
Abstract
Purpose
Examine possible message topics to promote rural vaccination using psychosocial antecedents of vaccination.
Design
Cross-sectional survey administered by Research America, Inc.
Setting
West Virginia (WV).
Sample
756 WV adults via convenience sample (n = 370; ∼2% response rate from online panel of ∼20 000 WV residents), and random digit dial of landlines (n = 174; ∼1% response rate from 18 432 numbers) and cellphones (n = 212; ∼1% response rate from 20 486 numbers).
Measures
Outcome measures included self-reported vaccination intention and behavior. Predictor measures, rooted in theories of social and behavioral science that have been found to be predictive of vaccination outcomes (i.e., Reasoned Action Approach, Extended Parallel Process Model), included perceived severity and susceptibility, negative affect, instrumental and affective attitudes, social norms, self-efficacy, response efficacy, and perceived control.
Analysis
Multivariate linear regression for intention and logistic regression for behavior.
Results
Intention was positively predicted by affective attitude, β = .30, P < .05, instrumental attitude, β = .19, P < .05, response efficacy, β = .19, P < .05, negative affect, β = .16, P < .05, self-efficacy, β = .13, P < .05, and subjective norm, β = .13, P < .05, F(10, 267) = 30.12, Adj. R2 = .53. Vaccination status was predicted by instrumental attitude, exp(B) = 2.09, and subjective norm, exp(B) = 2.00, Pseudo R2 = .29, log likelihood = 125.11, χ2(10) = 38.34, P < .05. Promising message targets were instrumental attitude, M = 3.21, SD = 1.46, and subjective norms, M = 3.76, SD = 1.71.
Conclusion
COVID-19 vaccine confidence messages should address (1) positive feelings and safety perceptions, (2) vaccination’s effectiveness in preventing serious COVID-19, and (3) subjective vaccination norms.
Keywords
Purpose
Vaccination is effective at reducing severe disease, hospitalization, and death from COVID-19.1,2 Vaccines have been available in the U.S. since December 2020 to varying degrees, 3 but vaccination rates have slowed while COVID-19 remains a global crisis.4,5 One explanation for lower vaccination rates is “vaccine hesitancy,” which the WHO defines as “the delay in the acceptance or refusal to vaccinate despite the availability of vaccine services.” 6 Common reasons for “hesitancy” include reluctance toward vaccines, concerns about safety, belief that vaccines are ineffective, lack of trust in government recommendations and/or medical advice, and believing one’s existing or disease-induced immunity is superior to vaccination.7,8
Rural U.S. residents are particularly less likely to get vaccinated.9,10 Vaccine hesitancy in rural communities has been linked to factors such as cultural conservatism, government distrust, and health literacy.11-14 This is particularly concerning as COVID-19 mortality rates are pronounced in rural areas. 15
That being said, social and behavioral research tends to not include rural populations and especially those within the Appalachian Region, 16 While some research provides insight into potential reasons for vaccine hesitancy, less is known about motivators of vaccine uptake and confidence. This study addresses this gap by building on vaccine perceptions research while exploring motivators for COVID-19 vaccination among rural Appalachian residents. Based on such insights into West Virginians’ vaccine decision-making, recommendations for rural vaccination promotion messaging will be provided.
Public health and communication science commonly leverage theories such as the Theory of Planned Behavior and the Health Belief Model to explain behavior and plan interventions. These theories have evolved over time to become more informative in guiding health-related decision-making and in strategic communication to promote behaviors like vaccination. Communication science researchers have developed a validated approach for pinpointing impactful topics for persuasive health messaging, informed by such theories, based on their predictive ability. Health intervention messages consist of a topic (e.g., benefits of vaccination), structural features (e.g., audiovisual components or imagery), and actual linguistic content. 17 To inform messaging content that affects decision-making, a data-driven method was developed to identify statistical predictors of the motivation or intention to enact a given behavior, such as vaccination.18-20 Intervention planners use regression analyses with theory-informed predictors to identify statistically significant associations with intention. This is followed by assessment of relative strength or magnitude across predictors and their descriptive statistics to identify which are subject to movement in the desired direction through messaging.
The logic of this approach is that messaging can strengthen or weaken an audience’s endorsement of behavior-related beliefs (e.g., the perceived safety of vaccination). Focusing messaging on beliefs that are not deeply entrenched and have a strong (potentially causal) association with behavioral intention should result in subsequent movement in intention. Intentions are a consistent predictor of actual behavior, such as vaccination. Thus, shifting beliefs that are associated with intention should prompt behavior change. This approach has been validated with experimental study wherein exposure to persuasive pro-social messages informed by quantitative data led to comparatively stronger message-consistent beliefs. 19 This suggests that such an approach can help identify pro-vaccination messaging topics for interventions.
This data-driven method for identifying the topics of public health messaging typically draws from predictions of the Reasoned Action Approach (RAA),20,21 which is the most recent iteration of the Theory of Planned Behavior. The RAA is also called the “Integrated Behavioral Model” or “Integrative Model.” 22 This paper refers to the model as the original Theory of Reasoned Action theorists do in their paper outlining the current state of the model. 21 Yet, in the realm of vaccine decision-making, guidance often comes from the concept of vaccine hesitancy. The most complete conceptualization of vaccine hesitancy comes from the 5C Model of Vaccine Hesitancy. 23 The “5C’s” include confidence (i.e., trusting a vaccine’s effectiveness and safety), constraints (i.e., personal barriers like limited availability and affordability), complacency (i.e., believing one is at low/minimal risk of the disease), calculation (i.e., seeking and considering vaccination information), and collective responsibility (i.e., willingness to shield others from disease and being influenced by normative pressure). Since these concepts are not concrete psychosocial constructs, they are not as informative for translation. However, theories and models used in public health and communication science map well onto “vaccine hesitancy.”
It is imperative to assess these decision-making processes in general to improve the public health communication approaches to increasing vaccination rates, and especially important in rural contexts. 6 Meta-analyses of factors influencing vaccine decision-making suggest some psychological constructs consistently predict intentions to vaccinate, 24 though findings are limited by theoretical scope, national 25 rather than population-specific samples (e.g., limited inclusion of rural regions and especially Appalachian subregions), 16 as well as a limited focus on ongoing pandemic and specifically COVID-19 dynamics. More pragmatically, data collected since the beginning of the COVID-19 pandemic suggest rurality is associated with reduced rates of COVID-19-specific precautions such as mask-wearing, 14 and a history of reduced vaccination rates both in general 26 and especially for COVID-19 vaccination. 5 At the time of this study’s initiation, approximately 57% of the state of West Virginia (WV), a predominately rural state, received at least one dose of a COVID-19 vaccine, 27 compared to approximately 77% of the U.S. population. 28 To further demonstrate the rural-urban disparities in vaccination, WV counties that are considered “rural” (i.e., fewer than 50 000 residents) 29 had a vaccination rate of approximately 54% while urbanized counties had a vaccination rate of approximately 60%.
A theoretical model reflecting vaccine hesitancy that is often used to focus pro-social messaging is the RAA. 21 The RAA argues that a behavior is predicted by a person’s intention or motivation to enact that behavior, which is shaped by a combination of a person’s attitude (reflecting the 5C Model’s “confidence”), perceived social norms (reflecting the 5C Model’s “collective responsibility”), and perceived efficacy (reflecting the 5C Model’s “constraints”). More specifically, the RAA would predict a person’s intention to get vaccinated is predicted by their affective attitude toward COVID-19 vaccination (i.e., positive or negative emotions associated with vaccination), instrumental attitude (i.e., the perceived consequences or outcomes of vaccination), subjective norm (i.e., pressure perceived from one’s network about whether they should get vaccinated; Park & Smith, 2007), 30 descriptive norm (i.e., how much a person believes their network has gotten or plans to get vaccinated), perceived behavioral control (i.e., the control a person believes they have over getting vaccinated), and, finally, self-efficacy (i.e., a person’s comfort or confidence in getting vaccinated).
The RAA predicts the above perceptions that are positively associated with intention. As such, public health messaging that influences any of these beliefs should also alter a person’s intention to get vaccinated. Meta-analyses suggest these constructs are associated with vaccination intention, 24 though, again, this has been less studied in the rural, and especially Appalachian context, and particularly regarding COVID-19 vaccination. Cross-sectional data analysis can empirically identify exactly which belief(s) the messages should target.
Much of the rest of what “vaccine hesitancy” speaks to can be found in the EPPM. This model suggests that risk-reducing behaviors (e.g., vaccination to reduce disease burden) are predicted by how much a person believes their health and well-being are threatened and the efficacy of precautionary behaviors. 31
Threat perceptions in the EPPM include perceptions of severity and susceptibility, and experiences of negative affect. Perceived severity refers to how serious a person believes the consequences are of some risk or disease. The more a person believes a disease like COVID-19 is serious and has harmful consequences to their wellbeing, the more likely they will be to take action to protect themselves. Perceived susceptibility, on the other hand, is defined as how likely a person believes they are to experience a risk like COVID-19. The more someone believes they are likely to develop COVID-19, the more likely they will be to take action to protect themself. Finally, negative emotions such as fear and worry act as motivational drives to enact risk-reducing behavior. 32 Perceived threat, overall, resembles the 5C Model’s “complacency” dimension, in that when threat perceptions for a disease are low, vaccination is unlikely.
The EPPM also includes efficacy perceptions in the prediction of risk-reducing behavior. Perceived efficacy refers to how much a person believes they can control and prevent an unfavorable consequence like COVID-19. It consists of 2 dimensions: self-efficacy and response efficacy. 31 Self-efficacy reflects the same component of the RAA explained above. Response efficacy is the confidence a person has that a behavior like vaccination can protect them from a risk like COVID-19. Response efficacy, similar to the RAA’s attitude constructs, reflects “confidence” from the 5C model and may be a useful message target.
In all, to influence COVID-19 vaccination outcomes, effective message strategies for conveying information that encourages the public to pursue vaccination much be identified. One way to do so is by examining what factors strongly predict vaccination motivation and appear to be flexible and thus able to be shifted using public health messaging. This study attempts to achieve this by examining factors analogous to “vaccine hesitancy” and identify which beliefs predict vaccination intention. Thus, the following research question is explored:
Which beliefs are best suited for targeting with strategic messaging to increase COVID-19 vaccination intention?
Method
Design and Sample
A cross-sectional survey, approved by the authors’ university IRB, was administered January 19 to 31, 2022, shortly after the omicron variant of the virus that causes COVID-19 was labeled as a variant of concern, 33 by Research America, Inc. The survey was conducted online (convenience sample from Research America’s online panel of ∼20 000 WV residents; n = 370, ∼2% response rate) and via a combination of random digit-dialed landline (n = 174, ∼1% response rate from 18 432 random landlines) and mobile phone interviews (n = 212, ∼1% response rate from 20 486 random cellphones). Participants were required to be WV residents at least 18 years of age. After being recruited, participants reviewed a digital informed consent form and indicated their willingness to participate. Participants had the opportunity to not answer any questions or end their participation at any time. No personally identifiable information was connected to the dataset or provided to researchers.
Measures
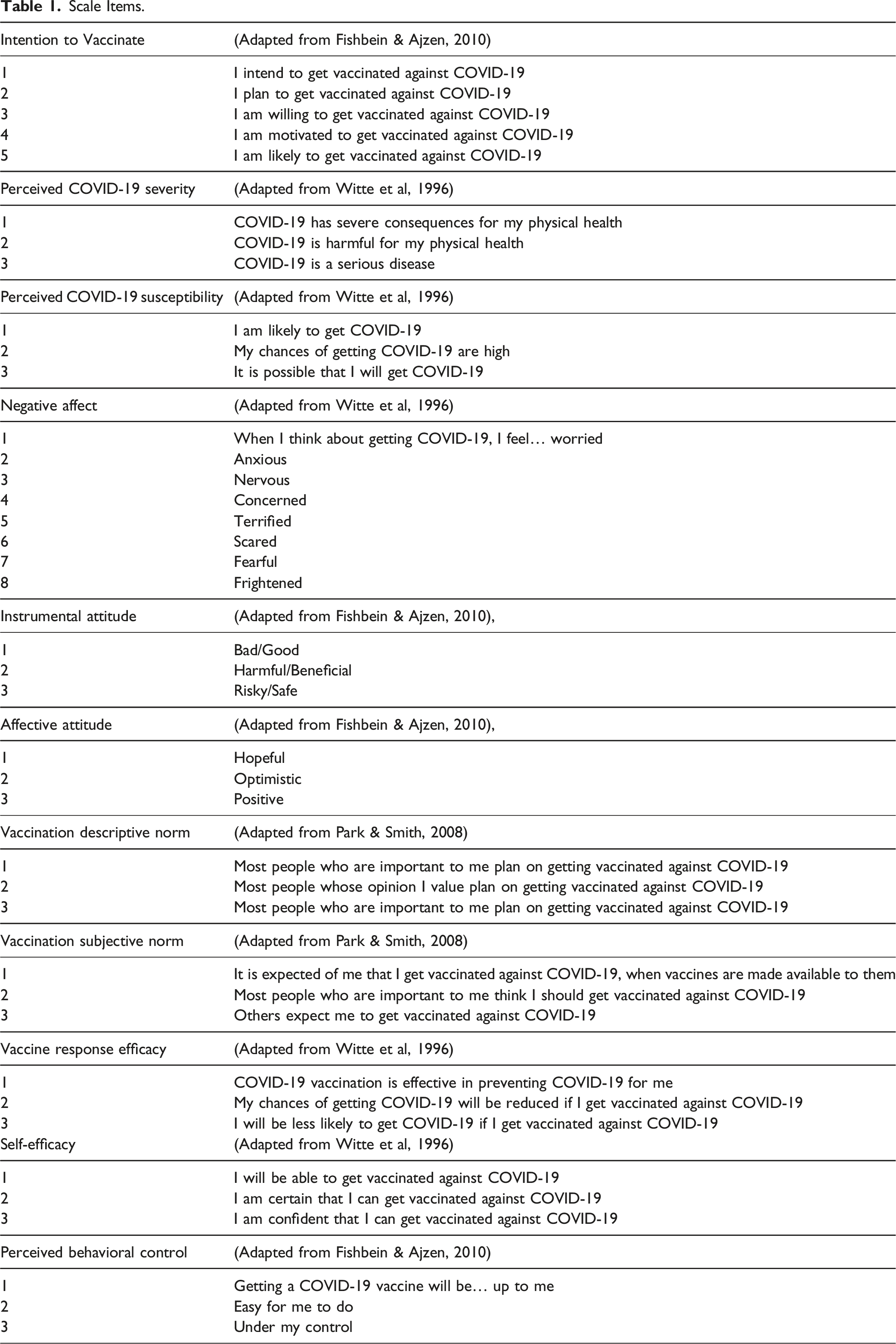
Scale Items.
Outcome Variables
COVID-19 vaccination intention 21 (α = .96) was measured with 5 items asking individuals about their plans to get vaccinated (e.g., “I intend to get vaccinated against the virus that causes COVID-19”). This measure follows standard language of other intention measures that only replace the object (i.e., “against the virus that causes COVID-19”). Meta-analyses have demonstrated that such changes translate to subsequent changes in actual behavior. 34
Then, vaccination behavior was collected with via self-reported vaccination status (1 = “Fully vaccinated (2 doses of an mRNA vaccine or a single dose of the Johnson & Johnson vaccine) and a booster shot,” 2 = “Fully vaccinated (2 doses of an mRNA vaccine or a single dose of the Johnson & Johnson vaccine) but no booster shot,” 3 = Partially vaccinated (1 dose of an mRNA vaccine),” or 4 = “Not vaccinate (no COVID-19 vaccine doses received)”), that included all medically-accurate vaccination options available at the time of data collection. These options were additionally reviewed and approved by members of the State of WV’s COVID-19 Medical Advisory Board. Parenthetical descriptions represented the common nomenclature from the CDC to depict vaccination status to the public at the time. This was transformed into a binary variable (1 = “Received any vaccine dose(s),” 0 = “Unvaccinated”).
COVID-19 Vaccination Attitude
COVID-19 vaccination attitudes were measured on 2 dimensions: instrumental attitude and affective attitude. 21 Instrumental attitude was measured using four 7-point semantic differential items (α = .95) indicating the general safety and usefulness of vaccination (e.g., 1 = Harmful, 7 = Beneficial). Affective attitude was measured with three 7-point Likert-type items (α = .93) that assessed positive emotions toward COVID-19 vaccination (e.g., Hopeful).
COVID-19 Vaccination Social Norms
Social norms were measured on 2 dimensions: descriptive and subjective. 31 Descriptive norms (α = .95) were measured with 3 items (e.g., Most people who are important to me plan on getting vaccinated against COVID-19). Subjective norms (α = .90) were measured with 3 items (e.g., It is expected of me that I get vaccinated against COVID-19).
COVID-19 Vaccine Efficacy Beliefs
Efficacy perceptions around COVID-19 vaccines were measured on 3 dimensions: self-efficacy, perceived behavioral control, and response efficacy. Self-efficacy 35 (α = .92) were measured with 3 items (e.g., I will be able to get vaccinated against COVID-19). Perceived behavioral control 20 (α = .77) was measured with 3 items (e.g., Getting a COVID-19 vaccine will be up to me). Response efficacy 35 was measured with a single item, reading “COVID-19 vaccination is effective in preventing COVID-19 for me.”
COVID-19 Threat Perceptions
COVID-19 threat perceptions were measured on 2 dimensions: perceived severity and perceived susceptibility. 35 Perceived severity (α = .94) was measured with 3 items (e.g., COVID-19 has severe consequences). Perceived susceptibility (α = .86) was measured with 3 items (e.g., I am likely to get COVID-19). Negative affect 35 (α = .96) towards COVID-19 was measured with 8 items (e.g., When I think about getting COVID-19, I feel worried).
Analysis
Inter-item Correlations (Pearson’s r) With Means, Standard Deviations, and 95% Confidence Intervals for all Study Variables.
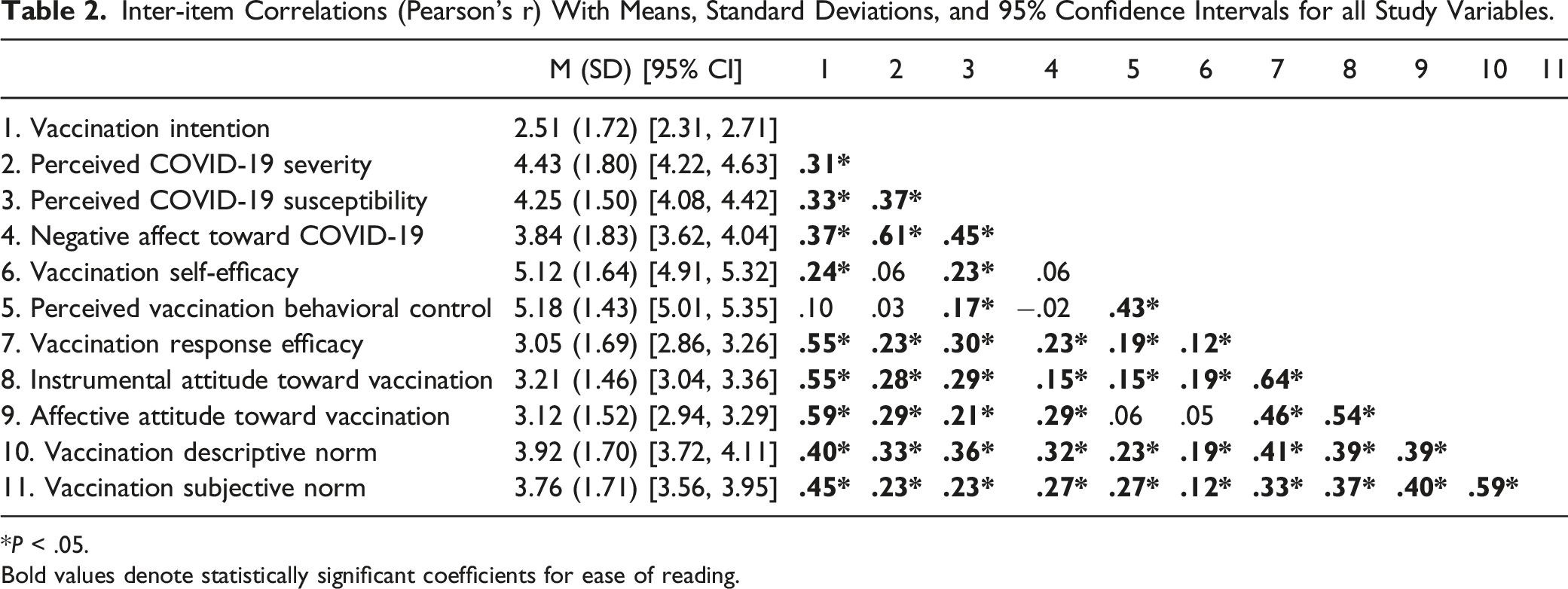
*P < .05. Bold values denote statistically significant coefficients for ease of reading.
Statistical predictors of vaccination intention were assessed by regressing vaccination intention on each of the independent variables noted above simultaneously, including an analytic sample of only participants who were unvaccinated. Model fit was assessed via the squared correlation ratio (R2), representing the amount of variance explained in the outcome by predictor variables, its standardized form, Adjusted R2, and the F null-hypothesis significance test, in which values with P values below the conventional .05 value suggesting rejection of the null hypothesis and retention of the estimated model. 37 Multicollinearity was assessed via the variance inflation factor (VIF), in which values below 2.5 are treated as small enough to ignore. 38
Statistical predictors of receiving any vaccine doses were assessed via logistic regression in which that binary dependent variable was regressed on each independent variable simultaneously, using the full dataset as its analytic sample. Model fit for the logistic regression was assessed via the log likelihood and χ2 coefficients.
Finally, assessment of mean values involved inspection of 95% confidence intervals computed around each variable’s mean value, primarily for variables with statistically significant regression coefficients. 19 Mean values at or near the scale midpoint of “4” resemble ambivalence or uncertainty regarding a particular statement. These values resemble a lack of endorsement of a particular belief or evaluative judgment and is thus open to persuasive messaging.17,39 If a belief is already endorsed (e.g., believing COVID-19 vaccination successfully protects one against severe COVID-19 illness), then persuasive health messaging is not necessary. Analyses used listwise deletion in which cases with any missing values across variables were excluded.
Results
In-text coefficients are reported as standardized, when available. Table 2 shows the means, standard deviations, 95% confidence intervals and correlations for all study variables. The confirmatory factor analysis found that the measurement model fit the data well, χ2 (369) = 681.81. p < .05, CFI = .961, RMSEA = .055 90% CI [.055, .062], SRMR = .054.
Sample Characteristics
The sample (N = 756) predominantly identified as White/Caucasian (89.7%, n = 678), with ages ranging from 18 to 99 years (M = 48.06 years, SD = 17.47). Most of the sample identified as women (51.2%, n = 357), reported no previous COVID-19 infection (61.5%, n = 465) and having received at least one COVID-19 vaccine dose (71.6%, n = 499). Most reported having had some college, but no degree (27.4%, n = 207) or being a high school graduate (27%, n = 204). Most respondents reported not having a college degree (66.3%, n = 501) and earning less than $50,000 annually (61.5%, n = 400). A plurality of respondents reported being employed as an hourly employee (26.2%, n = 198) or being retired (21%, n = 159). The sample consisted of self-identified Republicans (45.6%, n = 345), Democrats (32.7%, n = 247), and Independents (21.7%, n = 164). Respondents further reported being Politically Moderate (approx. 41.3%, n = 312), Conservative (approx. 36.1%, n = 273), or Liberal (approx. 36.1%, n = 273).
Complete Linear Regression Model Predicting Intention to Vaccinate Against the Virus That Causes COVID-19 With Variance Inflation Factors (VIF; Left) and Complete Logistic Regression Model Predicting the Self-report of Receipt of Any COVID-19 Vaccine dose(s) (right).

Note: Intention to vaccinate regression includes an analytic sample of only unvaccinated participants (n = 277) while the logistic regression for receiving any vaccine dose(s) includes the full sample (N = 756).
*P < .05.
The same analysis was conducted using logistic regression to predict whether participants reported receiving at least one dose of a COVID-19 vaccine. This analysis, also shown in Table 3, found the only significant predictors to be instrumental vaccination attitude, exp(B) = 2.09 95% CI [1.28, 3.41], and the subjective norm around COVID-19 vaccination, exp(B) = 2.00 [1.25, 3.20], Pseudo R2 = .29, log likelihood = 125.11, χ2 (10) = 38.34, P < .05.
Following the identification of statistical predictors of both intention and self-reported vaccination, mean scores were inspected to identify potential for movement by persuasive messages.19,20 The strongest predictor, affective attitude toward vaccination, had a mean score that was below the scale midpoint, M = 3.12, SD = 1.52, 95% CI [2.94, 3.29], as had the second strongest predictor of instrumental attitude, M = 3.21, SD = 1.46, 95% CI [3.04, 3.36]. These suggest that negative attitudes toward vaccination were held. Vaccination response efficacy, which had a similar magnitude as the instrumental attitude, was also below the scale midpoint, M = 3.05, SD = 1.69, 95% CI [2.86, 3.26]. Thus, sampled West Virginians did not, on average, believe COVID-19 vaccination was effective. Negative affect toward COVID-19 was at the midpoint, M = 3.84, SD = 1.83, 95% CI [3.62, 4.04], and the subjective norm was just below the midpoint, M = 3.76, SD = 1.71, 95% CI [3.56, 3.95].
Discussion
Leveraging interdisciplinary social and behavioral science in application to real-world problems through strategic communication is useful for positive movement on various public interest issues. Such attention is crucial around COVID-19, where communication has been offered by public health officials, government agencies, global health organizations, and researchers as an essential component for contributing to (or deterring from) vaccine uptake.
This study builds on frameworks from communication science and public health, seeking to identify promising topics for persuasive health messaging. This was achieved by predicting key motivators of COVID-19 vaccination intent, based on theories and models of health behavior change and concepts related to vaccine hesitancy19,20 along with evaluating the potential for shifting related beliefs. In addition to the theoretical grounding, these data represent estimates gleaned from a roughly representative sample of WV, with oversampling for racial/ethnic identity—by the latest U.S. Census, 40 WV is estimated to be slightly majority woman (i.e., 50.1%), predominately White/Caucasian (i.e., 93.1%), about one-quarter reportedly having a bachelor’s degree or higher (i.e., 21.8%) and being over the age of 65 years (i.e., 20.7%), and a median household income of $50,884. This translational approach enables development of data-driven messaging to build vaccine confidence within the surveyed population.
These findings can be translated through strategic public health messaging. Our analyses suggest predictors of vaccination intention (i.e., instrumental attitude toward vaccination, and subjective norms around COVID-19 vaccination) can be promising message targets given their relatively low-moderate mean scores. These data are particularly useful given the added nuance (i.e., separating “attitudes” into affective vs instructional, distinction of social norms, etc.) not reflected in existing vaccination intention meta-analyses, 24 and the differing pattern of results from national samples in this rural context.
Incorporating considerations of instrumental attitude and subjective norms into campaign planning may be particularly fruitful, given that each was not only predictive of vaccination intention but also of self-reported vaccination behavior. To illustrate, the more participants reported thinking COVID-19 vaccines were safe, beneficial, and good, the more they reported intending to get vaccinated. To positively shift instrumental attitudes, messaging should address safety, such as underscoring that billions of people worldwide and millions of people in the U.S. have safely received a COVID-19 vaccine, and that COVID-19 vaccines continue to undergo the most rigorous safety monitoring in U.S. history. 28 This messaging could be enhanced with storytelling from diverse rural residents sharing their experiences with COVID-19 vaccination safety. Messaging should also underscore self-interests and benefits of vaccination, protection against hospitalization and death, safely living a regular life, protecting livelihoods, protecting vulnerable loved ones, or other key motivators (such as those tailored through additional key audience analysis). Ultimately, these messages should offer logic, evidence, and storytelling from trusted sources to highlight the benefit of COVID-19 vaccination for oneself, the people they care about, and the specific communities in which they see themselves as members.
Positively shifting subjective social norms (i.e., perceptions that others who are important expect vaccination) may be the most challenging. Nonetheless, communication programming and targeted interventions can leverage subjective norms. For example, vaccination ambassador programs that inform and empower trusted opinion leaders at the local levels (e.g., faith leaders, parent-teacher groups, local business leaders) to share clear, consistent, scientifically sound information about vaccination along with their own personal vaccination stories could foster a sense of positive local social pressure to get vaccinated. Further, facilitating conversations between patients and their healthcare providers (e.g., through continuing medical education, distribution of patient education materials) can create the opportunities for building a sense of close encouragement (positive social pressure) from trusted medical sources. Additionally, partnerships between local businesses or employers, and local health departments or state government, to share COVID-19 vaccination information and answer questions, could facilitate shifts in subjective social norms. In the 2022 Edelman Trust Barometer, business was rated as the most trusted U.S. institution, with 77% of respondents citing trust in “My Employer.” 41 The endorsement of COVID-19 vaccination from a trusted employer alongside other daily colleagues could be the nudge some need to enact the recommended behavior. When addressing social norms, however, caution should be taken. Emphasizing what one should do (i.e., subjective norm) may cause psychological reactance, or the phenomenon of rejecting a message stance due to the perceived imposition or limiting of one’s freedom. 42 Messaging directly to social norms is not advised given the likelihood of inducing reactance, but the influence of social norms in vaccination among this population further emphasizes the need for public health partnerships that build the capacity of local trusted influencers who are on the group via accurate vaccination information and tools to effectively share with their communities vaccination information. These should be broadly considered, ranging from employers, to health organizations, to residential community leaders, to faith communities, and so on.
It is also worth noting, however, that shifting perceptions revealed in these data might require a change from rejecting to endorsing beliefs (i.e., moving from one side of the scale midpoint to the other). Crisis, risk, and health communication science can provide insight to address this challenge. Communicating effectively, especially to shift perceptions in this way, requires attention not only to the message topics targeting those specific intention-predictive perceptions but also consideration of other key factors such as communication source (i.e., the individual or entity distributing the message), channel (i.e., the form or location through which the message is delivered), and audience contexts such as prior risk/crisis exposure, lived experience, and sociocultural factors. 43 Thus, it is advisable that to design messages that address perceptions predictive of vaccination intentions and are culturally competent, and then deliver those messages through the full mix of channels that specific audiences are already using and from sources perceived as credible and trustworthy. Refining such delivery considerations in practice can be achieved through additional data collection among the target audience(s).
Limitations
This study has limitations that are worth considering when interpreting these findings. First, data from a cross-sectional survey are not causal and represent participants’ self-reported sentiment. Yet, using theory and concepts from communication science and public health to predict health behaviors to inform communication is a research framework of value that goes above and beyond the application and context. While vaccine reluctance in rural populations is crucial to understand given COVID-19’s impacts and lower vaccination confidence among these populations, 9 the views of rural Appalachians may not be reflective of all U.S. rural populations. Moreover, other regions of the U.S. and around the globe ought to be investigated using these approaches.
Conclusions
Messaging to nurture individuals along the vaccination confidence spectrum is an essential endeavor as COVID-19 continues to claim lives and disrupt livelihoods. The data presented here provide a snapshot
44
of messaging targets for increasing COVID-19 vaccination intentions among rural Appalachian audiences, while offering a theoretically driven yet practically applicable framework to assist more evidence-based and data-driven communication activities for health intervention. Our findings suggest that affective attitude toward vaccination, instrumental attitudes toward vaccination, vaccination response efficacy, negative affect toward COVID-19, vaccination self-efficacy, and subjective norms around COVID-19 vaccination, represent the most promising messaging targets. Rural vaccination rates are relatively lower than urban and suburban areas due to numerous social, cultural, and environmental factors. Theoretical frameworks offer some explanation and tools to address this need, but often exclude rural and especially Appalachian populations. This article applies robust social and behavioral science methodologies to a priority population, West Virginians, to understand possible psychosocial antecedents to vaccination and identify possible targets for strategic public health communication. Strategic public health messaging should consider instrumental attitudes and subjective norms to boost COVID-19 vaccination rates. Emphasizing vaccine safety and benefits, backed by evidence and real-life stories, can influence attitudes. Shifting subjective social norms may be challenging, but leveraging trusted local leaders and healthcare providers, as well as employer endorsements, can create positive social pressure for vaccination.So What?
What is Already Known About This Topic?
What Does This Article Add?
What are the Implications for Health Promotion Practice or Research?
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Centers for Disease Control and Prevention, Connecting Behavioral Science to COVID-19 Vaccine Demand Network (Grant U48DP006391-20C5).