
Abstract
Purpose
Weight concern is a barrier to smoking cessation. We examined the impact of weight concern on post-cessation weight gain, abstinence and program engagement.
Design
Randomized-controlled trial.
Setting
Telephone-based and group-based intervention sessions.
Subjects
305 participants were randomized and analyzed.
Intervention
Participants were randomized to receive a self-guided intervention, a weight loss intervention, or a weight stability intervention prior to all receiving the same smoking cessation intervention.
Measures
Level of weight concern on three measures, point-prevalence abstinence, weight change, and session attendance at 12 months.
Analysis
Continuous and discrete outcomes were compared between weight-concerned and non-weight-concerned participants using two-sample t-tests and chi-square tests respectively.
Results
There were no significant differences in weight change (range: +1.77, −1.91 kg) when comparing weight-concerned and non-weight-concerned participants. Point-prevalence abstinence ranged from 36% to 64%, with no differences by condition based on level of weight concern. There were no significant differences in session attendance by weight concern (Weight sessions: 50–70%, Smoking cessation sessions: 41–56%, Booster sessions: 28–45%). Weight concern, on all measures, significantly decreased between screening and 2 months (after the weight management intervention), for most of the comparisons made overall and by condition.
Conclusion
It may not be necessary to screen for weight concerns in smoking cessation and/or post-cessation weight management programs, as the trial interventions were beneficial regardless of weight concern.
Purpose
Cigarette smoking is associated with cardiovascular, respiratory, neoplastic, and other diseases; moreover, 480,000 deaths annually in the United States are attributable to smoking.1,2 Consequently, benefits of quitting smoking include reduced all-cause mortality from smoking-related diseases.3,4 Despite these benefits, concerns about weight gain have been shown to be a deterrent to quitting, and weight gain is associated with relapse.5,6 This is a concern rooted in reality; 84% of those who quit smoking gain weight, with an average weight gain of 4.67 kilograms within 1 year. 7 Nonetheless, it is still of prime importance for smokers to quit, as reduced mortality from cessation outweighs any mortality risk associated with weight gain.8–10 Since long-term weight maintenance post-cessation is difficult, integrated weight management and smoking cessation programs are needed, perhaps particularly for those individuals with high weight concern.7,11,12 However, research thus far has provided low-certainty evidence that programs can prevent long-term post-cessation weight gain (≥ 12 months) and may even worsen abstinence rates. 13
Post-cessation weight concern is prevalent among smokers (∼60%). 14 Despite being prevalent among both men and women, weight concern rates are higher in women than in men.15,16 Women with weight concern are also generally younger, 17 and are more likely to identify as White.18,19 Previous research on the relationship with body mass index (BMI) category is mixed, with one study indicating that individuals with lower BMIs have more weight concern 17 and other research finding that individuals with higher BMIs have more weight concern. 20 Consideration of weight concern may be critical because, previous research has shown higher weight concern levels to be associated with shorter quit attempts, less cessation treatment-seeking, increased perceived difficulty in smoking cessation, and increased relapse in quitters who gain weight.5,21,22 Weight concern is also associated with heightened beliefs about efficacy of smoking as a weight control strategy. 23
In addition to modulating smoking beliefs/behaviors, weight concerns may influence quitters’ post-cessation weight-related outcomes. One smoking cessation/weight gain prevention intervention in women found pre-treatment weight concern positively predicted short-term post-cessation weight gain. 24 Another trial where participants only received smoking cessation treatment found increased weight concern predicted higher weight gain at post-treatment. 11 Nonetheless, little is known about engagement levels in weight management programs among people who have differing levels of weight concern.
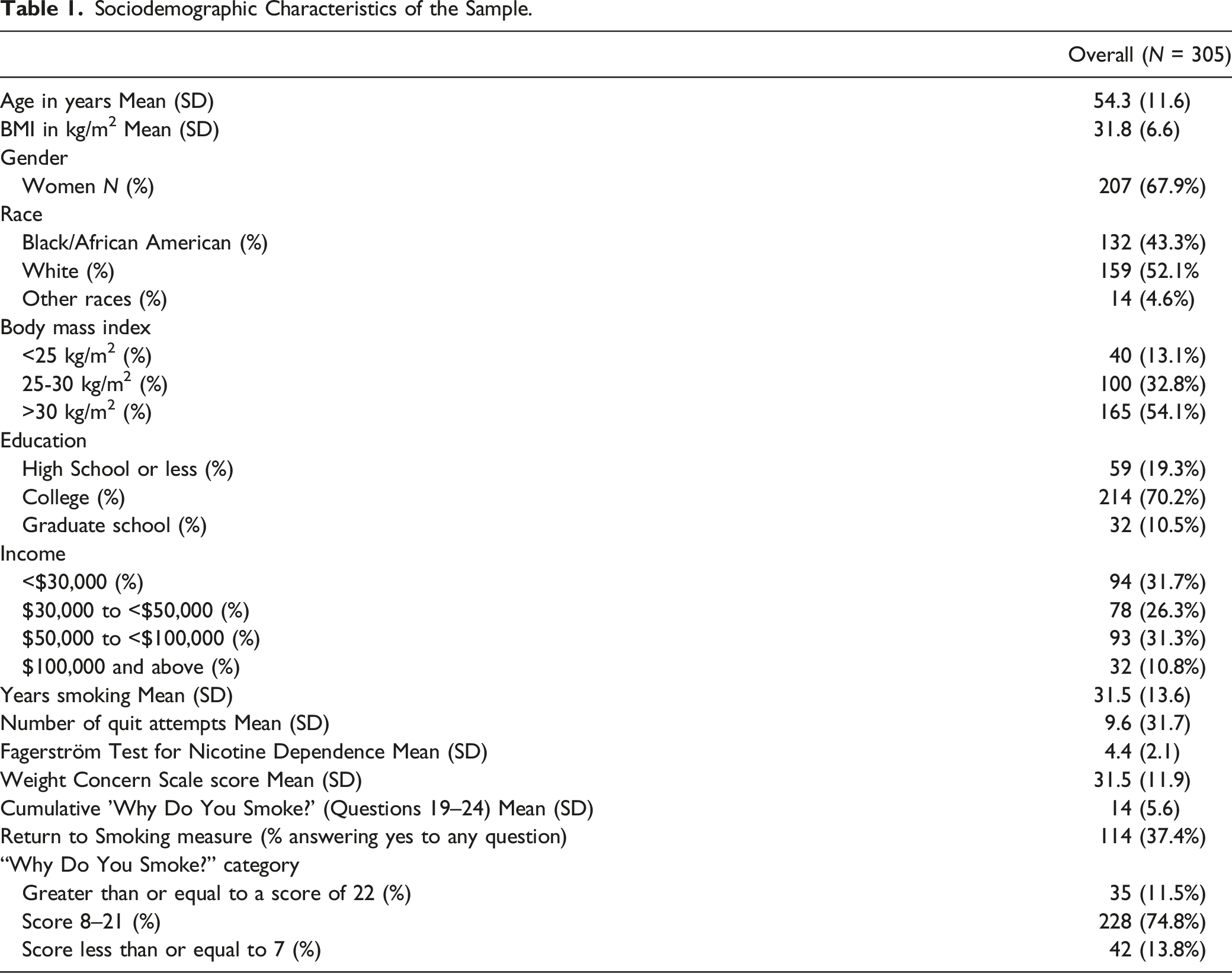
Thus, in this study, we investigate the influence of weight concern on weight-related and cessation outcomes for participants enrolled in a combined smoking cessation and weight management program, with three hypotheses: (1) Weight-concerned participants will gain more weight compared to those without weight concern, (2) Weight-concerned smokers will achieve lower abstinence rates than their non-weight-concerned counterparts, and (3) Participants with weight concern will have less engagement with smoking cessation components (e.g., session attendance) and greater engagement with weight management components (e.g., session attendance). Finally, since previous investigations into smoking cessation related weight concern have been mostly homogenous (i.e., predominantly women, and people identifying as White), we explore these relationships in a more diverse sample (i.e., 32.1% identifying as men, 43.3% identifying as Black/African American).
Methods
Design
These secondary analyses related to the influence of weight concern on weight and cessation outcomes as well as treatment engagement were conducted using data from a randomized, controlled trial designed to assess the efficacy of post-cessation weight gain prevention interventions; the main outcomes of weight change and point-prevalence abstinence from this trial are described elsewhere. 25 Briefly, 305 participants were randomized to receive a self-guided weight management intervention (Bibliotherapy, n = 86), weight loss intervention (Loss, n = 110), or a weight stability intervention (Stability, n = 109) for 2 months. All participants also received the same smoking cessation intervention and varenicline (Chantix™) pharmacotherapy for 6 months. Overall, 11% of participants had missing outcome data at 12 months with no differential attrition between conditions (Bibiliotherapy, n = 77; Stability, n = 94; Loss, n = 101). Results indicated the Loss intervention led to significantly lower post-smoking cessation weight gain (−2.01 kg, SE = 1.58) over 12 months compared to the Bibliotherapy intervention (+1.08 kg, SE = 1.49, P = .0004). The Stability group, on average, experienced weight stability (−.30 kg, SE = 1.56) and the Bibliotherapy group experienced less weight gain than anticipated, with no significant differences in weight change between these conditions (P = .17). The University of Tennessee Health Science Center Institutional Review Board approved the study procedures.
Sample
Detailed inclusion/exclusion criteria were described previously. 26 Briefly, inclusion criteria were: smoking ≥ 5 cigarettes daily, ≥18 years old, a BMI ≥ 22 kg/m2, willingness to use phone/email for intervention components, and ability to exercise for ≥ 10 min daily. Exclusion criteria were: those who may have been unable to actively and safely participate in study activities (e.g., varenicline hypersensitivity; current suicidal ideation or eating disorder; unstable cardiovascular disease; pregnancy; breastfeeding), or had recent participation in another smoking cessation or weight management intervention.
Recruitment strategies included postcards, medical referrals, radio advertising, Facebook advertising, and institution emails, as described elsewhere. 27 Respondents completed a preliminary phone screening (n = 2667), after which eligible individuals participated in a screening visit (conducted in-person before March 2020 and by phone after July 2020) (n = 636). At this visit, individuals were consented, and demographic information, self-report measures, and physical measurements were obtained. If they continued to be interested, they attended a baseline visit where they submitted their 3-day diet and exercise journal and medical clearance letter (n = 314). Approximately 11% of participants who were screened or contacted for participation were eligible and randomized.25,27
Participants were randomized to one of three conditions (Stability, Loss, and Bibliotherapy) by the study biostatistician, using a randomization approach that accounted for participant availability and group size while balancing the groups based on demographic and clinical characteristics. Specifically, first, the days of week that intervention was going to be provided were randomly assigned to an intervention condition. Then, those participants who were available on only one day that intervention was occurring for the given wave were assigned to that intervention/day. Those participants who were available on two or all three days that the intervention was occurring for the given wave were randomized to an intervention while controlling sample size by intervention arm and assuring equal distribution between the groups in regard to age, gender, race/ethnicity and BMI. The original randomization plan goal included 2:2:1 randomization strategy, with fewer in the Bibliotherapy condition. However, due to slow initial recruitment and concern about having groups that were too small in the Bibliotherapy condition, we modified the randomization scheme to be 1:1:1 randomization with the guidance of our Data Safety and Monitoring Board.
Intervention
Weight Management Interventions
Participants were oriented to their condition by their interventionist and received a BodyTrace™ e-scale and group-specific materials. In brief, participants in the Stability intervention had 8 weekly group-based phone sessions focused on strategies for making small behavioral changes in diet and physical activity to keep their weight stable. 28 Participants were provided with feedback via a personalized, color-coded weight trajectory graph (i.e., red, yellow, and green zones) representing how much their weight was over their baseline weight. The Loss intervention aimed to help participants lose 5% of their body weight after 8 weekly group-based phone sessions, through caloric/fat/exercise goals, diet and exercise self-monitoring, and meal replacements. 29 In the first session of the Stability and Loss interventions, there was content about the mechanisms of post-cessation weight gain (e.g., changes in metabolism, eating as a stress management strategy). The Bibliotherapy condition (the control group) received the self-directed weight management program in ‘The EatingWell® Diet’ book, 30 which includes a 7-step program for weight management based on the evidence-based VTrim program31,32 as well as healthy recipes. All participants were encouraged to measure their weight daily using the BodyTrace™ e-scale, which automatically uploaded data daily to a personalized graph for the participant and study staff.
Smoking Cessation Intervention
Immediately after the 2-month weight management period, all participants received a behavioral smoking cessation intervention consisting of 6 sixty-minute group sessions and one individual session over 6 weeks. The first and second group sessions focused on rate reduction and preparing for quitting smoking, the third and fourth group sessions focused on the quitting process and managing the first few days of not smoking, and the fifth and sixth sessions focused on relapse prevention. Participants were encouraged to set a quit date after the second group smoking cessation session. The individual session occurred during the week of the recommended quit date, and this session focused on goal setting and problem solving related to personalized strategies for quitting and staying quit. Additionally, all randomized participants received 6 months of varenicline (Chantix™) as smoking cessation pharmacotherapy.
Booster Sessions
After completing the smoking cessation behavioral intervention, Stability and Loss participants received monthly booster sessions focused on problem solving related to weight management and smoking cessation, with the final booster session occurring approximately 8 months after baseline. At each booster session, the facilitator presented an example challenge related to weight management and smoking cessation, and then led the group through problem solving strategies related to the example challenge. Next, the facilitator solicited recent challenges from group members, and discussed strategies for overcoming these real challenges. These booster sessions focused on problem solving, given previous research indicating that problem solving is more effective than relapse prevention for weight maintenance. 33
Measures
Post-cessation weight concern was assessed using three measures. (This construct may be better described as “weight gain concern” given participants concern about future weight gain due to quitting smoking; however, to be consistent with the previous literature, we used the term “weight concern”.) While all of these measures broadly assess post-cessation weight concern, each of these measures assess a slightly different aspect of weight concern, 34 as described below.
Weight Concern Measures
First, participants completed items 19–24 of the ‘Why Do You Smoke’ questionnaire (5-point scale, range = 6–30), only assessed at the screening visit. This questionnaire assesses the degree to which participants self-report smoking to control their weight, their appetite, and eating in the absence of hunger. Participants with a score ≥22 were classified as having high weight concern, similar to previous research. 35 Cronbach alpha for this measure with the current sample was .81.
The second measure was the 11-item ‘Return to Smoking’ survey assessing the degree of weight gain (i.e., 2 lbs to 20 lbs or more) that would trigger a return to smoking, at both the screening and 2-month visits. Those who indicated they would return to smoking after any weight gain were classified as weight concerned. 17 Cronbach alpha in the current study was .81.
Finally, participants completed the 6-item ‘Weight Concern Scale’, with each item scored on a 10-point scale, at the screening and 2-month visits. This questionnaire assesses importance of maintaining/losing weight, importance and perceived effectiveness smoking to control weight, perceived likelihood of post-cessation weight gain, level of concern about post-cessation weight gain, and perceived likelihood of returning to smoking due to post-cessation weight gain. The ‘Weight Concern Scale’ was examined on a continuous scale, with each participant receiving a score between from 10–60, since there were not clear cut-points for categorizing weight concern.11,34 For comparability to the dichotomous analyses above, we also categorized participants as above or below the 50th percentile of that scale (i.e., median split = 31). Cronbach alpha in this current sample was .78.
Socio-Demographic Characteristics
At screening, participants reported their self-identified race, ethnicity, and gender.
Anthropometrics
At baseline, height was measured in centimeters using wall-mounted stadiometer prior to March 2020, and self-reported during the COVID-19 pandemic. Weight in kilograms was measured with participants on a calibrated digital scale in the research clinic prior to March 2020 and was assessed using the BodyTrace™ e-scale thereafter at baseline, 2 months, 4 months, 8 months and 12-month follow-up visits. Previous research has indicated concordance between e-scale weights and clinic measured weights. 36 The primary outcome was mean weight change from baseline to 12-month follow-up (i.e., 12 months after the baseline visit).
Smoking Status
Smoking status was assessed at 2-, 4-, 8-, and 12-month follow-up visits using self-reported point-prevalence abstinence as a primary outcome (i.e., “if they had smoked a cigarette, even just a puff, in the past seven days”). Smoking status was verified by measuring salivary cotinine levels at follow-up visits (using NicAlertTM prior to the COVID-19 pandemic and iScreenTM after the pandemic started), and high concordance was found with self-reported abstinence. 25
Weight Management Session Attendance
For both the Loss and Stability groups, interventionists monitored participant attendance for 8 weight management sessions and 5 weight booster sessions. Mean percentage of sessions attended within each group was used as a program engagement measure.
Smoking Cessation Session Attendance
For all conditions, interventionists monitored participant attendance at smoking cessation sessions and coded each day as present or absent (range = 0 to 7 sessions). Mean percentage of sessions completed within each condition was also used as program adherence measure.
Analyses
All analyses were performed with SAS/STATv15.2. Descriptive statistics consisted of means and standard deviations for continuous and frequencies and proportions for discrete variables, respectively. Continuous and dichotomized weight concern measures were compared by race, gender and BMI category using two-sample t-test and analysis of variance (ANOVA) and chi-square test, as appropriate. Similarly, continuous (i.e., weight change at 12 months) and discrete outcomes (i.e., abstinence, attendance) were compared between weight-concerned and non-weight-concerned participants by intervention group using a two-sample t-test and chi-square test respectively. These analyses included all participants with complete follow-up data. In addition, we examined the impact of weight concern at screening on the main outcomes (i.e., weight and smoking) using mixed effects regression models by intervention group, including all participants (including those with missing data). The mixed effects regression models adjusted the associations for age, gender, race, and baseline BMI. Changes in weight concern score over time by group was tested using a mixed effects general linear model with between-factor group, within-factor visit and their interaction term, including all available data. Similarly, dichotomous weight concern measures over time by group were analyzed with the same model structure using generalized linear model. All post-hoc multiple comparisons for linear models used Bonferroni adjustment, where applicable. Differences and associations were considered significant at an alpha level of .05.
Results
Participant Characteristics
Sociodemographic Characteristics of the Sample.
Weight Concern by Sociodemographic Factors and BMI Category
Sociodemographic Differences in Weight Concern Scores.
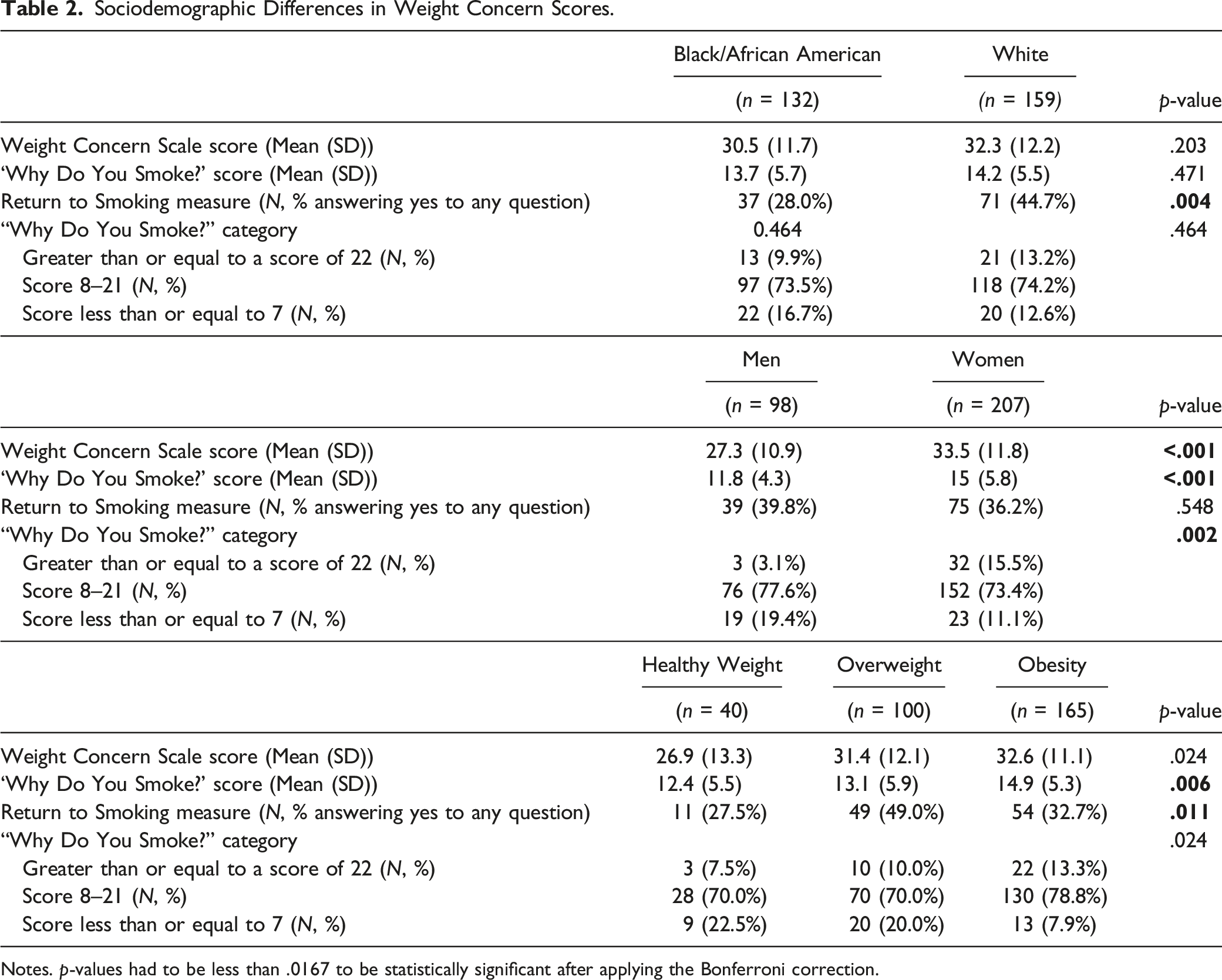
Notes. p-values had to be less than .0167 to be statistically significant after applying the Bonferroni correction.
Women had a higher mean ‘Weight Concern Scale’ score (M(SD) = 33.5 (11.8)) compared to men (M(SD) = 27.3 (10.9)) (t = 4.38; df = 303; p < .0001). Additionally, 15.5% of women were classified as weight concerned with the ‘Why Do You Smoke’ questionnaire compared to 3.1% of men (χ2 = 12.37; df = 2; p = .002). Conversely, a slightly higher proportion of men (39.8%) reported weight concern on the ‘Return to Smoking’ questionnaire than women (36.2%); however, this difference was not significant (Table 2).
Weight-concerned participants were significantly different by BMI, for the ‘Why Do You Smoke’ mean score and the ‘Return to Smoking” measure. According to the ‘Why Do You Smoke’ measure, those with obesity had significantly higher weight concern than those with overweight and healthy weight (Table 2). In addition, proportions of participants with obesity, overweight, and healthy weight who reported they would return to smoking after some weight gains were 32.7%, 49%, and 27.5% respectively, with participants with overweight having significantly higher weight concern than those with obesity (χ2 = 6.94; df = 1; p = .008) and healthy weight (χ2 = 5.39; df = 1; p = .02).
Weight Change
Impact of Weight Concern at Screening on Intervention Engagement and Weight/Smoking Outcomes (Unadjusted Model).
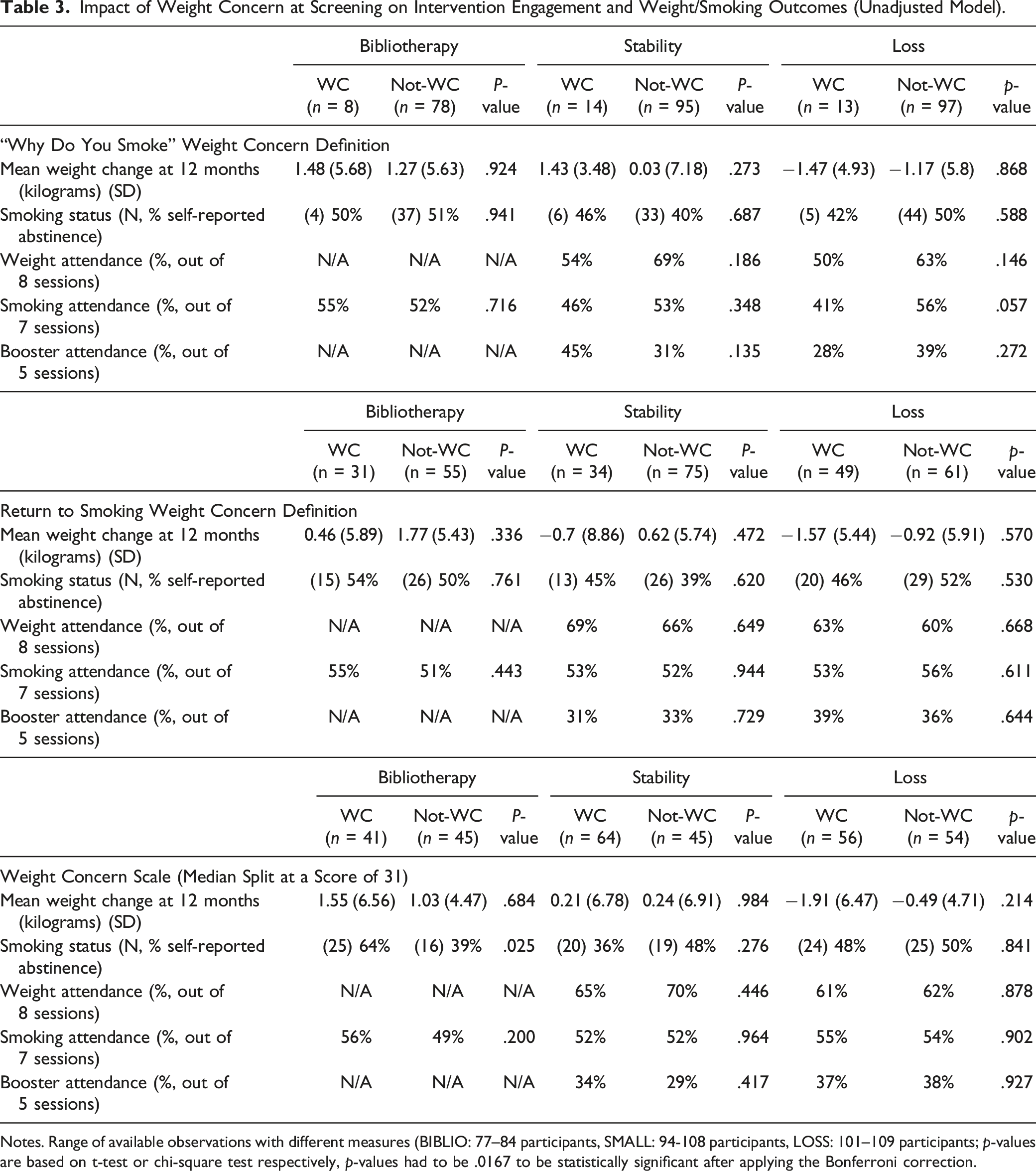
Notes. Range of available observations with different measures (BIBLIO: 77–84 participants, SMALL: 94-108 participants, LOSS: 101–109 participants; p-values are based on t-test or chi-square test respectively, p-values had to be .0167 to be statistically significant after applying the Bonferroni correction.
Impact of Weight Concern at Screening on Weight/Smoking Outcomes (Adjusted Model).
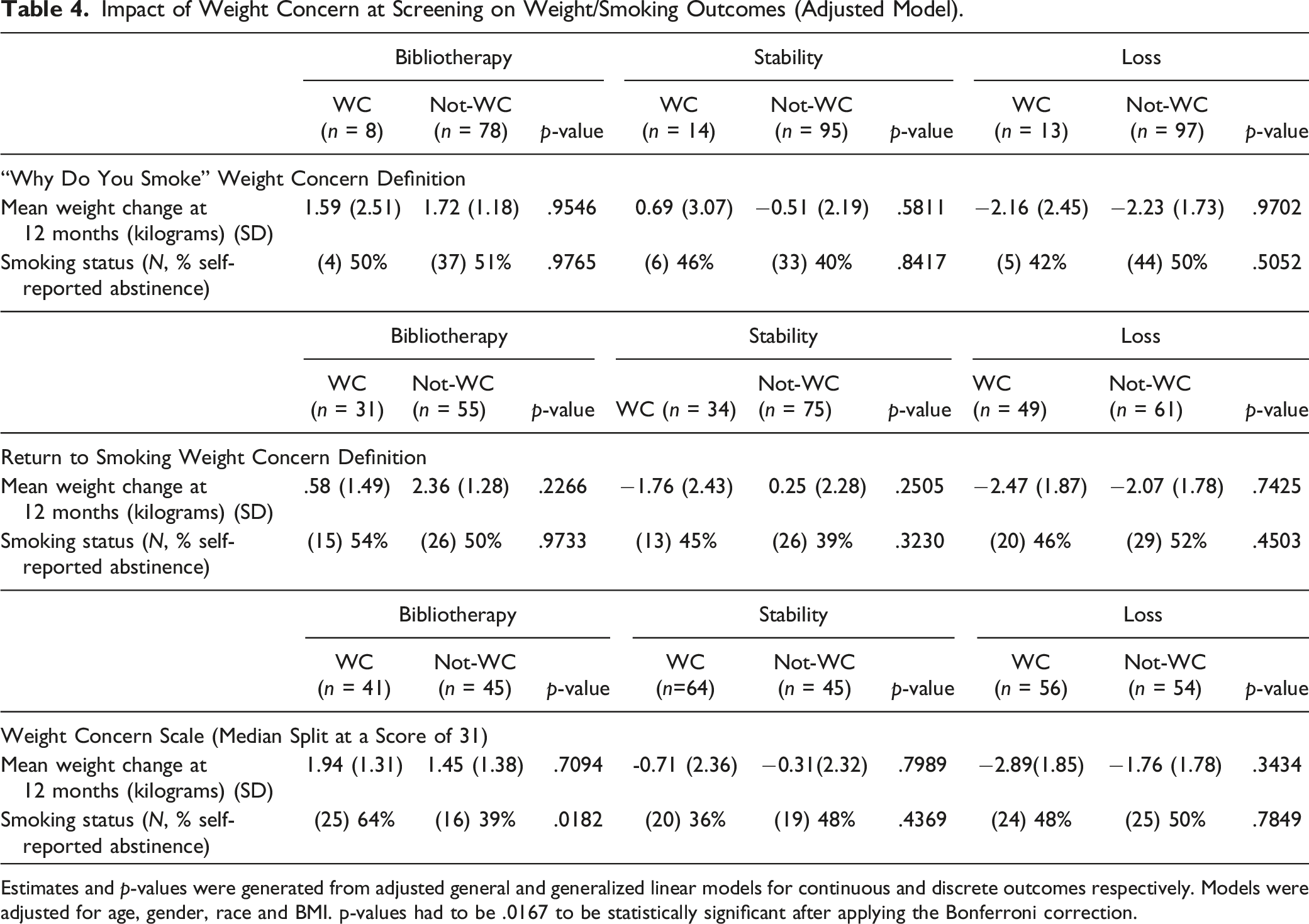
Estimates and p-values were generated from adjusted general and generalized linear models for continuous and discrete outcomes respectively. Models were adjusted for age, gender, race and BMI. p-values had to be .0167 to be statistically significant after applying the Bonferroni correction.
Abstinence
Using the ‘Why Do You Smoke’ and the ‘Return to Smoking’ definitions of weight concern, there were no significant differences in 12-month self-reported smoking status when comparing weight-concerned and non-weight-concerned participants within each of the three intervention groups on any of the measures in the unadjusted (Table 3) and adjusted models (Table 4).
Study Engagement
There were no significant differences in weight session attendance and smoking session attendance, for any of the weight concern measures, when comparing weight-concerned and non-weight-concerned participants within each of the Stability, Loss, and Bibliotherapy groups (Table 3). Overall, 8% of participants received no behavioral smoking cessation sessions, with no significant differences between the assigned conditions in lack of initiation of the behavioral smoking cessation intervention (χ2 = 2.59; df = 2; p = .273).
Change in Weight Concern between Screening and the 2-Month Data Collection Visit (After the Weight Management Intervention).
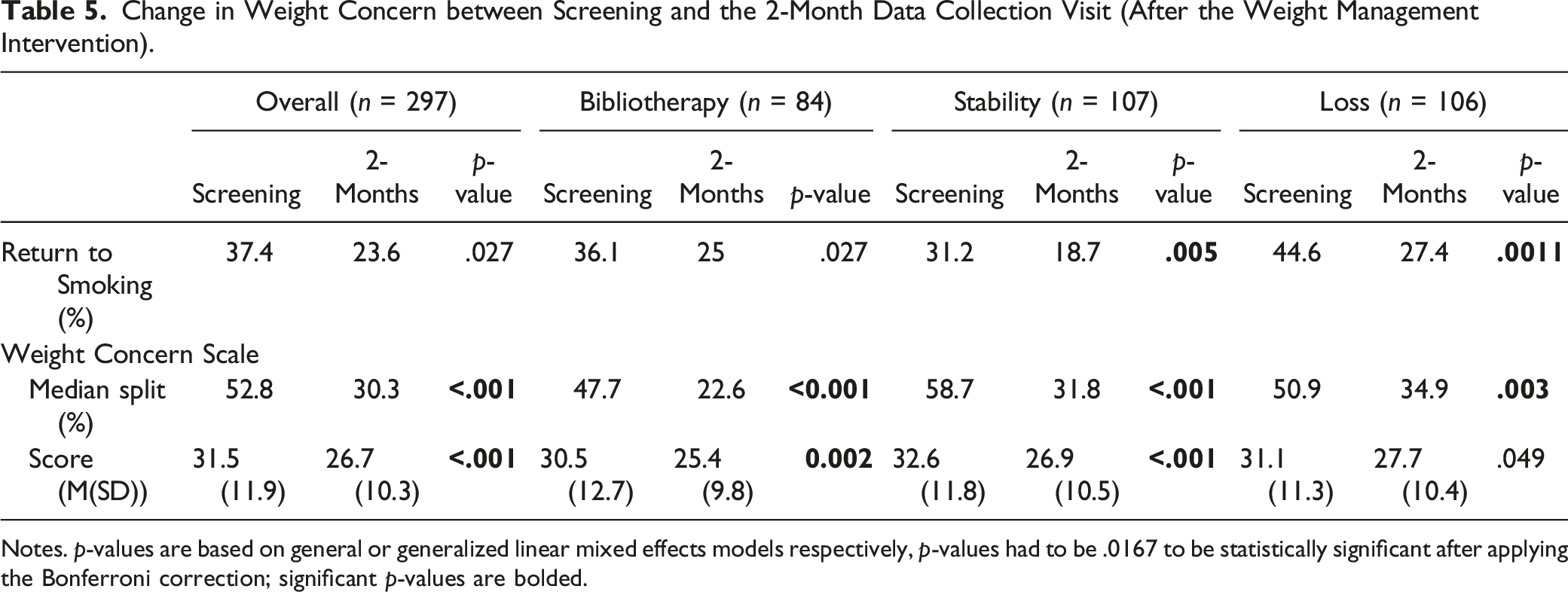
Notes. p-values are based on general or generalized linear mixed effects models respectively, p-values had to be .0167 to be statistically significant after applying the Bonferroni correction; significant p-values are bolded.
Discussion
Contrary to our hypotheses, there were no significant differences in 12-month weight change and program engagement when comparing weight-concerned and non-weight-concerned participants, regardless of the weight concern measure. There were also no significant differences in smoking cessation when comparing weight-concerned and non-weight-concerned participants within the three intervention groups on any of the measures. Results suggest weight concern may not affect how much benefit participants may get from combined cessation and weight management programs.
Baseline levels of weight concern were similar in this sample compared to previous studies using these weight concern measures.37–41 In addition, similar to previous research which found women were more likely to be weight concerned,6,16 women in this trial reported more weight concern than men, and this difference was significant with the ‘Weight Concern Scale’ and ‘Why Do You Smoke’ measures. Furthermore, participants with overweight or obesity reported significantly more weight concern than healthy weight participants, on some weight concern measures, consistent with some of the previous research. 20 Finally, participants identifying as Black reported significantly less weight concern than participants identifying as White using the ‘Return to Smoking’ questionnaire, which is consistent with previous research which found Black women reported less weight concern than White women and higher tolerance for post-cessation weight gain.18,19
Contrary to our hypothesis that weight-concerned smokers would have greater increase in weight post-cessation than non-weight-concerned participants, we found no significant differences in weight gain at 12-month follow-up, regardless of weight concern measure used. Results were inconsistent with previous research performed: one prospective study where weight concern positively predicted weight gain 8-weeks and 16-weeks after combined smoking cessation and weight management treatment, and another where weight concern predicted weight gain at 3 months after smoking cessation treatment.11,24 However, it is possible that, given the longer time horizon of the current study, we did not see these potentially short-term weight gain differences.
We also hypothesized, based on previous research, that weight-concerned participants would have lower abstinence at 12 months compared to non-weight-concerned participants and would have lower engagement in the smoking cessation program. Contrary to our hypothesis, we found no significant differences in smoking session attendance and smoking cessation status between weight-concerned and non-weight-concerned participants, across all three measures of weight concern. These findings could indicate that participants’ weight concerns may have been alleviated by receiving a weight management intervention, and consequently they felt prepared to engage in smoking cessation. In addition, it is possible that we did not find differences in smoking cessation by level of weight concern in this sample, since many previous studies were restricted to those with weight concern while the current study was not restricted to those with weight concern.42,43
Finally, we hypothesized that weight-concerned smokers would engage more in the weight management program components, because participants with weight concern, by definition, have more concern about post-cessation weight gain. However, contrary to this hypothesis, there were no significant differences in weight session attendance between weight-concerned and non-weight-concerned participants, across all three weight concern measures. These findings are somewhat consistent with a previous study which found that while weight-concerned individuals were more likely to enroll in attend initial cessation program sessions if offered weight management program, the majority did not actually utilize the offered weight management program. 44
This study is unique in that it assessed the impact of weight concern status on engagement in weight management and smoking cessation programs, as well as the influence of weight concern on weight change and self-reported abstinence status. This trial also combined behavior cessation treatment with varenicline pharmacotherapy and was successful in assisting approximately half of the sample quit smoking, which is slightly higher than previous pharmacotherapy-only cessation trials as well as trials that have combined behavior therapy with pharmacotherapy.45–48 The study also expands the literature in this area with a racially diverse group of men and women. 13 While we did not report the relationship between weight concern and biochemically-verified abstinence in this secondary analysis, we previously reported the high level of concordance between self-reported abstinence and biochemically-verified abstinence elsewhere. 25 Additionally, this study followed participants over 12 months, which is a longer period than several previous studies. Further, multiple weight concern measures were used that measure slightly different aspects of weight concern, 34 so the results do not rely on a single self-reported measure. However, this trial had low sample representation of participants who identified as Hispanic and those with high school degrees or less education, and those identifying with races other than White and Black. In addition, the trial had stringent inclusion/exclusion criteria (e.g., ability to walk for exercise) and a behavioral run-in, so future research will need to determine if these results generalize to a more inclusive sample. Also, the trial was not designed to conduct these secondary analyses and some of sample sizes were small, particularly related to the engagement, weight change, and smoking cessation parameters; thus, it is possible that we did not have sufficient power to detect differences. Additionally, these findings are based on three types of post-cessation weight management programs, but the generalizability of these findings to other post-cessation weight management strategies 49 is unknown. Furthermore, the level of engagement with the EatingWell Diet book in the Bibliotherapy condition was not assessed. Finally, since all participants received a weight management intervention, it is unclear how weight concern might impact a true control group.
Overall, weight-concerned participants did not differ from non-weight-concerned participants in weight gain at 12 months, abstinence status, and program engagement. Results suggest that weight concern status does not affect the level of need or benefit that participants may obtain from a program that combines weight management with smoking cessation. Thus, when participants are enrolled in post-cessation weight management programs, baseline weight concern may not be an important concern, should these results be confirmed in other research. Additionally, based on our findings of significantly lower weight concern after the 2-month weight management period in this study, all of these weight management programs may have successfully addressed weight concern.
• Weight concern is generally higher among women and those who identify as White.
• There were no differences in weight change, smoking cessation, or program engagement based on weight concern level. • Weight concern significantly decreased between screening and 2 months. Thus, all of the weight management programs in this study may have successfully addressed weight concern.
• Weight concern status appears not to affect the level of benefit that participants may obtain from a program that combines weight management with smoking cessation.So What?
What Is Already Known on This Topic?
What Does This Article Add?
What Are the Implications for Health Promotion Practice or Research?
Supplemental Material
Supplemental Material - Impact of Weight Concern on Post-Cessation Weight Management, Smoking Cessation, and Program Engagement
Supplemental Material for Impact of Weight Concern on Post-Cessation Weight Management, Smoking Cessation, and Program Engagement by Anjola Toyon, Zoran Bursac, PhD, Nicole Werner, PhD, and Rebecca A. Krukowski, PhD in American Journal of Health Promotion
Footnotes
Author Contributions
Anjola Toyon: Literature Review, Writing-Original Draft; Zoran Bursac: Formal analysis, Data curation, Writing- Review & editing. Nicole Werner: Review & editing. Rebecca Krukowski: Conceptualization, Methodology, Funding acquisition, Supervision, Writing- Review & editing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by a grant from the National Institutes of Diabetes and Digestive and Kidney Diseases, with the title of “Efficacy of Two Novel Behavioral Post Cessation Weight Gain Interventions” (R. Krukowski, Principal Investigator, R01DK107747).
Ethical Statement
Clinical Trial Registration
The trial is registered on clinicaltrials.gov (NCT03156660).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.