
Abstract
Purpose
Examine trust in sources of COVID-19 information and vaccination status.
Design
Cross-sectional.
Setting
Chicago, Illinois.
Subjects
Convenience sample of 538 Black adults surveyed between September 2021 and March 2022.
Measures
Trust in sources of COVID-19 information, COVID-19 vaccination.
Analysis
Using latent class analysis, we identified classes of trust in sources of COVID-19 information. We considered predictors of class membership using multinomial logistic regression and examined unadjusted and adjusted associations between trust class membership and COVID-19 vaccination while accounting for uncertainty in class assignment.
Results
Our analytic sample (n = 522) was predominantly aged 18-34 (52%) and female (71%). Results suggested a four-class solution: (1) low trust, (2) high trust in all sources, (3) high trust in doctor and government, and (4) high trust in doctor, faith leader, and family. Unadjusted odds of vaccination were greater in the high trust in all sources (OR 2.0, 95% CI 1.2-3.2), high trust in doctor and government (OR 2.7, 95% CI 1.4-5.3), and high trust in doctor, faith leader, and family classes (OR 2.1, 95% CI 1.2, 3.9) than the low trust class. However, these associations were not significant after adjustment for sociodemographic and health status factors.
Conclusion
Although COVID-19 vaccination varied across trust classes, our adjusted findings do not suggest a direct association between trust and vaccination, reflecting complexities in the vaccine decision-making process.
Purpose
The COVID-19 pandemic has highlighted and exacerbated stark racial and ethnic health inequities in the US. This is particularly true for Black Americans, who were more likely to be hospitalized or die from COVID-19 than white Americans during the initial stage of the pandemic.1,2 These inequities were dynamic over time, highlighting unequal access to and uptake of life-saving interventions, including the COVID-19 vaccine. For example, Black Americans were 2.6 times more likely to be hospitalized with COVID-19 than white Americans during the Omicron variant wave in January 2022, 1 months after vaccine eligibility had been expanded to all adults.
Although the rapid development of the COVID-19 vaccine during the pandemic was a remarkable achievement, vaccine rollout was inequitable. Black and Hispanic communities were less likely to have distribution sites during the initial vaccine rollout,3-5 which likely worsened racial/ethnic inequities in preventable COVID-19 deaths. 6 Inequities in COVID-19 vaccine coverage at the national level have since narrowed, 7 potentially due to the increased adoption of disadvantage indices, such as the Centers for Disease Control and Prevention Social Vulnerability Index, 8 by public health jurisdictions as a way to more equitably distribute vaccines. 9 Nevertheless, non-Hispanic (NH) Black individuals continue to have the lowest COVID-19 vaccination coverage in many large cities throughout the US, including New York, Los Angeles, and Detroit.10-12 In Chicago, only 57% of NH Black residents had completed their primary vaccine series as of November 2023, compared to 70% of NH white residents, 72% of Hispanic residents, and 79% of Asian residents. 13 These persistent disparities suggest that addressing vaccine access is necessary, but not sufficient, to increase vaccine uptake in the Black community.
Based on research prior to the pandemic, trust in the institutions that produce and promote vaccines, including the government and medical establishment, can impact vaccine hesitancy and behaviors.14,15 Qualitative research on influenza vaccination with Black and white participants in Washington DC suggests that confidence and trust in the vaccine may be more important than access in determining vaccine uptake. 14 A history of egregious medical mistreatment of Black individuals in the US,14,16 along with continued racism in the health care system, 17 fuels medical mistrust in the Black community today. In a 2015 national survey, Black Americans had lower levels of trust in the influenza vaccine than white Americans, as well as less trust in the Centers for Disease Control and Prevention and Food and Drug Administration, who are heavily involved in the vaccine approval and promotion process. 15
Trust in the institutions producing vaccines becomes acutely important during a pandemic. There is a small but growing body of evidence that trust in specific sources of COVID-19 information, including the government and health care providers, is associated with COVID-19 vaccine uptake in the general population.18,19 Additionally, qualitative findings suggest that mistrust in the government and medical institutions may partially explain the persistent Black-white inequities in COVID-19 vaccination in large urban cities. 20 However, we are only aware of 1 study that empirically examines associations between trusted sources of COVID-19 information and COVID-19 vaccine uptake by race/ethnicity. 18 To build on these preliminary findings, our objectives were to (1) examine trust in sources of COVID-19 information, including how trust in multiple sources may cluster together; (2) assess sociodemographic and health-related predictors of trust profiles; and (3) examine associations between trust profiles and COVID-19 vaccine uptake using a sample of Black adults in Chicago. Findings can be used to better understand trust in sources of health information in the Black community and whether levels of trust influence health behaviors, including COVID-19 vaccination.
Methods
Sample
We recruited a convenience sample of Black adults to take an online survey about COVID-19 behaviors and beliefs. Recruitment methods included word-of-mouth, community events, and social media. We screened potential respondents via telephone to ensure they were eligible for the study, including (1) being 18 years of age or older, (2) self-identifying as Black or African American, and (3) living in Chicago, Illinois for at least 3 months. A total of 538 eligible adults provided informed consent and completed the survey between September 2021 and March 2022 using a personalized REDCap link shared by text or email. Participants received a $50 incentive for completing the survey. All study protocols were approved by the Institutional Review Board at the Medical College of Wisconsin.
Measures
We used the following question from the National Institutes of Health RADx-UP Common Data Elements 21 to measure trust in sources of COVID-19 information: “How much do you trust each of these sources to provide correct information about COVID-19?” Respondents provided their level of trust using a Likert scale (not at all, a little, somewhat, a great deal) for these sources of COVID-19 information: your doctor or health care provider; your faith leader; your close friends and members of your family; people you go to work or class with or other people you know; news on the radio, TV, online, or in newspapers; your contacts on social media; the US government; and the US Coronavirus Task Force.
We measured vaccination status, our primary outcome, with the question: “Have you received a COVID-19 vaccine?” We included sociodemographic covariates that may influence levels of trust and COVID-19 vaccination status, including age group (18-34; 35-54; 55+), self-identified gender (woman; man), and annual household income (<$5000; $5000-$24,999; $25,000+). For our binary measure of gender, we considered respondents self-identifying as women (including transgender women, n = 1) as women and respondents self-identifying as men (including transgender men, n = 1) as men. Respondents identifying as non-binary or another gender category were set to missing (n = 8). For income, we selected cut points to reflect the predominantly low-income status of the sample. Additional covariates that may influence levels of trust and vaccination status included educational attainment (less than high school degree; high school degree/GED; some college or more), marital status (never married; married; divorced, widowed, or separated), employment status (employed; unemployed, including temporarily; retired, disabled, keeping house, student, or other), health insurance coverage (uninsured, private, public, other/don’t know), number of diagnosed physical health conditions (0, 1, 2+), and diagnosed mental health condition (yes/no). Diagnosed physical conditions included a count of the following self-reported diagnoses: immunocompromised condition, autoimmune disease, hypertension, diabetes, chronic kidney disease, cancer diagnosis/treatment in the past 12 months, cardiovascular disease, asthma, COPD, other chronic lung disease, sickle cell anemia, and other chronic condition. Diagnosed mental health condition was based on self-reported diagnosis of depression or ‘other mental health disorder.’
Analysis
We performed descriptive analyses in SPSS Version 28 22 using the full Likert scale to examine levels of trust in sources of COVID-19 information. To characterize classes of trust, we used a stepwise approach with latent class analysis (LCA) and subsequent regression models in which we dichotomized the response options for levels of trust (not at all and a little vs somewhat and a great deal). In step 1, we used LCA to identify classes based on levels of trust in the 8 sources of COVID-19 information included in our survey, fitting a series of models specifying 1-6 latent classes in Mplus 8. 23 We determined the optimal number of classes using standard fit indices, including the Bayesian Information Criterion (BIC) and the sample size-adjusted BIC (Adj. BIC), which are smaller for models with better fit; the adjusted Vuong-Lo-Mendell-Rubin likelihood ratio test (VLMR-LRT), which tests for an improvement in fit for each model vs the model with 1 fewer class; and the entropy, which assesses the extent to which classes are distinct from one another. 24 We also considered the interpretability of different classes.
Following the selection of the optimal class solution, in step 2, we added the outcome variable (COVID-19 vaccination) into the model as an additional classification variable to assess differences in vaccination across latent classes. During this step, we assessed potential shifts in LCA profiles and found that the same class profiles were maintained as in step 1, with the same percentages of the sample in each class. In step 2, we used unadjusted odds ratios to compare vaccination across classes. In step 3, we used the R3STEP procedure in Mplus 8 to consider predictors of class membership by including sociodemographic covariates as auxiliary variables. With this approach, the LCA solution from step 2 was retained while predictors of class membership were tested with multinomial logistic regression analyses. 25 We considered individual sociodemographic covariates first, and then combined covariates in a multiple regression analysis. Finally, in step 4, we added sociodemographic covariates into the LCA model as predictors of COVID-19 vaccination and compared adjusted rates of vaccination across latent classes to assess whether differences in vaccination persisted after accounting for covariates. We again assessed whether there were shifts in LCA profiles at this step, finding that the interpretation of classes and the percentage of participants in each class was the same as in steps 1 and 2. Simple and multiple logistic regressions tested sociodemographic predictors of vaccination, and adjusted rates of vaccination were compared by calculating odds ratios. This approach to considering predictors and outcomes accounts for the uncertainty in class assignment and avoids the assumption of perfect classification.
Missing data on latent class indicators (trust variables) was handled using a full-information maximum likelihood (FIML) approach, while missing data on sociodemographic covariates was handled with multiple imputation (MI). These approaches avoid biases associated with complete case analysis. 26 We imputed 100 datasets with all analytic variables included. 27 Analyses were conducted with all 100 datasets, and parameter estimates were pooled using the imputation algorithms in Mplus 8.26,28
Results
Description of the Analytic Sample (n = 522), Chicago, IL, September 2021 - March 2022.

aIncludes immunocompromised condition, autoimmune disease, hypertension, diabetes, chronic kidney disease, cancer diagnosis/treatment in the past 12 months, cardiovascular disease, asthma, COPD, other chronic lung disease, sickle cell anemia, other chronic condition.
bIncludes depression or ‘other mental health disorder.’
Trusted Sources of COVID-19 Information
Trusted sources of COVID-19 information varied by vaccination status (Figure 1). Doctor or health care provider was the most trusted source across the sample, although a higher proportion of vaccinated respondents trusted their doctor ‘a great deal’ (68%) than unvaccinated respondents (43%). Nearly half (47%) of vaccinated respondents and over one-third (37%) of unvaccinated respondents trusted their faith leader ‘a great deal.’ Notably, twice as many vaccinated (42%) vs unvaccinated respondents (21%) reported trusting the US Coronavirus Task Force ‘a great deal.’ Contacts on social media had the lowest levels of trust for both vaccinated and unvaccinated respondents. Trust in sources to provide correct information about COVID-19 by vaccination status for a sample of Black adults in Chicago, IL, September 2021 - March 2022 (percent).
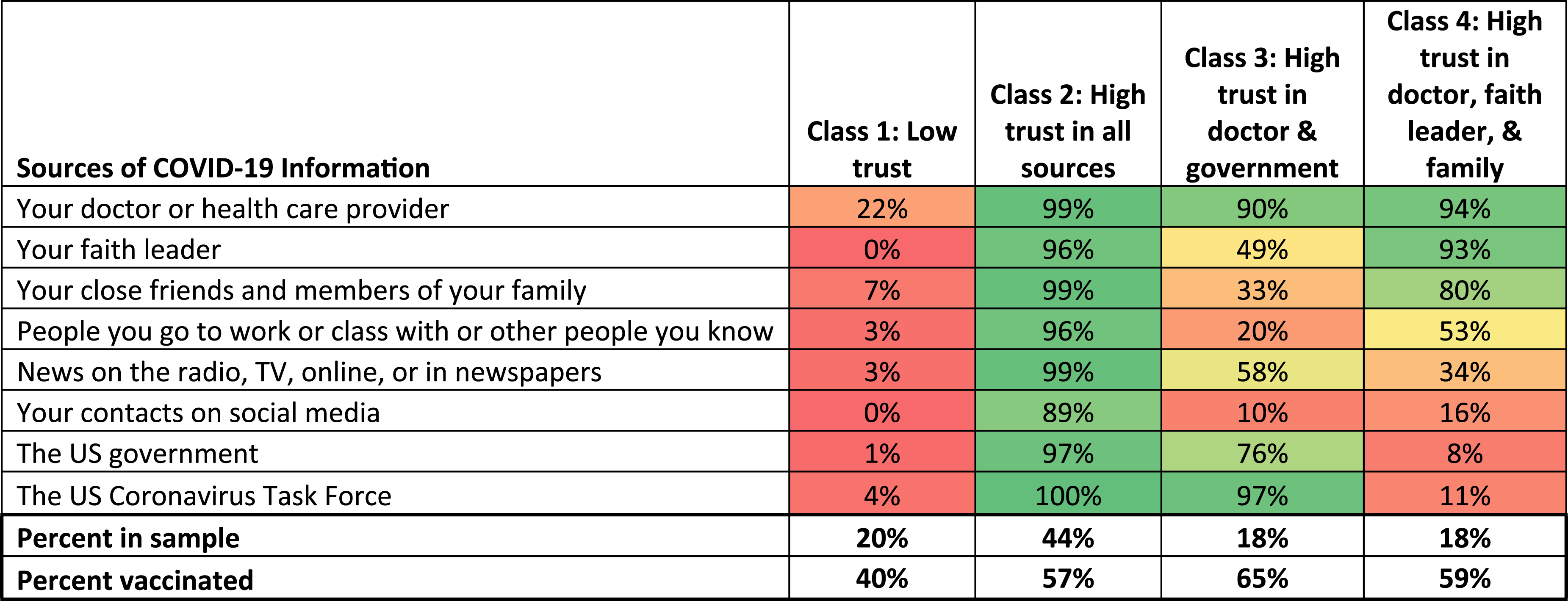
Latent Class Analysis of Levels of Trust in Sources of COVID-19 Information for a Sample of Black Adults in Chicago, IL, September 2021 - March 2022 (n = 522).

Predictors of Trust Class Membership
Multinomial Logistic Regressions Examining Odds of Belonging to a Specific Trust Class (Referent Category: Low Trust), Chicago, IL, September 2021 - March 2022 (n = 522).

Trust Class Membership and COVID-19 Vaccination Status
Logistic Regression Predicting Receipt of COVID-19 Vaccine, Chicago, IL, September 2021 - March 2022 (n = 522).

Discussion
In our sample of over 500 Black adults in Chicago, we identified 4 distinct classes of trust in sources of COVID-19 information: low trust, high trust in all sources, high trust in doctor and government, and high trust in doctor, faith leader, and family. Our classes representing low trust or high trust in all sources are somewhat consistent with a study of trusted sources of COVID-19 information in racial/ethnic minority individuals in Florida, which identified a low, medium, and high trust class. 29 However, our results are distinct in that we also identified 2 classes of high trust in specific sources only, representing a more nuanced picture of perceived trustworthiness across a wide range of sources of COVID-19 information.
Despite the differences in levels of trust across the 4 classes we identified, doctor or health care provider had high levels of trust relative to other sources. This is consistent with several studies reporting high trust in doctors as a source of COVID-19 information.18,19,29,30 The probability of trusting one’s doctor was ≥90% in the high trust in all sources, high trust in doctor and government, and high trust in doctor, faith leader, and family classes. Even for the low trust class, the probability of trust in one’s doctor was 22%, compared to probabilities of trust ranging from 0-7% in other sources of COVID-19 information. This finding suggests a critically important role for doctors in serving as a trusted source of information during a health crisis. As discussed by Bassler et al, providing COVID-19 vaccines to doctor’s offices during the initial rollout, in addition to mass vaccination sites, may have “provided opportunities for vaccine-hesitant persons to learn more about the vaccine from their most trusted source of information about COVID-19,” thereby increasing vaccine uptake. 19 More broadly, this finding highlights the importance of building relationships with primary care providers during periods of relative normalcy so that this trusted source is available during health crises.
In terms of the demographic composition of the trust classes, our results align with prior research suggesting that age is an important determinant of trust. 18 In unadjusted models, older (vs younger) respondents had greater odds of belonging to all 3 classes that included high trust in at least some sources, including high trust in doctor and government. However, the direction of this association is somewhat mixed in the literature. One study on the influenza vaccine reported that older Black adults were less trusting of the government, 31 while another study on COVID-19 vaccination reported that older Black adults were more trusting of institutions. 18 These differences may reflect differences across study samples or a potential shift in trust levels within the Black community during the pandemic.
Higher income was associated with greater odds of membership in the high trust in all sources (vs low trust) class in the unadjusted, but not adjusted, model. Income was not associated with class membership for the other trust classes. This is consistent with 1 study reporting no association between socioeconomic indicators (including income and educational attainment) and trust profiles of sources of COVID-19 information among racial/ethnic minority respondents in South Florida. 29 Another study using a national convenience sample found a positive relationship between income and levels of trust in institutions for white, but not Black, respondents, suggesting differences in this association by race. 18
Other factors that are associated with age, including number of physical health conditions and employment status, were also associated with trust class membership in unadjusted models. Apart from the association between older age and membership in the high trust in all sources class, there were not significant differences in class membership after adjustment, suggesting an interrelatedness of these factors (ie, age, physical health conditions, employment). The lack of significant predictors of trust class membership also suggests that we did not capture additional constructs that may inform levels of trust in sources of COVID-19 information, such as political party or religious affiliation. 18
Furthermore, our results suggest complexities in the decision to get vaccinated. COVID-19 vaccination status varied across the trust classes, ranging from 40% in the low trust class to 65% in the high trust in doctor and government class, a relationship that was reflected in the unadjusted models predicting vaccination. This finding is consistent with studies reporting unadjusted associations between trust in sources of COVID-19 information and vaccination behaviors or intentions, including studies with a racially and ethnically diverse sample in South Florida 29 and predominantly white sample in Alabama. 19 However, trust class membership was not associated with vaccination in our adjusted model. Given the relationship between age and both trust class and vaccination status in our sample, the unadjusted association between trust class and vaccination status was likely confounded by age. In fact, age was the strongest predictor of vaccine receipt in our study. This may reflect the prioritization of older adults during the initial vaccine rollout, as well as a higher level of risk aversion among older adults due to poorer health status. The attenuated association between diagnosed physical health conditions and vaccine uptake in our adjusted model suggests a likely association between age and pre-existing conditions.
Our study is not the first to identify an unexpected relationship between trust and vaccination behaviors. In a qualitative study among Black and white adults examining influenza vaccination, although “participants articulated their concerns about influenza vaccines primarily through a lens of trust,” the researchers “observed no clear patterns between expressed trust and influenza vaccine behavior.” 31 Indeed, trust may not operate in ways that can be easily quantified. For example, in a study of Black residents in Washington DC, some participants reported that they traveled outside their neighborhood to receive the COVID-19 vaccine because they did not trust that they would receive the same product in their own neighborhood. 20 For these individuals, lack of trust in the government did not prevent them from getting vaccinated, but instead influenced where they chose to get vaccinated. In the same study, some vaccinated participants described independently researching vaccine safety and efficacy before ultimately deciding to receive the vaccine, regardless of their distrust of the government and medical establishment. As discussed by Jamison et al, 31 these findings suggest that vaccine behaviors are influenced by a complex set of factors and that vaccine uptake itself does not represent a complete lack of vaccine hesitancy.
Additionally, the relationship between trust and vaccination likely evolved over the course of the pandemic and may differ across racial/ethnic groups. In 1 qualitative study with Black, Native American, and Hispanic participants that spanned several states, while lack of trust in the government and pharmaceutical companies was influential earlier in the pandemic (December 2020), participants were more willing to get vaccinated at follow-up (January/February 2021). 32 However, Black and Native American respondents remained more vaccine hesitant at follow-up than Hispanic respondents. Alternatively, a national study found that vaccine hesitancy and refusal declined in Black populations, but remained stabled in white populations, between January and October 2021. 33 Future research should further explore associations between trust and vaccination over time and within multiple racial/ethnic groups, along with additional cultural factors that may influence vaccine status (eg, modeling, peer support, and communication).
Our study has several limitations. First, our survey was cross-sectional, and findings should be interpreted within the context of our data collection dates (September 2021 - March 2022). Second, our findings are based on a convenience sample and have limited generalizability beyond the study sample. Nevertheless, we successfully recruited both young and low-income adults, 2 groups who are historically underrepresented in research studies.34-37 Our diverse sampling strategy, including word-of-mouth, community events, and social media, may have been helpful in recruiting these populations by increasing the perceived trustworthiness of the study. Third, we did not capture information on some discrete factors that may influence vaccine uptake, including employment mandates, or more detailed information on the decision to get vaccinated despite hesitancy or mistrust. These topics are important avenues for future research focused on understanding vaccine behaviors in the Black community.
In conclusion, we found 4 unique classes of trusted sources of COVID-19 information that reflect a high level of discernment in perceived trustworthiness among our sample of Black adults in Chicago. Although COVID-19 vaccine receipt varied across the trust classes, our adjusted findings do not suggest a direct association between trust in sources of COVID-19 information and vaccination. Taken as a whole, this may reflect complexities in the vaccine decision-making process, as well as challenges in quantifying this process. Future research should explore how trust operates as a barrier to or facilitator of vaccination behaviors in the context of other factors that influence the decision to get vaccinated. Trust in the institutions that produce and promote vaccines, including the government and medical establishment, can impact vaccine hesitancy and behaviors. We found 4 unique classes of trusted sources of COVID-19 information that reflect a high level of discernment in perceived trustworthiness among our sample of Black adults in Chicago. However, our adjusted results do not suggest a direct association between trust and COVID-19 vaccination, likely reflecting complexities in the vaccine decision-making process. Our findings suggest that vaccine uptake may not represent a complete lack of vaccine hesitancy. Future research should explore how trust operates as a barrier to or facilitator of vaccination behaviors in the context of other factors that influence the decision to get vaccinated.So What?
What is Already Known on This Topic?
What Does This Article Add?
What Are the Implications for Health Promotion Practice or Research?
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this RADx® Underserved Populations (RADx-UP) publication was supported by the National Institutes of Health under Award Number R21MH122010. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Appendix
Latent Class Analysis Comparison of Class Solutions.
Classes
BIC
Adj. BIC
VLMR-LRT
VLMR-LRT P-Value
Entropy
1
5225.108
5199.714
—
—
—
2
3798.853
3744.892
1456.708
<.001
.901
3
3545.511
3462.981
304.259
<.001
.907
4
3445.97
3334.872
153.141
<.001
.902
5
3470.019
3330.353
31.707
.02
.879
6
3498.711
3330.477
27.144
.19
.887
Our objectives were to examine trust in sources of COVID-19 information, assess predictors of trust profiles, and examine associations between trust profiles and COVID-19 vaccine uptake using a sample of Black adults in Chicago. Our results suggested 4 classes of trust: (1) low trust, (2) high trust in all sources, (3) high trust in doctor and government, and (4) high trust in doctor, faith leader, and family. Before adjustment, odds of vaccination were greater in the high trust in all sources, high trust in doctor and government, and high trust in doctor, faith leader, and family classes than the low trust class. However, these associations were not significant after adjustment, reflecting complexities in the vaccine decision-making process. Future research should explore how trust operates as a barrier to or facilitator of the decision to get vaccinated.