
Abstract

Background
‘Health equity’ has become a central principle animating healthcare and social justice discourses in recent years. The concept of health equity signifies both the end-state goal that everyone has a fair and just opportunity to achieve the best health possible and the process through which economic and social obstacles to health, such as poverty and discrimination, are addressed and overcome. 1 Given these definitions, two things are evident. First, the United States is far from realizing fair and just opportunity to health for all, falling behind many of its peer nations on population-level health outcomes and burdened by more extreme inter-group health disparities. 2 Second, realizing significant improvement towards health equity will require vast social cooperation, both nationally to correct entrenched systemic barriers and locally to enact health-promoting changes at the community level.
This article describes how Northwell Health—the largest health care provider in New York State—and over one hundred community organizations across our New York City metropolitan service area organized a taskforce around the principle of health equity in order to distribute the first available COVID-19 vaccines. This Health Equity Taskforce (HET) has since diversified to address an array of community and population health disparities, prioritizing the wisdom of communities to better understand local contexts and guide our approach. This approach incorporates several existing public health and social justice principles while maintaining flexibility to identify communities’ needs and address their priorities. We also discuss challenges we have encountered along the way and reflect on how we have endeavored to adapt to these challenges, remain empirically focused, and build durable partnerships that improve health—especially for the most vulnerable people in our region.
A Call to Collective Action
The New York City metropolitan region was hit early and hard by COVID-19, becoming a national and global epicenter of infections in the first months of 2020. Before the first vaccines became available, Northwell partnered with state and local governments and leaders from dozens of local community service organizations, religious congregations, and tribal nations to offer accessible testing in underserved communities. During this time, Northwell increased communication with communities to foster knowledge exchange, build trust, and bolster our ability to respond to a perplexing pandemic. This included convening 55 “community listening tours” across the six-county service area, which involved thousands of participants and informed our testing deployment strategy.
The HET was formally established in January 2021 to tackle the challenge of distributing a limited supply of COVID-19 vaccines equitably throughout Nassau and Suffolk Counties of Long Island, as mandated by New York State Governor Andrew Cuomo. Yet, the HET’s foundation had been laid over the previous several years—not only by our COIVID-19 community testing efforts, but through a series of organizational policies enacted specifically to deepen our community partnerships and address health equity.3,4 To get vaccines distributed in a safe, timely, and equitable manner, our initial focus was on providing education and vaccinations to the most historically underserved communities on Long Island. The available epidemiological data indicated that these underserved communities were also disproportionately burdened by COVID-19 infections and deaths (Figure 1). Health Equity Taskforce area and priority neighborhoods.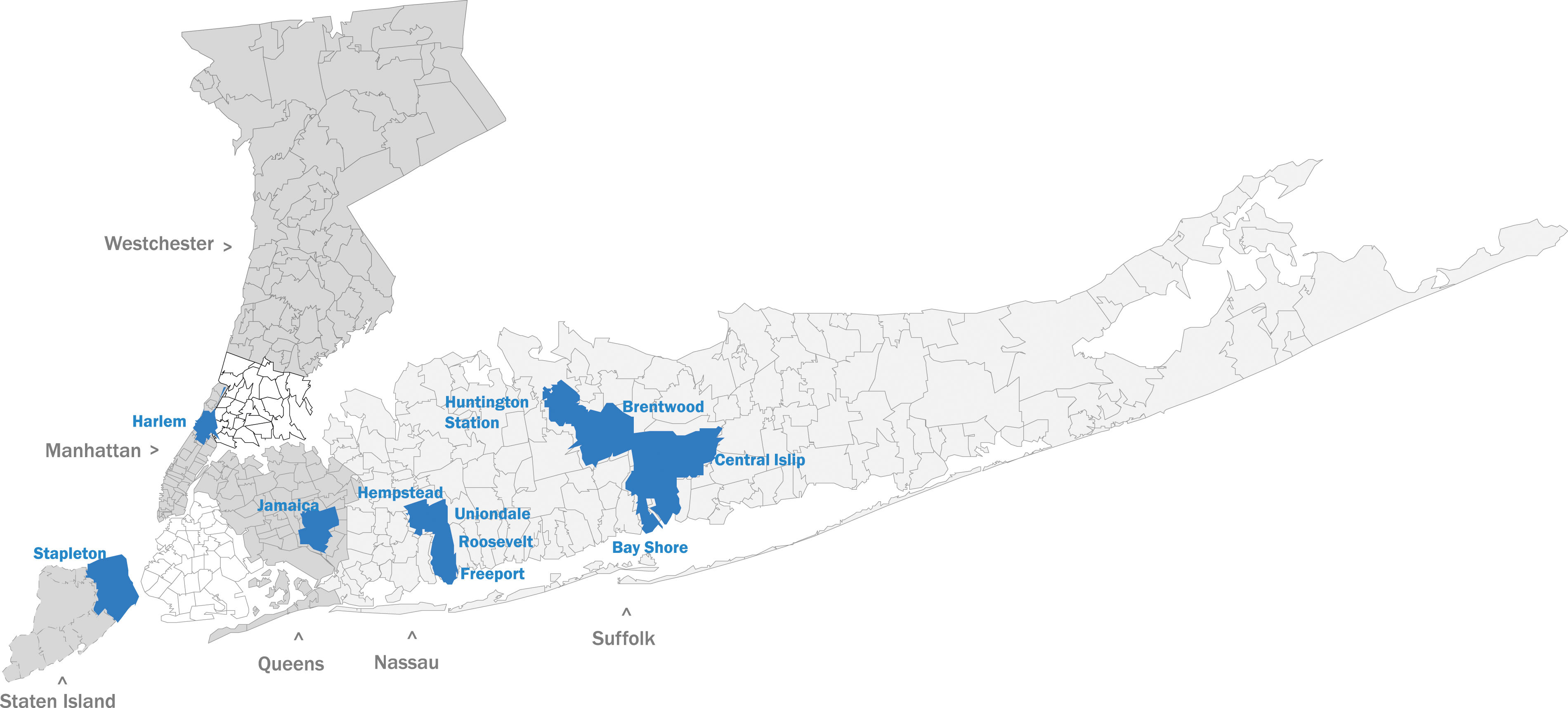
Early Challenges
The COVID-19 vaccines were scientifically validated to control the transmission and severity of the virus. However, several interrelated barriers to equitable distribution and vaccine uptake became readily apparent. In early HET meetings, members voiced significant skepticism about the vaccine itself and about the distribution process. We also encountered challenges emanating from lack of trust in health systems and the scientific community, which initially hindered efforts to achieve equitable vaccine distribution. These included: • Health care inaccessibility: Historically inequitable access to affordable, quality healthcare is an enduring and deadly problem in the U.S. Heavy disease burdens, high medical care costs, geographic inaccessibility, and discrimination, among other barriers, have long plagued socioeconomically disadvantaged and underserved groups, including minoritized racial-ethnic communities. Marginalization from quality healthcare was the baseline reality for many communities when limited quantities of the COVID-19 vaccine first became available. • Scarcity and competition: Some HET members expected that the needs of the communities they represented would again be overlooked. Vaccine scarcity led initially to a competitive, “us-versus-them” dynamic as we endeavored collectively to determine how many vaccine doses would be distributed to different communities. This also complicated efforts to gather local information in order to accurately assess communities’ needs. • Mistrust: Various American institutions, including the healthcare system, have long subjected marginalized communities to discriminatory treatment. Repeated experiences of personal and intergenerational mistreatment in medical settings can prime these communities to be mistrustful, presenting obstacles to vaccine uptake.5-7 • Uncertainty: Uncertainty and lack of clarity about the vaccine development process, potential side effects, and long-term efficacy further compromised trust. Some people felt that important information was being intentionally withheld or manipulated, leading to skepticism and reluctance. • Misinformation: A corollary of mistrust, the prevalence of conspiracy theories and other misinformation about vaccines further contributed to vaccine hesitancy, compounding doubts about the safety and effectiveness of the vaccine.
8
• Political polarization: In the U.S., perspectives on the COVID-19 pandemic became highly politicized. This polarization resulted in heightened skepticism towards public health measures, including vaccination. Some perceived the vaccine as more of a political contrivance than a politically neutral public health intervention.
9
• Religious and cultural factors: Some groups expressed reservations about the use of vaccines containing animal-derived ingredients or those developed using fetal cell lines.
Uncertain faith in government intentions on the part of some community members, as well as the sometimes-competing political agendas and messages of federal, state, and local governments, further complicated our efforts. Compounded by the stressors of pandemic isolation and occasional bouts of illness, this confluence of issues posed a significant challenge to achieving the HET’s initial objective.
Overcoming Obstacles
The HET was able to address many of these issues by proactively soliciting community members’ concerns, communicating information transparently in real-time, and incorporating community recommendations into the implementation strategy. Achieving equitable vaccine distribution depended on the input, expertise, and partnership of the diverse members of the taskforce. For instance, HET members recounted misinformation circulating within their communities that the vaccines contained harmful ingredients. They referenced historical instances of medical experimentation on marginalized populations, expressing concerns that COVID-19 vaccines might be another instance of exploitation and emphasizing the need for transparency and accountability from healthcare providers and government agencies. These insights informed the HET’s approach. Early meetings typically involved candid conversations among members about community level barriers and collective brainstorming to develop workable solutions. We also invited public health experts to share knowledge, dispel myths, and field questions.
HET members also raised concerns about vaccine access barriers, particularly for marginalized and underserved populations. They highlighted disparities in vaccine distribution, noting that affluent communities seemed to have easier access to vaccines compared to low-income neighborhoods. Some of these concerns were based on personal experiences of long wait times, scheduling issues, and limited vaccine supply. This feedback impelled the creation of more streamlined and community-led vaccination processes. The HET leveraged partnerships with community- and faith-based organizations to conduct focused outreach to the underserved communities they represented and assist with the enrollment of those community members.
Culturally and linguistically tailored outreach and education efforts that resonated with diverse communities were also critical. HET members representing different cultural backgrounds and faith communities stressed the need for public health messages that were respectful of and would resonate with the traditions, values, and worldviews of their members. The HET established an Education and Outreach subcommittee comprised of diverse members who informed the content, imagery, media, religious considerations, means of distribution, and languages represented in vaccine campaign materials.
These efforts resulted in the creation of a series of informational videos, flyers, brochures, and digital assets featuring messages from trusted community and faith leaders to encourage vaccination, dispel myths, answer common questions, and provide facts related to COVID-19 and the vaccine. These included “Be safe. Get vaccinated.” posters created in 17 languages and distributed widely in printed and digital formats; a HET Vaccine Education video featuring trusted community and faith leaders in multiple languages; a “COVID-19 MythBusters” brochure translated into multiple languages; and a social media campaign disseminated via outlets including Facebook, Instagram and YouTube. A publicly accessible online Community Resource Center was developed as a repository, allowing HET members to download, cobrand, and disseminate accurate and culturally tailored information into their communities. HET members and Northwell employees also distributed printed materials directly into communities, recognizing that some most-vulnerable groups were less likely to encounter digital media.
A Data-Driven Approach
Another key to achieving the HET’s goals has been a reliance on multiple data sources to objectively assess community needs and vulnerabilities. These have included regular COVID-19 epidemiological updates, the CDC’s Social Vulnerability Index, and neighborhood rates of under/uninsured individuals, among others. Those data were cross-referenced with existing community assets, including those operated by Northwell, state and county agencies, pharmacies, federally qualified health centers, and others, to establish deployment strategies and address access gaps. Data initially used to establish COVID-19 testing sites also informed the rollout of COVID-19 vaccination efforts.
These efforts appear to have had an impact: by June 2021, seven of the 10 ZIP codes on Long Island with the largest increases in COVID vaccination rates had majority Black or Hispanic populations. Public health experts and community leaders articulated that expanded outreach by local nonprofits, testimonials and information from trusted community members, greater accessibility, and the vaccinations of family and friends were among the reasons for these gains. 10 Together with the HET, Northwell provided the equitable distribution of over 500,000 COVID vaccine doses to approximately 250,000 community members at more than 100 locations, including houses of worship, community centers, housing projects, and other public places. In effect, the partnership established an efficient operating model to “meet people where they are” by delivering clinical services in community spaces.
Beyond COVID-19 vaccination, the HET has partnered with Northwell’s Community Wellness and Population Health team on a variety of community-engaged data gathering efforts. The data produced by these efforts have been employed to determine new priorities for collaboration and develop new programs, establish which neighborhoods are most vulnerable to poor outcomes in order to prioritize efforts in those neighborhoods, and evaluate program effectiveness. These data strategies have included the following: • Community Listening Tours to better understand health challenges and emerging trends from the perspectives of people living in specific communities. • Community Asset Mapping to identify resources and facilitators of positive change, from educational institutions to public parks, and from farmers markets to community centers. • The Community Health Needs Assessment (CHNA) to identify critical health needs. Together with the HET, Northwell has used knowledge gained from the CHNA to bolster partnerships and co-create programs that address food insecurity, diabetes and obesity, mental health and substance use disorders, youth education and career development, and maternal morbidity and mortality—especially in the most under-resourced communities of the NYC metropolitan region. • Secondary Data Analyses of publicly available datasets to better understand the communities in our service area, including the CDC’s Social Vulnerability Index, U.S. Census demographic data, and New York State Department of Health datasets to identify and bolster areas of greatest need.
A Model Emerges from Practice
The HET was established out of necessity in response to a specific public health emergency. As its purpose has expanded—and as its geographic reach has grown from Long Island to span Northwell’s six-county service area—it has coalesced around several interrelated public health and social justice paradigms (Figures 2 and 3). Conceptual frameworks. The Health Equity Taskforce model.
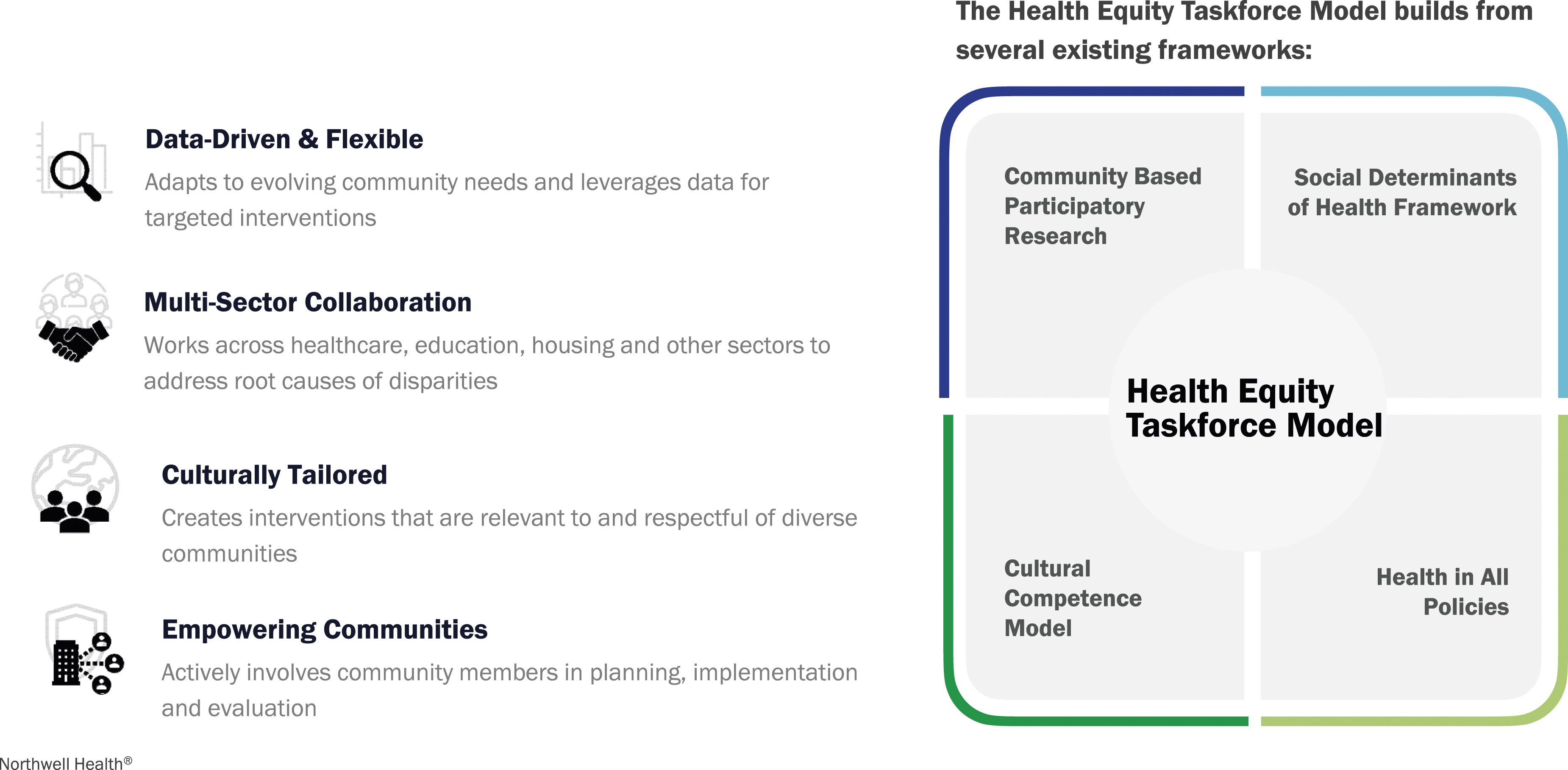
The HET model centers on principles of equity, partnership, and the incorporation of local community knowledge with other data sources to guide action. This approach respects the uniqueness of each community, prioritizes the inclusion of diverse perspectives, and is adaptable to the ever-changing landscape of health challenges.
Four key frameworks have shaped the HET’s approach:
Social Determinants of Health Framework (SDH)
The SDH framework recognizes that various social, economic, and environmental factors influence health. It highlights the necessity of addressing people’s broader social needs to achieve health equity. Interventions based on this framework focus on improving social and economic conditions, such as food insecurity, education, income, housing, and healthcare access to address health disparities. 11
The HET model and the SDH framework are complementary and interrelated; the HET model leverages insights from the SDH framework to inform its community-driven initiatives. As the HET has grown, its attention has moved further “upstream” to consider root causes of health inequities and—to the extent possible—address social determinants, which have an outsized impact on our health. The diverse nature of the HET’s membership, which represents a wide array of sectors, is conducive to taking the holistic perspective on health equity that the SDH framework presumes (Figure 4). Health Equity Taskforce partners.
Cultural Competence Model
The Cultural Competence Model emphasizes the importance of understanding and respecting the cultural beliefs, practices, and preferences of diverse communities. It seeks to enhance the effectiveness of health interventions by tailoring them to particular cultural contexts. This model emphasizes the importance of a deep understanding of the beliefs and practices of different communities on the part of healthcare professionals, promoting respectful and effective interactions with patients from various backgrounds. 12 The cultural diversity of the HET’s members and of the communities they represent lends itself to an approach that requires taking the role of culture for achieving more equitable health outcomes seriously.
Community Based Participatory Research (CBPR)
Community-Based Participatory Research involves community members, researchers, and other stakeholders in all phases of the research process. It emphasizes the importance of building partnerships, sharing power, and addressing the unique needs and strengths of the community. CBPR can be applied in research, program development, and policymaking to ensure that interventions are appropriate, relevant, and effective for the communities they address. 13
The HET model and CBPR are similar in their emphasis on community involvement and collaboration. However, they diverge somewhat in their primary focus and implementation processes. Whereas CBPR is research oriented and formally rigorous, the HET model solicits community-generated data to address a range of community-defined needs with an emphasis on flexibility. For instance, as the urgency of the COVID-19 pandemic began to recede, the HET began to pivot its attention to developing new programming to address declining mental health, identified by numerous community data sources as an emerging crisis.
Health in All Policies (HAP)
The HAP model involves integrating health considerations into decision-making across various sectors, such as education, housing, transportation, urban planning, and employment. It recognizes that policies outside the health sector can significantly impact health outcomes. This model promotes cross-sector collaborations, encouraging policymakers to consider the health implications of processes external to medical care. Similar to the SDH framework, it addresses the broader determinants of health by integrating health considerations into policies beyond the healthcare sector. It emphasizes a preventive approach to health by addressing upstream determinants, aiming to reduce the incidence of diseases and health disparities. 14
The HET model encourages partnership across various sectors to address health disparities and promote health equity. The HET operates from the premise that collaboration among its members broadens its influence and ability to affect change. It engages policymakers by way of government officials, community leaders, and stakeholders from diverse sectors to consider the health implications of policies and community programming. One example of this is the HET’s growing focus on education as a fundamental determinant of health and creating programs to expand educational and economic opportunities for young people in identified priority neighborhoods.
Expanding Our Purpose
The COVID-19 pandemic exacerbated and brought myriad longstanding societal inequities into sharper focus, including those in health care access and outcomes, education, and economic opportunity. With the worst of the pandemic behind, the HET unanimously decided that the collaborative should continue its work and expand to address other pressing community needs.
To do this, members of the HET are taking a broader view of what a regional partnership focused on health equity can accomplish. Using the multi-pronged, data-driven approach outlined above, Northwell and the HET identified four Wellness overarching areas for program expansion: 1. Health Disparities, including mental health, cancer, maternal health, and diabetes/obesity; 2. Neighborhood and Physical Environment, including food insecurity, gun violence, human trafficking, and climate change; 3. Economic Vitality, especially unemployment; and 4. Education, especially for youth.
Although full exploration of the work being undertaken in each of these areas is not possible in this article, we will highlight the HET’s expansion in 1 area identified as a top priority: mental health. In particular, we will discuss efforts to engage leaders of local faith communities to address mental health. Faith leaders, such as imams, pastors, and rabbis, are typically the trusted advisers of their congregations and are often among the first people called upon to support and guide members of their congregations who are experiencing distress. Despite this, few faith leaders have been trained to recognize or respond to mental health issues. Lack of engagement of faith leaders to promote mental health may represent a missed opportunity to address this growing health concern, particularly in communities experiencing higher burdens with fewer resources to address them.
First, the HET established a Faith Leaders Network of over 250 interdenominational members across its six-county area. From this Network, a smaller core Clergy Advisory Council was formed to guide community health equity initiatives. Most notably, the members serve as ambassadors for mental health-related work. In partnership with the HET and Northwell’s Community Wellness and Population Health team, this Council has convened a series of Faith Leader Forums to support open interfaith dialogue on mental health. The main themes addressed in these forums so far have included the provision of mental health education and training, self-care for clergy, bringing services into the community to meet people where they are, and prioritizing the youth mental health crisis.
As a result of the HET’s work with the Clergy Advisory Council, over 100 faith leaders to date have been trained in Stress First Aid by Northwell’s Center for Traumatic, Stress, Resilience, and Recovery. Stress First Aid provides a standardized framework of actions to address stress reactions and reduce their harms. More than 70 faith leaders thus far have undergone Mental Health First Aid and Youth Mental Health First Aid, evidence-based trainings from the National Council for Mental Wellbeing designed to increase knowledge and comfort with discussing and addressing mental health. The American Hospital Association’s Hospital Community Collaborative has recognized this partnership with the Association for Mental Health and Wellness and highlighted the HET as a model of effective community collaboration.
Northwell and the HET are currently piloting a program to offer lay counselor training to members of the Faith Leaders Network. The training offers individuals who are not licensed mental health providers with hands-on experience and education, equipping them to provide low-acuity mental health counseling in the community under the supervision of a licensed clinician. This model introduces task-sharing to help address the mental health crisis and a shortage of providers, which is especially acute in underserved neighborhoods. Additionally, Northwell has received nearly $1 million in grant funding to embed mental health professionals in faith-based organizations in order to increase access to mental health services. Northwell is also partnering with members of the HET to implement a youth mental health ambassador program in various faith and community-based organizations for high school students.
Discussion
As in many American metropolises, neighborhood-level inequities in health, wealth, and opportunity can be stark across metropolitan NYC. Cross-sector partnerships to promote health in underserved communities are vital because they bring together expertise and resources from sectors including healthcare, nonprofit organizations, education, government, and private sector businesses. These partnerships have the potential to leverage greater knowledge, data, infrastructure, and funding to create effectual interventions.
Cross-sector partnerships can also encourage diverse perspectives and ideas, fostering more holistic approaches to addressing social determinants of health. Importantly, such partnerships will have a greater likelihood of success when they actively involve community members in the planning, implementation, and evaluation of their work. A community-engaged approach is more likely to produce interventions that are culturally appropriate, respond to community needs, and empower local residents to be more receptive to adopting those interventions and improving their own health. Our experiences establishing and expanding the HET over the past few years has demonstrated the value of community-engaged partnerships to promote health, especially in neighborhoods that face the starkest disparities in health and social opportunity.
The HET was initially formed to address an acute public health crisis that impacted all community members and which garnered universal attention. As such, it was easy for the group to stay organized around a common objective. As our work expands to address a broader range of health inequities, some of which may be prioritized differently by different members and communities, it may be more challenging to maintain a unified sense of purpose. Moreover, health disparities are one part of the complex web of social and economic equality in America. The immensity and entrenched nature of the many barriers to health equity mean that positive change is often slow, incremental, uneven, and hard-won. This can lead to frustration, exhaustion, and complacency among even those most dedicated to agitating for equity. Limited resources and the uncertainties of grant funding can also threaten the viability of sustained progress.
In order to remain unified, effective, and immune to the traps of ‘health equity fatigue’, the HET continues to reevaluate its priorities with the input of its members and the broader community, engage in strategic planning, formalize processes for data collection and evaluation, and identify additional funding opportunities to support collaborations. As the HET settles into an era of expansion, it becomes increasingly important to enhance intragroup communication and data sharing, strengthen engagement with communities, engage in advocacy efforts, pursue funding opportunities, conduct program evaluations, and remain nimble to respond to emerging health challenges and new priorities. Without splintering apart, the HET is also forming smaller affinity groups to focus in on particular challenges, such as the Clergy Advisory Council’s work on mental health.
Another ongoing priority as the HET expands is to assess the impact of the work being undertaken. This assessment includes both quantitative measurements of health outcomes, access to services, and quality indicators, as well as less quantitatively precise but equally important considerations such as improved trust from communities and societal return on investment. While it is too soon to tell what the impact of newer initiatives will be, laying the groundwork to evaluate programs from multiple vantages is a necessity for the long-term success of the HET.
Conclusion
The HET’s work has been underpinned by a multi-pronged, data-driven community collaborative approach to identifying, prioritizing, and acting on the health problems facing communities across our diverse metropolitan region. The HET’s successes arise from its ability to bring people and resources together, harness collective wisdom, and drive tangible change. It is premised on the notion that “2 + 2 = 8”: our ability to make progress towards our objectives is exponentially greater when we bring our individual strengths, resources, and wisdom together in common purpose.
Building trust is a crucial first step for improving the health of communities, particularly among groups that have historically been marginalized. Building trust first requires listening to and seeking to understanding communities, engaging in open and transparent communication that addresses communities’ needs and concerns, and ensuring that community members have a voice in decisions that affect them. As our experience with equitable vaccine distribution made clear, overcoming mistrust based on longstanding inequities can be challenging, but the success of a public health initiative ultimately depends on it.
Partnerships among respected community leaders, community-based organizations, and healthcare institutions have innovative and under-explored potential to promote health and well-being. The HET will continue to align the collective efforts of its members, aiming to reduce health disparities and promote equity in our communities. To further amplify and scale its societal impact, the HET must further engage in advocacy efforts and deepen partnerships with policymakers and community leaders who share common goals. The accomplishments of the HET are a testament to the joint efforts a healthcare system working in concert with faith, community, tribal, government and private sector leaders toward the common goal of improving health equity.
Footnotes
Acknowledgments
The authors wish to thank the members of the Health Equity Taskforce, without whom this work would not have been possible. Dr Andrea Ault-Brutus offered insightful feedback and guidance throughout the preparation of this article. Mitchell Cornett, Mary Mahoney, and Edward Fraser have led community health engagement at Northwell and support the HET with unwavering commitment. Eugene Tangney and Emmett Walker, Jr have been steadfast champions of the HET since its inception. David Orner helped with the design of the figures. Maneeth Mylavarapu assisted with manuscript preparation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.