
Abstract
Purpose
Information on incentives for COVID-19 testing is needed to understand effective practices that encourage testing uptake. We describe characteristics of those who received an incentive after performing a rapid antigen test.
Design
Cross-sectional descriptive analysis of survey data.
Setting
During April 29–May 9, 2021, COVID-19 rapid antigen testing was offered in 2 Maryland cities.
Sample
Convenience sample of 553 adults (≥18 years) who tested and received an incentive; 93% consented to survey.
Measures
Survey questions assessed reasons for testing, testing history, barriers, and demographics.
Analysis
Robust Poisson regressions were used to determine characteristic differences based on testing history and between participants who would re-test in the future without an incentive vs participants who would not.
Results
The most common reasons for testing were the desire to be tested (n = 280; 54%) and convenience of location (n = 146; 28%). Those motivated by an incentive to test (n = 110; 21%) were 5.83 times as likely to state they would not test again without an incentive, compared to those with other reasons for testing (95% CI: 2.67-12.72, P < .001).
Critical Limitations
No comparative study group.
Conclusion
Results indicate internal motivation and convenience were prominent factors supporting testing uptake. Incentives may increase community testing participation, particularly among people who have never tested. Keywords COVID-19, pandemic, incentives, health behavior, community testing.
Purpose
From January to April 2021, coronavirus disease 2019 (COVID-19) testing rates sharply declined across the U.S. 1 It is unclear whether demand decreased due to barriers, increased vaccinations, or perception that testing was unneeded. Inadequate testing can hinder COVID-19 prevention and mitigation within communities. 2
Previous studies suggest that economic incentives may increase participation in health initiatives ranging from enrollment in wellness programs to improve diet and increase weight loss, to improving influenza vaccination coverage among children, breast cancer screenings, tuberculosis (TB) testing, and sexually transmitted infections (STI) screenings. 3 Incentives have been utilized to increase COVID-19 testing, but results have not been formally analyzed. 3 Little is known about motivating factors for COVID-19 testing and the impact convenience or incentives have on willingness to test.
During April 29–May 9, 2021, the U.S. Centers for Disease Control and Prevention (CDC) partnered with Maryland Department of Health (MDH), CDC Foundation, and U.S. Department of Health and Human Services Increasing Community Access to Testing Team to create free walk-up testing sites and offer incentives to understand the effects of convenience factors and incentives on testing participation.
Methods
Design
MDH used CDC’s Social Vulnerability Index 1 based on population vulnerability and percent positivity to identify areas in greater need of COVID-19 support. Testing was available in Hagerstown and Salisbury, Maryland at frontside parking lots of 2 commercial supercenters. Event promotion occurred on site and county-wide via flyers and social media.
BinaxNOW Ag CARD rapid antigen testing was offered to adult and pediatric populations over 2 4 day periods (Thursday – Sunday) spanning April 29 – May 9, 2021. Positive results were offered confirmatory testing via reverse transcription polymerase chain reaction (RT-PCR). Participants who completed rapid antigen testing were offered a $10 Visa gift card or a pair of cloth face masks of equal value. This activity was reviewed by CDC and conducted consistent with applicable Federal law and CDC policy 2 .
Sample
Participants aged ≥18 years were eligible for a voluntary survey (Supplement 1). Survey participation was not a prerequisite for testing nor receipt of the incentive. Surveys were distributed after testing via QR code for mobile and paper (paper surveys were manually entered into database at the end of data collection day). Anonymized individual-level responses were collected using REDCap. 4 Of the 634 participants, 553 (87%) were eligible for survey participation. Five hundred and fifteen (93%) individuals consented to the survey.
Measures
We investigated: (1) reasons for getting tested; (2) willingness to retest without an incentive; (3) differences in characteristics of those previously tested vs never tested.
Analysis
Using Robust Poisson regression modeling, prevalence ratios were estimated for stated intention to re-test (with an incentive vs without) and testing history (previously tested vs never tested). Control variables included race/ethnicity (non-Hispanic White, non-Hispanic Black or African American, non-Hispanic other, or Hispanic), age (18-34; 35-54; or 55 and older), gender (male or female) 3 , employment (working vs not working 4 ), distance to testing site (≤5 miles vs ≥5 miles), and location. We used P < .05 to determine statistical significance. Calculations were performed in R (R Core Team, version 4.0.3, 2020) with gee package. 5
Results
Testing
Over 8 days, 634 individuals were tested; 265 (42%) in Hagerstown and 369 (58%) in Salisbury. Eleven (2%) individuals tested positive for COVID-19, 1% in Hagerstown and 2% in Salisbury. Both cities averaged 5% positivity during this period. 6
Characteristics of survey participants during April 29–May 9, 2021 (n=515).
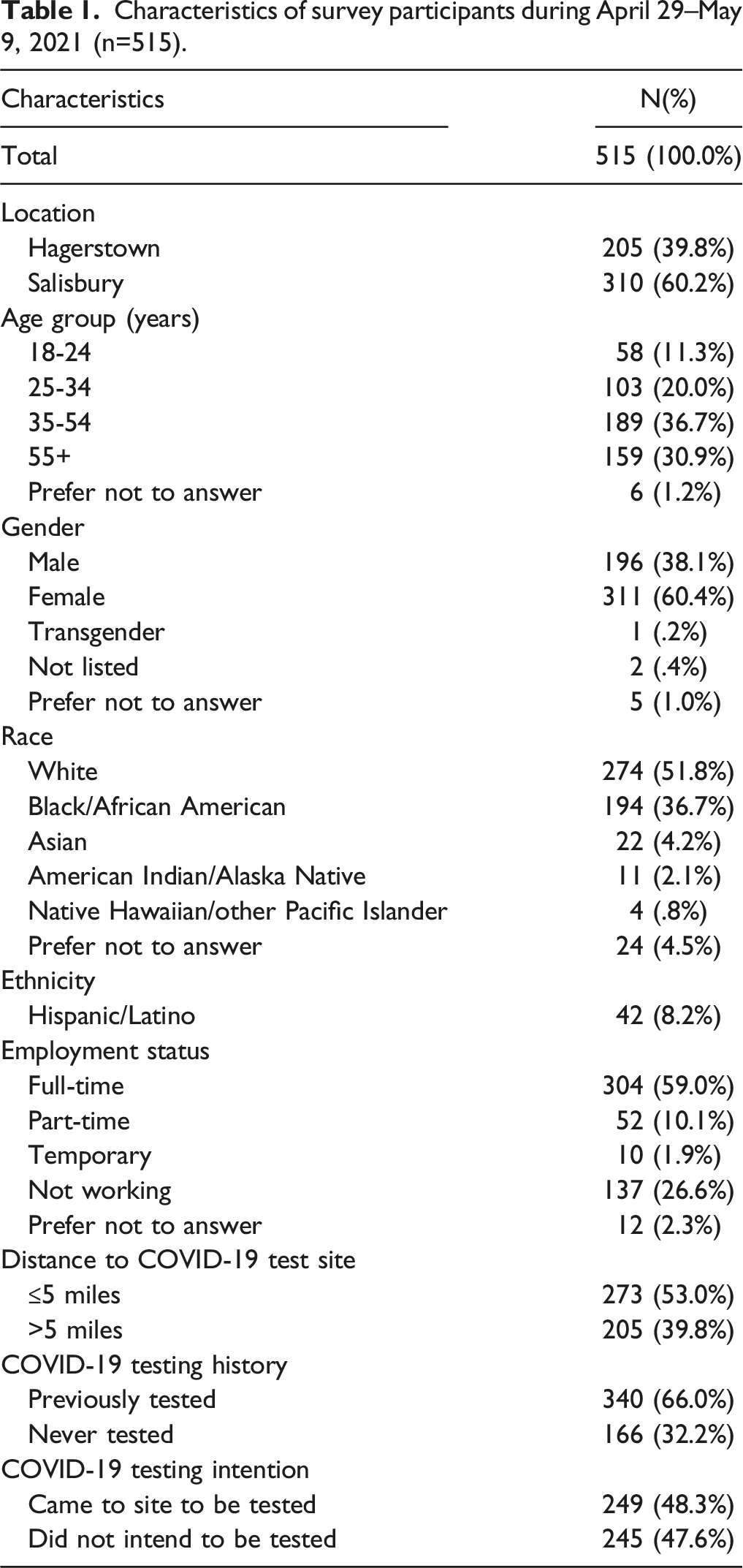
Convenience Factors Impacting Testing: The most common factor for testing was the need or want to be tested (54%), followed by convenience of testing location (28%), and time of operation (22%). Factors were not statistically different across age, race, ethnicity, or gender. The third most common reason for not getting tested was being unaware of testing locations (4%). Being asymptomatic (17%) or not having been exposed to a known infected persons (9%) were the 2 most common reasons for not getting tested.
Adjusted prevalence ratios (PR) of survey participants who would not get tested in the future without an incentive vs those who would re-test without an incentive (n=475 a ).
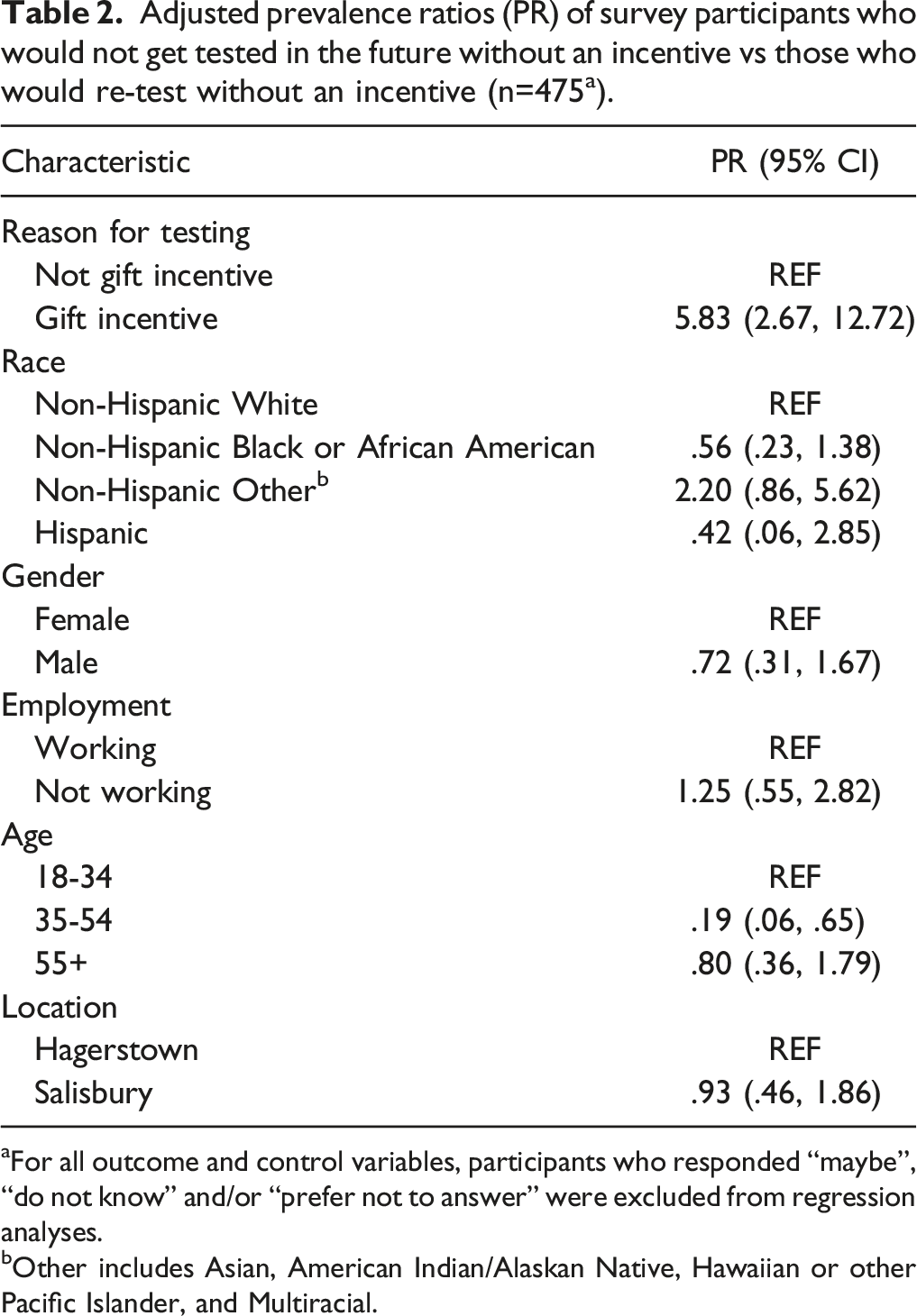
aFor all outcome and control variables, participants who responded “maybe”, “do not know” and/or “prefer not to answer” were excluded from regression analyses.
bOther includes Asian, American Indian/Alaskan Native, Hawaiian or other Pacific Islander, and Multiracial.
Differences Between Previously and Never Tested Populations: Those never tested for COVID-19 identified less as non-Hispanic Black or African American vs non-Hispanic White (Prevalence Ratio .55, 95% CI: .39-.77, P < .001), more as male vs female (PR 1.65, 95% CI: 1.29-2.13, P < .001), and currently unemployed vs working (PR 1.71, 95% CI: 1.29-2.27, P < .001). Those living within 5 miles of testing site were more likely to never have tested compared to those who lived farther away (PR 1.45, 95% CI: 1.11-1.89, P = .006).
Discussion
Summary
These findings support convenience and incentives for promoting health behaviors. Increasing accessibility of testing has shown to positively impact testing behaviors. 7 Testing in community locations can increase convenience, therefore increasing participation, especially in underserved or untested populations. 8
Participants who stated the incentive as a reason for getting tested (21%) combined with the high probability they would not test again without an incentive (PR 5.83, 95% CI: 2.67-12.72), support findings from previous studies examining the effect of incentives on uptake of health behaviors. 9
Limitations
These findings are subject to limitations. Survey participants were a convenience sample and participants may have tested or surveyed multiple times. Second, there is no comparative group. Last, race and age categories were collapsed which limited ability to thoroughly examine factors’ impact on outcome; findings may not be applicable to those who do not identify as non-Hispanic White or Black/African American.
Significance
Incentives serve as 1 strategy to achieve public health priorities, like COVID-19 testing. Commercial organization partnerships within communities can improve intervention accessibility. Public-private partnerships can increase the efficacy of community-based testing initiatives due to established trust and pre-existing relationships between community members and partners. 10 Our intervention paired an incentive with increased access to free testing services by targeting a frequented location offering varied operating times (weekday/weekend availability; walk-up and pre-registered appointments). The convenient location of the testing appeared successful in targeting untested populations within the nearby community. Furthermore, nearly one-third of respondents (28%) stated convenient location as a reason for testing participation. Community members wanted to be tested, and site convenience provided the opportunity.
These results support incentives and a convenient location may increase participation, especially among members who have never tested for COVID-19. Furthermore, in partnering with state health departments utilizing SVI, this testing design could lend to more equitable testing practices in areas in need of greater COVID-19 support. These findings highlight the need to investigate and understand motivations for testing to increase rates among individuals at-risk of COVID-19 transmission. Incentives and accessibility are effective in promoting health behaviors, including testing uptake. Evidence supporting accessible testing sites and use of incentives for increasing COVID-19 testing in underserved areas. Communities seeking to increase COVID-19 testing may want to broaden testing availability in community settings and consider offering incentives to encourage testing behavior.So What?
1 What is already known on this topic?
2 What does this article add?
3 What are the implications for health promotion practice?
Footnotes
Author Contributions
The following authors from the manuscript titled The Impact of Community-Based Testing Sites and Gift Incentives on COVID-19 Testing Uptake in Maryland, April 29 – May 9, 2021, have been included due to their involvement according to the ICMJE guidelines. Significant contributions to Conception, Design, and Analysis of Work Caitlin Turbyfill, MPH Isabel Thomas, MPH Namita Agravat, MPH Joanna M. Prasher, PhD, MPH Randall J. Nett, MD, MPH Melody Stevens, MA Jessica N. Ricaldi, MD, PhD Tambra M. Dunams, PhD Cuc H. Tran, PhD, MPH Charles Rose, PhD, MS Rieza Soelaeman, PhD, MPH
Significant Contributions to Acquisition of Data Latasha Brickhouse-Frazier, MPH Yonathan Gebru, MPH Ashley King, MPH Chigo Oguh, PharmD Amanda Pullman, MPH Kaylin Roman, MS Robert Scherr, BA Turquoise Sidibe, MPH Jonathan Weinstein, MA Todd Wilson, MS Melissa D. Carter, PhD, MBA Coral S. May, MS, RN Joseph D. Miller, PhD All co-authors listed above provided substantial contributions to this work from conception to finalization. Those that lead the drafting of the manuscript are the following: Turbyfill, Thomas, Prasher, Nett, Stevens, Ricaldi, Dunams, Tran, and Agravat. The rest of the coauthors listed critically revised the document for important intellectual content and provided final approval for this version to be published. All coauthors agreed to be accountable for all aspects of this work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.