
Abstract
Purpose
Lack of sleep is a harm that can lead to chronic diseases ranging from diabetes to heart disease. We examined the exposure to interpersonal violence and its association with sleep, following the COVID-19 stay-at-home order.
Design
Cross-sectional.
Setting
Surveys were completed online and via paper-and-pencil in English and Spanish (N = 2049; RR = 68.4%).
Subjects
Respondents were 18+ and residing in Chicago.
Measures
The Chicago Department of Public Health’s “2022 Healthy Chicago Survey COVID-19 Social Impact Survey”.
Analysis
We developed two weighted models. Model 1 examined the effects of neighborhood violence on meeting the national sleep recommendation. Model 2 examined the effects of violence in the home among friends or family on meeting the sleep recommendation, incorporating additional predictors: victimization, stress, gender, race/ethnicity, household income, and general health. Odds ratios were estimated using multivariate logistic regression.
Results
Exposure to neighborhood violence and sleep was not significant, but knowing a friend or family member who experienced violence or mistreatment in their home affected the odds of meeting the sleep recommendation (OR = .61, 95% CI = .44-.84). Non-Hispanic Blacks had 52% lower odds of meeting sleep recommendations (OR = .48, 95% CI = .37-.63).
Conclusion
Addressing the harms to sleep that followed COVID-19 should engage diverse stakeholders in implementing culturally responsive interventions to promote adequate sleep and prevent chronic disease.
Purpose
Interpersonal violence is a social determinant of health that affects a substantial proportion of the population. Approximately 25% of women and 14% of men experience domestic violence within their lifetime. 1 Numerous studies document the indirect harms of domestic violence on health – particularly among children and adolescents. For example, national estimates show that over 40% of adolescents, aged 14-17 years, have been exposed to family violence. 2 This exposure can harm cognitive development, behavioral regulation, and mental health. 3 Another type of interpersonal violence that affects health is community violence, including assaults and homicides. Among adults, even indirect exposure to community violence can result in stress and challenges to social function at school or work. 4 There is a paucity of research on the effects of interpersonal violence – both domestic and community violence – on health in adulthood, and this merits more research.3,5 This research is particularly important as scholars have documented increased risks for interpersonal violence during the COVID-19 pandemic’s stay-at-home order that disproportionately affected lower income households and communities of color.6–8
In addition to increased risks for interpersonal violence, there is evidence that health and health-related behavior changed during the pandemic. For example, recent research suggests that people experienced sleep disruptions. 9 The American Academy of Sleep Medicine recommends adults get 7 or more hours of sleep per night. 10 Poor sleep has been linked to chronic disease, including metabolic disorders, obesity, diabetes, and hypertension, which increases risk for heart disease and stroke. 11 Although some research suggests that people may have spent more time in bed during the pandemic, sleep problems were likely exacerbated. 12 In a recent study, approximately 10% of people reported improved sleep quality during the pandemic, but nearly 44% of people experienced a worsening of sleep quality. 13 Individuals with chronic conditions may have faced behavioral health challenges during the pandemic, as data show that obese adults reported less physical activity and less sleep during this time. 14 More generally, previous research has found that men and women get a similar amount of sleep per night, while non-Hispanic Blacks face worse quality sleep; higher levels of education, income, and socioeconomic status have also been associated with better sleep quality and duration.15,16
Sleep disruptions during the pandemic are important to understand, as “increasing the proportion of adults who get enough sleep” is a national health objective in Healthy People 2030. 17 Disruptions to sleep include exposure to violence, a relationship that was documented in a 2019 systematic review across 23 studies involving clinical and community samples. 18 Examining the population-level association between exposure to violence and sleep, following the COVID-19 pandemic, is important to assessing the pandemic’s harms on population health and to effectively promote sleep and healthy communities. The present study involved analysis of data from a public health surveillance survey by the Chicago Department of Public Health. The specific purpose of this study is to examine exposure to neighborhood-based violence and domestic violence and its association with meeting the national sleep recommendation, following the COVID-19 stay-at-home order in Chicago, Illinois.
Methods
Measure
Since 2014, the Chicago Department of Public Health (CDPH) has conducted an annual population-based survey of health among adults residing in Chicago, called the Healthy Chicago Survey (HCS). The 2021 HCS’s detailed methodology has been documented elsewhere, 19 briefly, it utilized an address-based sampling frame and gave sampled individuals the choice to complete the survey via web or paper. The HCS asked respondents of the 2021 survey (N = 4237) whether they would be open to contact in the future. Those who responded “yes” were contacted for the 2022 Healthy Chicago Survey COVID-19 Social Impact Survey (COVID-19 SIS). The purpose of this survey was to gain a deeper understanding of COVID-19’s impact on Chicago residents. The COVID-19 SIS was a 68-item survey that inquired about 12 topic areas related to the pandemic, including, general health, access to care, financial security, employment, housing, child education, violence, mental health, cannabis use, alcohol, sources of information, and COVID-19 specific information.
Sample
The majority of the 2021 HCS respondents, 2994 (70.6%), indicated a willingness to be contacted for the COVID-19 SIS. Among these respondents, 2049 completed the survey (response rate = 68.4%). The survey administration period occurred from April to June 2022. The majority of COVID-19 SIS surveys were completed via the web (N = 1970), while the minority were completed via paper (N = 79). Most were administered in English (N = 2033), while the remaining surveys were administered in Spanish (N = 16). Survey respondents were offered a $2 unconditional incentive in the first contact attempt and were promised a $10 incentive in the form of a check or gift card in the mail following their completion of the survey. A three-step weighting procedure was implemented to account for the presence of children within the household, non-consent, and non-response. The weighting procedure also made the 2022 HCS COVID SIS respondents more closely match population distributions. DePaul University’s Office of Research Services deemed the present study non-reviewable since it used secondary data with no identifiers.
Our primary focus was on the relationship between exposure to violence (occurring in the neighborhood or the home) and sleep. A COVID SIS item asked respondents whether they had “witnessed violence in [their] neighborhood,” while a second item asked if they “know of friends or family members who experienced violence or mistreatment in the home.” Respondents provided a yes or no answer for both items, over a recall period of 12 months. To estimate sleep, respondents were asked “On average, how many hours of sleep do you get in a 24-hour period?” Respondents provided both hours and minutes. Responses that were under 7 h were coded as not meeting sleep guidelines, per the American Academy of Sleep Medicine recommendation, 10 while responses that were 7 h or more were coded as meeting sleep guidelines.
We also used COVID-19 SIS data for eight additional predictor variables. These predictors included having “personally experienced violence in your neighborhood,” and having “experienced violence or mistreatment within your home” (both yes/no responses within the past 12 months). To account for stress among respondents, we used data on being “worried or stressed about having enough money to pay rent or mortgage.” Response options were always, usually, sometimes, or never. We also used self-reported general health as a predictor variable (excellent, very good, good, fair, poor). Demographic data from the survey were also used for gender (male or female), age (18-24, 25-29, 30-44, 45-64, 65 or older), race and ethnicity (non-Hispanic White, non-Hispanic Black, non-Hispanic Asian American or Pacific Islander, Other, or Latino), and household income (Less than $10,000, $10,000 to less than $15,000, $15,000 to less than $20,000, $20,000 to less than $25,000, $25,000 to less than $35,000, $35,000 to less than $50,000, $50,000 to less than $75,000, $75,000 or more).
Design and Analysis
We used a cross-sectional design, developing two multivariate logistic regression models. Model 1 examined the effects of neighborhood violence on meeting the sleep recommendation (i.e., 7 or more hours per night, on average). Model 2 examined the effects of violence in the home among friends or family on meeting the sleep recommendation. We began our model building process by conducting Pearson chi-square analyses, examining the relationship between these focal variables on meeting the sleep recommendation. We also examined the relationship between personally experiencing violence in the neighborhood and meeting the sleep recommendation, and personally experiencing violence in the home and meeting the sleep recommendation. Finally, we conducted chi-square analyses on meeting the sleep recommendation and stress, as well as meeting the sleep recommendation and five additional predictors (gender, age, race/ethnicity, income, and general health). We kept each predictor variable for the model building process if P ≤ .2.
Next, we ran unadjusted univariate logistic regression models with each predictor and our outcome of meeting the sleep recommendation. We built our multivariate logistic regression models, in a stepwise fashion, and used them to calculate adjusted odds ratios and 95% confidence intervals. The first step involved our focal independent variables – witnessing neighborhood violence (Model 1) and knowing of domestic violence (Model 2) as well as victimization variables – personally experiencing violence in the neighborhood (Model 1) or the home (Model 2) and our dependent variable of meeting the sleep recommendation. In our second step, we added four predictor variables to each model (stress, gender, race/ethnicity, and household income). In our final step, we added general health. We assessed collinearity among our predictor variables; the variance inflation factor was 1.4, showing minimal correlation among these predictors. The reference group for the models was a white man (18-24 years old) with an income of $75,000 or more, in excellent health, who had not witnessed, known of, or experienced violence. We performed these analyses with StataSE 16.1 using the svy: suite of commands to account for features of the complex survey sample design (StataCorp LLC).
Results
Demographic Results
Demographic Characteristics of Study Sample in Chicago, Illinois, April–June 2022.
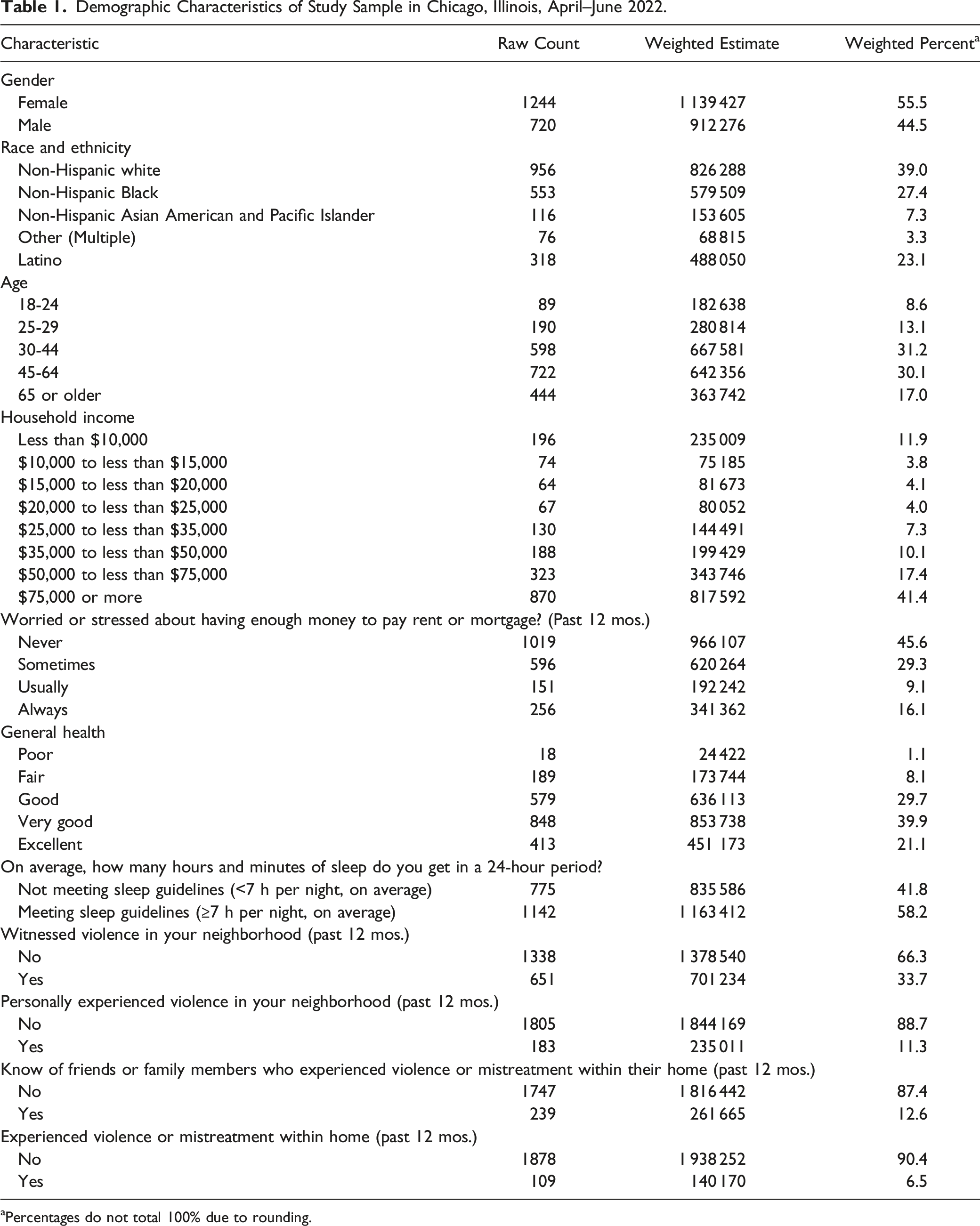
aPercentages do not total 100% due to rounding.
Bivariate Results
Descriptive Statistics of Study Sample and Bivariate Analysis Used for Model Building in Chicago, Illinois, April–June 2022.

aχ2 test was used.
bNon-Hispanic Asian American and Pacific Islander included: Asian Indian, Chinese, Filipino, Japanese, Korean, Vietnamese, and “Another Asian origin.”
cSome other race included any race that did not include the racial categories provided, here.
Regression Model 1 – Neighborhood Violence and Sleep
Unadjusted logistic regression models showed that when meeting the sleep recommendation was regressed on each predictor, they were all significant (P ≤ .2), except age (OR = .95, 95% CI = .87-1.03); therefore, age was excluded from both regression models. Those who were exposed to neighborhood violence had 39% lower odds of meeting the sleep recommendation (OR = .61, 95% CI = .50-.74). This relationship remained significant when “experiencing neighborhood violence” was added into the model (OR = .69, 95% CI = .56-.85), but when adding stress and other predictors (gender, race and ethnicity, and household income), the model was not significant (OR = .83, 95% CI = .66-1.04).
Regression Model 2 – Knowledge of Domestic Violence and Sleep
Weighted Multiple Logistic Regression Model of Predictors for Meeting Sleep Guidelines in Chicago, Illinois, April–June 2022.
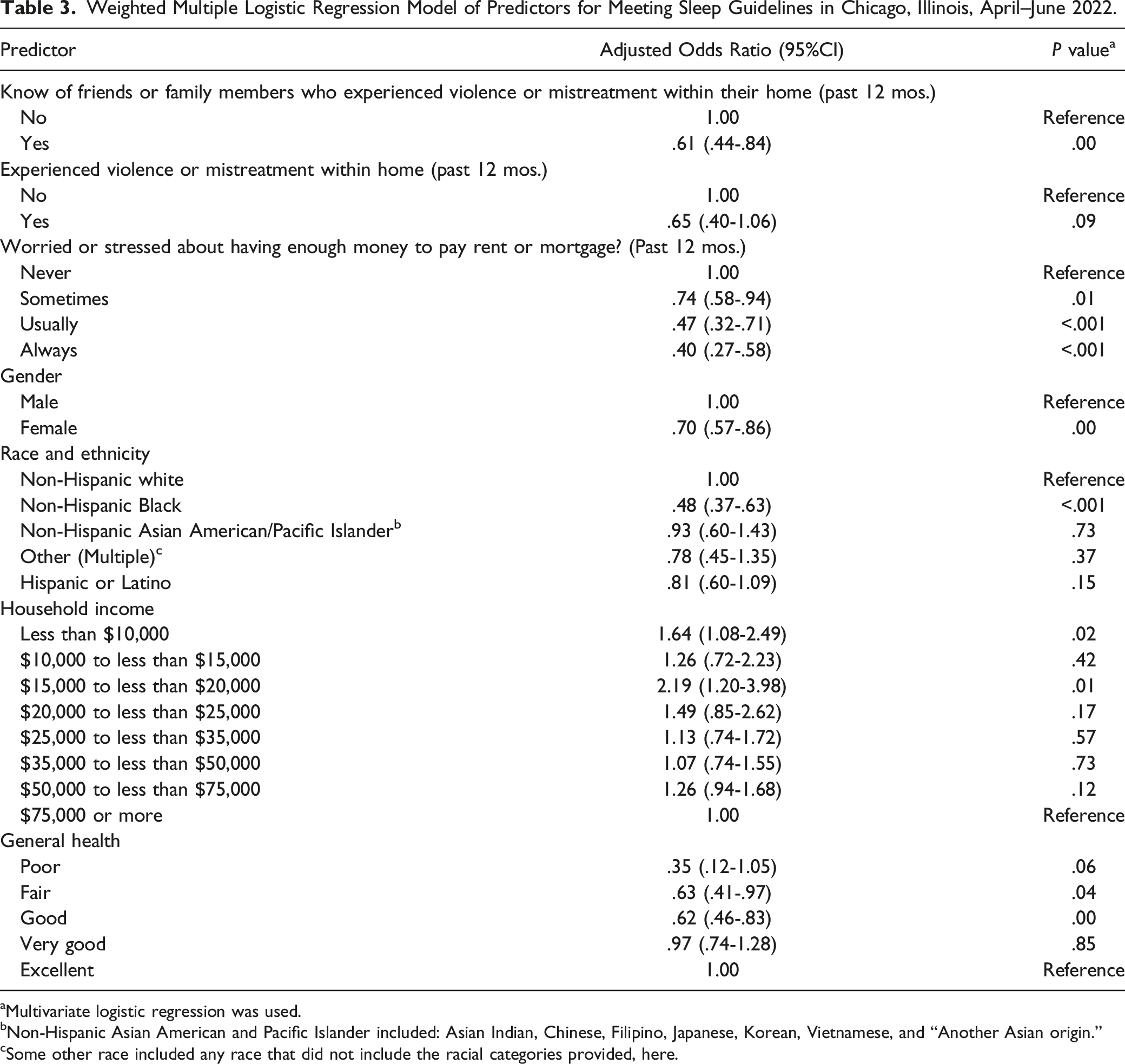
aMultivariate logistic regression was used.
bNon-Hispanic Asian American and Pacific Islander included: Asian Indian, Chinese, Filipino, Japanese, Korean, Vietnamese, and “Another Asian origin.”
cSome other race included any race that did not include the racial categories provided, here.
Discussion
The aim of this study was to examine the effects of neighborhood violence and domestic violence on meeting the national sleep recommendation, following the COVID-19 stay-at-home order. Although respondents who were exposed to neighborhood violence had a lower odds of meeting sleep recommendations, this relationship was not statistically significant in the full model with all predictors. In terms of domestic violence exposure, results showed that knowing a friend or family member who experienced violence or mistreatment in their home affected the odds of meeting the sleep recommendation in the full model.
A recent review study that examined the link between intimate partner violence victimization and sleep disturbances found a relationship in all 23 studies that were reviewed. 18 In the present study, it was surprising that domestic violence victimization did not meaningfully reduce the odds of meeting sleep recommendations when added into regression model 2 (knowledge of domestic violence and sleep). One explanation for this could be insufficient statistical power to detect an effect given the low percentage of the sample that reported experiencing domestic violence within the home (5.4%). Our results align with previous studies that document the effects of domestic violence on sleep across a variety of contexts. One such study examined a large sample of young adults from 25 countries. Respondents from the Americas who had experienced intimate partner violence had 34% higher odds of short sleep (average sleep duration ≤6 h), which is generally comparable to the results of our study. 20 In another recent study that examined domestic violence and sleep, respondents sampled from Chicago who had witnessed domestic violence anytime in their lives had 43% lower odds of meeting sleep recommendations (an average sleep duration ≥7 h). 21
Results from this study also show that compared to non-Hispanic Whites, non-Hispanic Blacks had 41% lower odds of meeting sleep recommendations. The present study showed a stronger, significant effect among non-Hispanic Blacks who knew of domestic violence among friends or family having 52% lower odds of meeting sleep recommendations. Further, no other racial/ethnic group that knew of domestic violence among friends or family were significantly less likely to meet the sleep recommendation. It is important to note that a confluence of factors may have affected sleep among Black respondents during and after the stay-at-home order, including social determinants such as excess exposure to COVID-19, crowded housing, and inequities in healthcare. 22 Regardless of the precise contribution of these social determinants during the COVID-19 pandemic, the present study documents exposure to domestic violence as an important risk factor for non-Hispanic Blacks not getting adequate sleep. This has the potential of putting them at risk of developing chronic conditions such as heart disease, which may contribute to population-level Black-White health disparities. 23
This study had several strengths and limitations. In terms of strengths, this study used a self-administered address-based sampling design known to have good coverage properties and the ability to target lower-level geographies. The response rate for this follow-up survey was high (68.4%) and data were weighted to closely match population distributions, enabling inferences to be made across a large urban population. The survey enabled participation in two modes (web and paper) and in two languages (English and Spanish). Further, this survey was administered following the COVID-19 stay-at-home order in Illinois and it documents important health harms that emerged from the pandemic. In terms of limitations, the cross-sectional design of this study does not allow for causal inference. Respondents to recent self-administered versions of the HCS are more likely to be female, Non-Hispanic White, and higher educated than in interviewer-administered telephone versions prior to 2020. 24 Weighting procedures may not completely account for these discrepancies or for survey non-consent and non-response correlated with variables analyzed in the present study. Although self-reported sleep measures are often used on population-based surveys such as the Behavior Risk Factor Surveillance Survey, average sleep duration was self-reported at a point-in-time and other aspects of sleep, such as sleep quality, were not measured. In addition to this, the dependent variables related to violence are self-reported and a measure of intensity of exposure and victimization, was not incorporated. Additionally, the race and ethnicity variable reduced diverse racial and ethnic groups to broad categories (e.g., “Latino” and “Other”). Among the present sample, counts within some racial and ethnic categories were small and may not fully reflect the overall diversity in Chicago. Future research should examine additional health behaviors that may have been affected by COVID-19, that could impact sleep quality such as alcohol use and physical activity. Specific to sleep, the causal mechanisms between exposure to violence and its effects on sleep, should be examined. This may be accomplished with a longitudinal study that follows participants over time.
This study adds to previous research that has identified a link between domestic violence and sleep. The present study examined this relationship during a consequential time for public health – coming out of the stay-at-home order in response to COVID-19. The results of this study highlight the importance of addressing the harms that emerged from increased risk factors for violence during the COVID-19 pandemic. This involves treating the trauma for those who are exposed to domestic violence and using evidence-based practices to prevent it before it occurs.25,26 There are also several types of behavior change interventions, including structured routines and mind-body exercises such as yoga, to address sleep issues on the individual level. 27 Researchers have called for more training among health service providers, to assure that they can assess and treat sleep disorders; this would be a critical support for those whose sleep has been disrupted by knowledge of domestic violence among friends and family.28,29 Within neighborhoods, interventions that include improvements to urban planning and neighborhood safety have been identified as approaches to address racial sleep disparities. 29 The dissemination of these interventions and improvements to health services are important even for people that were not directly affected by violence during the pandemic, as ensuring an adequate amount of sleep is a Healthy People 2030 objective for the nation. 17
Interpersonal violence burdens the mental and physical health of the population. Increases in community and domestic violence were associated with the odds of being less likely to meet sleep recommendations – a harm that can lead to chronic diseases that range from diabetes to heart disease. Addressing the disruptions to sleep that followed the COVID-19 pandemic would involve contributions from health providers in diagnosing and treating sleep problems, from public health practitioners in preventing and addressing violence that disrupts sleep, and for local leaders in ensuring equitable built environments. Compared to non-Hispanic Whites, non-Hispanic Blacks had lower odds of meeting sleep recommendations. Therefore, promoting sleep recommendations may also be an important step in addressing racial health disparities. Exposure to violence can harm sleep – an important health behavior – that in deficit, is linked to chronic diseases such as diabetes and heart disease. This report documents how knowledge of domestic violence disrupted sleep, following the COVID-19 stay-at-home order. It also documents a racial health disparity in sleep disruption following COVID-19 – compared to Non-Hispanic Whites, Non-Hispanic Blacks with knowledge of domestic violence had significantly lower odds of meeting sleep recommendations. Addressing the harms to sleep that followed the COVID-19 stay-at-home order should engage diverse stakeholders – including health providers, public health practitioners, and local leaders – in implementing culturally responsive interventions and developing built environments to promote healthy sleep and prevent chronic disease.So What?
What is Already Known on this Topic?
What Does this Article Add?
What are the Implications for Health Promotion Practice or Research?
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Chicago Department of Public Health/RTI International. The views expressed are those of the authors and do not represent those of the Chicago Department of Public Health or RTI International.
Corrections (November 2023):
This article was updated to correct the article type to Quantitative Research.