
Abstract
Purpose
To assess the relationship between behavioral health provider (BHP) perceptions of support during COVID-19 and burnout and self-reported workload.
Design
We conducted a cross-sectional analysis of provider-level data collected from the 2020 and 2021 All Employee Survey (AES).
Setting
The Veterans Health Administration.
Subjects
36,541 (10,332 [28.28%] with missing data) respondents in 2020 and 2021 combined.
Measures
Main outcomes were self-reported burnout and self-reported workload. Main predictors were 6 COVID-19-related provider-perceived support domains. Covariates were 11 AES demographic predictors.
Analysis
We conducted mixed-effects logistic regression modeling for each domain and outcome pairing. We summarized our results using average marginal effects (AMEs) and odds ratios (ORs).
Results
All 6 domains of feeling prepared, heard, protected, cared for, honored, and having flexible policies were significantly negatively associated with burnout (AMEs −.20 to −.10, ORs .38-.63, P < .001) and positively associated with reasonable workload (AMEs .11-.20, ORs 1.63-2.59, P < .001). Feeling prepared had the largest associations with burnout (OR .38) and reasonable workload (OR 2.59).
Conclusion
Creating a work environment with flexible policies and where staff feel prepared, heard, protected, cared for, and honored could support BHPs in feeling less burned out and that their workload is reasonable.
Purpose
The COVID-19 pandemic had well-established negative impacts on the health care workforce, particularly front-line workers 1 and, to a lesser extent, second-line workers such as behavioral health providers (BHPs).2,3 Historically, BHPs experienced one of the highest rates of burnout among health care workers, reaching 50%.4,5 Within the Veterans Health Administration (VHA), BHP burnout rates ranged from 31% to 38% during 2015-2018. 6 In this context, we sought to assess the relationship between VHA BHP self-reported burnout and workload with perceptions of supervisory, leadership, and organizational support during the COVID-19 pandemic.
Methods
Design
We analyzed provider-level data from the 2020 and 2021 All Employee Surveys (AES), which included a COVID-19 module. 7 We included respondents who self-identified as psychiatrists, psychologists, or social workers. The VA Ann Arbor Healthcare System Institutional Review Board (IRBNet ID 15975568) approved this study waiving informed consent.
Measures
Our main outcomes were self-reported burnout and self-reported workload. We used responses to 2 burnout-related items: “I feel burned out from my work” and “I worry that this job is hardening me emotionally” (response scale from 1 = never to 7 = every day), where responses to either question of
COVID-19 Module Items by Domain, all Employee Survey (AES) 2020 and 2021.
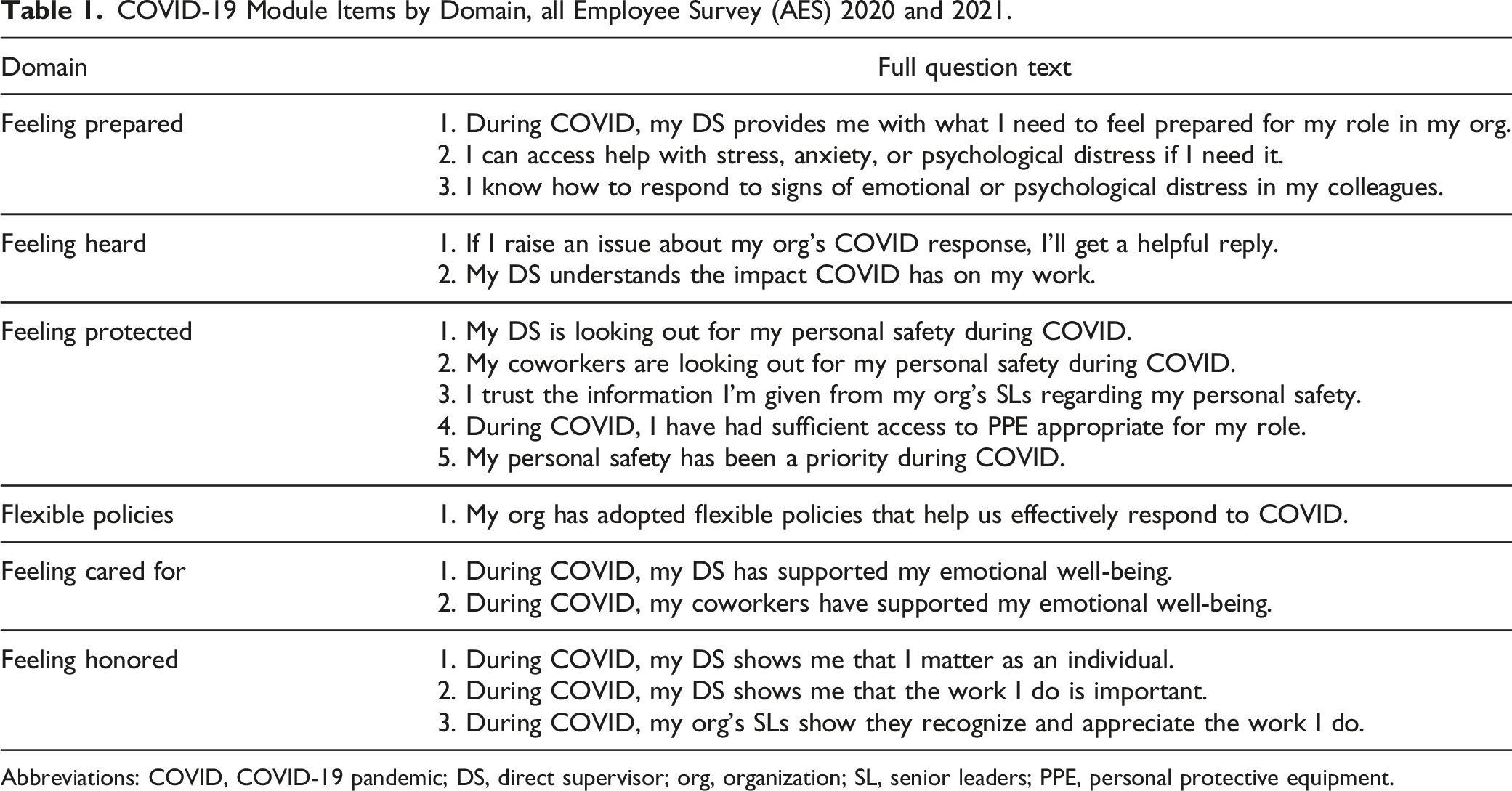
Abbreviations: COVID, COVID-19 pandemic; DS, direct supervisor; org, organization; SL, senior leaders; PPE, personal protective equipment.
We adjusted for 11 socio-demographic characteristics from AES: gender, race, Hispanic background, VHA tenure, supervisory role, prior active duty, assigned to care team, faculty position, prior VHA training, disabled, and teaches or supervises health trainees. We also adjusted for facility-level staffing ratio, available from VHA Office of Mental Health and Suicide Prevention.
Analysis
We combined 2020 and 2021 respondents and summarized percentage of respondents reporting burnout and RW and compared each of the 6 domain scores by burnout status and by RW status. Due to missing data, we created 5 imputed datasets by chained equations to conduct fully adjusted mixed-effects logistic regression models predicting burnout and predicting RW. We ran separate multi-level logistic models for each of the 6 COVID-19-related domains and outcome pairings, for a total of 12 models. In each model, we included facilities as random intercepts to account for clustering and adjusted for year and socio-demographic characteristics. We summarized our results using average marginal effects (AMEs) and odds ratios (ORs).
Results
Among our total sample of 36,541 respondents (18,293 in 2020 and 18,248 in 2021), 13,320 (36.45%) of the respondents experienced burnout and 22,303 (61.04%) of the respondents reported a RW. Details on our sample appear in the Online Supplement.
28.28% of respondents had missing data for at least one variable. Missingness in individual variables ranged from 0% to 7.62%. Results of our adjusted models appear in Figure 1. Feeling prepared, heard, protected, cared for, honored, and having flexible policies were significantly associated with burnout (ORs .38-.63, P < .001), with AMEs of −.20 to −.10, indicating higher domain scores were negatively associated with burnout. Feeling prepared, heard, protected, cared for, honored, and having flexible policies were significantly positively associated with RW (ORs 1.63-2.59, P < .001), with AMEs of .11 to .20. Feeling prepared had the strongest association with both decreased burnout (OR .38) and RW (OR 2.59). Forest plots of AMEs and 95% CIs calculated from multivariable cross-sectional models predicting burnout and reasonable workload in the 2020 and 2021 AES*. *All models are adjusted for demographic characteristics and facility-level staffing ratio as fixed effects and are adjusted for facilities as random intercepts. Abbreviations: All Employee Survey (AES); Average Marginal Effect (AME); confidence interval (CI). Interpretation: An AME of −.09 corresponds to a 9% point reduction in the outcome associated with a 1 unit increase in the domain score.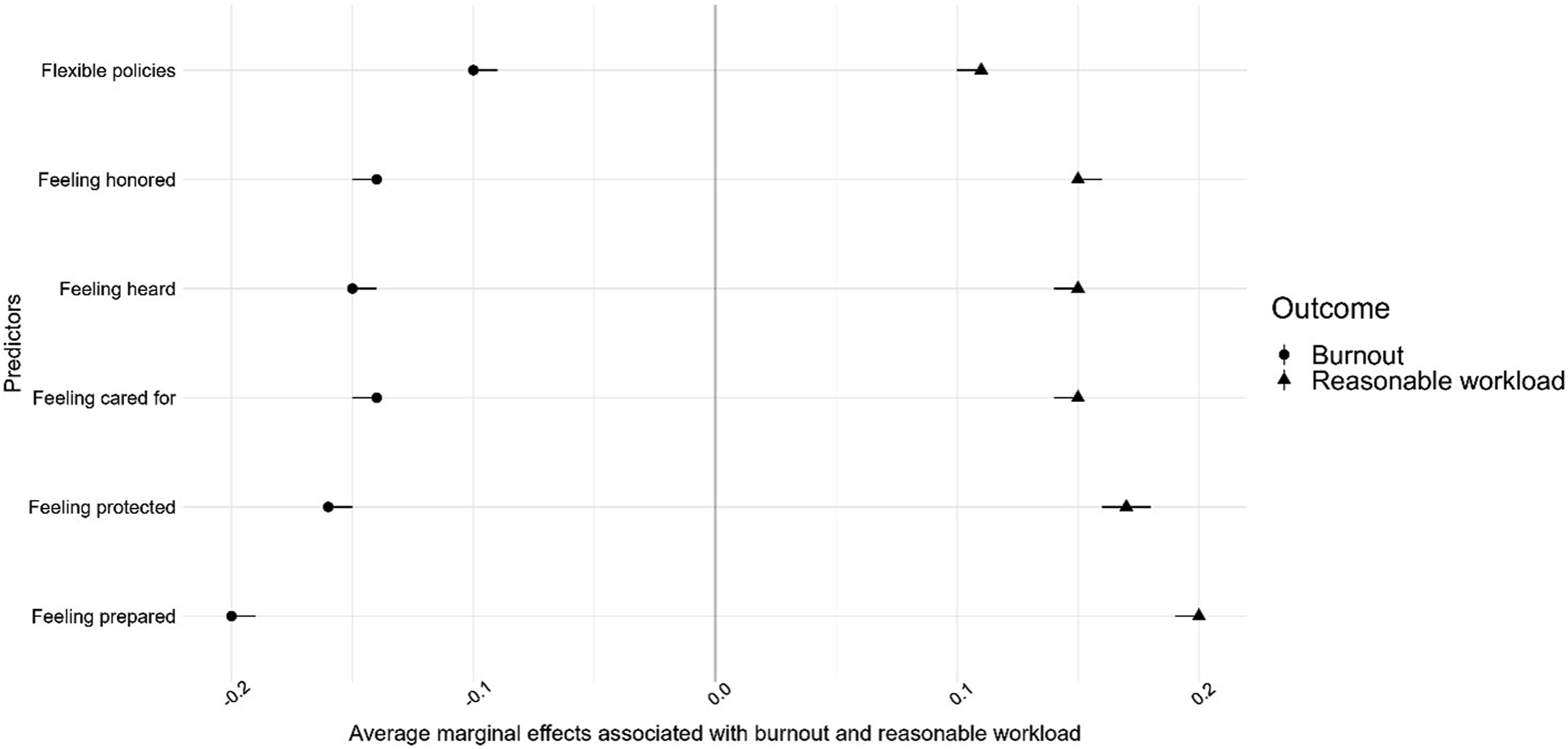
Discussion
Summary
BHPs who felt their organization had flexible policies and made them feel prepared, heard, protected, cared for, and honored during the COVID-19 pandemic experienced less burnout and viewed their workload as more reasonable. Within these domains, a commonality is the role supervisors play in supporting staff, including providing what staff need to feel prepared, looking out for staff personal safety, understanding the impact of the pandemic on staff’s work, supporting staff’s emotional well-being, and showing staff that they matter and do important work. Leadership also played an important role in responding to staff when they raised an issue, providing appropriate personal protective equipment to staff, appearing trustworthy to staff, and showing recognition and appreciation for staff’s work. These findings align with other work indicating that front-line provider well-being had associatons with workplace, supervisor, and leadership support, 8 as well as having conditions that supported productivity and enough time to complete work.8,9 Feeling prepared had the largest association with decreased burnout and RW. Along with supervisors making staff feel prepared in their position, this domain included items related to accessing help for emotional distress and knowing how to respond to coworker emotional distress. A 2021 literature review showed that workplaces that promoted mental health awareness and coworker support experienced enhanced provider well-being. 10
Our findings align with the Job Demands-Resources model, where burnout is experienced when job demands, such as workload and emotional strain, outweigh job resources. The support domains in this study reflect job resources that have been included in the model by others, such as supervisory support, role clarity, trust in leadership, and recognition. 11
Training supervisors in how to make their staff feel prepared, heard, protected, cared for, and honored could support the emotional well-being of BHPs, especially during large-scale events that strain health systems. Providing access for BHPs to help for psychological distress, training BHPs to recognize distress symptoms in colleagues, and training supervisors and leadership to show respect and appreciation for BHPs and the work they do could provide an environment where providers feel that their workload is reasonable and feel less burned out.
Limitations
We imputed data for 28.28% of combined respondents with at least one missing data. Missing responses on individual items ranged from zero to 7.62%.
Significance
In the early months of the COVID-19 pandemic, the World Health Organization declared that the provision of care to the community was dependent on protecting health care workers from stress.
12
Although the health care strain has significantly lessened since then, health care systems should utilize the knowledge of how providers felt most supported during the pandemic in order to ensure that they are ready to face future pressures. The COVID-19 pandemic not only had significant impacts on front-line health care workers,
1
but also second-line workers such as behavioral health providers (BHPs).
2
This work uses 2020 and 2021 VHA survey data to assess the relationship between BHP perceptions of supervisory, leadership, and organizational support during COVID-19 and burnout and self-reported workload. To protect against burnout and promote reasonable workload, health care systems should use knowledge of how providers felt most supported during the pandemic, namely providing access to help for psychological distress and training on recognizing symptoms in colleagues, and training supervisors and leadership in how to make staff feel prepared, heard, protected, cared for, and honored.So What?
What is already known on this topic?
What does this article add?
What are the implications for health promotion practice or research?
Supplemental Material
Supplemental Material - Burnout and Perceived Workload Among Behavioral Health Providers During the COVID-19 Pandemic: Importance of Supervisory, Leadership, and Organizational Support
Supplemental Material for Burnout and Perceived Workload Among Behavioral Health Providers During the COVID-19 Pandemic: Importance of Supervisory, Leadership, and Organizational Support by Jennifer Burgess, Hyungjin Myra Kim, Brittany R. Porath, and Kara Zivin in American Journal of Health Promotion
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by VA Health Services Research and Development Service (VA IIR 17-262; VA RCS 21-138 and VA RCS 21-238).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.