this view, emphasizing an imbalanced relationship between the patient and the doctor. 24 According to Cramer and colleagues, 19 patient compliance is closely related to developing the habit of taking medication in accordance with the physician’s prescription (time, quantity, and frequency). Similarly, compliance has been defined as the extent to which the patient’s behavior matches the prescriber’s recommendations. 25 Given that the term “compliance” implies a passive action, some scholars have associated it with the issues surrounding the dominance of medicine where patients surrender all decision-making and control to health care providers.26,27
Adherence, on the other hand, implies persistence in practice and maintenance of behavior beyond compliance.28,29 Coming from the Latin word adhaerere, which means “to cling to, keep close, or remain constant,” adherence refers not to the accurate following of rules but rather to the extent to which the individual keeps following the previously accepted rules. 17 Adherence is also distinguished from the passive nature of compliance in that adherence decreases when patients do not perceive any benefit from changing their behavior.30,31 Thus, “adherence” has been considered a broader term that incorporates factors affecting a patient’s ability and motivation to follow treatment recommendations. This notion of adherence aligns with the modern vision of healthcare, which assumes that the patient participates in the treatment development process, being a “consumer” of medical services rather than a passive obedient participant. 32
While the concept of compliance has been valuable in understanding the complex problems and decision-making processes involved in diabetes care, 16 an examination of how adherence evolves from compliance will further enhance our understanding. Diabetes self-management is complex and at times can be discouraging. 33 Once it is established that the patient is sufficiently familiar with the recommended treatment plan to perform it correctly, it is equally important to ensure that the patient continues performing the accepted self-care plan for an extended period of time. Thus, the main goal of this study is to examine the factors that can lead from compliance to adherence.
The Role of Patient’s Potential for Mindful Non-Adherence
While adhering to management regimes instructed by a doctor in everyday life is a challenging task by nature, 34 non-adherence has also been viewed as a result of rational decision-making based on patients’ personal beliefs about the medical advice they receive.35-37 Donovan and colleagues 36 were some of the first to note that doctors and patients could have different perspectives on health and illness. According to them, illness is considered normal to doctors, and they have a clear understanding of appropriate treatment. To patients, illness is considered abnormal, and they have a range of alternative beliefs that are rational on their own terms. When their beliefs conflict with the doctors’ view and the conflicts are unresolved, they may stay confused and dissatisfied. 37 Donovan and Blake 36 also argued that patients’ choice to ignore advice or alter prescribed doses of medication could be a reasoned decision because they carefully analyze each treatment option offered and make their own decisions based on those analyses. In this case, the process of following doctor’s recommendations is strategic and “mindful” rather than “mindless.” 36 Other scholars have also conceptualized (non-)adherence as a multifactor phenomenon that can be the result of a mindful decision process based on patients’ personal beliefs. 38 For example, patients do not simply perceive that taking drugs is entirely an action of obeying the doctor’s orders31,39 Instead, they weigh the costs and benefits of taking particular medications as they perceive them within the context of the constraints of their everyday lives and need.36,40 Thus, patients’ increasing desire for autonomy can shape a central component of patient’s potential for mindful non-adherence. 39
Based on the review of the linkage between compliance and adherence, we first hypothesize that, in general, there is a positive relationship between them (H1). Furthermore, as the literature suggests that patients’ mindful autonomous decision-making process can serve as a filter for medical advice, it is reasonable to posit that patients’ increased mindfulness may lead them to choose to ignore some medical recommendations that they initially complied with. Thus, we hypothesize that patient’s potential for mindful non-adherence will mediate the relationship between compliance and adherence (H2).
The Role of Physician-Patient Communication
The next natural question is under what conditions patients are more likely to make their own mindful decisions that will lead them to continue or discontinue following doctors’ medical recommendations. As reviewed in the previous sections, compliance may be achieved even in the traditional physician-patient interaction setting in which the doctor weighs all risks and benefits, makes a decision, and assumes the patient will follow it. Mindful adherence, on the contrary, may not be achieved without a shared decision-making and cooperation communication process. Indeed, increasing patient empowerment—a self-determination of health and treatment-related goals—through effective physician-patient communication has become an important component of modern healthcare.32,41 According to the patient-centered care approach introduced to confront the conventional paternalistic view of physician-patient relationship, 24 patient’s view of illness, life circumstances, unique needs, and perspectives on recovery should be considered before prescribing a treatment.42,43 Similarly, a contemporary mutual participation model of physician-patient relationship emphasizes an equal distribution of power, a shared decision-making, and a mutual cooperation between the 2 parties. 44
Extensive research has shown the effectiveness of these approaches in promoting patient adherence and various positive health outcomes.41,43,45 For example, collaborative, goal-oriented, communication between health professionals and patients was found to enhance patients’ satisfaction, self-efficacy, and commitment.41,46-48 Researchers have also reported that patients who play an active role in the communication process by asking questions and sharing opinions tend to understand the treatment regimen better
49
and are more likely to seek healthcare options.
46
In particular, scholars point out that chronic illness care decisions are more likely to require an active patient role.
50
Thus, perceptions about physician-patient communication can be an important factor in understanding the relationship between compliance and adherence through patient’s potential for mindful non-adherence in diabetes care. The role of patient’s potential for mindful non-adherence in explaining the relationship between compliance and adherence may vary according to how satisfactory and positive the patients perceive their interaction with physicians. Thus, we propose that the effect of patient’s potential for mindful non-adherence in intervening the compliance and adherence relationship will be moderated by the quality of physician-patient communication (H3). By examining these hypotheses, the present study aims to facilitate an understanding of the relationship between 2 important, and often interchangeably used, concepts in diabetes management: compliance and adherence. Figure 1 presents the conceptual model and hypothesized paths tested in this study. Hypothesized model.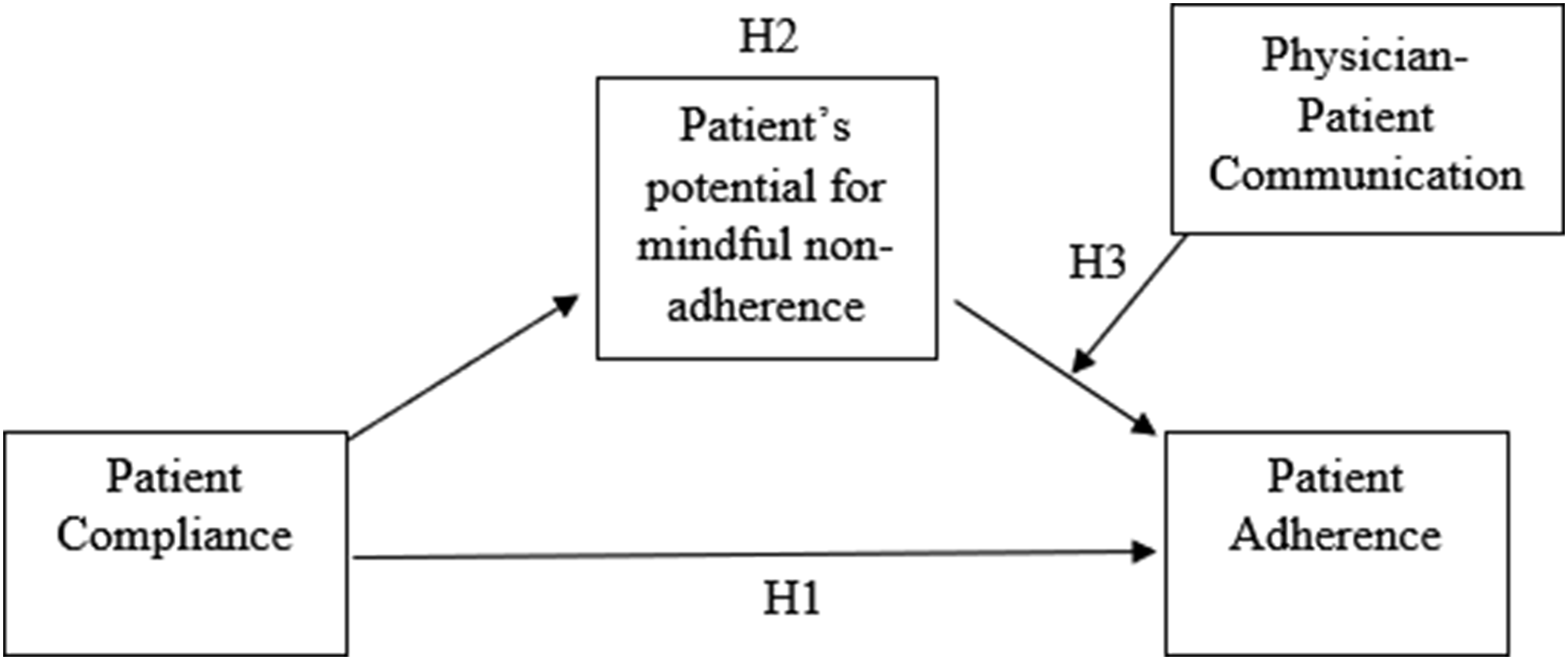
Methods
Design and Sample
We recruited participants through the online data-collection service Mechanical Turk (MTurk). MTurk is a website where participants from across the globe can take surveys and receive compensation for their efforts. MTurk samples are more demographically diverse with respect to race, age, educational attainment, income, and other factors and are inexpensive compared to other non-subject pool options such as survey panels. 51 In this study, MTurk’s geographic qualification function was applied to recruit participants only from the United States. To be eligible for participating in this survey research, a person had to be at least 18 years of age and currently in treatment for diabetes. When recruiting rare populations, however, it is essential to use pre-screening measures (e.g., masking qualification criteria) to prevent fraudulent responses. 52 Thus, we created a short pre-survey with 3 masked questions to determine eligibility. Among the 1852 respondents who participated in the pre-survey, only those who met the eligibility (n = 367) were provided with a link to the main survey hosted on Qualtrics and asked to sign an informed consent. Participants were compensated $.50 for their work. Based on the examination of the quality of responses and outliers in the collected data, those who submitted unfinished questionnaires or unreliable responses, such as unvarying responses across different measurement items including identical responses for reverse-coded items (n = 14), and those who spent less than 3 minutes or over 35 minutes to complete the survey (n = 36) were excluded.
Measures
Compliance
Compliance is operationalized as the extent to which a patient’s behavior (in terms of taking medications, following diets, or executing lifestyle changes) coincides with medical or health recommendation. A 16-item Diabetes Self-Management Questionnaire (DSMQ) developed by Schmitt and colleagues 53 was used to assess recommended self-care activities associated with glycemic control in patients with diabetes. The DSMQ has previously demonstrated efficiency to provide reliable and valid information on diabetes self-management. All items were scored on a four-point scale with anchors 1 applies to me very much) to 4 (does not apply to me). In the present study, the reliability across the items was .84.
Adherence
Adherence is operationalized as persistence in practice and maintenance of diabetes self-care behavior. In this study, 4 items were used to assess patient adherence to recommended treatment. Example items include “I stick to my diabetes treatment schedule even when I don’t feel well” and “I continue with my diabetes treatment even if doing so interferes with my daily activities.” Items were answered on a 5-point scale ranging from 1 (not true at all) to 5 (very true). In the present study, the scale scores had an estimated internal consistency reliability of .79.
Patient’s Potential for Mindful Non-Adherence
Based on the literature that considers non-adherence as a type of mindful decisions led by a patient’s rational analysis of the doctor-recommended diabetes treatment based on the patient’s beliefs,35,36,38 the 4-item “mindful non-adherence” sub-dimension of the Patient Self-Advocacy Scale (PSAS) 35 was used to assess a patient’s mindfulness. The 4 items were specifically developed to measure the potential of a mindful non-adherence in health behaviors, which is a tendency to reject treatments or a willingness to be non-adherent when treatments fail to meet patient expectations. Items were answered on a 5-point Likert scale ranging from 1 (not true at all) to 5 (very true), rating participants’ agreement with statements such as “Sometimes I think I have a better grasp of what I need medically than my doctor does” and “If I am given a treatment by my physician that I don't agree with, I am likely to not take it.” In the present study, the scale scores had an estimated internal consistency reliability of .85.
Physician-Patient Communication
Correlations, Means, and Standard Deviations for Study Variables.

Note. ** P < .01 level, *P < .05 level.
Analysis
We first estimated the measurement model by conducting a confirmatory factor analysis (CFA) to assess the validity of the factor structure of each construct measured in this study. A minimum factor loading of .50 was used as a criterion for including items to be a part of a construction. The measurement model was constructed and analyzed in Mplus v.8. 54 using maximum likelihood estimation. We used the following indices to assess fit: χ2, comparative fit index (CFI) with values of .90 indicating adequate fit and values of .95 indicate good fit; root mean square error of approximation (RMSEA), with values of .05 or lower suggesting good model fit and values between .05 and .08 suggesting reasonable fit; and standardized root mean square residual (SRMR) with values of less than .10 indicating good model fit.
To test hypotheses 1 through 3 (see Figure 1), we used the PROCESS macro developed by Hayes. 55 PROCESS macro facilitates the implementation of bootstrapping methods and allows for probing the significance of conditional indirect effects at different values of the moderator variable. Model 4 in the PROCESS permits testing the indirect effect of an independent variable (compliance with diabetes treatment recommendations in the present study) on a dependent variable (adherence to diabetes treatment recommendations) through a mediator (patient mindful non-adherence). Model 14 in the PROCESS 55 permits testing the conditioned indirect effect of an independent variable (compliance with diabetes treatment recommendations in the present study) on a dependent variable (adherence to diabetes treatment recommendations) through a mediator (patient’s potential for mindful non-adherence) for different levels of a moderator (physician-patient communication). Three variables were controlled for in this study: age, gender, and ethnicity. Hayes’s bootstrapping procedure 55 provides an estimation of both direct effects and conditional indirect effects. PROCESS reports a bootstrap 95%-confidence interval for the indirect effect, which is considered significant if the confidence interval does not include zero. The index of moderated mediation shows whether and to what extent an indirect effect is moderated in a model. 55
Results
Study Sample Demographics.

The result of the CFAs with maximum likelihood estimation showed good overall model fit to the data, (χ2[371] = 777.09, P < .05, CFI = .906, RMSEA = .059, 90% confidence interval [CI] = .053, .065, SRMR = .053), indicating that the hypothesized factor structure was reasonable.
Indirect Effect of Compliance on Adherence through Patient’s Potential for Mindful Non-adherence.

Note. The table reflects values controlled for effects of age, gender, and ethnicity.
Conditioned Indirect Effect of Compliance on Adherence through Mindfulness by Physician-Patient Communication.

Note. Values for the quantitative moderator (physician-patient communication) are the mean and plus/minus one SD from mean. The table reflects values controlled for effects of age, gender, and ethnicity.
Discussion
The present study contributes to the extant diabetes research and practice by examining the role of patient’s potential for mindful non-adherence and quality of physician-patient communication as factors that bridge compliance and adherence. The existing literature uniformly emphasizes the crucial role of adherence to treatment recommendations in the complex and longstanding diabetes management process. However, non-adherence to recommended treatment regimens remains as a major barrier in the management of patients with diabetes, and factors that can lead from an initial compliance to persistent adherence to recommended medication regimen and exercise requirements have been underexamined.
To understand how patients’ with diabetes adherence can evolve from compliance, we first focused on the role of patient’s potential for mindful non-adherence. The results indicate that increased patient’s potential for mindful non-adherence could negatively intervene in the positive relationship between compliance and adherence. Specifically, patients with diabetes who perceived good reasons not to follow the advice of their doctor are less likely to adhere to the recommended diabetes treatment. As reviewed earlier, patient’s potential for mindful non-adherence encompasses a patient’s right to choose whether to follow treatment recommendations, making the patient’s autonomous decision-making a main contributor to adherence or non-adherence.31,35-37 This finding is consistent with the argument that non-adherent health behavior is often strategic and a result of rational decision-making, demonstrating that patient’s potential for mindful non-adherence can serve as a filter for any medical advice patients receive.
To further examine under what conditions patients are more likely to make their mindful decisions to maintain or stop following doctors’ medical recommendations, we focused on the role of physician-patient interaction. Previous research has shown that patients tend to be more satisfied and are more likely to follow the agreed treatment plan when their physician engages in a cooperative communication style.41,43, Consistent with the literature, we found that physician-patient communication played a significant role in the transition from compliance to adherence in patients with diabetes. Patients with diabetes who felt empowered by their doctor and were involved in a collaborative decision-making process about their treatment reported better adherence to recommended self-care behavior. Moreover, their positive perception of physician-patient communication significantly reduced the negative mediating effect of mindfulness on adherence.
These findings together indicate that even though patient’s potential for mindful non-adherence, based on personal beliefs and autonomy level, can reduce adherence to diabetes self-care, patient-centered care with the emphasis on effective physician-patient communication32,42,43 can mitigate this tendency and thus improve adherence. Effective physician-patient communication not only focuses on the well-being of the individual but also accounts for the patient’s experience of the illness and personal beliefs in a shared decision-making process.35,40,49,56,57 Our finding confirms that an established partnership and collaboration between patient and doctor is essential to promoting adherence in patients with diabetes; when the treatment coincides with the patient’s beliefs and needs, mindful non-adherence is less likely to occur.
Given that patients with chronic illnesses are usually involved in complex self-care and need to persistently follow the recommended medication regimen and exercise requirements, many scholars have pointed out that understanding and promoting passive compliance may not be sufficient to improve positive outcomes in managing a chronic diabetes condition.18,26,36 Findings from this study provide empirical support regarding how treatment plan following (compliance) can be promoted into persistent self-care (adherence) by overcoming possible barriers of patient autonomous decision-making through a patient-centered approach to healthcare. While it is important to educate patients on following the recommended treatment, it is also crucial to inform doctors about the importance of understanding and responding to patients’ personal beliefs that might contradict effective treatment. Patient-centered care with an emphasis on proper physician-patient communication can help facilitate this process.
It should be noted that the findings and discussions of this study cannot be isolated from the ongoing discussions about the inconsistent conceptualization and operationalization of compliance and adherence. For example, another concept, concordance, has been used as a synonym for compliance or adherence in the literature.25,58,59 Thus, while the conceptual definitions of variables and their relationships examined in this study were carefully chosen based on the existing literature, we acknowledge that our approach might be only a subset of a larger body of research concerning patient compliance and adherence. Also, a number of different approaches have been used in previous studies to assess patient compliance and adherence, including the use of direct, behavioral measures, such as blood testing. 60 The present study, by contrast, relies on self-reported responses to measure the two concepts. Moreover, in our study, mindful non-adherence and physician-patient communication was measured solely based on the patients’ perspective and was not observed directly. This decision was on the basis of previous research reporting that patient perception was the most reliable measure of patient-centered communication. 61 However, we cannot rule out the possibility that those self-reported measures involve errors in the survey and statistical estimation processes. For instance, some patients might have reported a higher level of compliance than it is due to self-representation bias, while other participants with a low self-advocacy and autonomy level have under-reported their compliance or adherence behavior. In addition, the current study focuses on examining the role of two variables—patient’s potential for mindful non-adherence and physician-patient communication—to shed light on the path from compliance to adherence in relation to diabetes self-care. It should be noted, however, that there are other significant factors that can produce critical conditions that influence the relationship between compliance and adherence. 62 For example, our analyses did not differentiate between Type 1 and Type 2 diabetes while they differ in their clinical characteristics and treatment methods. 5 Relatedly, although we took the influence of age, gender, and ethnicity into account in the analysis, there were only few participants in the age group over the age of 65. This may reflect the known tendency of MTurk recruitment to attract younger population. 63 Moreover, other individual- and social-level factors (e.g., income level, education level, type of health insurance, self-regulation, social support, etc.) may also provide critical conditions that influence patient adherence in diabetes management. Lastly, the findings of the present study should be limited to the particular health behavior and individuals examined in this study. Despite the limitations outlined above, this study provides an important opportunity to update the existing diabetes care literature by distinguishing adherence from compliance and providing empirical evidence about the role of patient’s potential for mindful non-adherence and physician-patient communication for understanding their relationship.
So What? (Implications for Health Promotion Practitioners and Researchers)
What is already known on this topic?
Patients with chronic illnesses are usually involved in complex self-care and need to persistently follow the recommended medication regimen and exercise requirements. While adherence to these recommendations is crucial in leading to positive health outcomes during the prolonged diabetes management process, non-adherence to recommended treatment regimens remains as a major barrier.
What does this article add?
Distinguished from the concept of compliance which implies the passive role of patients, the concept of adherence encompasses elements associated with a patient’s ability and motivation to follow treatment recommendations. However, factors that can lead to adherence from compliance have been underexamined. This study contributes to the literature by examining the role of patient’s potential for mindful non-adherence and physician-patient communication as factors in understanding the compliance-adherence relationship.
What are the implications for health promotion practice or research?
Our findings highlight that patients’ mindful and autonomous decision-making can be a barrier in facilitating the flow from compliance to adherence. Equally importantly, however, an established physician-patient partnership based on collaborative communication process is essential to promoting adherence in patients with diabetes, mitigating the occurrence of mindful non-adherence. These findings can help health researchers and practitioners better understand how to lead active, persistent self-care (adherence) from the passive following of treatment recommendations (compliance).
Footnotes
Acknowledgments
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors. The authors declare that there is no conflict of interest. The study was approved by the Institutional Review Board at the University of Miami. Approval number is 20190622. All participants gave their consent by signing a written consent form.
Author Contributions
KS and ME: conceptualization and design of the study, data collection, data analysis, writing process, content editing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.