
Abstract
Objective
This systematic review aimed to evaluate the effects of Tai Chi on the health-related quality of life (HRQoL) of people with neurodegenerative diseases.
Data Source
This review followed the guidelines of the updated PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) 2020. A systematic search in five electronic databases (Medline via PubMed, Web of Science, Scopus, PEDro, and OTseeker) was performed.
Study Inclusion and Exclusion Criteria
Randomized control trials (RCTs) examining Tai Chi interventions to improve HRQoL in patients with neurodegenerative diseases published through March 2023 were included.
Data Extraction
Data were extracted from each study by two independent researchers into a data extraction form based on the Cochrane recommendations. Methodological quality and risk of bias were assessed.
Data Synthesis
A meta-analysis was performed using Review Manager 5.3 software.
Results
Of the 439 records that were screened, eight RCTs met the eligibility criteria. They assessed cognitive decline (n = 2) or Parkinson’s disease (n = 6). RCT comparison groups included active interventions or usual care. The duration of Tai Chi therapy ranged from 8 to 24 weeks. A sensitivity analysis using a fixed effect model indicated that Tai Chi therapy significantly increased HRQoL [P < 001, SMD (95% CI) = .41 [.21, .60], I2 = 4%].
Conclusion
Tai Chi can effectively improve the HRQoL of people with neurodegenerative diseases, but the heterogeneity across intervention was relatively high. Further studies are needed as research into the benefits of Tai Chi in neurodegenerative disease rehabilitation is still limited.
Keywords
Objective
Neurodegenerative disease is an umbrella term for diseases characterized by progressive impairment and the loss of neurons and axons in the central nervous system causing a heterogeneous group of neurodegenerative disorders.1,2 These neurodegenerative diseases are chronic disease states that can be classified as Alzheimer’s disease, amyotrophic lateral sclerosis, multiple sclerosis, motor neuron disease, Parkinson’s disease, spinocerebellar ataxia, or spinocerebellar atrophy. Each of these diseases manifests and progresses differently. However, all neurodegenerative diseases have some common features – they are progressive, disabling, and result in a variety of functional impairments, such as cognitive impairment, motor dysfunction, and loss of independence. Absolute patient numbers have considerably climbed over the past 30 years. Moreover, the burden of chronic neurodegenerative diseases is expected to at least double over the next two decades. Due to this evolution, which can largely be attributed to the expansion of the ageing population, the number of people diagnosed with chronic neurodegenerative diseases has increased.2-4 People with such diseases have multiple symptoms due to the degeneration, which may affect their daily activities (eg, work capability, socialization with others, walking). This in turn decreases patients’ health-related quality of life (HRQoL). Despite the tremendous efforts of the scientific and clinical community, no effective therapeutic therapies are available to stop, cure, or reverse the progression of neurodegenerative diseases. 5 Along with pharmacological therapy, strategies that include non-pharmacological therapies need to be explored and implemented to better cope with the growing incidence of these neurodegenerative diseases. These non-pharmacological strategies are a crucial support in the treatment of neurodegenerative disorders.
Tai Chi is a type of non-pharmacological therapy that shows similarities with aerobic exercise. It includes relaxation, deep and regulated breathing techniques, and rhythmic movement. 6 It is now used as a form of movement to improve body awareness and balance.7,8 Tai Chi plays an important role in health promotion and its positive effect has been widely reported among patients with chronic conditions. It has therapeutic value given its beneficial effects on cardiorespiratory and musculoskeletal function, which contribute to health promotion, rehabilitation, and maintenance of mental and physical state in chronic, connective tissue, circulatory, and nervous system diseases.9-11 A recent systematic review exploring the safety and effectiveness of Tai Chi analysed a total of 210 systematic reviews (with no meta-analysis) of controlled clinical trials. Its conclusion suggests that Tai Chi has multidimensional effects, including physical and psychological benefits for a wide range of conditions, as well as multimorbidity. 12 Although the systematic review reported the beneficial effects of Tai Chi on several aspects, the studies reviewed including diverse neurological conditions. Despite existing literature exploring the effects of Tai Chi, there were gaps in the evidence provided in the systematic review. Tai Chi may have great clinical relevance for improving several aspects of patients such as the HRQoL. However, the literature only summarized some aspects of the effectiveness of Tai Chi on neurodegenerative diseases. Comprehensive and clear interpretation of the benefits on HRQoL of Tai Chi as a therapeutic strategy in this population is relevant and crucial.
HRQoL is a significant concept and target for research and practice in the fields of health and rehabilitation. The term HRQoL refers to the health aspects of quality of life, generally considered to reflect the impact of disease and treatment on disability and daily functioning; it has also been well thought-out to reflect the impact of perceived health on an individuals’ ability to live a fulfilling life. 13 More specifically, HRQoL is a measure of the value assigned to duration of life as modified by impairments, functional states, opportunities, and perceptions and as influenced by disease, injury, rehabilitation treatment, and policy.14,15 The 36-Item Short-Form Health Survey (SF-36) is one of the most frequently used instruments to evaluate HRQoL among individuals with neurodegenerative diseases. However, it should be considered that in certain populations there are specific questionnaires to assess HRQoL. For example, in Parkinson’s disease, which is the second most frequent neurodegenerative disease, the Parkinson’s Disease Questionnaire-39 (PDQ-39) is the most widely used instrument to evaluate HRQoL. HRQoL reflects how well a patient functions in their life and their perceived well-being in the physical, mental, and social domains. The aim of this systematic review was to evaluate the effects of Tai Chi on the HRQoL of people with neurodegenerative diseases.
Methods
Data Sources
This systematic review and meta-analysis was undertaken in accordance with the updated PRISMA (Preferred Reporting Items for Systematic reviews and Meta-Analyses) guidelines. 16 It was registered in the PROSPERO database (ID: CRD42023396382) and is available online.
Electronic literature searches were conducted in various electronic databases: Medline (via PubMed), Web of Science, Scopus, PEDro, and OTseeker from their inception to March 2023. The search was conducted by means of the thesauri and the search in Title/Abstract/Keywords when it was possible, using terms related to the population of interest and others related to the intervention. When searched databases allowed limits, searches were restricted to human beings, randomized control trials (RCTs), and English, French, Italian, or Spanish languages. We also screened the reference lists of the potentially eligible articles identified in database searches. An example of the search strategy is available in Supplemental Appendix 1. The electronic search was supplemented with a manual review of reference lists from relevant publications to locate additional publications. Grey literature (eg, abstracts, conference proceedings, or editorials) was excluded. We established our research question following the PICOS (Population, Intervention, Comparison, Outcome measures and Study design) recommendations.
17
- Population: adults diagnosed with a neurodegenerative disease - Intervention: Tai Chi - Comparison: no intervention, standard treatment, usual care, interventions without Tai Chi, placebo, or control - Outcomes: HRQoL - Study design: RCTs
Inclusion and Exclusion Criteria
The inclusion criteria established for this systematic review were RCTs, articles written in English, French, Italian or Spanish, analysing the effects of Tai Chi on the HRQoL of patients with a neurodegenerative disease. All interventions applying Tai Chi were included, regardless of dose and frequency. HRQoL had to be measured using general or pathology-specific instruments. Participants had to be adults over 18 years of age with a diagnosis of neurodegenerative disease. No exclusion criteria were applied regarding aetiology, severity, gender, ethnicity, disease progression, or sequelae. Studies that combined Tai Chi with other interventions such as dance where Tai Chi could not be assessed separately were excluded.
Data Extraction
The data extraction process review was completed following the steps established by the updated PRISMA recommendations. 16 Two reviewers independently screened the title and abstracts to ascertain relevance to the topic. The full text of all potentially relevant articles was read.
Data extraction followed the PICOS recommendations to design systematic reviews. 17 Two reviewers independently extracted data from the studies included. Information was obtained about the objectives, number and age of participants, population group, intervention (intensity, duration, and frequency), and instrument to evaluate HRQoL. Data were collected using a standardized data extraction sheet. Disagreements between the two reviewers were resolved by a third reviewer. If the required data were not published, they were obtained from the study authors whenever possible.
Data Synthesis
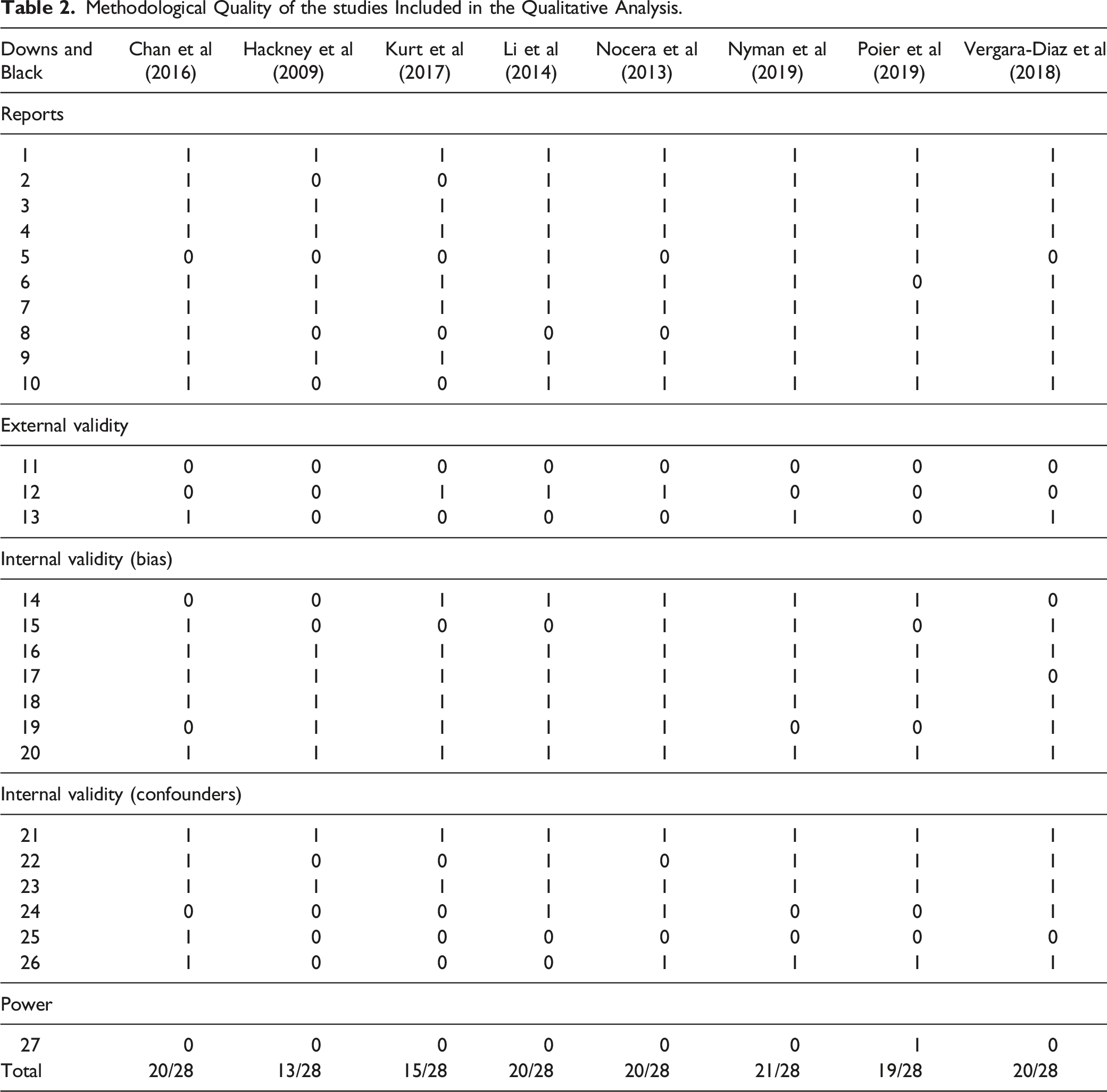
Reviewers performed a methodological quality assessment using the Downs and Black 18 Scale. This instrument consists of 27 questions relating to quality of reporting (ten questions), external validity (three questions), internal validity (bias and confounding; 13 questions), and statistical power (one question). The original scale provides a total score out of 32 points, with one question in the reporting section carrying a possible two points, and the statistical power question carrying a possible five points. In line with previous studies, a modified version was used by simplifying the power question. A modified version of the Downs and Black Scale was used in line with previous studies. 19 The modified version has a maximum score of 28 points. Each paper was assigned a grade of “excellent” (24-28 points), “good” (19-23 points), “fair” (14-18 points), or “poor” (<14 points).
Risk of bias was assessed with version 2 of the Cochrane risk-of-bias tool for RCTs (RoB 2). This tool is divided into a fixed set of domains of bias, focusing on different aspects of trial design, conduct, and reporting, A proposed judgment about the risk of bias arising from each domain is generated by an algorithm, based on answers to the signalling questions. The judgment can be “low” of “high” risk of bias, or can express “some concerns”.
Where appropriate, study results were pooled and a meta-analysis was undertaken using Review Manager software (RevMan v5.3; Cochrane Collaboration, Oxford, UK). All variables included were continuous data. Study authors were contacted by email whenever data were insufficient for the purposes of the meta-analysis (eg, neither means nor standard deviations were provided). If they had not responded within a week, a reminder was sent. Authors were given two weeks to answer. The main outcome considered for this meta-analysis was quality of life. Standardized mean differences (SMD) were used because all scales were assumed to measure the same underlying symptom or condition, but some studies measured outcomes on different scales and 95% confidence intervals (CI) were calculated for all outcomes. The scoring of the different scales was converted so that a higher score always indicated a better outcome.
The Q and I2 statistics were calculated to examine statistical heterogeneity, and a visual inspection of the forest plots was also performed to identify outlier studies. The I2 is a statistical value that is interpreted as the percentage of the total variation observed between studies that is due to the difference between them and not to sampling error (i.e., chance). I2 of ≥50%; I2 >25% and <50%; I2 of ≤25% were considered to indicate high, moderate, and low heterogeneity, respectively. When the I2 value was greater than 50%, the meta-analysis was considered heterogeneous and therefore a random effects analysis had to be used. Statistical significance was established as P < .05, which means that the effects differ significantly between the control and intervention groups. We also explored sources of heterogeneity and performed a sensitivity analysis excluding trials with high risk of attrition or detection bias. Forest plots were generated to illustrate the overall effect of interventions.
Results
A total of 439 records were obtained from the search of five databases. After excluding duplicate articles (n = 155), 284 articles entered the next phase, where articles were reviewed in terms of title and abstract. Of these, 262 articles were excluded for not meeting the inclusion criteria. In the last phase, 22 full-text articles were reviewed, and nine of these met the inclusion criteria. Thirteen articles were excluded because they included no Tai Chi intervention (n = 1), did not include HRQoL as an outcome (n = 3), the population was not adequate (n = 3), Tai Chi was combined with another activity in the intervention group (n = 5), or they were written in another language (n = 1). Figure 1 shows the flowchart of the selection process of the studies. Study selection flow diagram.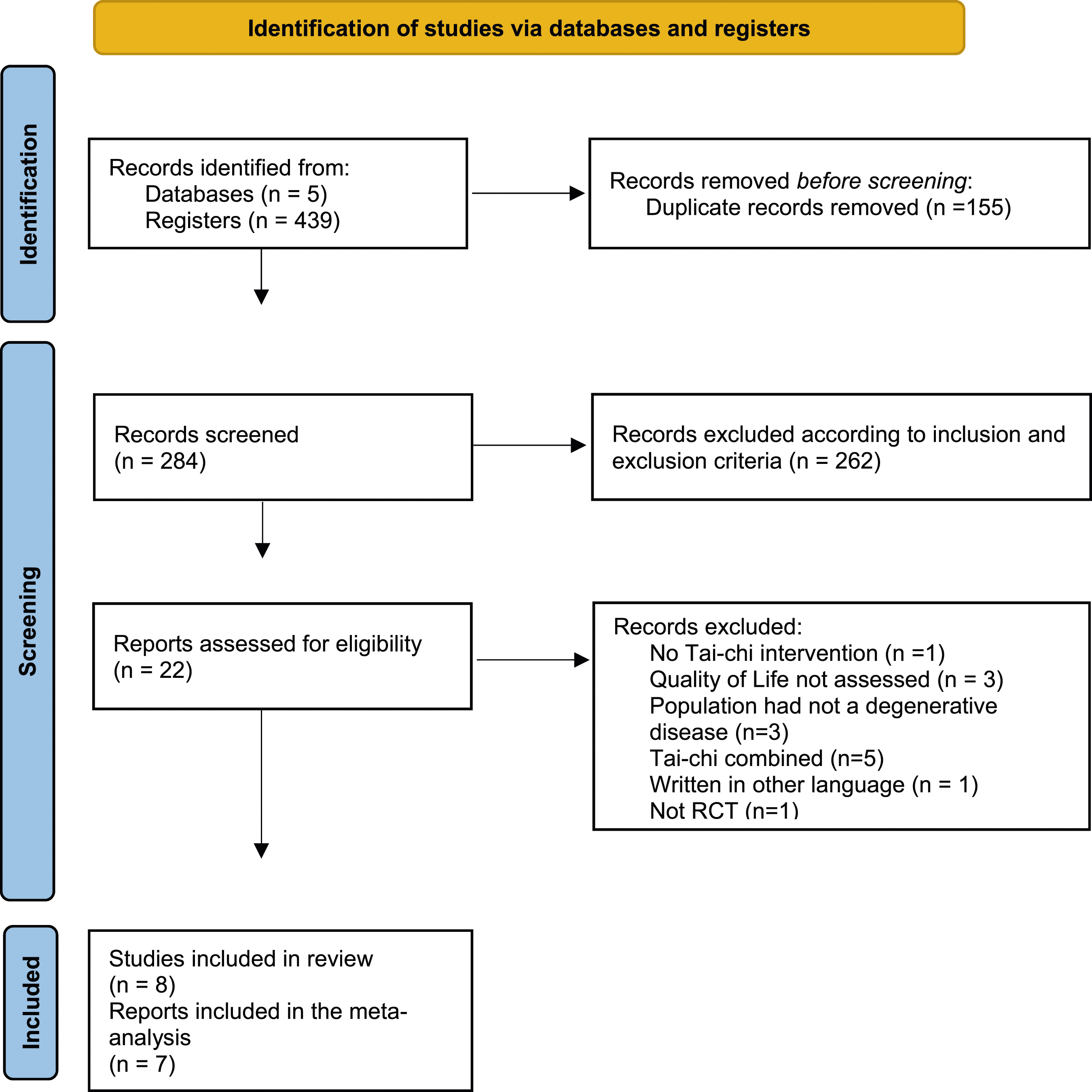
Characteristics of Included Randomized Controlled Trials.
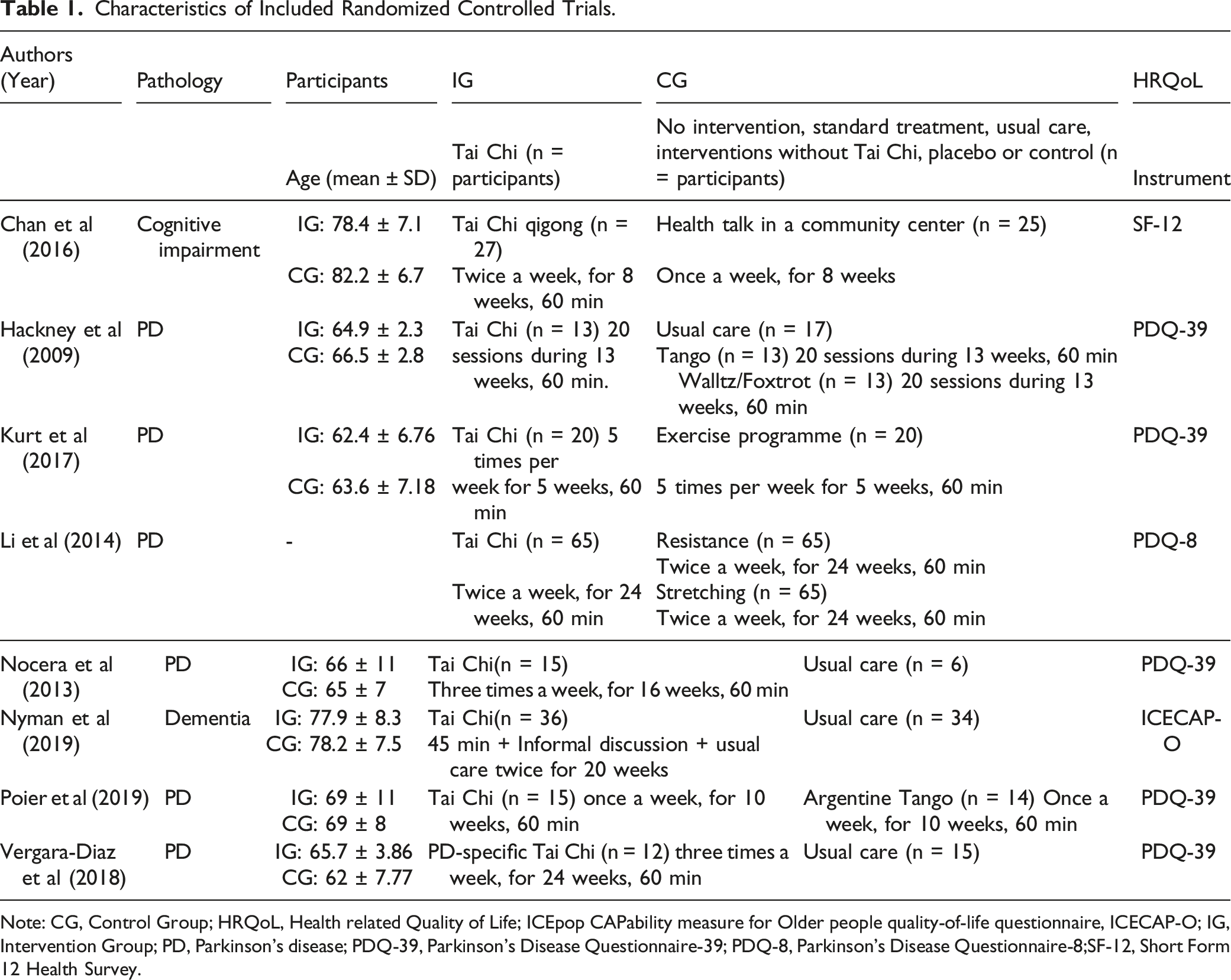
Note: CG, Control Group; HRQoL, Health related Quality of Life; ICEpop CAPability measure for Older people quality-of-life questionnaire, ICECAP-O; IG, Intervention Group; PD, Parkinson’s disease; PDQ-39, Parkinson’s Disease Questionnaire-39; PDQ-8, Parkinson’s Disease Questionnaire-8;SF-12, Short Form 12 Health Survey.
Methodological Quality of the studies Included in the Qualitative Analysis.

Risk of bias summary.
In seven20-24,26,27 of the eight studies, the duration of each session was 60 minutes. The frequency of sessions ranged from 1 26 to 5 times 22 a week for a minimum of 5 weeks 22 and a maximum of 6 months.23,27 Three studies compared Tai Chi intervention with usual care,24,25,27 three studies compared the intervention with other active interventions,22,23,26 one study compared Tai Chi with an education programme in groups, 20 and only one study compared Tai Chi with both usual care and active interventions. 21 No studies reported adverse events or new symptoms that may emerge during the Tai Chi intervention period.
Five studies assessed HRQoL with the Parkinson’s Disease Questionnaire-39 (PDQ-39),21,22,24,26,27 one study used the SF12,
20
one study used the Parkinson’s Disease Questionnaire-8,
23
and one study used the ICEpop CAPability measure for Older people quality-of-life questionnaire (ICECAP-O).
25
Figure 3 shows the results of the meta-analysis. However, data showed that there were no significant improvements and also that there was high heterogeneity between the interventions [SMD (95% CI) = −.50 [-1.14, .15], P = .13, I2 = 91%]. Forest plot for the meta-analysis of the HRQoL.
A sensitivity analysis was conducted in the meta-analysis removing the study by Hackney et al (2009). When this study was removed, results using a fixed effect model showed that, compared to conventional treatment, Tai Chi therapy significantly increased HRQoL [SMD (95% CI) = .41 [.21, .60], P < .0001, I2 = 4%]. Data are presented in Figure 4. Forest plot for the meta-analysis of the HRQoL applied a sensitivity analysis.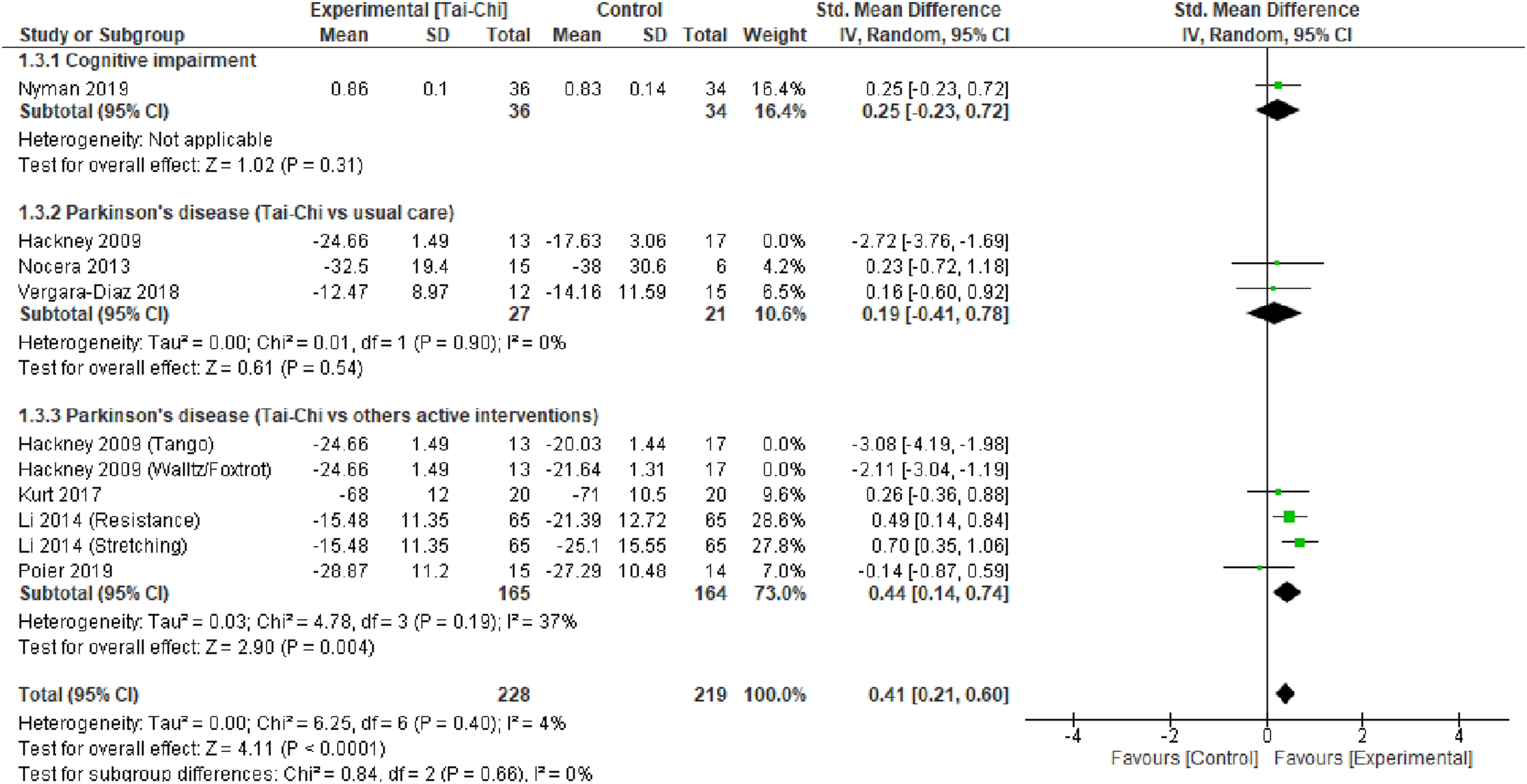
Discussion
The aim of this systematic review was to evaluate the effects of Tai Chi on the HRQoL of people with neurodegenerative diseases. The eight studies included 490 participants. The duration of interventions ranged from eight to 24 weeks with varying forms of Tai Chi practice. All studies reported that the practice had low to moderate intensity with repetitive, flowing, meditative movements that aimed to maintain and cultivate health and HRQoL. Tai Chi was found to be a safe and health-enhancing intervention for people with neurodegenerative diseases.
The consequences of neurodegenerative diseases are rather complicated because the physical and mental disability may influence the psychosocial components of HRQoL. An umbrella review of systematic reviews and meta-analyses of RCTs 28 provided a broad overview of the existing evidence on Tai Chi for 16 types of chronic conditions management. Authors 28 concluded that the benefits of Tai Chi intervention compared with nonactive or active control group on the health outcomes (e.g. gait, balance, emotion or physical function) of patients with chronic conditions such as cancer, cardiopulmonary diseases, chronic pain, mental disorders, musculoskeletal conditions, rheumatoid arthritis, stroke and type 2 diabete in general have been widely proven. Authors described Tai Chi as unique in being multimodal or holistic, blending aerobics, resistance and stretch training. Yet, debates are ongoing regarding its benefits to improve HRQoL among people with neurodegenerative diseases. Tai Chi effectiveness is important as health care is slowly undergoing a paradigm shift in which a biopsychosocial model of care is gaining popularity. This systematic review and meta-analysis evidenced that Tai Chi interventions in a patient’s plan improves HRQoL and can also enhance the individual’s mind, body, and spirit providing an approach focusing on many aspects of the biopsychosocial model.
Tai Chi, a type of low-impact mind-body exercise, has spread worldwide over the past decades. It integrates musculoskeletal conditioning along with training in multiple cognitive skills and breathing regulation. Tai Chi shows great promise for addressing the many physical and psychological morbidities faced by patients with neurodegenerative diseases. 12 In addition, Tai Chi is usually performed in groups, is a popular activity, and has a high acceptability rate among individuals and it provides psychosocial support. In the psychosocial context of neurodegenerative diseases, group interventions may tend to buffer against the negative effects of such diseases on HRQoL of patients. Practising Tai Chi in a group provides a broadened social network, decreases feelings of loneliness, and increases satisfaction due to social support in individuals with chronic conditions.
However, few evidence-based syntheses are available to inform the integration of Tai Chi in patient care. Among the existing literature, previous studies have explored the effect of low impact mind-body exercise such as Tai Chi in various neurodegenerative diseases such as Alzheimer’s disease, 29 Parkinson’s disease, 30 or multiple sclerosis. 31 Wang et al 32 (2022) conducted a systematic review (with no meta-analysis) including different types of studies such as systematic reviews, meta-analyses, and clinical trials only published in English to summarize the protective effects of Tai Chi for motor function, cognition, quality of life, and mood in patients with neurodegenerative diseases. The authors concluded that Tai Chi therapy can effectively improve the motor function, global cognitive function, and falls in patients with neurodegenerative disease, but that more studies are need regarding HRQoL. This systematic review with meta-analysis addresses a relevant gap about the effects of Tai Chi regarding HRQoL in people with neurodegenerative diseases. Although the safety of Tai Chi in most RCTs included was not systematically assessed or reported, no serious adverse events were cited in any studies. This finding, along with other more comprehensive reviews of adverse events reported in RCTs,33,34 suggests that Tai Chi is likely to be adequate and safe for patients with neurodegenerative diseases.
It is relevant highlight that Tai Chi is a complete philosophy to improve body awareness and balance. However, most studies did not report an explicitly described Tai Chi protocol, especially Tai Chi style, intensity, instruction methods, and the progression of the Tai Chi program.
Tai Chi principles, stances, philosophy, flexibility and its measurement, and the measurement of mind were not mentioned in any of the enrolled trials. In the current study, the intensity of Tai Chi for each trial was not be able to calculate to examine dose intensity effects due to the lack of intensity information. The complete descriptions of each component of Tai Chi intervention are needed for future research to fully investigate the dose-response effects.
The length of Tai Chi intervention varied from five to 24 weeks in this systematic review and meta-analysis. The frequency of intervention was one to five sessions weekly. The most reported frequency of intervention was two sessions weekly. The Tai Chi sessions varied in length from 15 to 60 minutes. Most studies had 60 minutes sessions.
This systematic review and meta-analysis summarizes and updates the results of the effects of Tai Chi therapy on HRQoL among people with neurodegenerative diseases. To our knowledge, this is the first study to conduct a meta-analysis analysing the effects of Tai Chi on HRQoL in this population using only RCTs. The results obtained are relevant and provide evidence of the effect of Tai Chi on HRQoL. Like many other neurological diseases, the burden of the neurodegenerative disease is increasingly appreciated as a complex biopsychosocial condition. 12 The biopsychosocial framework emphasises that physical, psychological, and social dimensions of health and their optimal care are often highly interdependent. 35 This perspective supports a potentially unique role for holistic mind-body therapeutic approaches that target multiple physical and psychosocial aspects of symptomatology, and that may offer patients a flexible toolset for addressing their experience of the disease.
Strengths and Limitations
The present study also had strengths and several limitations. The first limitation is language, as only articles in English, French, Italian and Spanish were included. Several articles on this topic were published in Chinese, a language not included. The second limitation is that only RCTs were included in this systematic review and meta-analysis; these RCTs showed moderate risk of bias due to the lack of blinding, low sample size, and the absence of a deeply detailed intervention protocol. Overall, our findings and the results of the meta-analysis results provide evidence that Tai Chi significantly improves HRQoL in patients with neurodegenerative diseases. Tai Chi is a simple, adequate, safe, and easy therapy that can enhance motor, cognitive, and emotional functions. Future studies with a larger number of participants, a high-quality experimental design (i.e., well-designed RCTs, rigorous statistical analysis, specific-disease instruments, a clear description of Tai Chi protocol, and a report of adverse events), and a follow-up should be applied to test the long-term effectiveness of Tai Chi in patients with neurodegenerative diseases.
Conclusion
The evidence shows that Tai Chi improved HRQoL in patients with neurodegenerative diseases when a sensitivity analysis was carried out. In addition, the methodological quality of the studies included was moderate-good. However, a moderate level of risk of bias was found, so the results obtained in this review should be taken with caution. Tai Chi interventions are effective to promote HRQoL in the general population. However, little is known about whether Tai Chi can improve HRQoL in people with neurodegenerative diseases. This manuscript supports the idea that Tai Chi intervention improves HRQoL among people with neurodegenerative diseases. Then, Tai Chi is potentially an acceptable and feasible intervention to be integrated into the primary health care for promotion for the neurodegenerative disease. However, the Tai Chi intervention content and dose varied significantly among studies, and most of the Tai Chi intervention development processes are not properly described. This manuscript provides the best existing evidence to health practitioners that Tai Chi is a health-enhancing and safe therapeutic approach to improve HRQoL in people with neurodegenerative diseases. Therefore, health practitioners can safely include Tai Chi in their interventions. However, there is a need for more RCTs describing their protocols in detail.So What?
What is Already Known on this Topic?
What does this Article Add?
What are the Implications for Health Practitioners or Research?
Supplemental Material
Supplemental Material - Effects of Tai-Chi on Quality of Life in People With Neurodegenerative Diseases. A systematic Review of Randomised Clinical Trials
Supplemental Material for Effects of Tai-Chi on Quality of Life in People With Neurodegenerative Diseases. A systematic Review of Randomised Clinical Trials by Alba Navas-Otero, Alicia Pineda-Nogueras, Araceli Ortiz Rubio, Andrés Calvache Mateo, Irene Torres-Sánchez, Marie Carmen Valenza, and María Granados-Santiago in American Journal of Health Promotion
Footnotes
Author’s Note
The data is based on Suelo Pélvico Córdoba, Calle Manuel Fuentes Bocanegra, 2 Córdoba, Spain.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Systematic Review Registration Number
PROSPERO (CRD42023396382).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.