
Abstract
Purpose:
The ‘5-2-1-0’ guidelines recommend that children: eat ≥5 servings of fruits/vegetables (‘5’), have ≤2 hours of screen-time (‘2’), have ≥1 hour of activity (‘1’), and drink 0 sugar-sweetened beverages (‘0’) daily. The pediatric emergency department (PED) treats children at risk for obesity and tobacco smoke exposure (TSE). We examined body mass index (BMI), overweight, obesity, TSE, and ‘5-2-1-0’ rates in children with TSE in the PED.
Design:
Cross-sectional study of PED children.
Setting:
The PED of a children’s hospital.
Sample:
Children with TSE >6 months-5 years old (N = 401).
Measures:
Sociodemographics, ‘5-2-1-0’ behaviors, BMI, and cotinine-confirmed TSE.
Analysis:
Associations between ‘5-2-1-0’ and sociodemographics were examined with logistic regression.
Results:
Mean (SD) age = 2.4 (1.6) years; 53.1% were Black; 65.8% had low-income; and 93.4% had TSE. Of 2-5-year-olds, mean (SD) BMI percentile was 66.2 (30.1), 16.1% were overweight and 20.6% were obese. In total, 10.5% attained ‘5’, 72.6% attained ‘2’, 57.8% of 2-5-year-olds attained ‘1’, and 9.8% attained ‘0’. Compared to White children, “other” race children were more likely to meet ‘5’ (aOR(95% CI):4.67(1.41, 5.45)); 2-5-years-olds (aOR(95%CI):0.60(0.38, 0.95)) and Black children (aOR(95%CI):0.36(0.21, 0.60)) were at decreased odds to meet ‘2’ compared to younger or White children, respectively. Compared to younger children, 2-5-year-olds were at decreased odds to meet ‘0’ (aOR(95%CI):0.08(0.02, 0.26)).
Conclusion:
Racially diverse, low-income children with TSE had low ‘5-2-1-0’ attainment. Interventions are needed to improve lifestyle habits in this population.
Keywords
Purpose
Overweight and obesity in children may result in negative health consequences in adulthood. 1,2 Although overweight and obesity rates are highest in children who are: Black, non-Hispanic, Hispanic, low-income, or older, 1,3 -6 13.9% of 2-5-year-olds are obese. 6 Tobacco smoke exposure (TSE) is a modifiable risk factor for overweight and obesity. 7,8 Compared to unexposed children, children with TSE are at increased risk to have higher body mass index (BMI), waist circumference, higher lipid levels, 7 -9 metabolic syndrome, and insulin resistance. 7,10 The pediatric emergency department (PED) and urgent cares (UC) are frequently utilized by low-income children 11 who have TSE, 12,13 high obesity rates, and unhealthy dietary practices. 14,15 Thus, PEDs/UCs may be ideal, yet largely underutilized settings in which to conduct obesity and TSE screening and counseling to at-risk children.
The “Let’s Go! 5-2-1-0” program 16 is an obesity prevention program which recommends that children: eat ≥5 servings of fruits/vegetables (‘5’), have ≤2 hours screen-time (‘2’), have ≥1 hour of activity (‘1’), and drink 0 sugar-sweetened beverages (‘0’) daily to prevent obesity. Multiple settings have used ‘5-2-1-0’ as a screener to assess lifestyle habits of children prior to providing diet and exercise-related interventions. 17 -20 Prior research indicates that children who are racial/ethnic minorities and who have low-income have poor attainment of the ‘5-2-1-0’ recommendations. 21 -25 Although TSE is associated with obesity, 7 -10 ‘5-2-1-0’ attainment has not been evaluated or used as a tool to provide anticipatory guidance to parents of children with TSE. Thus, we sought to assess the rates of overweight, obesity, TSE, and attainment of the ‘5-2-1-0’ recommendations among a racially/ethnically diverse sample of children whose parents smoked and thus were exposed to varying levels of TSE.
Methods
Design
We conducted a randomized controlled trial (“Healthy Families”; www.clinicaltrials.govIdentifier:NCT02531594) 26 designed to promote parental smoking cessation. A convenience sample of child-parent dyads who presented to one of two PEDs or UCs in a large children’s hospital were recruited by clinical research coordinators (CRC). We analyzed cross-sectional data from the PED/UC visit of children in this study.
Sample
Eligible parents of children age >6 months-5 years old in the PED/UC were >18 years old and daily smokers. We chose this age group given the need for diet and exercise interventions targeting younger children. 27,28 IRB-approved informed consent was obtained and dyads were randomly assigned to the “Healthy Habit Control”(HHC)) “Let’s Go! 5-2-1-0” 16 group or the “Screening, Brief Intervention, and Referral to Treatment”(SBIRT) group. HHC parents received counseling tailored to 2 self-reported areas of their child’s ‘5-2-1-0’ attainment that they selected; details are elsewhere. 26
Measures
Parents completed assessments of sociodemographics and their child’s ‘5-2-1-0’ daily behaviors: ‘5’-fruit and vegetables: “How many servings (i.e., the size of your child’s fist) of fruits and vegetables does your child eat on a typical weekday?” Children met ‘5’ if they consumed ≥5 servings of fruits and vegetables. ‘2’-screen-time: “How many hours of non-school-related ‘screen-time’ (e.g., phone, tablet, video games) does your child spend a day on a typical weekday?” Children met ‘2’ if they had ≤2 hours of screen-time. Additionally, parents were asked: “Does your child have his/her own television, tablet, smartphone, iPod, video game console, or computer;” total numbers of devices were summed. ‘1’-physical activity (age >2 years): “How many minutes a day does your child spend in active play (e.g., faster breathing, sweating) on a typical weekday?” Children met ‘1’ if they were active ≥1 hour. ‘0’-sugar-sweetened beverage intake: “How many times a day does your child drink the following (e.g., milk, water, fruit-flavored drink, sports drink) on a typical weekday?” Water and milk products were considered non-sugar-sweetened beverages. Children met ‘0’ if they consumed 0 sugar-sweetened beverages.
Measures of BMI, overweight, and obesity were only assessed on 2-5-year-olds since BMI may not accurately assess adiposity in younger children 29 and overweight/obesity categories are not established for children <2 years old. 30 CRCs abstracted children’s weights from their medical records and measured children’s heights; age- and sex-specific BMI percentiles were calculated based on the Centers for Disease Control and Prevention 2000 growth charts for children age >2. 31 Children with BMI percentiles >95th and 85-94th percentiles were classified as obese and overweight, respectively. 30
We tested child saliva samples for cotinine, a measure of recent TSE, 32 using enzyme-linked immunosorbent assay (ELISA) techniques or liquid chromatography tandem mass spectrometry (LC-MS/MS). Cotinine >1.0 ng/ml was considered equivalent to TSE. 13
Analysis
Descriptive statistics were derived for sociodemographics; attainment of individual ‘5-2-1-0’ recommendations are presented within sociodemographic categories. The associations between sociodemographics and ‘5-2-1-0’ attainment were examined using multivariable logistic regression, adjusting for sex, race, and income. P-values ≤0.05 were considered statistically significant; SAS 9.4 (SAS Institute, Cary, NC) was used.
Results
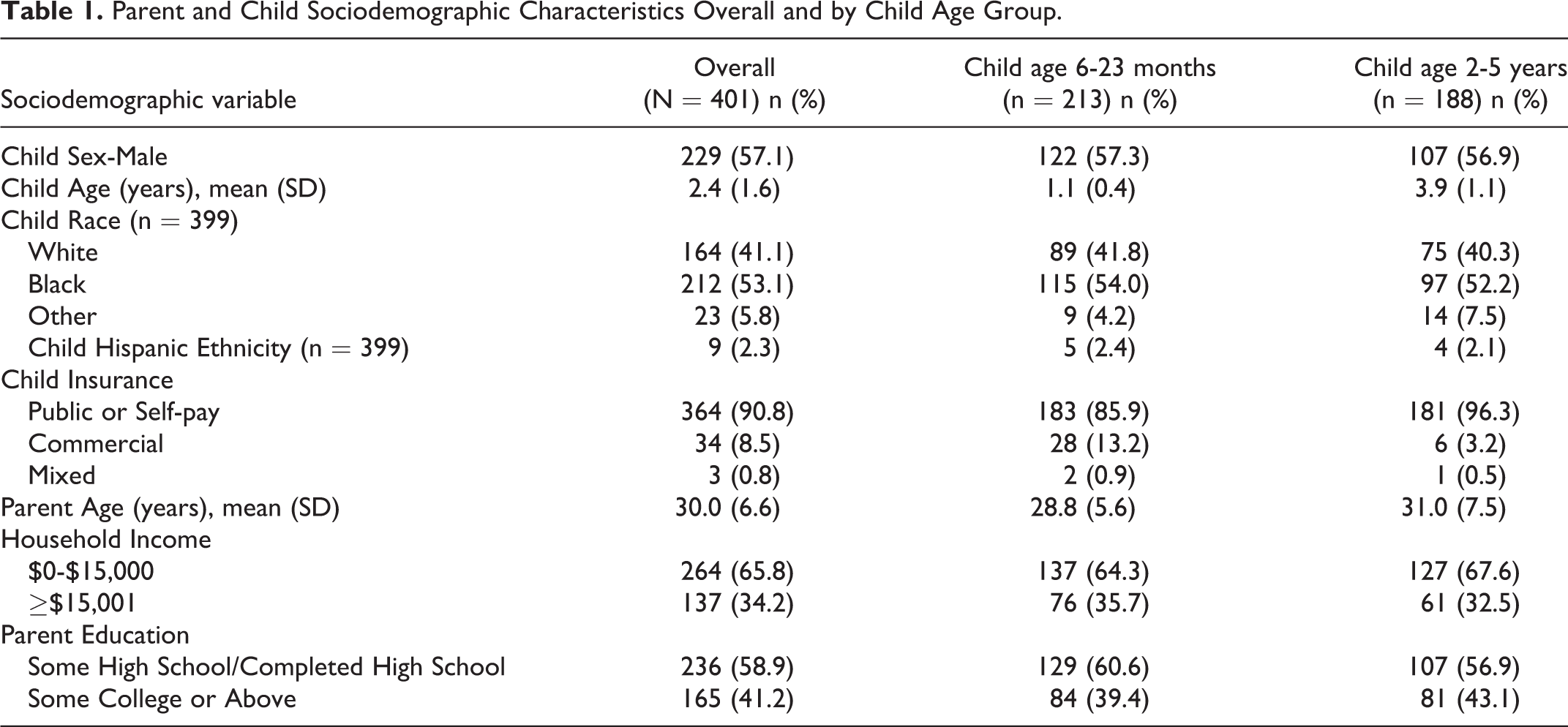
Among the 401 children in this study, mean age (SD) was 2.4 (1.6) years; 53.1% were Black, Non-Hispanic; 90.8% had public insurance/self-pay and 65.8% had an income of <$15,000 (Table 1). The mean (SD) BMI percentile in 2-5-year-olds was 66.2 (30.1); 16.1% were overweight and 20.6% were obese. Based on cotinine levels, 93.4% had TSE. GeoM (95% CI) and median (IQR) of cotinine was 6.65 ng/ml (5.83, 7.58) and 7.33 ng/ml (3.14, 15.09), respectively.
Parent and Child Sociodemographic Characteristics Overall and by Child Age Group.
Overall ‘5-2-1-0’ attainment rates were low. Of 6-23-month-olds, 6 (2.8%) did not attain any of the ‘5-2-0’ (‘1’ was not assessed in <2-year-olds) recommendations; only 1 met all 3. Of 2-5-year-olds, 40 (21.3%) did not attain any of the recommendations and none met all 4 recommendations. A total of 10.5% of children met ‘5’; 72.6% met ‘2’, 57.8% of 2-5-year-olds met ‘1’, and 9.8% met ‘0’ (Table 2). Of note, 153(38.1%) children had >2 personal devices with screens and 200 (50.0%) consumed >4 sugar-sweetened beverages daily.
Attainment of the ‘5-2-1-0’ Recommendations by Sociodemographic Characteristics.

* Physical activity was only assessed in children age 2-5 years.
** Missing values excluded.
Compared to White children, “other” race children were more likely to meet ‘5’ (aOR(95% CI):4.67(1.41, 5.45)); 2-5-years-olds (aOR(95%CI):0.60(0.38, 0.95)) and Black children (aOR(95%CI):0.36(0.21, 0.60)) were at decreased odds to meet ‘2’ compared to children who were younger and White, respectively (Figure 1). Compared to younger children, 2-5-year-olds were at decreased odds to meet ‘0’ (aOR(95%CI): 0.08(0.02, 0.26)).
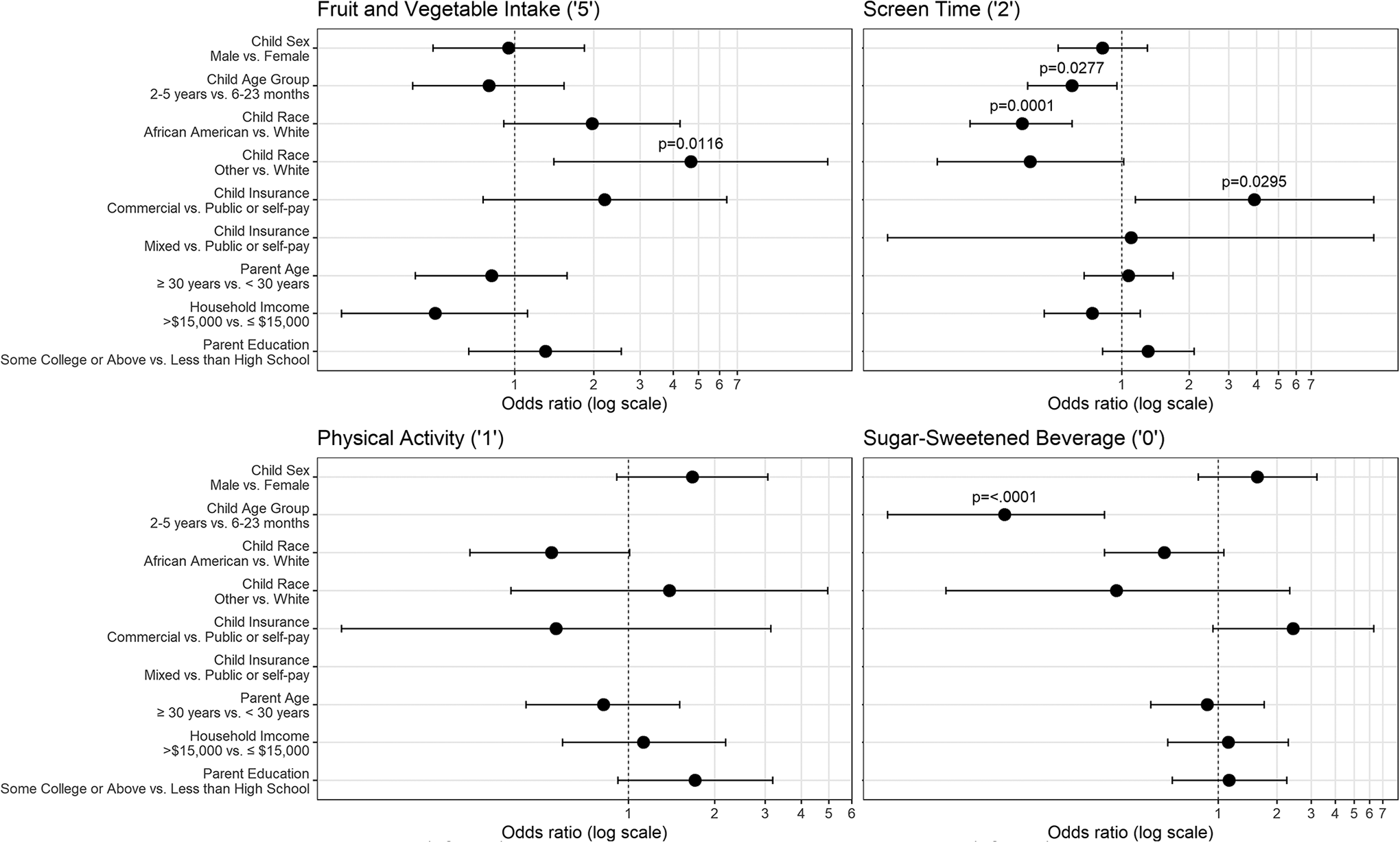
Multivariable logistic regression results of child and parent characteristics based on children meeting ‘5-2-1-0’ recommendations.
Summary
Interventions to prevent childhood obesity that include diet, physical activity, screen-time and beverage recommendations in the ‘5-2-1-0’ program may decrease children’s risk of obesity 28,33 and related morbidities in later life. 1,2 We examined ‘5-2-1-0’ attainment in a racially diverse sample of infants, toddlers and preschoolers. Results indicate that none of the 2-5-year-olds attained all 4 and 21.3% did not attain any of the recommendations. This parallels a study of preschoolers which demonstrated a wide range of ‘5-2-1-0’ attainment (<1% to 81%). 17 In our study, one-in-five 2-5-year-olds were obese which is higher than national prevalence rates of obesity of 13.9% in this age group. 6 Additionally, over 9-in-10 children were exposed to tobacco smoke. Since TSE is an independent risk factor that may be associated with higher risk of obesity in children, this population is also in need of TSE reduction interventions. 7 -9 The overall low rates of 5-2-1-0 attainment in this group of tobacco exposed children reflects the suboptimal diet and physical activity patterns and higher rates of TSE in children who are racial/ethnic minorities and come from low-income homes. 21 -25,34,35
The attainment of ‘5’ was low at 10.5%, which is typical among low-income populations. 21 -23 While we did not find lower ‘5’ attainment levels in children who were Black as in other studies, 23,25 children of “other” races including mixed races had increased odds of attaining this recommendation. These results provide additional evidence that interventions targeted to racially diverse, low-income populations are needed to improve the diets of young children.
It is encouraging that 72.6% attained ‘2’; this parallels other research. 17,36 -38 However, consistent with other research, 39,40 older children had higher odds of not meeting ‘2’. Unlike prior studies, 24,39 we did not find associations with screen-time and income but the majority of our sample had an income <$15,000 which may explain why differences may not have been apparent. Research indicates that increased screen-time is associated with adverse pediatric effects including delayed development, attention problems, cognitive delays, poorer academic performance, and obesity. 41 -45 Interventions to decrease screen-time are warranted.
A total of 57.8% of 2-5-year-old children met ‘1’ which is higher than previously reported rates. 17,46 While this is encouraging, differences may be because parents reported this measure and other studies used concrete physical activity measures (e.g., accelerometers). 17,47 There is room for improvement in this area as when young children engage in regular physical activity, they are more likely to continue to be physically active which may result in decreased obesity in adulthood. 48,49
Only 9.8% of children attained ‘0’ which is lower than prior studies of young children in which up to 56% met ‘0’. 17,50 Although older children were at decreased odds of attaining ‘0’, no other associations were seen in sociodemographic variables. Other research demonstrates high rates of sugar-sweetened beverage intake in low-income and minority children. 51,52 Since consumption of soda and sugar-sweetened beverages is associated with increased obesity rates and continued consumption throughout life, 52 this area is an important target of future interventions.
Collectively, our ‘5-2-1-0’ findings suggest that the PED/UC population of low-income infants, toddlers and preschoolers need interventions to improve these lifestyle habits. These interventions should not be limited to certain subpopulations as we did not find many sociodemographic characteristics that were associated with attainment of these recommendations. Due to time constraints in the PED/UC setting, parents were briefly counseled on two ‘5-2-1-0’ areas they self-selected. A similar approach might be adopted in future research.
Limitations
Limitations include our evaluation of a largely low-income sample of children of smokers who presented to one children’s hospital, thus it is unknown if the same results would be obtained in children without TSE or with different sociodemographic characteristics. Since parent-reported data was used, parental recall and reporting biases may have over- or underestimated ‘5-2-1-0’ behaviors. Nevertheless, our results provide information on child subgroups and lifestyle topic areas to target in the future interventions.
Significance
This study indicates that young, low-income children with TSE who visit PED/UC settings are in need of obesity reduction interventions. The lowest levels of ‘5-2-1-0’ attainment were in the areas of fruit and vegetables and sugar-sweetened beverage consumption. Since lack of consumption of a diet rich in fruits and vegetables and excess consumption of sugar-sweetened beverages may lead to preventable obesity-related morbidity, 53,54 interventions in this age group are needed to encourage healthy diets prior to school entry. Although screen-time and physical activity levels in our sample were closer to the recommendations, improvements in these areas may result in lower obesity rates and potential improvements in cognitive functioning and academics. 44,48 Finally, the adverse effects of TSE are well-understood and include the associations of TSE and obesity. 8,9 Thus, efforts are needed to reduce TSE and improve early lifestyle behaviors in the emergency and other settings that care for low-income children. Since diet and exercise habits established in the early, formative years may result in healthy lifetime practices and prevent future obesity-related morbidity, 2,28 PED/UC interventions may have lasting health benefits.
So What?
What is already known on this topic?
Childhood obesity results in negative health consequences in adulthood. The pediatric emergency department (PED) treats children at risk for obesity and tobacco smoke exposure (TSE), another risk factor for obesity. The ‘5-2-1-0’ program contains recommendations on physical activity, screen-time, and beverage intake. Prior research indicates that few, if any, children who are racial/ethnic minorities and who have low-income attain all 4 of the ‘5-2-1-0’ recommendations and this group also has suboptimal attainment of the individual components. The ‘5-2-1-0’ screener has not been evaluated in children with TSE being treated in the PED.
What does this article add?
We examined a racially diverse, low-income sample of children with TSE age >6 months-5 years of age being treated in the PED and observed high rates of obesity, varying levels of TSE, and low ‘5-2-1-0’ attainment rates.
What are the implications for health promotion practice or research?
Diet and exercise habits established in the early, formative years may result in healthy lifetime practices and prevent future obesity-related morbidity. Thus, PED interventions may have lasting health benefits in this population.
Footnotes
Authors’ Note
Author Contributions
Dr. Mahabee-Gittens conceptualized and designed the study and drafted the initial manuscript. Dr. Ding and Dr. Khoury conducted the statistical analyses and interpreted the results. Dr. Merianos and Dr. Gordon provided content expertise and edited revisions of the manuscript. All authors approved the final manuscript as submitted.
Data Sharing Agreement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Ethics Approval
The conduct of this study was approved by the Institutional Review Board at Cincinnati Children’s Hospital Medical Center.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funded by the Eunice Kennedy Shriver National Institute of Child Health and Human Development at the National Institutes of Health: R01HD083354 and the National Institute on Drug Abuse: K01DA044313. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.