
Abstract
Purpose
To describe healthcare experiences and health outcomes among rural LGBTQ + individuals.
Design
2022 cross-sectional survey.
Setting
Southern Illinois.
Sample
85 individuals.
Measures
Demographics, sexual orientation and gender identity, healthcare experiences, health outcomes.
Analysis
Experiences and outcomes were assessed vs orientation and identity. Distribution comparison was by t-test and chi-square, risk prediction by logistic regression, and significance assumed at P < .050.
Results
By orientation, participants were: 35.3% gay, 16.5% lesbian, and 45.8% bisexual plus; and by identity they were: 49.4% cisgender, 25.9% transgender, and 24.8% other identity. Survey item responses ranged from 95%-99%. Compared to gay men, lesbians and bisexual plus individuals more frequently reported medical bill payment difficulty (58.3% and 57.9% vs 25.0%; P = .020) and more past month days of poor mental health (19.4 and 15.8 vs 10.6; P = .018). Compared to heterosexual and other identity, transgender individuals less frequently reported having a routine medical provider (72.7% vs 92.7% and 95.0%; P = .037) and more frequently reported past healthcare denial (45.5% vs 17.5% and 18.8%; P = .042). Current health was associated with medical bill payment ability (OR = .33, 95% CI = .13-.86) and respectful treatment by healthcare administrators (OR = 3.90, 95% CI = 1.34-11.35) and clinicians (OR = 3.82, 95% CI = 1.39-10.47). Significance of some findings likely limited due to sample size.
Conclusions
Our data describes healthcare experience and health outcome disparities among rural lesbian, gay, bisexual, transgender, queer and other sexual and gender minority individuals, and indicate that clinical experiences directly influence health outcomes.
Purpose
Rural individuals more frequently lack accessible healthcare and have increased morbidity and mortality rates, compared to urban individuals.1–4 Some sexual orientations and gender identities (SOGI) are systematically stigmatized and discriminated against. 5 This is why we see disparities among lesbian, gay, bisexual, transgender, and queer (LGBTQ+) who are more likely to experience health challenges such as decreased healthcare access and satisfaction, reduced rates of preventive screenings, poor physical and mental health, and increased substance use, compared to cis-gender heterosexual individuals.6-9
While disparities have been examined in relation to SOGI and geography, little research focuses on the intersection of SOGI and = and rurality.10-12 This paucity is observed in the lack of data regarding rural LGBTQ + individuals as it compares to urban areas and even their rural cisgender heterosexual peers. Still, at least one study reports that rural LGBTQ + may have worse self-reported health measures than their rural non-LGBTQ + peers. 13
This study explores healthcare experiences among rural LGBTQ + individuals and how they varied by SOGI, and determine how SOGI and health experiences are associated with specified health outcomes.
Methods
Design
Data were obtained from a cross-sectional survey implemented within the 2022 rural Illinois Cohort. This study was approved by the Southern Illinois University School of Medicine Institutional Review Board (protocol #22-140).
Sample
The Cohort consisted of LGBTQ + individuals aged ≥18 years residing in the substantially rural central and southern Illinois.
Measures
All measures were self-reported and included: demographics (age, race, sexual orientation, gender identity); healthcare experiences (insurance status and access; healthcare experiences; and respectful treatment); and four health outcomes (general health, past 30-day physical and mental health 14 ; and life satisfaction 15 ).
Analysis
Descriptive analysis was performed for measures of age, gender identity, sexual orientation, and race. Bivariate analyses (chi-square and ANOVA) examined healthcare measures by gender identity or sexual orientation. Further analyses (logistic and linear regression) was used to derive odds ratios, and compare characteristics and experiences with health outcomes.
Results
There were 85 participants, and all (100%) provided demographic information. The mean age was 42.1 years [s.d.13.7]; 51.2% were assigned male at birth; 95.3% were White race; and 44.7% had completed some graduate school. Sexual orientation was condensed to gay (35.3%), lesbian (16.5%), and bisexual plus (bi+; 45.8%); and gender identity to cisgender (49.4%), transgender (25.9%) and other gender identity (24.8%). Heterosexual and asexual individuals were not retained for orientation-based analyses.
Nearly all participants possessed health insurance and had a primary care provider they saw on a routine basis, though transgender individuals were more likely to report not having a regular primary care provider (27.3%, Table; OR = 4.76, 95% CI = 1.06, 21.37). There was increased difficulty to pay medical bills among individuals who were lesbian (58.3%; OR = 4.20, 95% CI = 1.00, 17.54) and bi+ (57.9%; OR = 4.13, 95% CI = 1.41, 12.05; both vs gay), and other gender identity (68.4%; OR = 4.50, 95% CI = 1.39, 14.49; vs cisgender). Further, transgender individuals were more likely to report past denial of healthcare due to their SOGI (18.8%; OR = 3.92; 95% CI = 1.22-12.66; vs cisgender). Transgender individuals were more likely to report their healthcare provider specifically attempting to be respectful and affirming (OR = 3.62; 95% CI = 1.15-11.36; vs cisgender). Though other differences across SOGI were not significant, the data indicate areas of less-than-optimal experiences, such as: >48% reporting ever avoiding healthcare and ≥25% reporting ever denial of healthcare due to their SOGI; >52% reporting past poor experiences making them consider not returning; and only ∼2/3 reporting being treated with respect by healthcare staff and clinicians (the other ∼1/3 sometimes or no).
Variation in 2022 Illinois Cohort Healthcare Access and Experiences by Sexual Orientation and Gender Identity.
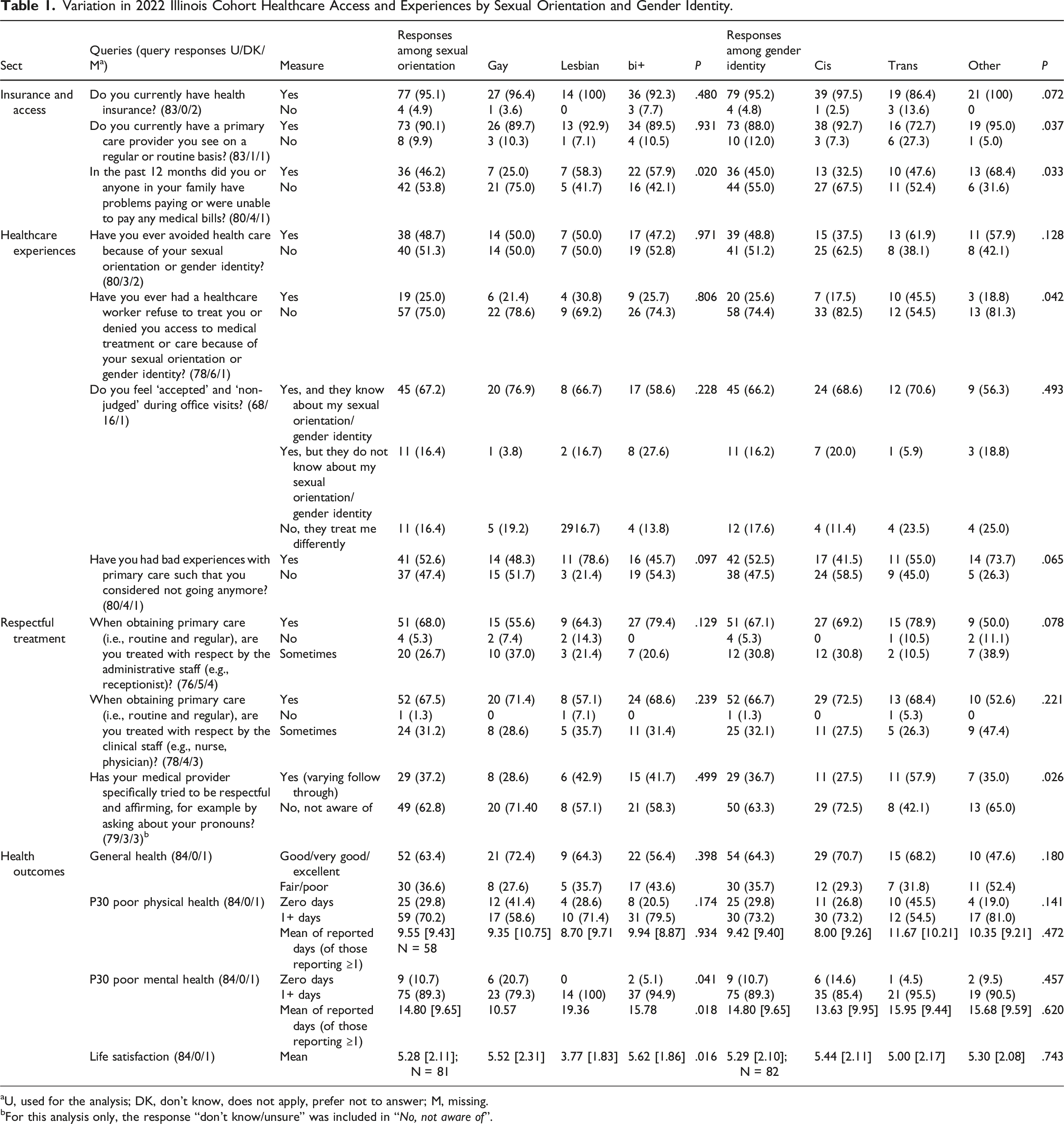
aU, used for the analysis; DK, don’t know, does not apply, prefer not to answer; M, missing.
bFor this analysis only, the response “don’t know/unsure” was included in “No, not aware of”.
SOGI and healthcare access and experiences were associated with the four health outcomes above. The variables associated with current fair/poor health included no past difficulty paying bills (OR = .33, 95% CI = .13, .86), and only sometimes feeling respected by administrators (OR = 3.90, 95% CI = 1.34, 11.34) and clinicians (OR = 3.82, 95% CI = 1.39, 10.47). Age was associated with zero vs 1 + P30 poor mental health (OR = .93, 95% CI = .88-.98). No variables were significantly associated with P30 physical health or life satisfaction.
Discussion
Summary
The 2022 rural Illinois Cohort recruited 85 LGBTQ + individuals across (largely rural) central and southern Illinois with a wide diversity of age, sexual orientation and gender identity. We observed several healthcare access and experience differences by SOGI (e.g., medical bill payment difficulty among lesbians; healthcare denial among transgender individuals), and several poor experiences consistent across SOGI (e.g., approximately half reporting past healthcare avoidance due to their SOGI). We found that lesbian individuals reported more days of poor mental health and less life satisfaction. Finally, current health was associated with medical bill payment ability and occasional respectful treatment by healthcare administrators and clinicians.
Limitations
There are limitations to this work. First, sample set is relatively modest (85 participants). As this may diminish analytical power, it also reaffirms the importance of our significant findings. Second, the sample is generally highly educated. As such, participants may be more likely to be self-advocates and selective consumers that have the capacity to find and manage care that is respectful and affirming. Thus, our results of poor experiences may underestimate the experience of LGBTQ + as a whole. Finally, the sample is almost entirely White race, preventing analyses of specific healthcare disparities and stigma associated with minoritized race and ethnicities. Again, the data regarding healthcare experiences and outcomes may thus underrepresent that which may be found in a larger group of LGBTQ+.
Significance
The data suggest both strong motivation and direction for addressing health disparities among rural LGBTQ+. The extant literature has described disparity healthcare-related treatment and satisfaction among LGBTQ + generally, and in our sample, we find that (a) these are reaffirmed for a rural population and (b) significantly associated with specific health outcomes. This suggests that both formal medical education and continuing professional education should make specific, consistent, and long-term efforts to provide cultural competency training to all in healthcare. The modest size of this work may serve to reinforce the significance of some finding, and point the way to specific interventions and further work. Needs assessments should be conducted to inform locally-specific interventions. There are significant health disparities across geography and SOGI. There are significant health disparities among rural LGBTQ + which are associated with treatment in healthcare. Continuing research and training should further examine the intersection of rurality and LGBTQ + status, its influence on health outcomes, and how providers may better care for such patients.SO WHAT?
What is already known on this topic?
What does this article add?
What are the implications for health promotion practice or research?
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by a grant from Blue Cross/Blue Shield of Illinois, and the study sponsor had no role in study design; collection, analysis, and interpretation of data; writing the report; or the decision to submit the report for publication.