
Abstract
Purpose
Since LGBTQ + communities experience disproportionate rates of suicidality; it is important to identify strategies for suicide prevention. Research shows that supportive interpersonal communication and identity affirmation helps prevent suicide. The purpose of this analysis is to explore the role of communicative resilience in suicide prevention among LGBTQ + communities.
Approach
This analysis is part of a community-based participatory research project.
Setting
In November 2021, a Community-Academic Partnership hosted a virtual town hall, via Zoom, immediately followed by five Community Conversation (CC) groups.
Participants
Participants were aged 18 years or older and identified as an LGBTQ + community member or active ally. We define active ally as an individual who, through their personal relationships, service to the community, or professional work, actively advocates for and supports members of LGBTQ + communities.
Method
CC groups were audio-recorded and transcribed (n= 25 participants). Transcripts were inductively coded for thematic analysis and identified themes were deductively coded using Communication Theory of Resilience (CTR) to identify observations of communicative resilience (MaxQDA2020).
Results
Themes aligned with CTR, including importance of peer and professional support, affirming identities, reducing stigma, cultivating hope, and advocating for equitable policies.
Conclusion
Findings demonstrate that through communication, members of LGBTQ + communities enact processes of resilience that support and promote suicide prevention. These findings support community mobilization, communicative resilience, and advocacy to help save lives.
Keywords
Introduction
Background
Suicide is the 2nd leading cause of death in the United States (US) for adolescents and young adults (ages 10 – 34 years of age), and the 10th leading cause overall. 1 The US Centers for Disease Control and Prevention (CDC) views suicide prevention as a priority and the National Institute of Mental Health (NIMH) declares intersectional perspectives of population health, including sexual and gender minority (SGM) populations (often referred to as LGBTQ+) as a focus area for research and intervention. 2 According to The Williams Institute at University of California in Los Angeles, in 2017, approximately 4.6% of adult Florida residents identified as LGBT. 3 Additionally, almost half of the adult LGBT population of Florida was between the ages of 18 – 34. 3 Although there has been much research in the field of suicide prevention, more research is needed regarding strengths-based suicide prevention and interventions at a population level. 2
For example, the Zero Suicide approach demonstrates the value and success of integrated screening and treatment pathways for suicide prevention in clinical settings. 4 However, this framework which includes seven steps (e.g., four clinical: Identify, Engage, Treat, Transition and three administrative: Lead, Train, and Improve) does not emphasize the role of supportive relationships outside the clinical setting. Additionally, frameworks such as Appreciative Inquiry (AI) focus on strengths-based community mobilization for complex change. 5 Yet, AI lacks specificity in how best to harness identified resources to promote resilience and strengthen community connections. Both frameworks are valuable tools for addressing this critical issue, but there are still gaps in how to mobilize these efforts across the community, including formal treatment pathways, as well as informal social support to help build connectedness and resiliency with vulnerable populations.
Purpose
Research shows connectedness, along with supportive and affirming social networks can help prevent suicide, particularly for individuals of LGBTQ + communities.6-11 Communication is an essential and intricate aspect of connectedness, which occurs in community settings. However, studies examining communication as a process of resilience for community-wide suicide prevention are extremely limited. Specifically, the role of communicative resilience and strengths-based suicide prevention has been understudied among LGBTQ + communities.6-11 Communicative resilience is an umbrella term for describing the resilience cultivated through five processes described in Buzzanell’s Communication Theory of Resilience (CTR). 12
Since LGBTQ + communities experience disproportionate rates of suicidal thoughts and attempted suicide, it is important to identify and explore strategies for suicide prevention among these communities.13-23 For these reasons, this study pursued the following objectives: 1) use AI to engage members of local LGBTQ + communities in conversations regarding suicide prevention and 2) identify and assess the use of communicative resilience in suicide prevention for these local LGBTQ + communities. Therefore, this analysis seeks to answer, “How are communicative resilience processes enacted for suicide prevention among LGBTQ + communities?”
Method
This analysis is part of a larger, ongoing, community-based participatory research project. An established Community-Academic Partnership (CAP) collaborated in planning and hosting a virtual community engagement event in late November 2021, via Zoom. The CAP consists of community representatives from multiple behavioral health organizations, advocacy groups, faith groups, government agencies, youth groups, and other community organizations. Additionally, students, staff, and faculty from a local college and a local state university represent the academic component of the CAP. All representatives of the CAP were provided an opportunity to join planning sessions separate from the monthly CAP meeting. Those who chose to participate in planning for this study provided insights, feedback, edits, review, and approval of the event format, recruitment materials and strategy, public communications, design of the data collection, and the data analysis plan.
The study protocol was submitted to an academic Institutional Review Board (IRB) and determined to be exempt from IRB review because the study poses no greater than minimal risk for participants. The research was completed in accordance with the Declaration of Helsinki as revised in 2013. Participants were provided information regarding the purpose of the study, data collection, and processes of audio-recording and transcription.
The online event included opening remarks by a leader of a partnering organization and a moderated panel of community members and allied health professionals. The panel session was moderated by a behavioral health professional who serves individuals of local LGBTQ + communities and who also identifies as a member of an LGBTQ + community. This portion of the event was not audio-recorded and is not included in the analysis.
At the conclusion of the panel session, attendees were invited to participate in audio-recorded virtual Community Conversation (CC) groups. 24 Attendees were randomly assigned to one of five CC groups via Zoom breakout sessions. At this point, the IRB-approved verbal consent process began. Participants provided verbal consent prior to recording and data collection. Anyone who did not wish to participate was able to remove themselves from the breakout session and participate in an unrecorded discussion in the main Zoom meeting. No data were gathered from the main Zoom session while groups were being conducted.
Setting
During the virtual CC groups, participants were free to choose whether they would like to use the Zoom video function or turn their camera off for the conversation. Most participants chose to keep their videos on. Most breakout sessions were small in number of participants (e.g., 3-6 participants) so that everyone would be provided with a chance to share during the CC group. Facilitators introduced themselves (including their pronouns) and conducted the verbal consent process prior to recording the CC group session.
Participants
The virtual event was open to anyone in the public via pre-registration. However, purposive sampling guided recruitment efforts, with the event flyer specifying that the event was focused on suicide prevention among LGBTQ + communities. The virtual flyer was shared across Facebook and Instagram platforms through non-sponsored posts by member organizations of the CAP. Additionally, the virtual flyer was shared among online newsletters and list servs by the academic representatives of the CAP to those within their organizations. Print copies of the flyer were shared by member organizations in their community centers, waiting rooms, and on bulletin boards of LGBTQ + -friendly local businesses.
Participants were 18 years of age or older and identified as an LGBTQ + community member or active ally. For this study, an active ally is defined as an individual who, through their personal relationships, service to the community, or professional work, actively advocates for and supports members of LGBTQ + communities. One participant opted to leave the CC group early, about half-way through the breakout session, and returned to the main Zoom session.
Approach
Community Conversations
The semi-structured groups employed a Community Conversations style of engagement and inquiry. 24 Before the event, a facilitation guide was developed by academic representatives of the planning team and reviewed during a planning meeting. Once approved, it was provided to select CAP members who volunteered to serve as CC group facilitators. The purpose of the guide was to assist facilitators in leading the group sessions, including which data questions were to be asked and how to respond to disruptive participants. As members of local LGBTQ + communities, facilitators were also invited to participate by sharing their insights and experiences related to mental health, suicide, connectedness, community, and resilience.
Appreciative Inquiry Framework
During Community Conversations, participants were asked four questions, informed by the AI framework, related to suicide prevention in their community.5,24 AI emphasizes the identification, cultivation, and utilization of collective strengths, assets, and hope in addressing concerns common to a group or community. 5 The four questions were: 1) What services have helped you or someone you know in a suicide situation? 2) What would an ideal community look like that is absent of suicides? 3) What would a community look if all people are flourishing? 4) What actions are we going to take to improve and change the culture to reduce suicides in our community? The questions were asked one at a time, providing participants within the groups time to respond to the question and one another.
Coding and Analysis Strategies
The five Zoom audio recordings were individually transcribed via Microsoft Word Online, providing speaker numbers and timestamps for each of the five transcripts. Transcripts were compared to original audio and edited for verbatim transcription by the first author. Additionally, participant names were manually redacted, by the first author, prior to coding and analyses. The anonymous transcripts were then imported into MaxQDA2020 and inductively coded, by the first author, to identify processes of communicative resilience, as informed by CTR.12,25 The five processes described by CTR are Using and Maintaining Communication Networks, Affirming Identity Anchors, Crafting Normalcy, Putting Alternative Logics to Work, and Backgrounding Negative Emotion While Foregrounding Productive Action. 12
Emergent themes within the five processes of communicative resilience were also captured via open coding, by the first author, to provide context and rich descriptions of how the processes are enacted by the participants, particularly for the purposes of suicide prevention. Final CTR processes and related emergent themes were reviewed, and a consensus reached by all authors.
Results
Across the five groups, data were gathered from a total of twenty-five participants. Although participants’ specific demographic information was not collected due to the data collection method, some participants self-identified within their responses during the community conversations. Any demographic information provided by participants was unsolicited. The identities explicitly captured within the transcripts were likely not exhaustive of participants’ demographic identities. Multiple gender identities, sexual orientations, and races were self-identified by participants across the five groups. However, due to missing demographic data for some participants, demographic and intersectional analyses are not possible.
CTR Processes & Emergent Themes
Themes of communicative resilience in suicide prevention as demonstrated by Participant quotes.
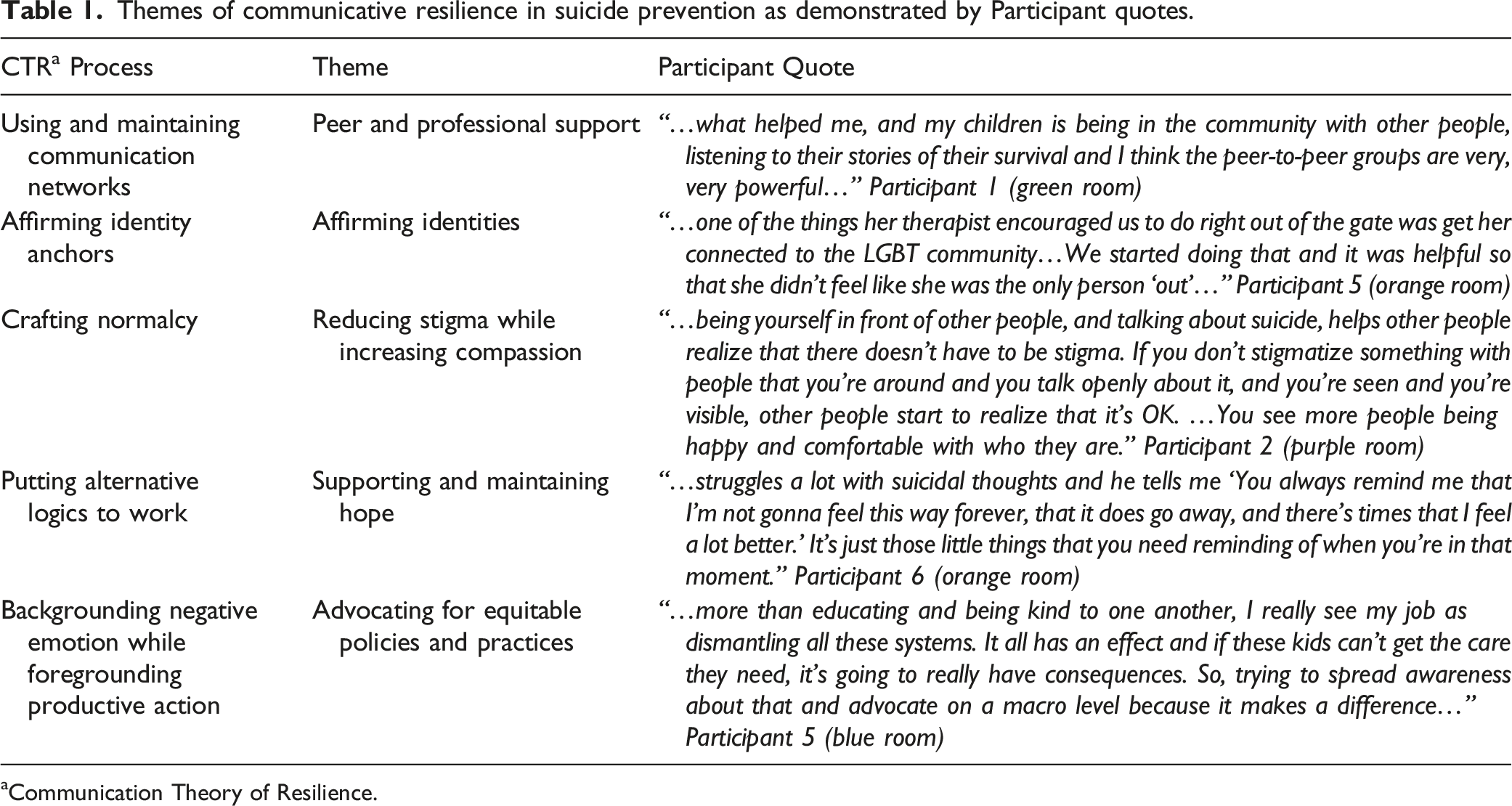
aCommunication Theory of Resilience.
Process 1. Using and Maintaining Communication Networks
By far the most salient theme was the vital role of peer and professional support (#1). Professional support was described as gender-affirming medical care, therapeutic counseling, and psychiatric support. Additionally, peer support was emphasized as an essential tool for communicative resilience. Participants described multiple systems and formats of peer support. Formal systems of peer support included crisis lines, community support groups, peer-to-peer grief support, and peer-led behavioral health events.
Other peer support was informal, such as turning to loved ones for support with building safety plans, reaching out to friends when they are having difficult times, and sharing information about mental health resources. Importantly participants shared that in helping others through difficult times, they too felt a renewed sense of hope and connectedness that supported their own processes of enacting communicative resilience.
Process 2. Affirming Identity Anchors
One participant shared their experience of supporting their young daughter as she struggled with feelings of isolation and stigma, after openly identifying as queer at school and suffering from suicidal thoughts (#2). By normalizing conversations of identity, mental health, and seeking support while affirming their daughter’s identity as a queer youth, this parent was able to save their daughter’s life through connecting with professional and peer support in the community. Although this example demonstrates the enactment of multiple processes of communicative resilience, the participant focused on the powerful impact of affirming their child’s identity. Affirming the identities of LGBTQ + individuals, especially youth, was discussed across all groups.
Process 3. Crafting Normalcy
Participants emphasized the impact communication has had on them and their loved ones during moments of crisis. Feelings of connectedness and acceptance were described in examples of brief, informal conversations among colleagues (#3). Dreams of creating a community where kindness is normalized, and even taught, at early ages to foster empathy, compassion, and connection were present across groups. Additionally, normalizing conversations around suicide, mental health, and difficult emotions were deemed vital for reducing the stigma faced by individuals and families going through crises or who have experienced suicidality. Participants explained that by reducing the stigma around these issues and encouraging open, honest conversations, there would be better opportunities for the prevention of crises and suicidality.
Process 4. Putting Alternative Logics to Work
Participants consistently responded that the cultivation and maintenance of hope are essential to suicide prevention (#4). Hope was described both as an aspiration gained through other communicative resilience practices and a tool of communicative resilience directly impacting suicide prevention efforts. Supporting and maintaining hope were detailed in participant stories of therapeutic communication, supporting siblings through crises by focusing on the temporary nature of the present pain, and through systemic changes that enable communities to visualize and actualize a flourishing future for themselves.
Process 5. Backgrounding Negative Emotion While Foregrounding Productive Action
The form of communicative resilience with the broadest potential impact on suicide prevention for LGBTQ + communities but also the most daunting (emotionally and logistically) was advocating for equitable policies and practices (#5). Participants provided examples exclaiming the: destructive nature of proposed state legislation targeting transgender youth, difficulty of supporting queer youth in schools, need for more caregiver education on youth mental health, trauma of involuntary hospitalization, disproportionate impact lack of affordable housing has on LGBTQ + communities, and the need for culturally competent mental health care in schools. Participants spoke of these issues with passion, frustration, concern, and determination. 26
LGBTQ + Youth
Participants across all five groups shared thoughts, fears, recommendations, and hopes specifically related to LGBTQ + youth. Although the AI questions asked by facilitators during the CC groups did not reference youth, there was a panelist who had lost her daughter (identified as queer) to suicide and shared her story of loss during the moderated panel discussion, prior to the CC groups. Participant comments regarding LGBTQ + youth included personal stories of their children, reflections of their own experiences growing up, and examples of working with LGBTQ + youth through their professional roles.
Discussion
Discussions of suicide prevention, whether taking place in a clinical setting or in the community, are often dominated by recitation of risk factors and warning signs.1,13 When support and resources are brought into these conversations, they are primarily focused on suicide prevention call centers, seeking behavioral health treatment, and crisis intervention strategies.4,14 The use of AI in CC groups regarding suicide prevention allows space for more expansive discussions, including identifying strengths (rather than solely risks), sharing stories of healing, envisioning a more empathic and connected community, and cultivation of hope through community mobilization.5,10-12,24
The benefits of this strategy may be applicable to multiple populations. 5 In particular, as demonstrated in the results shown here, the use of AI in discussions of suicide prevention for LGBTQ + communities enabled participants to identify and enact processes of communicative resilience through participating in these CC groups.5,12 LGBTQ + communities, which are often marginalized and experience some of the highest rates of suicidality among any demographic population in the US, were able to share strengths, strategies, sources of hope, and connection through these discussions.13-16,24
Though not previously explored within the field of suicide prevention, communicative resilience processes can be identified throughout many best practices in suicide prevention.7,12 For example, affirming communication and support reduces suicidality among LGBTQ + individuals. 11 Additionally, feeling a sense of connectedness to their peers and a sense of belonging within their community also serve as protective factors. 17 Though these are broadly discussed in suicide prevention literature, findings from this analysis provide an example of how communicative resilience serves as a framework for cultivating and supporting these protective factors for suicide prevention among LGBTQ + communities. 12 The CTR themes identified: peer and professional support, affirming identities, reducing stigma while increasing compassion, supporting and maintaining hope, and advocating for equitable policies and practices represent a spectrum of evidence-based practices and community-defined evidence to support suicide prevention among LGBTQ + communities.9-12 Furthermore, the stories shared by participants underscore both the need for suicide prevention efforts throughout this community and also the capacity for collective healing and transformation.5,9,17,26
Limitations
As mentioned previously, demographic data were not asked of participants. Processes of communicative resilience may vary by specific LGBTQ + populations. This study utilized a qualitative cross-sectional Community Conversations format and therefore our findings are not meant to be generalizable. This methodology may be a replicable and sustainable option for other geographic areas and priority populations for researching communicative resilience for suicide prevention. Although all participants were local, some findings may be transferable to LGBTQ + communities in similar geopolitical settings. Additionally, further research is warranted to explore the potential of using a combined AI and CTR framework for community-wide suicide prevention.5,12
Next Steps
The Community-Academic Partnership will continue collecting data through additional outreach events, including events specifically for LGBTQ+ and youth for suicide prevention. As data collection and analyses are completed for future outreach events, the partners will share findings with stakeholders to inform future work and promote collaboration through community engagement, communicative resilience, and ongoing advocacy to help save lives.
Conclusion
Community Conversations identify and provide opportunities for resilience.
24
It is common for suicide prevention resources to emphasize the importance of talking with others, reaching out for help, and maintaining a sense of connectedness.6-11 By applying the Communication Theory of Resilience in our analyses of Community Conversation groups, we provide a framework for how these communicative practices are identified, perceived, and enacted by local LGBTQ + communities for resilience and suicide prevention.24,26 Our findings demonstrate that through multiple forms of communication, members of LGBTQ + communities enact processes of resilience that support and promote suicide prevention. Participants responded to the four AI questions with stories, examples, and insights that spanned, and occasionally overlapped with, all five CTR processes. Suicide is a leading cause of death in the U.S. and LGBTQ + communities face disproportionate rates of suicide.
1
Research shows connectedness, along with supportive and affirming social networks can help prevent suicide, particularly among LGBTQ + communities.6-11 Communication is an essential aspect of connectedness.
24
A community-academic partnership conducted Community Conversations with local LGBTQ + community members to learn about strategies for community-wide suicide prevention.
24
We learned communication enables processes of resilience which support connection, compassion, hope, empathy, and equity for suicide prevention in LGBTQ + communities. This is the first-time communicative resilience has been studied in the context of suicide prevention. By applying the Communication Theory of Resilience in our analyses of Community Conversations, we provide a framework for how communicative resilience is enacted by local LGBTQ + communities for connectedness and suicide prevention.24,26 This methodology is a replicable and sustainable option for researching communicative resilience for suicide prevention among other populations.So what? (Implications for Health Promotion Practitioners and Researchers)
What is already known on this topic?
What does this article add?
What are the implications for health promotion practice or research?
Footnotes
Acknowledgments
The authors would like to acknowledge the organizations and community members who assisted in planning, recruiting, hosting, facilitating, and otherwise supporting this event. Additionally, all involved would like to give special thanks to the community members and participants who attended the event and provided their valuable insights and incredible stories. Finally, the authors would like to acknowledge those who have struggled or are currently struggling with suicidal thoughts, have survived suicide attempts, and have lost loved ones to suicide. You are not alone and there is help available. 988 connects to the national 24/7 suicide prevention lifeline and 1-866-488-7386 connects to The Trevor Project’s national lifelines for LGBTQ + youth.
Authors’ Contribution
Author 1: Writing – original draft (lead); Methodology (equal); Data ![]() curation (lead); Formal analysis (lead); Visualization (lead); Writing – review and editing (equal). Author 2: Supervision (equal); Data curation (supporting); Conceptualization (lead); Resources (supporting); Writing – review and editing (equal); Methodology (equal). Author 3: Supervision (equal); Conceptualization (supporting); Resources (supporting); Project administration (lead); Writing – review and editing (equal). Author 4: Methodology (equal); Formal analysis (supporting); Writing – review and editing (equal). Author 5: Conceptualization (supporting); Methodology (equal); Data curation (supporting); Project administration (supporting); Writing – review and editing (equal). Author 6: Supervision (supporting); Resources (lead); Conceptualization (supporting); Methodology (equal); Formal analysis (supporting); Writing – review and editing (equal).
curation (lead); Formal analysis (lead); Visualization (lead); Writing – review and editing (equal). Author 2: Supervision (equal); Data curation (supporting); Conceptualization (lead); Resources (supporting); Writing – review and editing (equal); Methodology (equal). Author 3: Supervision (equal); Conceptualization (supporting); Resources (supporting); Project administration (lead); Writing – review and editing (equal). Author 4: Methodology (equal); Formal analysis (supporting); Writing – review and editing (equal). Author 5: Conceptualization (supporting); Methodology (equal); Data curation (supporting); Project administration (supporting); Writing – review and editing (equal). Author 6: Supervision (supporting); Resources (lead); Conceptualization (supporting); Methodology (equal); Formal analysis (supporting); Writing – review and editing (equal).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The study protocol was submitted to the University of South Florida’s Institutional Review Board (IRB) and determined to be exempt from IRB review because the study poses no greater than minimal risk for participants (Study003380).
Clinical Trial Registration
Clinical trial registration is not applicable to this study, as this is not a clinical trial.