
Abstract
Background
Hypertension-related knowledge, attitude and practice (KAP) of hypertensive patients can affect the awareness, treatment and control of hypertension. However, little attention has been paid to the association between the change of hypertension preventive KAP and blood pressure (BP) control in occupational population using longitudinal data. We assess the effectiveness of a workplace-based multicomponent hypertension intervention program on improving the level of KAP of hypertension prevention, and the association between improvement in KAP and BP control during intervention.
Methods
From January 2013 to December 2014, workplaces across 20 urban regions in China were randomized to either the intervention group (n = 40) or control group (n = 20) using a cluster randomized control method. All employees in each workplace were asked to complete a cross-sectional survey to screen for hypertension patients. Hypertension patients in the intervention group were given a 2-year workplace-based multicomponent hypertension intervention for BP control. The level of hypertension prevention KAP and BP were assessed before and after intervention in the two groups.
Results
Overall, 3331 participants (2658 in the intervention group and 673 in the control group) were included (mean [standard deviation] age, 46.2 [7.7] years; 2723 men [81.7%]). After 2-year intervention, the KAP qualified rate was 63.2% in the intervention groups and 50.1% in the control groups (odds ratio = 1.65, 95% CI, 1.36∼2.00, P < .001). Compared with the control group decreased in the qualified rate of each item of hypertension preventive KAP questionnaire, all the items in the intervention group increased to different degrees. The increase of KAP score was associated with the decrease of BP level after intervention. For 1 point increase in KAP score, systolic blood pressure (SBP) decreased by .28 mmHg and diastolic blood pressure (DBP) decreased by .14 mmHg [SBP: β = -.28, 95%CI: −.48∼-.09, P = .004; DBP: β = −.14, 95%CI: −.26∼-.02, P = .024]. SBP and DBP was significantly in manual labor workers (SBP: β = −.34, 95%CI: −.59∼-.09, P = .008; DBP: β = −.23, 95%CI: −.38∼−.08, P = .003), workers from private enterprise, state-owned enterprise (SOE) (SBP: β = −.40, 95%CI: −.64∼−.16, P = .001; DBP: β = −.21, 95%CI: −.36∼−.06, P = .005) and a workplace with an affiliated hospital (SBP: β = −.31, 95%CI: −.52∼−.11, P = .003; DBP: β = −.16, 95%CI: −.28∼−.03, P = .016). The improvement of knowledge (SBP: β = −.29, 95%CI: −.56∼−.02, P = .038; DBP: β = −.12, 95%CI: −.29∼.05, P = .160), as well as attitude (SBP: β = −.71, 95%CI: −1.25∼−.18, P = .009; DBP: β = .18, 95%CI: −.23∼.59, P = .385) and behavior (SBP: β = −.73, 95%CI: −1.22∼−.23, P = .004; DBP: β = −.65, 95%CI: −.97∼−.33, P < .001) was gradually strengthened in relation to BP control.
Conclusion
This study found that workplace-based multicomponent hypertension intervention can effectively improve the level of hypertension preventive KAP among employees, and the improvement of KAP levels were significantly associated with BP control.
Trial Registration
Chinese Clinical Trial Registry No. ChiCTR-ECS-14004641.
Keywords
Introduction
Hypertension is a major modifiable risk factor of cardiovascular disease (CVD) and premature death worldwide.1,2 An estimated 1.28 billion adults aged 30-79 years worldwide had hypertension. 3 In China, the estimated number of Chinese adults with hypertension was 245 million. Although it is well known that appropriate blood pressure (BP) control in hypertension patients has been known to reduce CVD events effectively; 4 however, only approximately 1 in 5 adults with hypertension have it under control. 3
According to the theory of knowledge, attitude and practice (KAP), 5 health care knowledge and information are the basis for building active, correct attitudes, and attitudes are the driving force for practice change. Only when patients understand the relevant health knowledge, can they establish positive and correct beliefs and attitudes, so as to actively form healthy practices. This suggests that hypertension patients correctly understand the hypertension-related knowledge plays a very important role in the prevention and treatment of hypertension. Previous study have also shown that hypertension-related knowledge, attitude and practice of hypertensive patients can affect the awareness, treatment and control of hypertension. 6 Therefore, it is necessary to evaluate the impact of interventions on hypertension preventive KAP and the association between the change of KAP with BP control, so as to better carry out hypertension management and control BP more effectively.
As the main force of the adult population, the occupational population accounts for more than 60%. On average, they spend about 1/3 of their time in the working environment every day. This period is a critical time in their life when they make contributions to society and their families, and their general health is of great significance for the stability and development of society. However, previous studies showed that the prevalence of hypertension was high among Chinese working population, but rates of awareness, treatment, and control were low,7-9 and cardiovascular health status was not ideal. 10 Therefore, carrying out hypertension management is of great importance and urgent need in occupational population. From the international perspective, a workplace-based intervention could be an effective approach to assisting employees with uncontrolled hypertension to reach their BP goals.11,12 Currently, many countries have developed worksite health and wellness policy, and achieved remarkable effects.13-17 However, little attention has been paid to the association between the change of hypertension preventive KAP and BP control in occupational population using longitudinal data.
In our previous study, we had proofed the effectiveness of a multicomponent intervention strategy that combined workplace health promotion and standardized management of hypertension to improve BP control among employees. 18 On this basis, our study aimed to analyze the improvement of KAP and the association with BP control during hypertension intervention in Chinese occupational population, so as to provide evidence-based basis for carrying out targeted prevention and control of hypertension in the workplace.
Methods
Study Design
We selected 20 urban medical institutions representing different geographical locations in China as subcenters (Figure 1). Full details of study design and protocol can be found in the previous publication.
18
In order to minimize bias, each subcenter comprises 2 to 4 workplaces, all of which should meet the following criteria: (1) more than 50 hypertension patients can be recruited per site; (2) workplaces within the same subcenter should be matched by sector, ownership, size, economic level and medical condition; (3) none similar programs were conducted before; (4) non-medical institutions; (5) agrees to arrange at least one full-time or part-time project officer to execute the workplace wellness program; and (6) can select a designated hospital clinic for implementing the standardized hypertension management for 2 years. Flow chart of the patient selection process.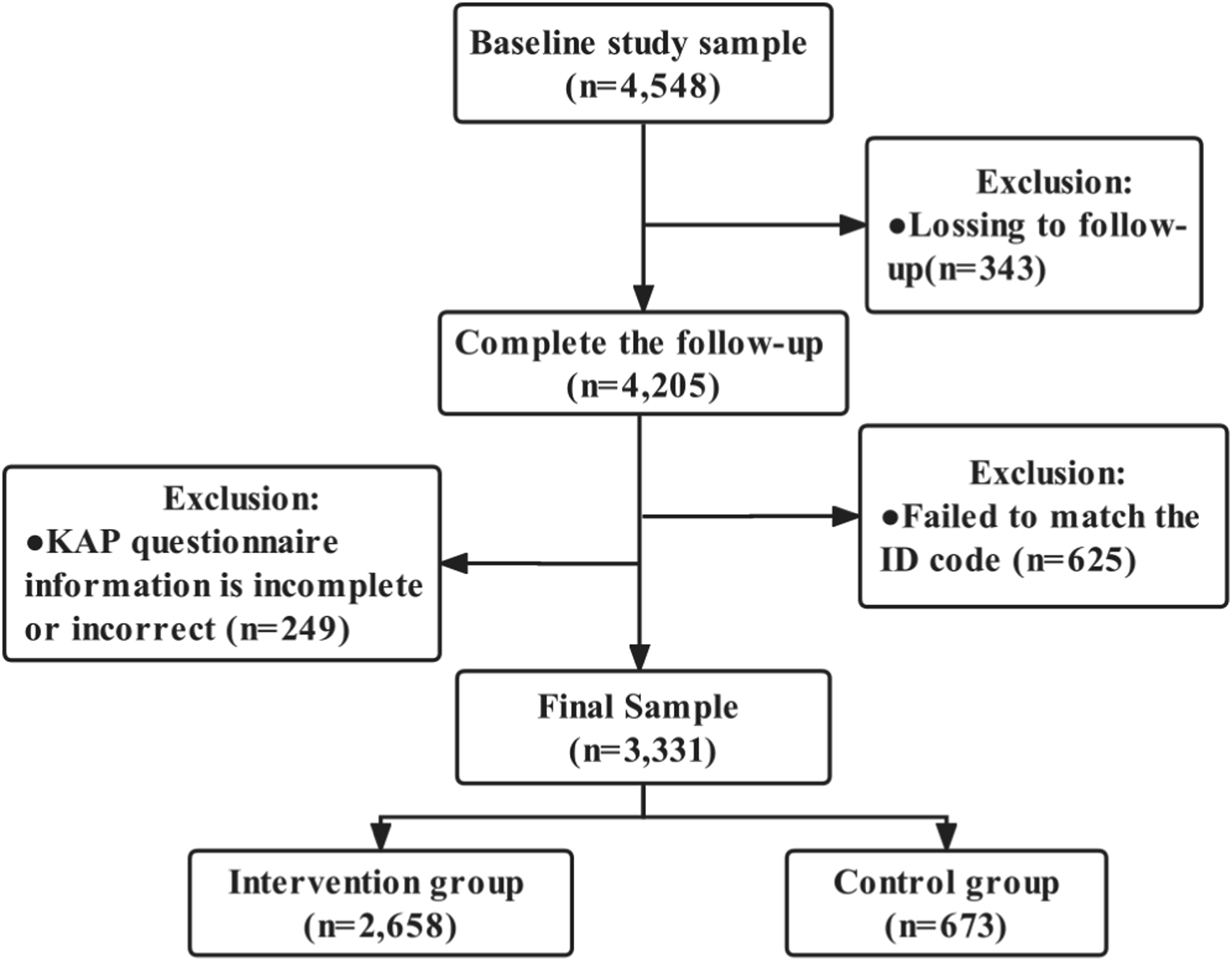
Considering the intervention benefits and ethical issues, subcenters served as clusters and the workplace was the unit of randomization in the 2: 1 cluster randomized controlled study. One workplace was randomly selected as the control group, and the remaining workplaces were as the intervention group. Finally, 40 workplaces were randomly divided into the intervention group and 20 workplaces into the control group. The duration of the intervention was 2 years, and participants completed standardized questionnaires under the guidance of the investigator before and after the intervention. The written informed consent was obtained from each participant. The Ethics Committee of Fuwai Hospital (Beijing, China) and each subcenter approved this study.
Participants
After randomization, at least 50 individuals with hypertension from each workplace in the intervention and control groups were selected. Inclusion criteria for individuals included: (1) diagnosis of primary hypertension, (2) age 18-60 years, (3) contracted employee, (4) signed consent form, and (5) agreed to participate in our program for a minimum of 2 years. Exclusion criteria were determined primarily on the basis of participant history taking, and further exclusions were made by specialized clinicians when conducted at baseline, including: (1) secondary hypertension; (2) acute myocardial infarction or stroke occurred within 3 months; (3) women who were pregnant or have given birth within 3 months; (4) Have a serious medical conditions and life expectancy of less than 2 years; (5) being mentally ill, hearing impaired or physically incapacitated; (6) health care practitioners. The improvement in KAP qualified rate, as well as the association between the changes of KAP score and BP control before and after intervention was analyzed. A total of 3331 employees were included in the final analysis after excluding individuals with incomplete or incorrect data related to our study (Figure 1).
Intervention
The 2-year intervention included 2 components: (1) a workplace wellness program based on the recommendations from the American Heart Association 19 and the 2010 Chinese hypertension management guidelines 20 for improving participants’ cardiovascular health, including (1) CVD health education, (2) a reasonable diet, (3) tobacco cessation, (4) physical environment promotion, (5) physical activity, (6) stress management, and (7) health screening, and (2) a guidelines-based hypertension management program with a community health center (CHC) intervention accompanied by monthly visits for achieving BP control, including (1) classification of hypertension, (2) stratification of global risk (the risk stratification of hypertension patients into low risk, medium risk and high risk based on medical history, family history, physical examination results, etc and according to guideline 20 ), (3) targets for BP control, (4) principles of treatment, (5) lifestyle changes, (6) drug treatment, and (7) follow-up management. The CVD health education used lectures, posters, and text messages to educate employees on the knowledge or prevention of CVD risk. The reasonable diet included providing nutrition education and/or healthy eating information to employees. Affordable low-salt or low-fat foods were easily available, and employees were encouraged to select healthy foods during lunch in the workplace cafeteria. Tobacco control regulation was developed and smoking was prohibited in the workplaces. Modifying workstations and office layouts to reduce sedentary behavior and increase movement. Encouraging employees to increase physical activity through exercise breaks during working hours. Accessible indoor or outdoor exercise facilities were provided for regular physical activity by employees. Relaxation techniques were provided monthly by employees who specialized in meditation, tai chi, or deep breathing to help employees cope with stress. Annual health examinations and feedback was provided for identify key risk factors. In the intervention group, employees were asked to monthly visit the CHCs, during which the physicians assessed their BP level. Employees in the control group were seen in the CHCs at baseline and the end of the program, received only usual care to prevention or treatment of diseases supported by health insurance, and did not receive any intervention from our program. Usual care is the basic public health services provided by the state without any restrictions, both intervention and control group employees were available, including screening, follow-up evaluation, classified intervention, health examination services. Therefore, the differences between the intervention and control groups were only for the multicomponent workplace-based hypertension interventions provided by our program to ensure that the intervention effect was indeed delivered by the intervention. Full details of intervention program can be found in the previous publication. 18
Definitions and Measurements
A unified hypertension prevention KAP questionnaire was used (S1 Appendix), which was filled in by the employees before and after the intervention and was withdrawn on the spot. The questionnaire was developed according to the dimensions and content of the KAP theory. After several rounds of expert review and revision, which has a certain degree of scientific rigor. The validity and reliability of knowledge, attitude and practice dimensions were analyzed respectively. Knowledge dimension: Cronbach’s α = .66, KMO = .78, Bartlett’s spherical test P < .001. Factor analysis extracted three common factors and the cumulative variance contribution rate is 47.1%; Attitude dimension: Cronbach’s α = .79, KMO = .76, Bartlett’s spherical test P < .001; Factor analysis extracted a common factor, and the cumulative variance contribution rate was 46.5%. Behavior dimension: Cronbach’s α = .61, KMO = .68, Bartlett’s spherical test P < .001; Factor analysis extracted two common factors and the cumulative contribution rate of variance was 53.9%. The reliability and construct validity of the questionnaire met the criteria. 21 About the hypertension prevention KAP questionnaire, items in the knowledge dimension were designed to investigate the correct awareness of hypertension knowledge of the subjects, and evaluated the diagnostic criteria of hypertension, risk factors of hypertension, complications of hypertension and so on. For each correct answer, the score was 1, and the wrong answer was 0. Items in the attitude dimension were designed to investigate the participants’ attitude towards the prevention and treatment of hypertension, and evaluating the importance of non-drug treatment and drug treatment respectively. For each question, the participants who answered “yes” scored 1 point, those who answered “don’t know” or “no” scored 0 point. Items in the practice dimension were designed to investigate the subjects’ hypertension-related practices and lifestyles, and evaluated them from smoking, drinking, dietary taste, physical exercise, BP measurement and so on. One point was scored for positive practice and 0 point for negative practice. The scores of dimension of knowledge, attitude and practice were 10, 10 and 7, respectively. The KAP score was the sum of the scores of each dimension of knowledge, attitude and practice, with a total of 27 points. The higher the score, the better the KAP status of the subjects. The KAP score was judged as qualified if it was greater than or equal to the median (≥18 points before the intervention and ≥20 points after the intervention), and if it was less than that, it was disqualified.
The diagnostic criteria for hypertension were three BP measurements on different days, systolic blood pressure (SBP) ≥ 140 and/or diastolic blood pressure (DBP) ≥90 mmHg (1 mmHg = .133 kPa), history of hypertension, or taking antihypertensive drugs within 2 weeks before the survey. Smoking was defined as those who smoked at least one cigarette a day for more than one year. Drinking (beer, white wine and yellow rice wine) was defined as those who drank at least one drink a week on average. Regular exercise was defined as exercising at least 3 times a week for at least 30 min each time. The low-salt diet was defined as self-reported low dietary taste. The low-fat diet was defined as low self-reported intake of fat-rich food at three meals per day. Less work/life stress was defined as participants’ recent feeling of little or no work/life stress. Regular BP measurement means that BP is measured at least once a quarter on average.
Outcome Measurements
In this analysis, we mainly conducted an exploratory analysis of the improvements of KAP and BP levels from baseline to 24 months in the two groups. On this basis, the intervention effect on KAP qualified rate and the association of KAP changes with BP control were further analyzed. The change in KAP qualified rate was defined as the post-intervention KAP qualified rate minus the pre-intervention KAP qualified rate, and the change in BP levels was defined as the post-intervention SBP/DBP value minus the pre-intervention SBP/DBP value, from baseline to 24 months.
Statistical Analysis
All employees who attended follow-up visits at 24 months and had complete primary outcome data and other variables were included in the analysis. Considering the clustering effect (intraclass correlation coefficient = .036), a mixed effects model with the subcenters as random effect was performed to examine the differences in baseline and follow-up data between groups as well as the intervention effect on change of KAP and other outcomes over time by additionally adjusting for age at recruitment (continuous), sex (male or female), marital status (married or unmarried), educational attainment (elementary or below, junior high school, college or above), history of CVD (yes or no), family history of hypertension (yes or no), pharmacological treatment (yes or no), employment status (manual labor worker, desk job worker, administrative workers, others), workplace ownership [private enterprise, state-owned enterprise (SOE), university, research institute], workplace-affiliated hospital [workplace without affiliated hospital (WWH), workplace with affiliated hospital (WAH)]. The hierarchical statistical techniques were used to capture the heterogeneity of workplace intervention. To handle the missing data on outcome and other covariates, a multiple imputation method was employed for sensitivity analyses to robust the primary outcome analyses. The results were reported as rate (%), mean, standard deviation (SD), and 95% confidence interval (CI) when appropriate. The improvement of KAP was reported by odds ratio (OR) and 95% CI, with the strength of the association between improvement of KAP and BP by β and 95% CI. All data analyses were conducted using R version 4.1.0. A 2-tailed P value less than .05 was considered statistically significant.
Results
Basic Characteristics of Participants at the Workplaces
Baseline Characteristics for all Hypertension Employees Who Completed Follow-Up in the Study.
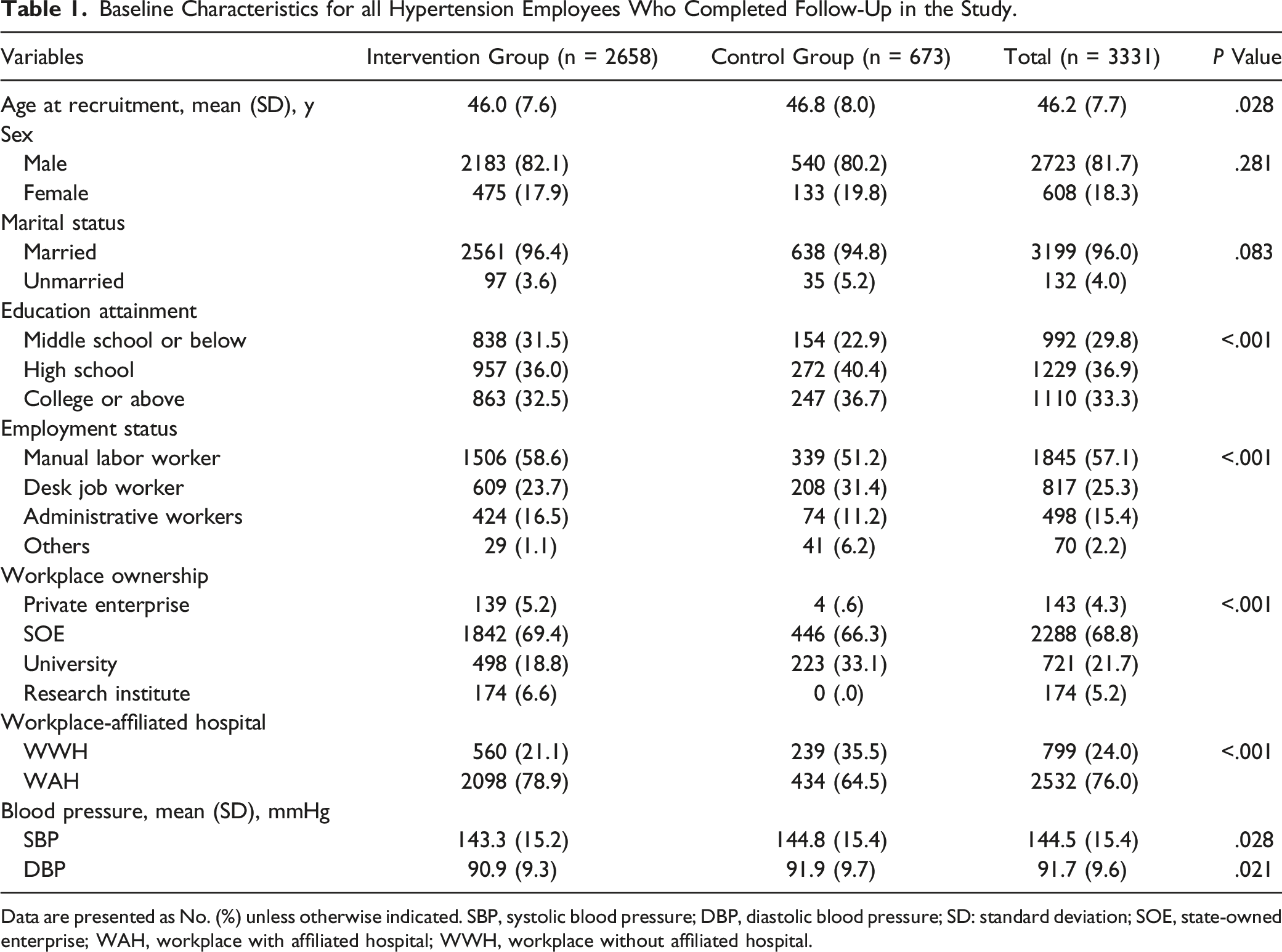
Data are presented as No. (%) unless otherwise indicated. SBP, systolic blood pressure; DBP, diastolic blood pressure; SD: standard deviation; SOE, state-owned enterprise; WAH, workplace with affiliated hospital; WWH, workplace without affiliated hospital.
Changes and Intervention Effects of the KAP Overall Qualified Rate
Changes and Intervention Effects in KAP overall Qualified Rate for Hypertension Employees.
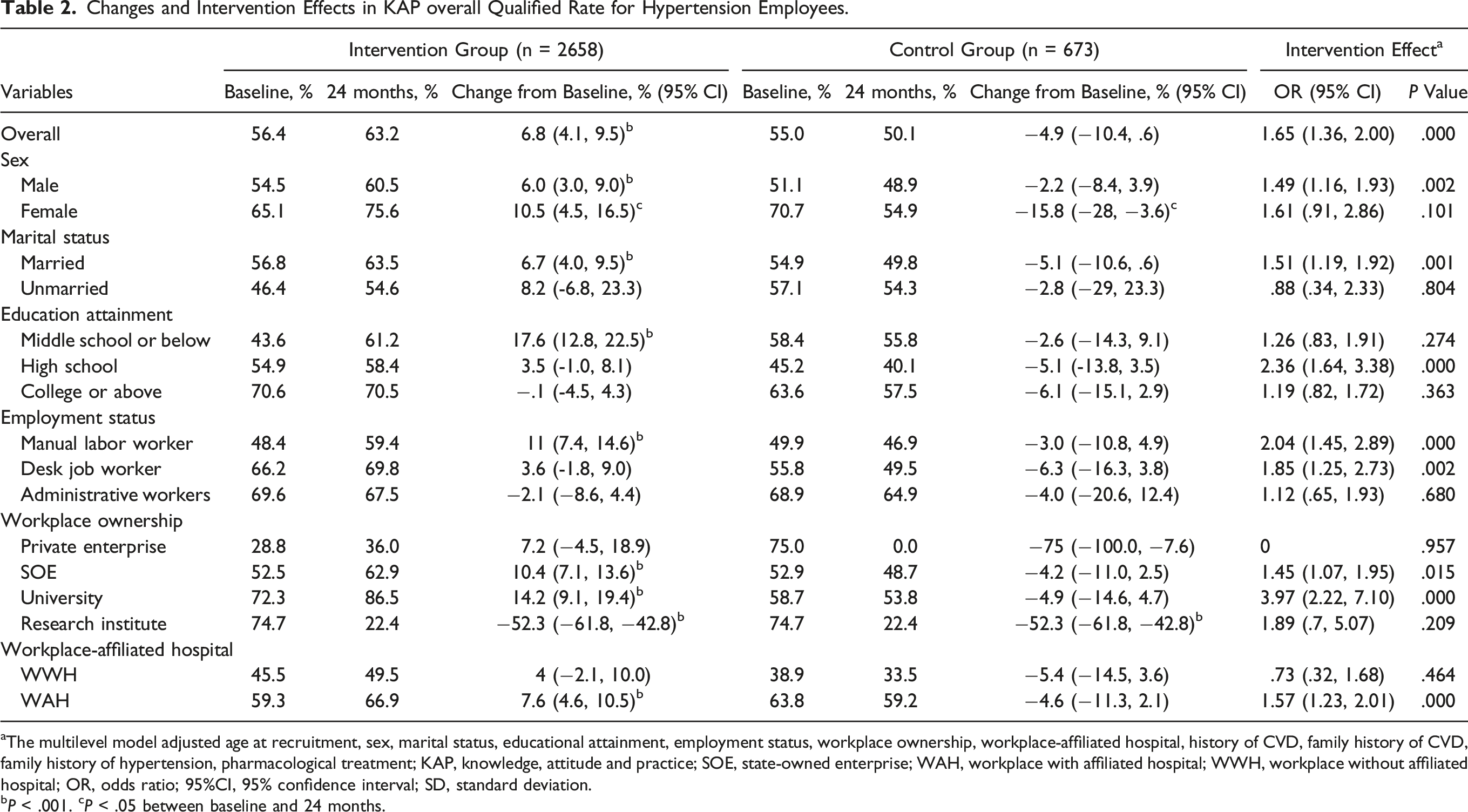
aThe multilevel model adjusted age at recruitment, sex, marital status, educational attainment, employment status, workplace ownership, workplace-affiliated hospital, history of CVD, family history of CVD, family history of hypertension, pharmacological treatment; KAP, knowledge, attitude and practice; SOE, state-owned enterprise; WAH, workplace with affiliated hospital; WWH, workplace without affiliated hospital; OR, odds ratio; 95%CI, 95% confidence interval; SD, standard deviation.
bP < .001. cP < .05 between baseline and 24 months.
Changes and Intervention Effects of the Qualified Rate of Each Item in KAP Questionnaire
Compared with the control group decreased in the qualified rate of all items in each dimension of KAP, the intervention group increased to different degrees. “standard daily salt intake for adults” (change: 21.8%, 95%CI: 19.2∼24.4, P < .001), “lifestyle treatment for hypertensive patients” (change: 22.4%, 95%CI: 19.7∼25, P < .001), and “regular BP measurement” (change: 22.3%, 95%CI: 19.8∼24.8, P < .001) increased most significantly and showed prominent intervention effect.
Changes of Score and Intervention Effects in Each Item for Hypertension Employees.
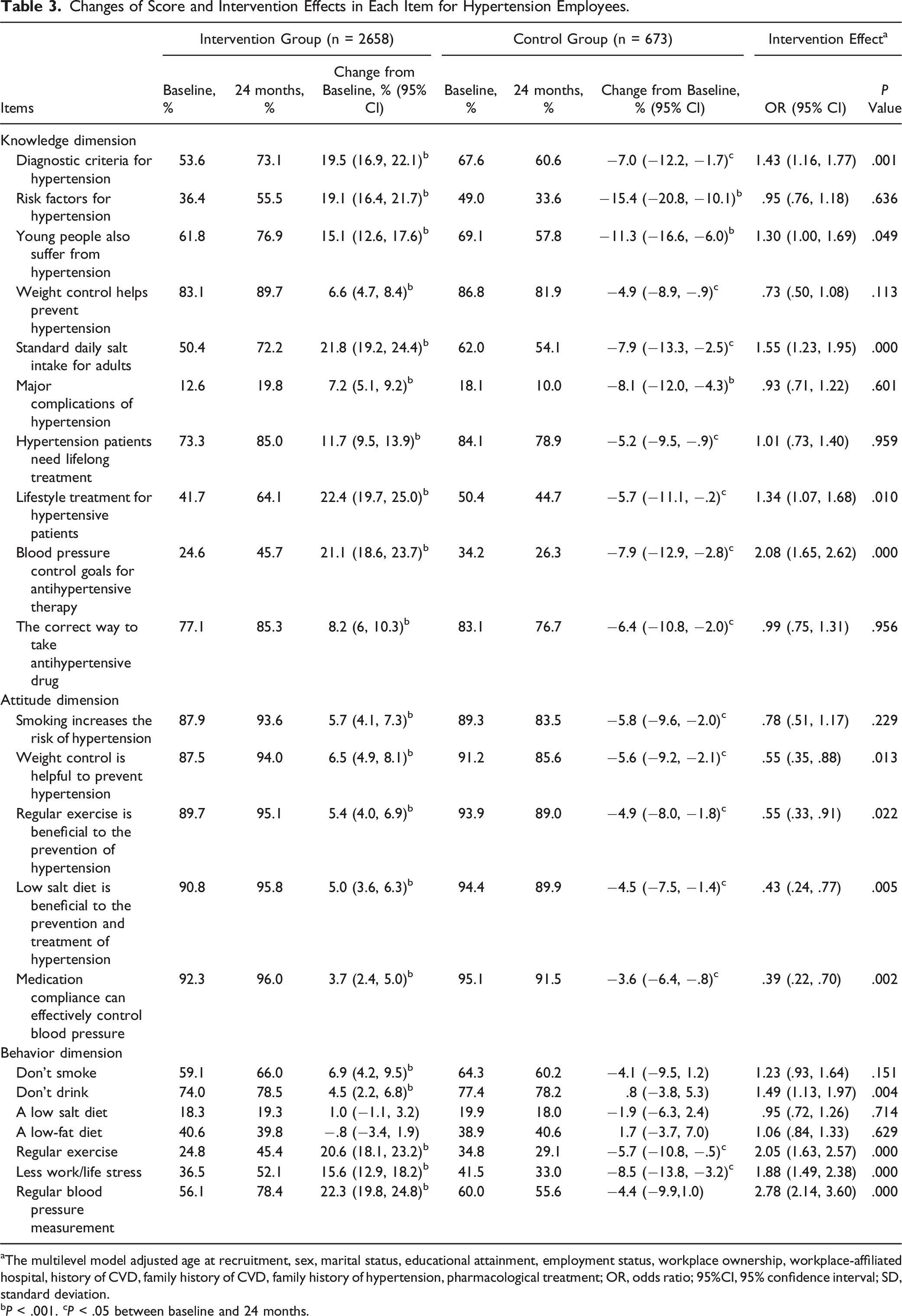
aThe multilevel model adjusted age at recruitment, sex, marital status, educational attainment, employment status, workplace ownership, workplace-affiliated hospital, history of CVD, family history of CVD, family history of hypertension, pharmacological treatment; OR, odds ratio; 95%CI, 95% confidence interval; SD, standard deviation.
bP < .001. cP < .05 between baseline and 24 months.
Association Between the Change of KAP Score and BP Control
The increase of KAP score was associated with the decrease of BP levels after intervention. For 1 point increase in KAP score, SBP decreased by .28 mmHg and DBP decreased by .14 mmHg (SBP: β = −.28, 95%CI: −.48∼−.09, P = .004; DBP: β = −.14, 95%CI: −.26∼−.02, P = .024) (Figure 2; S2 Table). The improvement of knowledge dimension (SBP: β = −.29, 95%CI: −.56∼−.02, P = .038; DBP: β = −.12, 95%CI: −.29∼.05, P = .160), attitude dimension (SBP: β = −.71, 95%CI: −1.25∼−.18, P = .009; DBP: β = .18, 95%CI: −.23∼.59, P = .385) and practice dimension (SBP: β = −.73,95%CI: −1.22∼.23, P = .004; DBP: β = −.65, 95%CI: −.97∼−.33, P < .001) score were gradually strengthened in relation to BP control (S3-5 Table). After multiple imputation for missing data, the association between the improvement of KAP score in each dimension and BP control remained significant (SBP: β = −.29, 95%CI: −.50∼−.07, P = .010; DBP: β = −.19, 95%CI: −.33∼−.05, P = .008) (S1 Table; S1 Figure). Association between the change of KAP score and blood pressure in employees. The multilevel model adjusted for age at recruitment, sex, marital status, educational attainment, employment status, workplace ownership, workplace-affiliated hospital, history of CVD, family history of CVD, family history of hypertension, pharmacological treatment; SBP, systolic blood pressure; DBP, diastolic blood pressure; SOE, state-owned enterprise; WAH, workplace with an affiliated hospital; WWH, workplace without an affiliated hospital.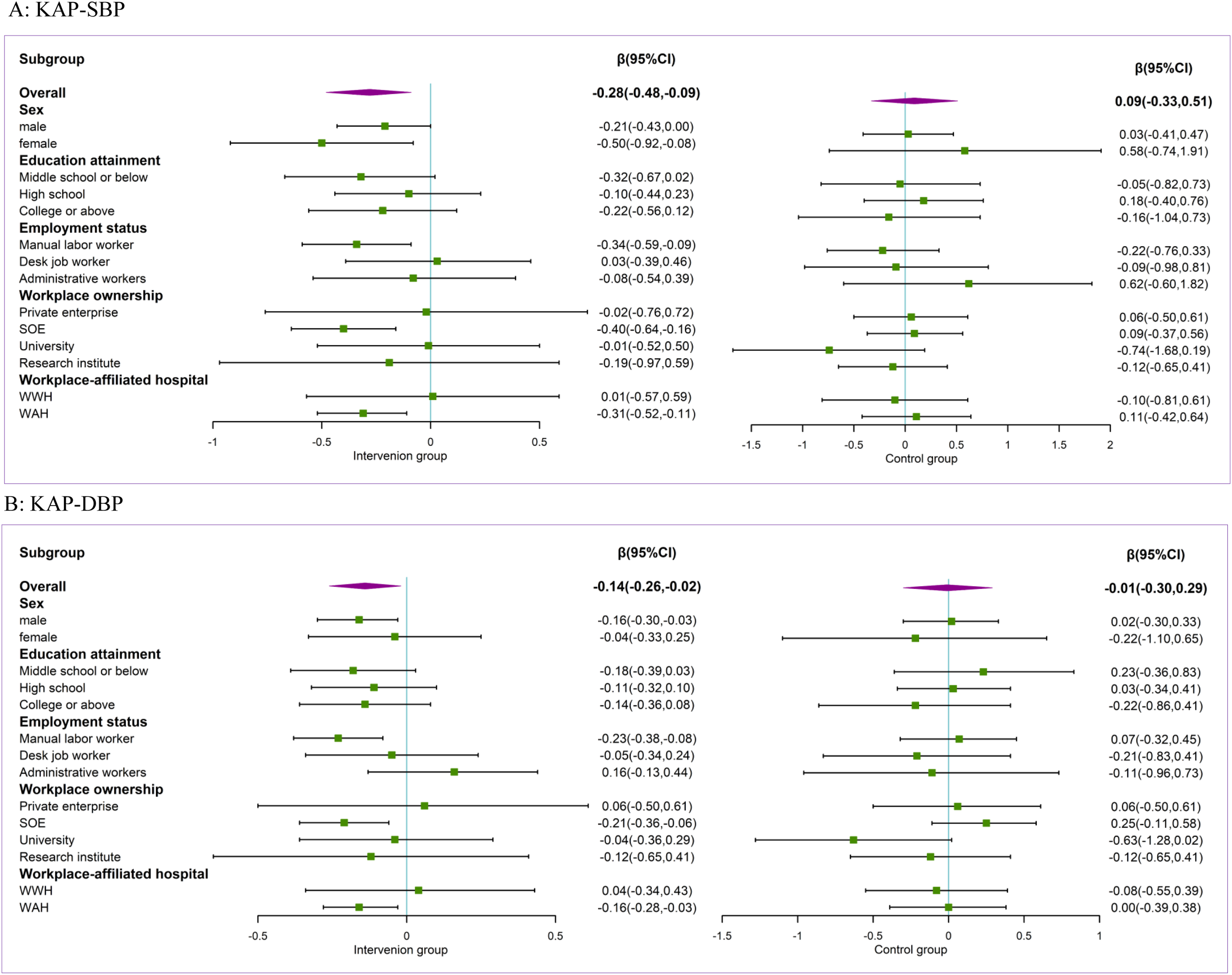
Discussion
In our study, we found that compared with the control group, the KAP overall qualified rate was significantly increased in the intervention group after 2-year intervention, and the qualified rate of almost all items in the KAP questionnaire were significantly increased, indicating a significant intervention effect. Increased KAP score was significantly associated with SBP and DBP control.
We found that the qualified rate of almost all items in the KAP questionnaire was significantly increased in intervention group. It may be attributed to our hypertensive management program based on guidelines, which covers the popularization of health education, the promotion of healthy environment, regular follow-up treatment to promote employees to master the hypertension-related knowledge, develop healthy lifestyle, seek medical treatment and take medication regularly to control BP. Prior finding also showed that an individual-level randomized controlled study of a 2-year comprehensive workplace wellness program significantly improved employee beliefs about their own health. 22 The comprehensive intervention can effectively improve the KAP level of the hypertension in community. 23 These results complement recent RCT evidence that workplace wellness programs affect hypertension-related KAP outcomes. However, in some items of KAP, such as “major complications of hypertension”, “low-salt diet”, “low-fat diet”, “less work/life stress”, and “regular exercise”, the qualified rate was still low, less than 55%. It is suggested that the above aspects should be taken as the focus of intervention, strengthen the health education in view of the problems in these aspects, and eliminate the blind spots in health education of hypertension prevention and control.
The improvement of KAP score was significantly associated with BP control. So far, few studies have used longitudinal data to explore the association between the improvement of KAP and BP control and our study provides results complement evidence. This result suggests that hypertension patients with good behaviors related to the prevention and treatment of hypertension may have better self-management ability and thus better BP control. For intervention on hypertension patients may be based on the popularization of health knowledge, improve the patients’ understanding level on the influence factors of hypertension control and self-management behavior, set up the right attitudes and beliefs for treatment of hypertension, understand the importance of self-management behavior, promote the formation of healthy behavior, so as to effectively control BP level and play the real value of intervention. Studies have also shown that active and effective self-management can improve BP control and significantly reduce the incidence and mortality of heart, brain, kidney and other diseases in hypertensive patients.24,25
In addition, the improvement of knowledge dimension, attitude dimension and behavior dimension were gradually strengthened in relation to BP control. This is consistent with previous knowledge. Hypertension knowledge, awareness, and self-management behaviors affect hypertension control. 26 According to KAP theory, the change of human behavior is divided into three continuous processes: knowledge acquisition, belief generation and behavior formation, and KAP should be positively related. 27 Knowledge affects behavior through attitude. Only when patients master hypertension related knowledge and establish positive and healthy beliefs and attitudes, can they take the initiative to form healthy behaviors. 28
Subgroup analysis showed that the intervention effect of KAP qualified rate and the association strength between the improvement of KAP score with BP control were most significant in manual labor workers, workers from SOE and WAH. In China, manual labor workers belong to blue-collar class, such as manufacturing and mining. According to the National Bureau of Statistics, 55 percent of blue-collar workers had a junior high school education and was lower than the national average. 29 In addition, the studies found that the lower the educational attainment, the lower the level of health literacy.30-32 Therefore, the net benefit of intervention may be greater for workers with less education. In addition, with more economic and human resources, it was easier to launch and mobilize workplace health interventions in SOE. Employees from WAH were more likely to have access to more medical resources and health care services. This suggests that health intervention targeted at the characteristics of employees should become an important part of Worksite Health Promotion Programs.
Limitation
This study has several limitations. First, in the investigation of “work and life stress”, the questionnaire items are relatively rough, so it may be inaccurate to infer the stress status of occupational population. In the future, we can consider the application of job content scale for accurate assessment. Second, questionnaire data were only collected at baseline and the end of follow-up for the intervention and control groups, making it difficult to assess change trends of KAP during the intervention. Thirdly, our study was conducted a decade ago, which may have an impact on the timeliness of the results. However, a review of previous literature found that little attention has been paid to the association between the change of hypertension preventive KAP and BP control in occupational population using longitudinal data. Therefore, our results can provide reference and enlightenment for research in related fields to some extent. Finally, compared to the perfect 1:1 intervention-to-control ratio, we adopted another common 2:1 randomized control design considering that the intervention purpose of our study is to benefit more participants.33,34 It is undeniable that this design method may have some limitations, such as, the results may be biased due to the imbalance of the number of people in the two groups. However, the advantages of our design also obvious, with a larger sample size allowing for more efficient assessment of intervention effect and improving reliability of results. At the same time, the literatures from our team based on this research design has also been recognized and published in relevant professional journals.18,35 In fact, the design of cluster sampling cannot control the sex ratio of participants, resulting in the problem of gender imbalance in our study, and the generalization of the results may be limited. In the future study, we will actively follow up the latest data and literature, pay attention to the design of intervention-to-control ratio strictly following the characteristics of randomized controlled trials to make our study results more reliable and generalizability. In addition, we will optimize the study design to further measure the effect of enhancing practice on hypertension control based on clarifying the effect of improving knowledge and attitude score on practice, so as to make the design more scientific and rigorous.
Conclusion
Findings of our study suggested that a workplace-based multicomponent hypertension intervention program is effective in enhancing hypertension patients’ hypertension-related health knowledge, establishing correct treatment attitudes and adopting healthy practices. In addition, the improvement of KAP in hypertensive patients was significantly associated with BP control. Such intervention strategy may be considered for application in other types of workplaces in China and other countries.
Supplemental Material
Supplemental Material - Association Between the Improvement of Knowledge, Attitude and Practice of Hypertension Prevention and Blood Pressure Control-A Cluster Randomized Controlled Study
Supplemental Material for Association Between the Improvement of Knowledge, Attitude and Practice of Hypertension Prevention and Blood Pressure Control-A Cluster Randomized Controlled Study by Zhen Hu, Xin Wang, Congyi Zheng, Linfeng Zhang, Xue Cao, Yixin Tian, Runqing Gu, Jiayin Cai, Ye Tian, Lan Shao, and Zengwu Wang, MD, PhD in American Journal of Health Promotion
Footnotes
Acknowledgments
This study was accomplished through the fine work of the staff at the national level, we thank all of colleagues involved in the survey.
Author Contributions
Concept and design: Z. Wang, Wang.
Acquisition, analysis, or interpretation of data: All authors.
Drafting of the manuscript: Z. Hu, Wang.
Critical revision of the manuscript for important intellectual content: Z. Wang.
Statistical analysis: Z. Hu.
Data curation: L. Zhang, Zheng.
Investigation: X. Cao, Tian, Cai, Gu, Tian, Shao.
Obtained funding, supervision: Z. Wang.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by grant 2011BAI11B01 from the Projects in the Chinese National Science and Technology Pillar Program during the 12th Five-year Plan Period and by grant 2017-I2M-1-004 from the Chinese Academy of Medical Science Innovation Fund for Medical Sciences.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.