
Abstract
Purpose
To describe a 3-year demonstration project with selected Centers for Disease Control and Prevention National Comprehensive Cancer Control Program (NCCCP) award recipients to build partnerships with local organizations to improve knowledge and awareness of the association between injecting drugs and the risk for viral hepatitis and liver cancer, improve delivery of viral hepatitis services, and implement comprehensive syringe services programs.
Design
A mixed-methods descriptive evaluation of selected evidence-based interventions or promising strategies that each award recipient implemented based on the needs of their population.
Setting
Selected provider and patient populations served by NCCCP award recipients in Iowa, Minnesota (American Indian Cancer Foundation), Mississippi, and West Virginia.
Subjects
Four award recipients that implemented individually-tailored strategies and activities.
Measures
Processes were assessed through monitoring and tracking tools. Challenges, lessons learned, and recommendations were collected via qualitative interviews.
Analysis
We used descriptive statistics to analyze quantitative data. We analyzed award recipient interviews using thematic analysis.
Results
Activities were implemented across four strategies. Strong public-private partnerships, ongoing technical assistance, a deep understanding of individual populations, and a shared commitment to remaining flexible were main factors.
Conclusion
While challenges existed, award recipients implemented key strategies and activities in their populations. Findings contribute to the scaling of best practices to the larger cancer control community especially those whose populations are at higher risk for viral hepatitis.
Keywords
Purpose
Hepatitis B and hepatitis C are contributing factors to liver cancer. 1 Liver cancer has high mortality rates, especially among certain populations including Hispanic or Latino, Asian Pacific Islanders, and American Indian or Alaskan Native persons. 2 The risk of hepatitis B virus (HBV) and hepatitis C virus (HCV) transmission is particularly high among people who inject drugs (PWID).3,4 The rise in PWID during the current opioid crisis in the U.S. may in part explain the rise in liver cancer.5,6
Vaccination against HBV, and HBV and HCV testing and treatment are strategies to help prevent liver cancer. 5 The Centers for Disease Control and Prevention (CDC) funds the National Comprehensive Cancer Control Program (NCCCP) to create, implement, and evaluate plans to prevent and control cancer. 7 Increasing incidence and death rates between 2006 and 2015 made liver cancer an NCCCP priority. 8
We designed a demonstration project with NCCCP award recipients whose populations include PWID, to implement strategies to reduce viral hepatitis infections, with the goal of reversing liver cancer trends. We describe the implementation process of these award recipients in Iowa, Minnesota, Mississippi, and West Virginia.
Methods
Design
We planned for a mixed-methods descriptive evaluation to assess implementation (i.e., planning and delivering interventions) and outcomes. Based on their capacity for planning, implementation, and evaluation and the needs of their specific populations, each NCCCP award recipient selected evidence-based interventions and promising strategies (hereinafter, referred to as strategies) and activities derived from two sources: A National Strategy for the Elimination of Hepatitis B and C: Phase Two Report and Evidence-Based Strategies for Preventing Opioid Overdose: What’s Working in the United States.5,9 Strategies implemented included a hybrid of online (e.g., webinar) and in-person (e.g., outreach) activities. Each award recipient was paired with a technical assistance (TA) liaison from CDC’s contactor, ICF, to receive guidance and support throughout the demonstration period. Each pair met monthly to discuss project requirements and report on progress, challenges, and solutions. Through these meetings, we discovered that outcomes data would not be available as planned for some award recipients given shorter implementation periods as a result of the COVID-19 pandemic and lower than anticipated data collection response rates. We continued with the demonstration project with a focus on describing the process of planning and delivering strategies and activities.
Upon conclusion of the project, TA liaisons conducted four 90-minute, virtual closeout interviews, one with each award recipient. This research was reviewed and approved by the ICF Institutional Review Board (IRB) (FWA00002349, expires October 13, 2025). This project was determined by CDC not to be human subjects research requiring CDC’s IRB approval.
Sample
NCCCP award recipients were selected based on their description of needs and experience working with PWID to prevent viral hepatitis infections as a strategy for reducing liver cancer incidence in their populations. Capacity of award recipients to implement strategies and activities was assessed through completion of a worksheet and additional context during an informational call. Four NCCCP award recipients in Iowa, Minnesota, Mississippi, and West Virginia, including one tribal organization, (American Indian Cancer Foundation in Minnesota) were selected.
Measures
Each award recipient assessed process measures (e.g., reach, number of materials developed) through monitoring and tracking tools. The data monitoring and tracking tools used by award recipients included electronic medical records, Microsoft Excel, and web-based surveys (e.g., Mail Chimp, SurveyMonkey). We also assessed challenges, lessons learned, and recommendations from each award recipient during the qualitative closeout interview. Implementation and data collection occurred over an 18-month period.
Analysis
We used descriptive statistics (i.e., frequencies and ranges) to analyze quantitative process data. Qualitative data was analyzed by three team members using notes-based thematic analysis. As there were only four transcripts, the team manually coded each transcript, developing and assigning codes as we reviewed the transcripts. The team conducted the review and coding process together as a team, discussing the findings, determining the data that were relevant, and what codes to develop and use. We also synthesized contextual data from monthly reports, final reports, and closeout interviews to glean learnings across award recipients and understand ways to apply lessons to other NCCCP award recipients.
Results
Process Measures and Results by Strategy.
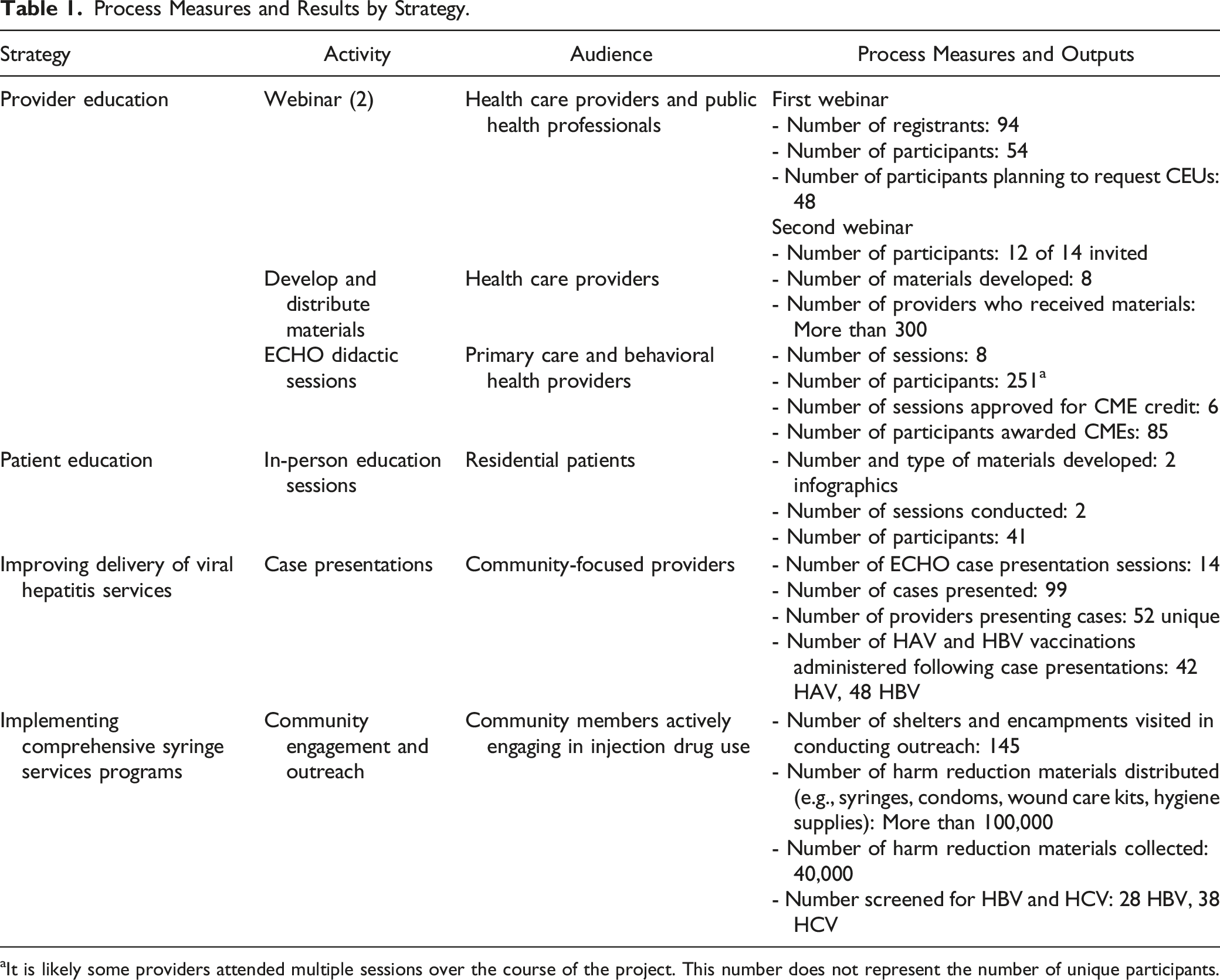
aIt is likely some providers attended multiple sessions over the course of the project. This number does not represent the number of unique participants.
The strategies conducted by each award recipient are described below. Table 1 further details the audience, process measures, and outputs for each strategy.
Provider Education
All four award recipients implemented provider education activities. Two conducted webinars on the association between opioid use, viral hepatitis, and liver cancer. Two developed and electronically distributed materials, including fact sheets, a news brief email, three infographics, and a data brief. Additionally, one award recipient implemented Project Extension for Community Healthcare Outcomes (ECHO), a model of education that brings together providers to increase access to specialty treatment in rural and underserved areas, 10 didactics to educate primary care, medication-assisted treatment, substance use disorder, and behavioral health providers on the association between opioid injection use, viral hepatitis, and liver cancer. Eight educational sessions were delivered via two separate ECHO platforms (HCV and behavioral health ECHOs).
Patient Education
One award recipient implemented activities to increase knowledge, awareness, ability, and intent focusing on the association between opioid use, increased rates of viral hepatitis, and liver cancer. Activities included distributing two infographics and conducting two in-person education sessions to educate residential patients at a substance abuse treatment center.
Improving Delivery of Viral Hepatitis Services
As part of one award recipient’s HCV ECHO activity, existing case presentation forms were updated, in conjunction with CDC, so that providers could better assess for risk factors, including opioid and injection drug use and current and past HBV infection status. With this modification, community-focused providers could virtually present cases of patients with HBV infection with more comprehensive information and consult on an appropriate course of treatment.
Implementing Comprehensive Syringe Services Programs
One award recipient partnered with a local community clinic to conduct community engagement and provide harm reduction, outreach, rapid testing, and medical services to build relationships with and bridge services for patients who decide to engage in recovery services. This award recipient also developed a data collection system to track hepatitis testing and, treatment, and for distributing and collecting harm reduction distribution materials (e.g., syringes, condoms, wound care kits, hygiene supplies).
Several themes emerged from the closeout interviews, including the need to engage partner contract offices often and early to avoid implementation delays. Conducting frequent, regularly scheduled calls and simultaneously planning implementation and evaluation of strategies and activities aided in successful execution of strategies. Additionally, award recipients learned that adapting existing materials is less burdensome than developing original content. Lastly, when working with partners, flexibility and the ability to change plans when challenges arose were key.
Discussion
Summary
Despite challenges encountered, award recipients successfully implemented their strategies and activities. Strategy implementation required strong public-private partnerships, ongoing TA, a deep understanding of award recipients’ individual populations, and a shared commitment to remaining flexible throughout the demonstration period.
These award recipients adopted strategies from past efforts of two other NCCCPs and expanded on the number and types of strategies and activities.11,12 While the current four award recipients implemented provider and patient education, they expanded their focus to include two new strategies: improving delivery of viral hepatitis services and implementing comprehensive syringe service programs. Conducting these two new strategies led to additional local partnerships, which in turn led to a broader reach of the intended audience. The addition of the viral hepatitis service strategy expanded the Project ECHO activities by including case presentations which resulted in more specialized treatment for patients with HBV and HCV infection. The addition of the comprehensive syringe service program strategy allowed for a specific focus on engagement with community members that were actively injecting drugs. These four strategies are promising practices that can be scaled13 and adopted by other NCCCPs.
Award recipients encountered several challenges. The project launched shortly before the onset of the COVID-19 pandemic, which strained the capacity of the award recipients, especially ones that were planning education activities since they had to transition to delivering content virtually. Some award recipients experienced staffing changes, which made developing presentation materials and pre-post assessments across strategies burdensome, and some found it challenging to develop new content for their activities. The TA in planning and executing strategies and developing content for presentations alleviated the burden for award recipients and allowed them to use and adapt content accordingly. Finally, providers’ competing priorities were a barrier to completing pre- and post-assessments for provider education activities. Offering incentives such as CME credits or an hour of administrative time were believed to be useful in addressing this challenge. 13
Limitations
Findings are based on a small number of award recipients and may not be generalizable to all NCCCP award recipients and populations. Also, award recipients had difficulty collecting adequate data to evaluate outcomes across strategies. Finally, the implementation period was too short to allow measuring of reductions in liver cancer diagnosis among PWID.
Significance
We identified key components for implementation of the strategies and activities described. These findings contribute to the scaling of best practices to the larger cancer control community and, in particular, will benefit other NCCCP award recipients whose populations live or work in settings that put them at increased risk for viral hepatitis or experiencing health disparities. Several new resources were developed as a result of this project which can be used by other award recipients interested in conducting similar work. These resources are publicly available at https://www.cdc.gov/cancer/liver/opioid-users/index.htm.
The Centers for Disease Control and Prevention provides funding and technical assistance to National Comprehensive Cancer Control Program award recipients to create, implement, and evaluate cancer plans. Vaccination and testing for viral hepatitis are strategies that can help prevent liver cancer among people who inject drugs. We describe strategies and activities to promote vaccination and testing for viral hepatitis among people who inject drugs implemented by National Comprehensive Cancer Control Programs whose populations are disproportionally affected by viral hepatitis and liver cancer. We also highlight successes and challenges in this work that may be useful for programs seeking to implement similar strategies. The award recipients expanded on the number and types of strategies and activities from past efforts. The addition of the two new strategies expanded the Project ECHO activities by including case presentations and allowed for a specific focus on engagement with community members that were actively injecting drugs. These additional strategies are promising practices that can be scaled and adopted by other NCCCPs. Future studies that explore readiness factors that contribute to successful implementation and measure longer-term outcomes in behavior change and vaccination and testing rates can provide information on the effectiveness and sustainability of these strategies.SO WHAT?
What is Already Known on This Topic?
What Does This Article Add?
What are the Implications for Health Promotion Practice or Research?
Footnotes
Acknowledgments
The authors would like to acknowledge staff from the following award recipients who implemented the demonstration project: American Indian Cancer Foundation in St. Paul, Minnesota, Iowa Department of Health and Human Services, Mississippi State Department of Health, and West Virginia Bureau for Public Health.
Author Contributions
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Disclosure
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.