
Abstract
Purpose
Drawing from the Health Belief Model, we explored how disadvantaged groups in the U.S., including Black, Hispanic, less educated and wealthy individuals, experienced perceived barriers and cues to action in the context of the COVID-19 vaccination.
Design
A cross-sectional survey administered in March 2021.
Setting
USA
Subjects
A national sample of U.S. residents (n = 795) recruited from Prolific.
Measures
Perceived barriers (clinical, access, trust, religion/spiritual), cues to action (authorities, social circles), attitudes toward COVID-19 vaccination.
Analysis
Factor analysis and Structural Equation Model (SEM) were performed in STATA 16.
Results
Black and less educated individuals experienced higher clinical barriers (CI [.012, .33]; CI [.027, .10]), trust barriers (CI [.49, .92]; CI [.057, .16]), and religious/spiritual barriers (CI [.28, .66]; CI [.026, .11]). Hispanics experienced lower levels of clinical barriers (CI [-.42, .0001]). Clinical, trust, and religious/spiritual barriers were negatively related to attitudes toward vaccination (CI [-.45, −.15]; CI [-.79, −.51]; CI [-.43, −.13]). Black and less educated individuals experienced fewer cues to action by authority (CI [-.47, −.083]; CI [-.093, −.002]) and social ties (CI [-.75, −.33]; CI [-.18, −.080]). Lower-income individuals experienced fewer cues to action by social ties (CI [-.097, −.032]). Cues from social ties were positively associated with vaccination attitudes (CI [.065, .26]).
Conclusion
Communication should be personalized to address perceived barriers disadvantaged groups differentially experience and use sources who exert influences on these groups.
Keywords
Introduction and Purpose
The COVID-19 pandemic brought catastrophic global human, economic, and social consequences. Vaccines remain one of the best ways to defeat COVID-19. However, to be successful, hundreds of millions of Americans should fully be vaccinated. 1 The U.S. still lags in this regard and leads the world in vaccine opposition and hesitancy. 2 For example, as of January 2022, COVID-19 cases and hospitalizations were the highest. Only around 64% are fully vaccinated, and only around half of those eligible have received a booster dose. 3 In addition, data show disparities in the vaccination rates in traditionally disadvantaged populations - across racial and ethnic minority groups (predominantly Black and Hispanic 4 ) and lower education and income groups.5,6 In this study, we defined socially disadvantaged groups as Black, Hispanic, and people of lower education and lower household income.
Effects continue to be felt disproportionally. 7 It is thus critical to identify the factors associated with attitudes toward COVID-19 vaccines for these most affected and disadvantaged groups. Vaccine refusal and hesitancy especially among the disadvantaged groups, were related to distrust (in the vaccine, vaccine developers, government, etc.), mis/dis-information (primarily about the vaccine’s side effects), and political differences.2,8 Consequently, we need to better understand how to change vaccine attitudes racial/ethnic minority and lower socioeconomic status groups hold.
Literature Review
The present study draws from the Health Belief Model (HBM) to address this critical issue. HBM is one of the widely adopted and tested frameworks for explaining and predicting attitudes toward health choices and designing health interventions.9,10 The model’s fundamental variables are perceptions of severity, susceptibility, barriers, benefits, self-efficacy, and cues to action. 11 HBM is widely used in the vaccination context, including COVID-19.8,12,13 In this context, the model focuses on perceived severity and susceptibility of the disease the vaccine would prevent, perceived benefits and barriers of the vaccine, cues to action, and self-efficacy for accepting/refusing the vaccine.
Barriers and Cues to Action
Perceived barriers are among the most powerful predictors of health behaviors. 14 While studies on HBM tend to treat barriers as a single variable, this conceptual approach may miss important facets social groups uniquely experience. Recent studies have shown the impact of different obstacles to COVID-19 vaccination, such as access, perceived clinical elements, trust, and a lack of information for decision-making.9,13 Further, not all barriers may be equally influential or relevant to attitudes toward the COVID-19 vaccine, with access and trust as salient barriers to vaccination for disadvantaged groups. 15 Our study fills this gap by examining potential dimensions of perceived barriers to COVID-19 vaccination with a focus on disadvantaged groups (ethnic/racial minorities, low income, low education). Specifically, based on existing literature, we propose four dimensions of perceived barriers: perceived clinical barriers; 12 perceived access barriers; 12 trust barriers (newly developed); and religious/spiritual barriers (newly developed).
Cues to action, another significant HBM predictor of health behaviors, refers to health messaging from different sources, including authority sources
12
and personally connected sources.
16
Despite its theoretical importance, this construct has been understudied relative to other HBM factors,
17
particularly as connected to disadvantaged groups’ experiences. It is plausible that they respond to messages from different sets of actors. Based on existing literature,12,16 we differentiate cues to action into authority/officials (eg, health departments, mayors, the President of the U.S., governor, CDC) and social ties (eg, employer/boss, spiritual advisor, doctor/nurse, family members, friends, colleagues) dimensions. We thus posit the following research questions and hypotheses:
Methods
Data Collection
Demographics of Participants.

Measures
All questions included in the survey were randomized to minimize order effects.
Disadvantaged groups
In this study, we defined socially disadvantaged groups as Blacks, Hispanics, and people of lower education and lower household income. Blacks and Hispanics were coded as dummy variables. Education was measured on an eight-point scale (1 = less than high school, 8 = Doctorate or equivalent) and then reversed coded so that larger values indicated lower education. Household income was measured on a ten-point scale (1 = under $10,000, 10 = $200,000 or more) and then reversed coded.
Severity of COVID-19
Four items by Coe et al 12 were used to measure perceived severity of COVID-19 (eg, “If I get COVID-19, I will get sick.” 1 = strongly disagree to 5 = strongly agree). The average of the four items was 3.33 (SD = .84, α = .70).
Susceptibility of COVID-19
Four items, adapted from Coe et al. 12 and Myers and Goodwin 18 were used to measure perceived susceptibility of COVID-19 (eg, “I am at risk for getting COVID-19.” 1 = strongly disagree to 5 = strongly agree). The average of the four items was 3.40 (SD = 1.01, α = .84).
Self-efficacy
Two items adapted from Guidry et al. 9 were used to measure self-efficacy of getting COVID-19 vaccines (“For me to have the COVID-19 vaccine would be...” 1= very difficult, 5 = very easy). The average was 3.34 (SD = 1.12, Pearson’s correlation = .50).
Attitudes toward the COVID-19 Vaccine
Barriers and Cue to Actions Scales and Corresponding Items with Descriptive Statistics, N = 741.
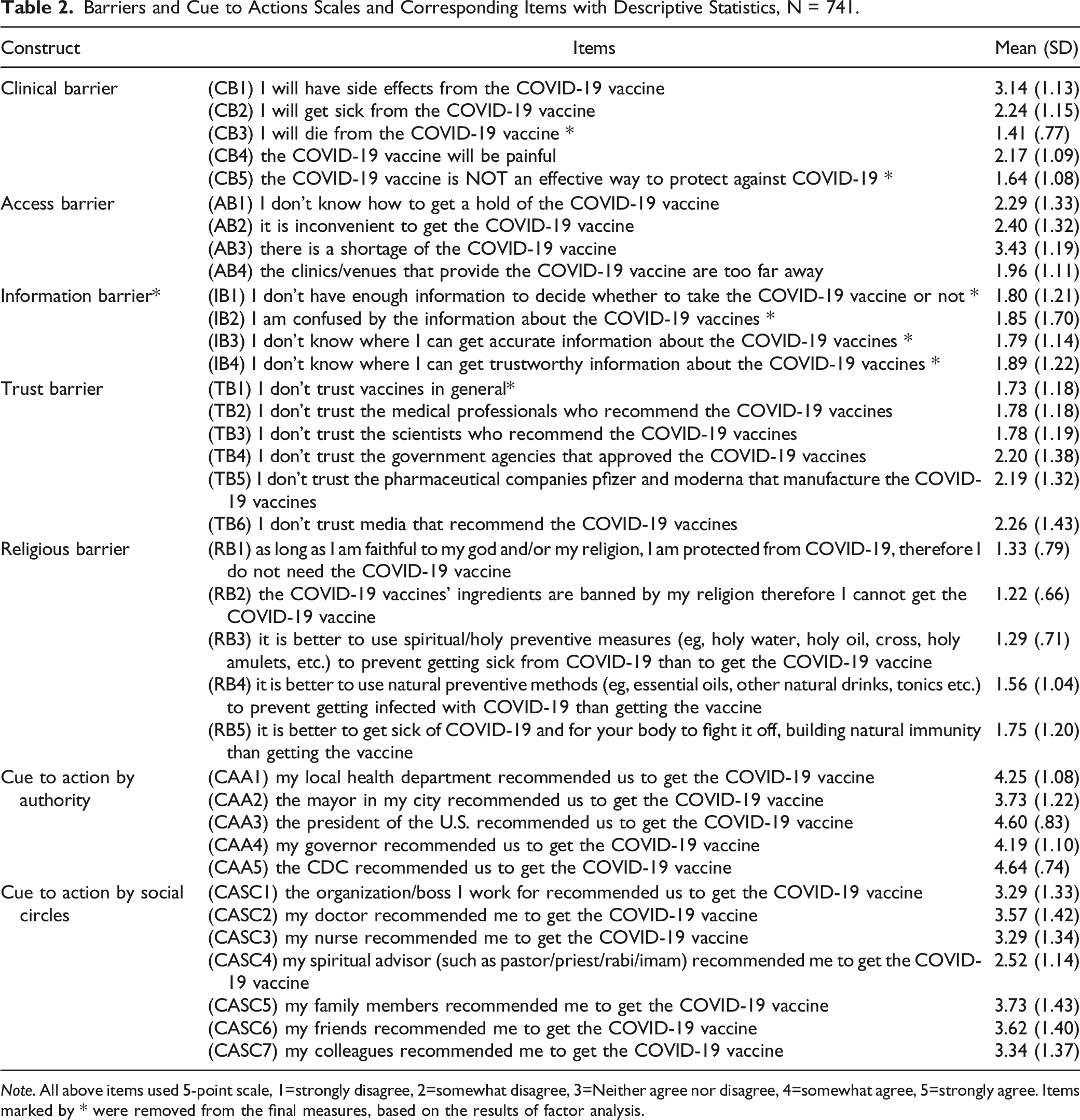
Note. All above items used 5-point scale, 1=strongly disagree, 2=somewhat disagree, 3=Neither agree nor disagree, 4=somewhat agree, 5=strongly agree. Items marked by * were removed from the final measures, based on the results of factor analysis.
Scale Development for Barrier and Cues to Action
We developed a scale of barriers based on existing literature on barriers to getting vaccines.9,12,19,20 The first dimension of the scale was related to clinical barriers leading to vaccine hesitancy. 12 Five items were developed (eg, “I will get sick from the COVID-19 vaccine”). Access barriers, the second dimension, refers to the perceived access people have to the COVID19 vaccine.12,21 Four items were developed (eg, “There is a shortage of the COVID-19 vaccine”). Another dimension was information barriers 22 – degrees of access to accurate and trustworthy information about the COVID-19 vaccines (eg, “I don’t know where I can get accurate information about the COVID-19 vaccines”). This dimension was later removed from the scale as factor analysis results indicated it overlapped with the trust barrier. The third dimension was trust barriers23,24 – how much people trust COVID-19 vaccines and vaccine-connected organizations (eg, “I don’t trust the government agencies that approved the COVID-19 vaccines”). The last dimension measured religious barriers9,23,25,26 – the extent to which religious/spiritual beliefs serve as barriers (eg, “As long as I am faithful to my God and/or my religion, I am protected from COVID-19, therefore I do not need the COVID-19 vaccine”).
A cue-to-action scale was developed based on research that emphasizes cues to action by authorities 12 and social circles. 16 Five items were developed for cues to action by authority (eg, “The President of the U.S. recommended us to get the COVID-19 vaccine”) and six by social circles (eg, “My family members recommended me to get the COVID-19 vaccine”).
Statistical Analysis Plan
We performed factor analysis to confirm the scales of barriers and cues to action. We first split the data (N = 741) into two separate samples (n1= 371 and n2 = 370) as a cross-validation strategy. 27 Then we conducted exploratory factor analysis (EFA) using the first sample. Maximum likelihood factoring with an Oblimin rotation was used to examine item loadings. Based on the EFA results, we performed confirmatory factor analysis (CFA) on the second sample. We inspected modification indices and correlated errors for item correlations when a model fit was not satisfactory for the measurement model. We then estimated a structural equation model (SEM) to test the hypotheses and research questions. Both factor analysis and SEM were performed in STATA 16.
Results
Factor Analysis
We started with EFA with the first sample (n1= 371). For the barrier scale, eigenvalues and the scree-plot indicated the retention of four factors, which is different from the original proposal of five factors. Upon reviewing the item loadings, we found that the four items used to represent information barriers cross-loaded on the trust barrier factor. Underlying trust issues may have caused a perceived lack of vaccine information and trustworthy information. 28 Based on the statistical results and existing literature, we thus decided to remove the information barrier items (see Supplemental Table 1).
CFA Factor Loadings of the Four-Factor Barrier Scale, n 2 = 370.
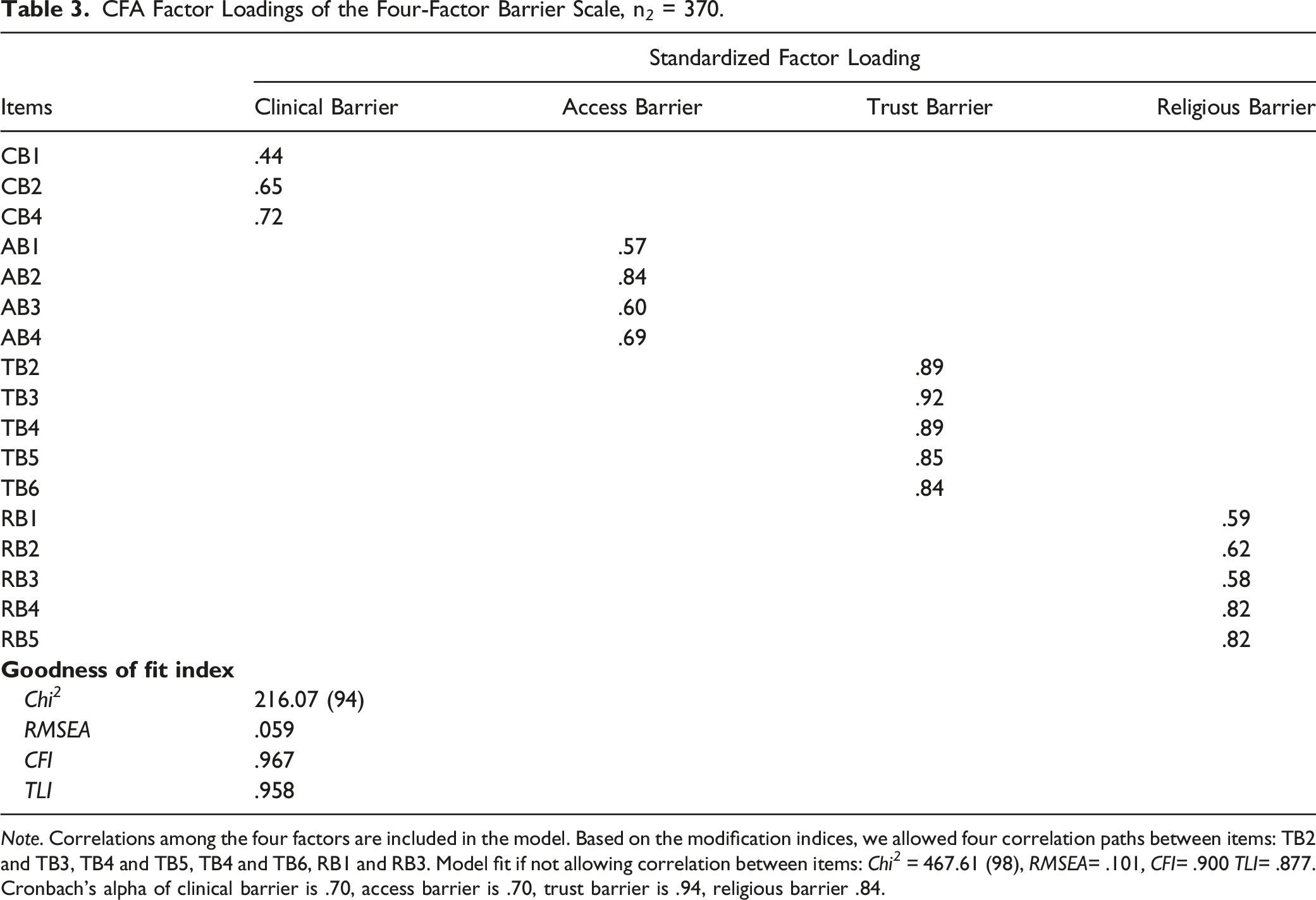
Note. Correlations among the four factors are included in the model. Based on the modification indices, we allowed four correlation paths between items: TB2 and TB3, TB4 and TB5, TB4 and TB6, RB1 and RB3. Model fit if not allowing correlation between items: Chi 2 = 467.61 (98), RMSEA= .101, CFI= .900 TLI= .877.
Cronbach’s alpha of clinical barrier is .70, access barrier is .70, trust barrier is .94, religious barrier .84.
CFA Factor Loadings of the Two-Factor Cue to Action Scale, n 2 = 370.
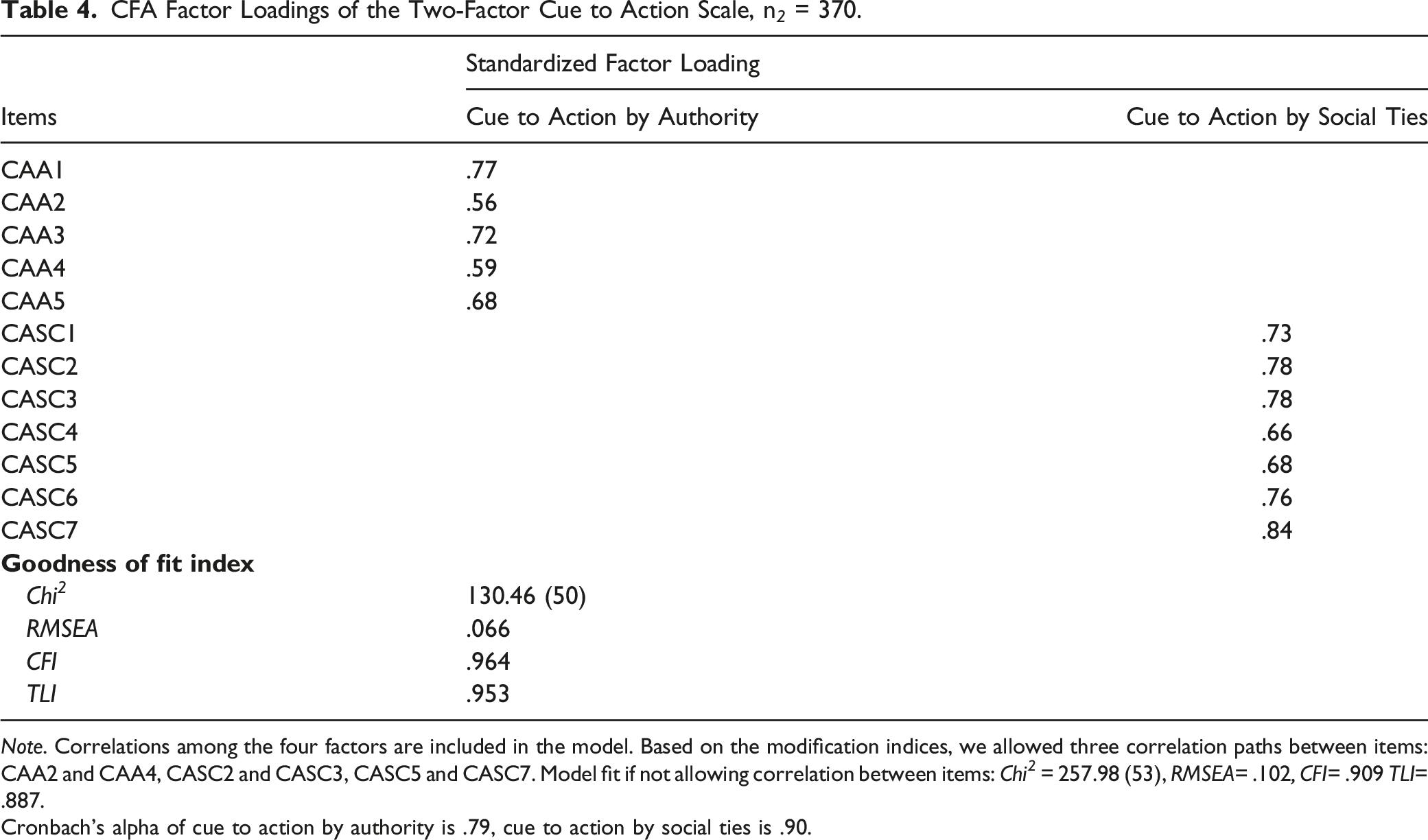
Note. Correlations among the four factors are included in the model. Based on the modification indices, we allowed three correlation paths between items: CAA2 and CAA4, CASC2 and CASC3, CASC5 and CASC7. Model fit if not allowing correlation between items: Chi 2 = 257.98 (53), RMSEA= .102, CFI= .909 TLI= .887.
Cronbach’s alpha of cue to action by authority is .79, cue to action by social ties is .90.
SEM Results
Unstandardized (B) and standardized (β) effects of variables in the full structural model.

Note. N = 741, with 8 missing data. * means statistically significant predictors: ***P < .001. **P < .01. *P < .05.
Regarding RQ1, results showed that Blacks and participants of lower education experienced a higher level of clinical barriers than other participants (B = .17, P < .05, CI [.012, .33] and B = .066, P < .001, CI [.027, .10], respectively). Hispanics, however, reported a lower level of clinical barriers (B= −.21, P = .05, CI [-.42, .0001]). Being Black or Hispanic and education and income were not related to access barriers. In terms of trust barriers, Blacks and people of lower education had a higher level of trust barriers (B = .70, P < .001, CI [.49, .92] and B = .11,P < .001, CI [.057, .16], respectively). For religious and spiritual barriers, Blacks and people of lower education had a higher level of religious barriers (B = .47, P < .001, CI [.28, .66] and B = .070, P < .01, CI [.026, .11], respectively).
Concerning RQ2, results showed that Blacks and people of lower education reported a lower level of cues to action by authority (B = −.28, P < .01, CI [-.47, −.083] and B =-.048, P < .05, CI [-.093, −.002], respectively). Blacks, people of lower education, and people of lower income reported a lower level of cues to action by social ties (B = −.54, P < .001, CI [-.75, −.33], B = −.13, P < .001, CI [-.18, −.080], and B = −.065, P < .001, CI [-.097, −.032], respectively).
H1 was partially supported. Results showed that clinical barriers, trust barriers, and religious/spiritual barriers were negatively associated with attitudes toward COVID-19 vaccines (B = −.29, P < .001, CI [.45, −.15], B = −.65, P < .001, CI [-.79, −.51], and B = −.28, P < .001, CI [-.43, −.13], respectively). However, access barriers did not have any significant association with attitudes toward COVID-19 vaccines. H2 was also only partially supported. Results showed that only cues to action by social ties were positively associated with attitudes toward COVID-19 vaccines (B = .16, P < .01, CI [.065,.26]). Cues to action by authority did not have any significant association with attitudes toward COVID-19 vaccines. Figure 1 shows the results of the SEM model. Results of the SEM model of COVID-19 Vaccine and Health Disparities: Barriers and Cue to Action. Note: N = 741, with 8 missing data. Blue paths indicate significant negative relationships, whereas red paths indicate significant positive relationships. Insignificant paths are not included for brevity. Correlation paths among the four barriers variables, correlation paths between the two cue to action variables, and the control variables: gender, age, party affiliation, perceived severity of COVID-19, perceived susceptibility of COVID-19, and self-efficacy are included in the full SEM model but not shown here for brevity.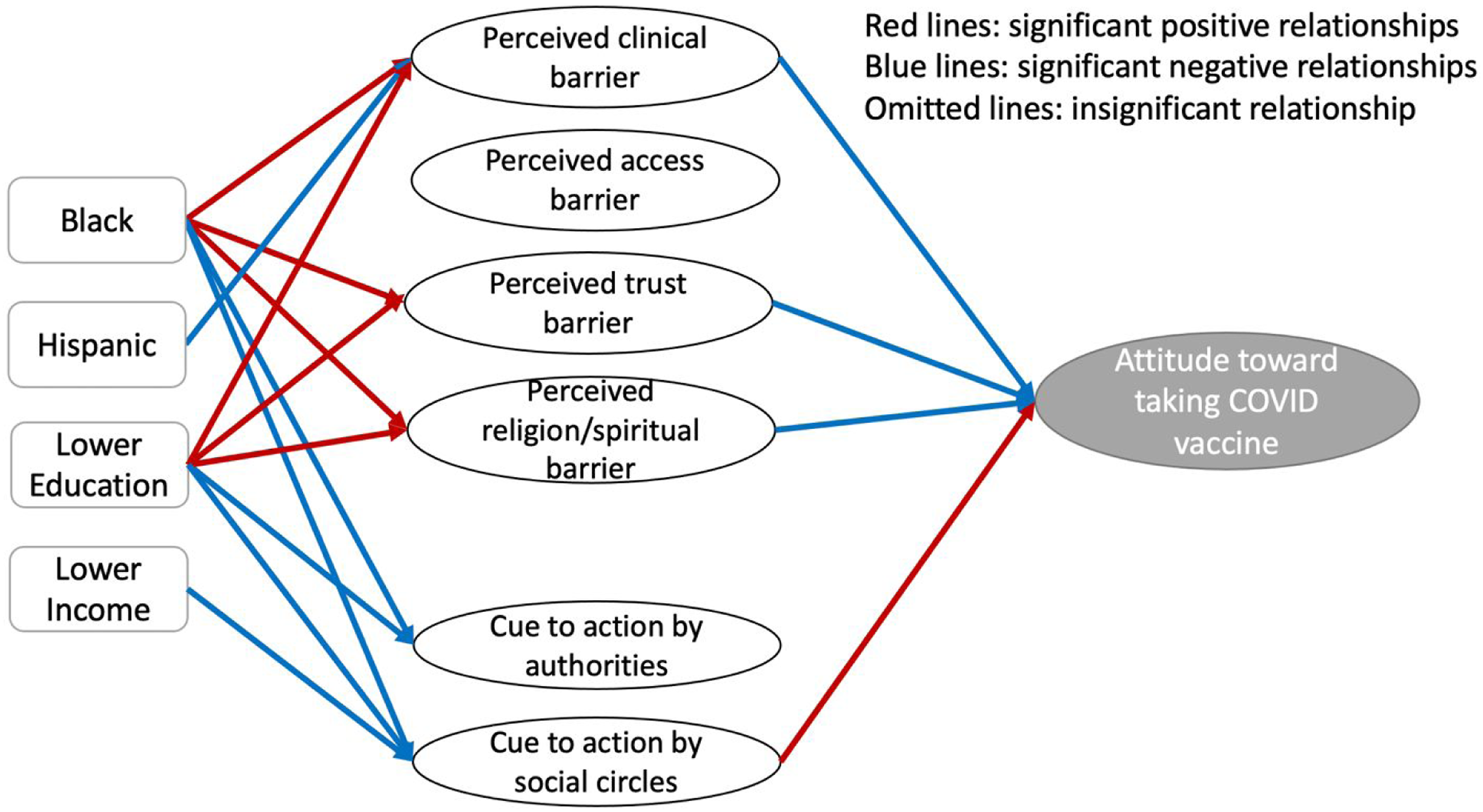
Discussion
This study examined socially disadvantaged groups’ experience with barriers to COVID-19 vaccination and cues to action. While supporting the HBM framework through a newly developed scale of barriers and cues to action, our study uncovered theoretically and practically meaningful results. Disadvantaged groups experienced higher clinical, trust, and religious/spiritual barriers, which led to a more negative attitude toward COVID-19 vaccines. Perceived access barriers did not play a role in this process, while only cues from social ties, not authorities, were positively associated with COVID-19 vaccine attitudes. Our study extended the HBM by showing that some perceived barriers and cues to action are stronger than others in their influences on COVID-19 vaccine attitudes.
Perceived Barriers
Disadvantaged groups differentially experienced barriers to COVID-19 vaccination. Concerningly, Blacks and individuals with lower education experienced higher clinical, trust, and religious/spiritual barriers, echoing other national studies.9,13 Specifically, these groups were more likely to believe that the vaccine was detrimental to their health, had severe side effects, and would make them sick. Some of these misconceptions might result from misinformation and anti-vaccine messages widely disseminated via social media and unfortunately reiterated by some opinion leaders. 30 Blacks and people of lower education also had a higher level of mistrust in actors connected to the vaccines, including the government, pharmaceutical companies, and media. Past and accumulative negative/traumatic experiences8,31 can explain such mistrust, especially for people of color. For example, the Tuskegee Study and other mistreatment examples are often cited as reasons for vaccine hesitancy/refusal. 32 Moreover, these groups are more likely to believe that they should not vaccinate because vaccines go against their religion or because religious or spiritual/natural preventive measures and cures are considered better. For example, White evangelicals and Black protestants are less likely to get vaccinated, with some calling the vaccine “the mark of the beast.” 33 Others believe natural alternatives offer better protection or cures. 34
Some findings, however, offer a silver lining. Hispanics, unlike Black individuals, did not experience religious barriers, probably because the Pope and Catholic leaders from early on promoted the COVID-19 vaccine. 35 We did not find a significant association between the four disadvantaged groups and access barriers. Thus, access barriers did not seem to be a key obstacle for disadvantaged groups in our study, even in the early stage of COVID-19 vaccination. This offers some optimistic news as access has been a concern in other vaccines in the past. 36
Clinical, trust, and religious/spiritual barriers had a significant relationship with attitudes toward COVID-19 vaccines. Even though we conducted the study early in March, access barriers were not a significant predictor of attitudes. These results have important theoretical and practical implications. On a theoretical side, the results confirmed the utility of the multidimensional conceptual approach to perceived barriers. This approach helps clarify a unique set of factors that disadvantaged groups experience when forming vaccine attitudes. On a practical side, the results point to the need for more targeted and personalized communication messages to achieve better persuasive effects for these disadvantaged groups. Health officials and communicators need to better focus on and address these perceived barriers (clinical, trust, religion/spiritual), especially as current data suggest that the increasing peak in cases is especially connected with the unvaccinated group. For example, messaging could address the vaccine’s safety, include trust-building elements, and connect the vaccine to the religious and moral duty. 8
Cues to Action
Black and less educated people experienced a lower level of cues to action by both authority and social ties. The result suggests that while these individuals were not exposed to pro-vaccine cues to action from authorities (eg, the president, local government), their social ties (eg, friends, family members) who can personally reach out to them did not encourage vaccination. There is thus a critical need to examine how authority cues to action can break through and how to engage people who can personally influence those around them within these social groups. Our results show that cues to action from social ties may be more influential in affecting attitudes toward COVID-19 vaccination.
We also found that only cues to action by social ties were significantly associated with vaccine attitudes. This result is not fully surprising. Research has shown that social norms or friends/families exert a greater influence on one’s vaccination decisions than authoritative figures. 37 It is also possible that misinformation about government, companies, and authority figures involved in vaccine development and dissemination contributed to the null finding for cues to action by authority (eg, intense disinformation campaigns against Dr Fauci). Therefore, researchers must differentiate the two types of cues to action and their differential impact. This study showed that, from a practical perspective, vaccine promotion efforts must focus on engaging ordinary people in one’s social ties because social ties are more influential than authoritative figures in promoting COVID-19 vaccination. Consequently, future messaging for COVID-19 vaccine interventions should include more people “just like them” instead of traditional sources such as governors and mayors. For example, messaging and campaigns on social media could encourage people who have been vaccinated to post about their experience so that others can see cues to action from their social ties. Thus, health professionals should engage the sources for cues to action that can have the most significant impact rather than the ones that might have traditionally worked.
The study had some limitations. The cross-sectional survey does not prove causality. Longitudinal studies are needed to draw a causal conclusion regarding how different barriers and cues to action experienced by disadvantaged groups may influence their subsequent attitudes toward COVID-19 vaccination. The national sample of participants was recruited from an online panel, which may not represent the U.S population. Moreover, the study did not include any measures related to emotions or past negative/traumatic experiences of vaccines or healthcare services, which might also affect perceived trust or clinical barriers. We identified several facts of barriers and cues to action based on existing research, but there may be other equally important dimensions. We do not have a cognitive interview from the individuals in these disadvantaged groups, to establish face validity. Finally, while HBM is a useful framework in vaccination research, it also has some limitations, such as not including past vaccination behavior
38
or cognitive or emotional predictors.
39
Nevertheless, our study serves as an essential first step toward developing effective intervention strategies to target different barriers and cues to action to increase COVID-19 vaccination. Future research should build on our study to design personalized or tailored messages to promote COVID-19 vaccination for disadvantaged groups. Research has been done to better understand individuals’ barriers and cues to actions in the context of vaccines, including the COVID-19 vaccine. This study develops and tests multidimensional barriers and cues to action in the context of COVID-19 vaccination. Furthermore, it is one of few quantitative studies to, more comprehensively, identify specific barriers and cues to actions experienced by disadvantaged groups toward COVID-19 vaccination. Trust, clinical, religious/spiritual barriers, and cues to action by social ties are stronger than the others in their influences on COVID-19 vaccine attitudes among disadvantaged groups. Therefore, health professionals need to better target and personalize the messages to these disadvantaged groups, focusing on their perceived barriers and engaging the sources for cues to action that can have the most significant impact.So What?
What is already known on this topic?
What does this article add?
What are the implications for health promotion practice or research?
Supplemental Material
Supplemental Material - COVID-19 Vaccine Hesitancy: Disadvantaged Groups’ Experience with Perceived Barriers, Cues to Action, and Attitudes
Supplemental Material for COVID-19 Vaccine Hesitancy: Disadvantaged Groups’ Experience with Perceived Barriers, Cues to Action, and Attitudes by Ioana A Coman, Shan Xu, and Masahiro Yamamoto in American Journal of Health Promotion
Footnotes
Author Contributions
IC and SX equally contributed to the design of the work, data analysis and interpretation, drafting and revising the manuscript, and approved this version for submission. MY contributed to data analysis and interpretation, drafting and revising the manuscript and approved this version for submission.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
IRB Approval Institution Information
Texas Tech U | IRB#: 00000276 | FWA: 00001568
Ethical approval/number for this study
IRB2021-49
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.