
Abstract
What does a good life look like? The present research investigated individual differences in people’s perceptions of the factors that are most important for living a good life using two waves of data in probability samples from the US (MIDUS; N = 4041) and Japan (MIDJA; N = 381). We examined country- and age-related similarities and differences in perceptions of a good life and associations of perceptions of a good life with experiences of wellbeing and physical health. Some factors were considered important for living a good life in both countries and across age (e.g., positive relationships with family), whereas other factors varied between countries (e.g., U.S. participants were more likely to perceive faith as important) and by age (e.g., younger adults were more likely to perceive having a good job as important). Further, perceptions of a good life were related to experiences of wellbeing and physical health concurrently and prospectively. This research informs our understanding of how people differ from one another in their perceptions of a good life, and how these differences may matter for individuals’ experiences of a good life.
Introduction
What does a good life look like? Centuries of philosophical debate and decades of wellbeing research have sought to understand the characteristics of a good life. Yet, lay perceptions of the factors that are important for living a good life are not well-understood.
Perceptions of what it means to live a good life are important because those perceptions may shape motivations and behaviors in pursuit of a good life (e.g., McMahan et al., 2013). Moreover, these perceptions could also influence what a given individual experiences as a good life (e.g., DeYoung & Tiberius, 2023). Finally, to the extent that people’s perceptions of a good life impact what they experience as a good life, understanding lay perceptions is vital to theoretical conceptualizations of what it means to live a good life. In the present research, we investigated individual differences in lay perceptions of a good life, whether those perceptions differ in the US and Japan or across adulthood, and if these perceptions have implications for individuals’ wellbeing and physical health.
Although relatively little research has addressed what people think of as “a good life,” past work has considered lay conceptions of related constructs such as wellbeing and happiness. In the following sections, we build from this research to inform our discussion. First, we review existing theory and empirical research on lay conceptions of wellbeing, and past research that speaks to cultural differences in perceptions of a good life, age differences in perceptions of a good life, and associations of perceptions of a good life with experiences of wellbeing and physical health. Then, we report empirical findings from two studies of people’s perceptions of the factors that are most important for living a good life.
Perceptions of a Good Life and Lay Conceptions of Wellbeing
Previous research has used a combination of qualitative and quantitative methods to investigate lay conceptions of wellbeing, happiness, and the good life. Qualitative studies have used interviews or writing prompts in which participants were asked open-ended questions about wellbeing (Ryff, 1989b; Sastre, 1999), happiness (Bojanowska & Zalewska, 2016; Lu & Gilmour, 2004; Uchida & Kitayama, 2009), and what it means to have a good life (Markus et al., 2004). Quantitative studies have asked participants to rate the desirability or goodness of hypothetical lives that vary in their attributes (e.g., King & Napa, 1998; Scollon & King, 2004), or to rate the degree to which specific factors are included in the experience of wellbeing and the good life (e.g., McMahan & Estes, 2011b, 2011a, 2012; McMahan et al., 2013). We refer to this collection of related constructs as lay conceptions of wellbeing.
The extent to which lay conceptions of wellbeing are synonymous with, related to, or distinct from people’s perceptions of the factors that are important for living a good life likely differs across measurement instruments and between individuals. Some instruments that have been used to assess lay conceptions of wellbeing included the term “good life” (e.g., “The experience of wellbeing and the good life necessarily involves…”) (McMahan & Estes, 2011a, 2011b, 2012; McMahan et al., 2013). In these cases, we can think of lay conceptions of wellbeing as synonymous with perceptions of the good life. In contrast, other measurement instruments have focused only on related constructs such as “wellbeing” (Ryff, 1989b; Sastre, 1999) or “happiness” (Bojanowska & Zalewska, 2016; Lu & Gilmour, 2004; Uchida & Kitayama, 2009). These wording differences may be arbitrary to some participants, and meaningful to others. For example, living a good life may by synonymous with living a happy life for some people. For these individuals, wellbeing and the good life may be relatively synonymous, because their vision of a good life is a life imbued with wellbeing. For others, giving back to one’s community or living a life full of accomplishments may be equally or more important to living a good life than personal wellbeing. For these individuals, wellbeing may be distinct from the good life, because their vision of a good life contains elements outside of their personal experiences of wellbeing. Thus, the literature on lay conceptions of wellbeing provides a rich conceptual foundation for research on perceptions of a good life, but the relationship between the two constructs is complex.
Results from these studies suggest that lay conceptions of wellbeing partially overlap with prominent theoretical models of wellbeing, such as eudaimonic (Ryff, 1989a), hedonic (Diener et al., 1984), social (Keyes, 1998), and health-related quality of life (Hanmer et al., 2006) models. Eudaimonic models of wellbeing emphasize living a virtuous life that is consistent with one’s full potential (Ryff, 1989a; Ryff et al., 2021). Prior research has observed eudaimonic concepts within lay conceptions of wellbeing, such as self-development and self-acceptance (e.g., McMahan & Estes, 2011b, 2011a, 2012; Ryff, 1989b). In contrast, hedonic models of wellbeing emphasize the experience of pleasure and the avoidance of pain (Diener et al., 1999; Ryff et al., 2021). Hedonic concepts such as positive emotion experience and avoidance of negative experiences are also prominent in lay conceptions of wellbeing (e.g., Markus et al., 2004; McMahan & Estes, 2011b, 2011a, 2012; Ryff, 1989b; Sastre, 1999). Social models expand wellbeing to the interpersonal realm, emphasizing personal relationships and one’s relationship to society as a whole (e.g., Keyes, 1998). Prior research has observed socially oriented lay conceptions of wellbeing such as an emphasis on family, social harmony, and contributions to others (e.g., Lu & Gilmour, 2004; Markus et al., 2004; McMahan & Estes, 2011b, 2011a, 2012; Ryff, 1989b; Sastre, 1999; Uchida & Kitayama, 2009). Finally, health-related quality of life models incorporate positive functioning as well as the absence of illness, pain, and functional impairment (e.g., Hanmer et al., 2006). A focus on health and the absence of illness can similarly be seen in lay conceptions of wellbeing (e.g., Markus et al., 2004; Ryff, 1989b).
Although lay conceptions of wellbeing share components of the aforementioned contemporary wellbeing models, they also differ from these models. For example, lay conceptions of wellbeing have been found to include elements that are typically considered causes of wellbeing rather than central components of wellbeing (e.g., money and faith). In sum, a growing body of research has found that lay conceptions of wellbeing include eudaimonic, hedonic, social, and health-related factors, as well as factors that fall outside of these traditional wellbeing categories. People’s perceptions of factors that are important for living a good life may similarly include wellbeing components as well as external circumstances and causes or sources of wellbeing.
Cultural Differences in Perceptions of a Good Life
Cultural values influence what it means to live a good life (Diener & Suh, 2000). As such, we might expect perceptions of the factors that are most important for living a good life to differ across cultures. Previous research on related constructs such as lay conceptions of wellbeing support this notion. For example, prior research has found that cultures with more collectivist values are more likely than cultures with more individualistic values to embrace social conceptions of wellbeing (Ford et al., 2015; Lu & Gilmour, 2004). Consistent with this idea, Chinese and Japanese participants’ definitions of happiness tend to emphasize social harmony, whereas U.S. American participants’ definitions of happiness tend to focus on positive emotion and personal achievement (Lu & Gilmour, 2004; Uchida & Kitayama, 2009). This does not mean that U.S. American and other Western conceptions of wellbeing do not include social elements, as cultural differences in conceptions of wellbeing may be a difference of degree rather than kind. For example, Ng and colleagues (2003) proposed a theoretical model of wellbeing in which agency and communion are universal elements, but the relative contributions of communion and agency to wellbeing differ across cultures.
Research on cultural differences in lay conceptions of successful aging provides additional insight. Although successful aging is a more narrow construct than wellbeing or the good life, people’s ideas about what it means to age successfully may share commonalities with their ideas about what it means to live a good life more generally. Thus, cultural differences and similarities in lay conceptions of successful aging may inform cultural differences and similarities in people’s perceptions of the good life. A review of the literature on lay conceptions of successful aging found that social engagement and having a positive attitude were the most commonly mentioned components of successful aging across 13 countries from seven world regions (Reich et al., 2020). Differences between countries and regions were relatively subtle, more often reflecting how frequently components were mentioned rather than if those components were mentioned at all. Others have argued that “successful aging” itself is a culturally bound idea, developed based on Western values (Liang & Luo, 2012). In their critique of theories of successful aging, Liang & Luo (2012) proposed a theory of harmonious aging based on Eastern philosophy that, much like lay conceptions of happiness in China and Japan, emphasizes harmony and balance during the aging process.
Taken together, there appears to be both shared and culturally distinct elements of people’s conceptions of wellbeing and successful aging. Regarding the culturally distinct elements, existing findings suggests that lay conceptions in East Asia may be more likely to focus on social factors, whereas lay conceptions in the U.S. may be more likely to focus on emotions and personal achievements. Cultural values may similarly influence the factors that people perceive to be most important for living a good life. For example, the U.S. is typically thought to hold more individualistic values, whereas Japan is typically thought to hold more collectivist values (Hamamura, 2012; Markus & Kitayama, 1991). These values may influence the extent to which self-focused factors (e.g., self-acceptance and sense of accomplishment) and social factors (e.g., relationships and giving back to one’s community) are included in people’s perceptions of a good life. In addition to these broad cultural values, prior research has observed cultural differences in preferences for particular types of emotions in the U.S. compared to East Asian Cultures (Tsai, 2007). These cultural values may influence the ways in which people living in those cultures view particular emotions (e.g., low arousal positive emotions) as important for living a good life. In addition to these cultural differences, many factors are likely to be perceived as important for living a good life in both the U.S. and Japan.
Age Differences in Perceptions of a Good Life
Several theories of adult development suggest that goals and priorities shift across the adult lifespan, which in turn may influence perceptions of the factors that are important for living a good life. For example, socioemotional selectivity theory (Carstensen, 1993, 2006, 2021; Carstensen et al., 1999) and the theory of strength and vulnerability integration (Charles & Luong, 2013) suggest that in response to a shortened time horizon, older adults prioritize emotionally meaningful goals and experiences, such as spending time with close others. In contrast, younger adults prioritize more knowledge-related goals, such as learning new things and pursuing career advancement. Relatedly, the selection, optimization, and compensation theory posits that older adults deprioritize achievement- and self-development goals as their physical, social, and cognitive function declines (Baltes, 1997; Baltes & Baltes, 1990; Freund & Baltes, 1998, 2002). These theories suggest that older adults may be more likely to incorporate emotionally meaningful experiences into their perceptions of a good life to a greater extent relative to younger adults. In addition, younger adults may be more likely to incorporate knowledge-acquisition, achievement, and self-development into their perceptions of a good life to a greater extent relative to older adults. However, like with cultural differences in perceptions of a good life, age differences in perceptions of a good life are likely to be differences of degree rather than absolute differences.
McMahan & Estes (2012) compared younger and older adults on four lay conceptions of wellbeing: experience of pleasure, avoidance of negative experience, self-development, and contributions to others. Partially consistent with theories of adult development, younger adults were more likely to perceive self-development and the experience of pleasure as important for wellbeing while older adults were more likely to perceive the avoidance of negative experience as important for wellbeing. Using a qualitative approach, Ryff (1989b) found that middle-aged adults placed greater emphasis on understanding and accepting one’s self, whereas older adults emphasized accepting one’s situation. Similarities in lay conceptions of wellbeing across the adult lifespan have also been observed. For example, an others-orientation, an emphasis on family, and elements of self-and/or situational-acceptance seem to be common elements in conceptions of wellbeing across the adult lifespan (McMahan & Estes, 2012; Ryff, 1989b; Sastre, 1999). Together, these findings suggest that some lay conceptions of wellbeing are relatively consistent across the adult lifespan (i.e., an orientation towards others and an emphasis on relationships), whereas other conceptions of wellbeing are more prevalent earlier (improving, understanding, and accepting one’s self, experiencing pleasure) or later (avoidance of negative experiences, acceptance of change) in the adult lifespan (McMahan & Estes, 2012; Ryff, 1989b). Perceptions of a good life may also demonstrate age similarities and differences across the adult lifespan.
Perceptions of a Good Life and Experiences of Wellbeing
People’s perceptions of the factors that are most important for living a good life may have importance implications for their experiences of wellbeing (e.g., Joshanloo, 2019). Research on the association between lay conceptions of wellbeing and experiences of wellbeing is consistent with this idea. People who have more eudaimonic conceptions of wellbeing tend to experience greater wellbeing across both eudaimonic and hedonic dimensions (McMahan & Estes, 2011a, 2011b). People who hold more hedonic conceptions of wellbeing also experience greater wellbeing, but effect sizes are smaller and less consistent across wellbeing dimensions. The link between conceptions of wellbeing and experiences of wellbeing may travel through behavior. Specifically, people may engage in behaviors that are congruent with their conceptions of wellbeing. For example, if someone perceives self-development as important for living a good life, they may be more likely to engage in behaviors that promote self-development. In turn, engaging in behaviors that promote self-development may increase their wellbeing. Consistent with this idea, McMahan et al. (2013) found that eudaimonic conceptions of wellbeing predicted engagement in eudaimonic behaviors in daily life, and engagement in eudaimonic behaviors partially explained the relationship between eudaimonic conceptions of wellbeing and experiences of wellbeing. However, hedonic conceptions of wellbeing were not associated with hedonic behaviors or with experiences of wellbeing.
The aforementioned findings may suggest that eudaimonic pursuits are a more effective pathway to wellbeing than hedonic pursuits. Indeed, in addition to a weaker link between hedonic conceptions of wellbeing and hedonic behaviors (McMahan et al., 2013), research has also found that hedonic behaviors are less strongly linked to experiences of wellbeing compared to eudaimonic behaviors (Steger et al., 2008). Thus, both the link between wellbeing conceptions and behaviors as well as the link between behaviors and wellbeing experiences may be weaker for hedonic relative to eudaimonic conceptions of wellbeing. In sum, there is consistent evidence for an association between eudaimonic conceptions of wellbeing and greater experiences of wellbeing; however, results are more mixed for hedonic conceptions of wellbeing. Further, relatively little is known about associations between lay conceptions of wellbeing that fall outside of the traditional eudaimonic and hedonic categories. Applied to perceptions of a good life, people may engage in behaviors that help them attain their vision of a good life. In turn, these behaviors are likely to influence their experiences of wellbeing.
Perceptions of a Good Life and Physical Health
In addition to influencing wellbeing, the factors that people perceive as important for living a good life may have implications for physical health. Consistent with a conception-congruent behavior model (McMahan et al., 2013), people who perceive health as important for living a good life may be more likely to engage in health-protective behaviors, and in turn should benefit from better health as a result of those behaviors. Perceptions of a good life that are not directly related to health may also influence health-relevant behaviors. For example, perceiving social factors as important for living a good life may foster more supportive social networks which are beneficial for health (Uchino, 2009), and perceiving hedonic factors as important for living a good life may lead to either health-detrimental (e.g., substance use) or health-promoting (e.g., going on a long walk) hedonic behaviors (Steger et al., 2008).
Alternatively, the causal arrow may go in the other direction. People’s perceptions of the factors that are important for living a good life may be driven by what they don’t have in their own lives. In this case, people in poor health may be more likely to recognize the importance of health for living a good life. This would suggest a negative association between health-related conceptions of a good life and physical health. Taken together, there are multiple reasons to expect perceptions of a good life to be associated with physical health, but the exact pattern of these potential associations is unclear.
The Present Research
The present research investigated individual differences in the factors that people perceive to be most important for living a good life. Using data from the U.S. and Japan, the current study had four research questions. First, how do perceptions of a good life differ in the U.S. compared to Japan (Aim 1)? Second, how do perceptions of a good life differ across the adult lifespan (Aim 2)? We preregistered our research questions for Aims 1 and 2, but we did not have specific hypotheses. Third, how are people’s perceptions of a good life associated with their experiences of wellbeing (Aim 3)? We examined concurrent associations between perceptions of a good life and experiences of overall psychological wellbeing (Aim 3a), concurrent associations between perceptions of a good life and experiences of perception-congruent facets of wellbeing (Aim 3b), and prospective associations between perceptions of a good life and experiences of perception-congruent facets of wellbeing (Aim 3c). We hypothesized that perceptions of a good life would prospectively predict increases in perception-congruent wellbeing experiences across time. For example, someone who perceives “sense of purpose” as important for living a good life should be motivated to engage in purpose-congruent behaviors, and in turn should experience more sense of purpose across time.
Fourth, how are people’s perceptions of a good life associated with physical health (Aim 4)? We examined concurrent associations between perceptions of a good life, self-evaluated physical health, and chronic health conditions (Aim 4a), prospective associations between perceptions of a good life, self-evaluated physical health, chronic health conditions, and mortality (4b), and whether perceptions of a good life moderated associations between wellbeing and physical health (Aim 4c). We hypothesized that perceptions of a good life would either not be associated with physical health, or that eudaimonic, hedonic, and social perceptions of a good life would be associated with better physical health (i.e., better self-evaluated physical health, fewer chronic health conditions, and longer survival). We did not expect eudaimonic, hedonic, and social perceptions of a good life to be associated with worse physical health. Finally, we hypothesized that positive associations between wellbeing and physical health would be more pronounced for people who perceived that particular type of wellbeing as among the most important factors for living a good life. 1
Method
Positionality Statement
The authors wish to provide the reader with information about our backgrounds and identities, which may have influenced our approach to conducting this research and our interpretation of study findings. All four authors are White U.S. Americans ranging from younger adulthood to midlife. Our identities likely impacted our approach to this research, particularly Aims 1 and 2 concerning cultural and age differences in perceptions of a good life. Whereas we have firsthand experience living in the U.S., our knowledge of the experiences and perceptions of Japanese adults and potential factors that may contribute to differences between the U.S. and Japan in perceptions of a good life is limited to the scientific literature. Similarly, although the authors span younger adulthood and midlife, our knowledge of the experiences and perceptions of older adults and potential factors that may contribute to age differences in perceptions of a good life is primarily based on the scientific literature.
Participants and Procedures
The MIDUS study includes a probability sample of U.S. adults (total N = 7108). The MIDJA study includes a probability sample of adults from the Tokyo metropolitan area (total N = 1027). We used data from MIDUS 2 (collected in 2004–2006), MIDUS 3 (collected in 2014–2016), MIDJA 1 (collected in 2008–2010), and MIDJA 2 (collected in 2012–14). In the remainder of the manuscript, we refer to MIDUS 2 as MIDUS Time 1 (analytic baseline) and we refer to MIDUS 3 as MIDUS Time 2. We tested Aims 1 and 2 and portions of Aim 3 using cross-sectional data at MIDUS Time 1 and MIDJA Time 1, because these are the first time points at which the good life measure was administered. Due to the smaller sample size in MIDJA relative to MIDUS, we preregistered the remaining aims using only MIDUS data, including cross-sectional analyses at MIDUS Time 1 and prospective analyses involving MIDUS Time 1 and MIDUS Time 2. MIDJA Time 2 data were used only to compute test–retest reliabilities for wellbeing measures and to evaluate the degree of stability and change in perceptions of a good life.
At each timepoint, participants reported their sociodemographic information, and completed a measure of their perceptions of the factors that are most important for living a good life, measures of wellbeing, and measures of physical health. The perceptions of a good life measure was administered to a subset (N = 382) of MIDJA participants who participated in the Biomarkers substudy in 2009–2010. Additionally, mortality status was tracked for MIDUS participants through 2019. In the present research, we focused on the subset of participants who completed the measure of perceptions of a good life in MIDUS Time 1 (N = 4041) and MIDJA Time 1 (N = 381). More detailed information about MIDUS and MIDJA can be found on the study websites [http://midus.wisc.edu/; https://www.icpsr.umich.edu/web/NACDA/series/203].
Across aims, 4041 MIDUS participants and 381 MIDJA participants met inclusion criteria for at least one analysis. Aim-specific inclusion criteria are described in the Analytic Approach section. For MIDUS, the full analytic sample ranged from 30 to 84 years old at MIDUS Time 1, with an average of 56.23 (SD = 12.39); 55.4% of the participants were female and 44.6% were male; and 91.5% White, 3.7% Black or African American, 1.5% Native American or Alaskan Native, 0.5% Asian, <0.1% Native Hawaiian or Pacific Islander, 2.2% Other Race or Ethnicity, and 0.5% No Response. For MIDJA, the full analytic sample ranged from 30 to 79 years old, with an average of 54.21 (SD = 14.12); 56.0% of the participants were female and 44.0% were male.
Measures
Perceptions of a Good Life
Perceptions of a good life were assessed in MIDUS Time 1, MIDUS Time 2, and the MIDJA Time 1 and MIDJA Time 2 Biomarker substudies. To assess perceptions of the factors that are most important for living a good life, participants received the following prompt: “Please check only five of the following items that you feel are the most important for living a good life.” The 17 response options included eudaimonic factors (i.e., “sense of purpose,” “autonomy,” “continual learning and growth,” “loving and caring for myself”), hedonic factors (i.e., “enjoyment of life’s pleasures,” “relaxation, contentment, and pleasure”), social factors (i.e., “positive relationships with family,” “positive relationships with friends,” “giving back to my community”), health-related factors (“absence of illness,” “physical fitness and strength”), and other factors (i.e., “achievement,” “having a good job,” “enough money to meet basic needs,” “extra money/disposable income,” “faith,” and “positive attitude”). We grouped these factors into categories for descriptive purposes only, based on content overlap with eudaimonic (i.e., Ryff, 1989a), hedonic (e.g., Diener et al., 1999), social (e.g., Keyes, 1998), and health-related quality of life (e.g., Hanmer et al., 2006) models of wellbeing. Factors that did not fall into these models were grouped into an “Other” category. These categories were not used in analyses except to aid interpretation, and they were not shown to participants.
Frequencies for each factor are shown in Table 3. We conducted exploratory analyses of the degree of stability versus change in people’s perception across time (see Table S2). Results are consistent with both stability and change in perceptions of a good life, at least in the long-term across several years. On average, people retained 2.76 (SD = 1.01) selections out of 5 across a 9-year period in MIDUS and 3.07 (SD = 1.03) selections out of 5 across a 4-year period in MIDJA. If participants were selecting factors at random (i.e., no within-person stability), we would expect participants to retain only 0.74 selections across the two measurement occasions on average.
Overall Psychological Wellbeing
Zero-order Pearson correlations between wellbeing and health variables.
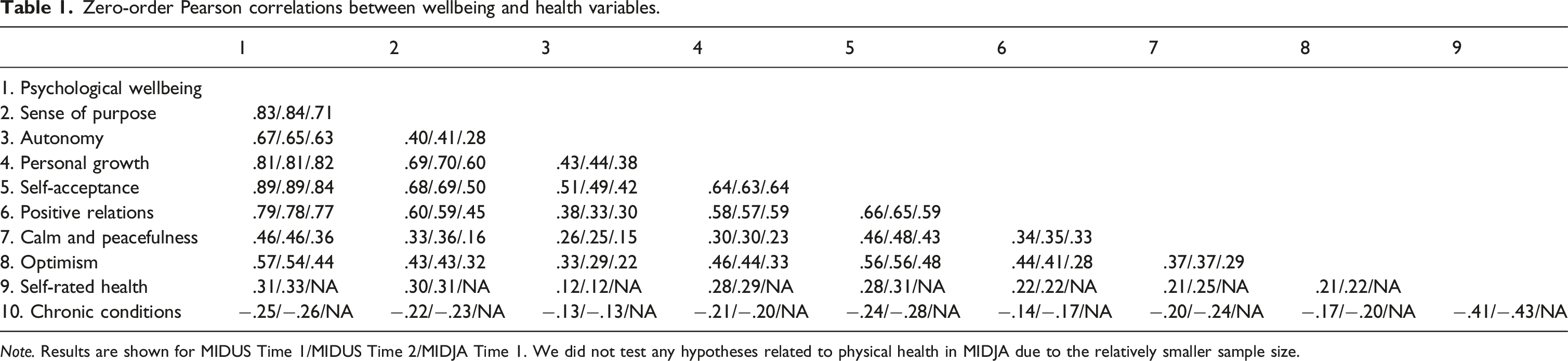
Note. Results are shown for MIDUS Time 1/MIDUS Time 2/MIDJA Time 1. We did not test any hypotheses related to physical health in MIDJA due to the relatively smaller sample size.
Descriptive statistics of wellbeing and health variables.
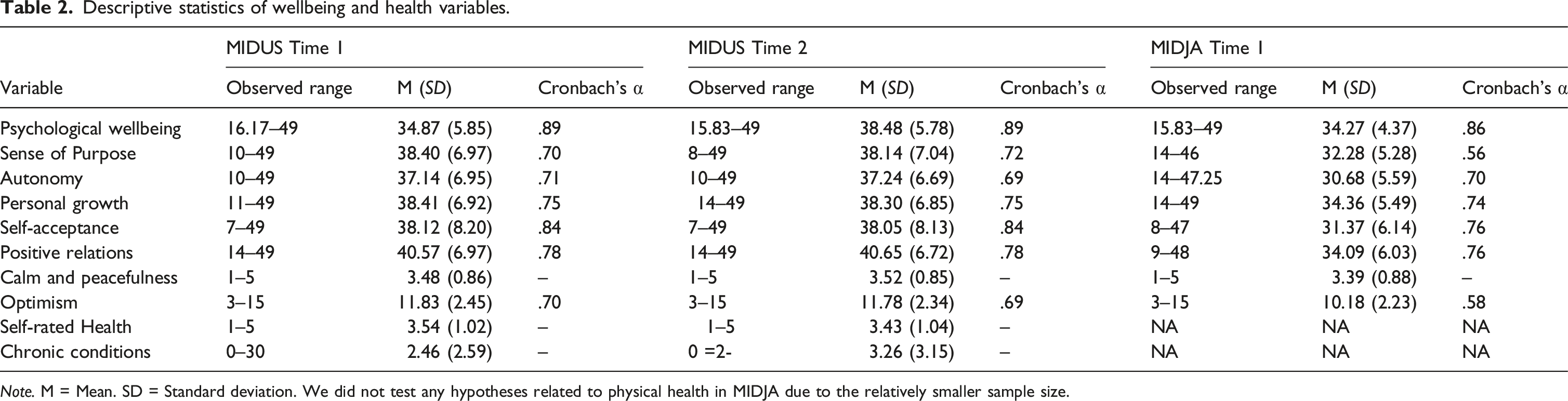
Note. M = Mean. SD = Standard deviation. We did not test any hypotheses related to physical health in MIDJA due to the relatively smaller sample size.
To assess overall psychological wellbeing, we used the 42-item version of the Ryff Psychological Wellbeing Scales (Ryff, 1989a). MIDUS participants responded to each item on a 1 (Strongly Disagree) to 7 (Strongly Agree) scale. MIDJA participants responded to each item on a 1 (Strongly Agree) to 7 (Strongly Disagree) scale. Responses were reverse-scored as necessary, such that higher values indicated greater wellbeing for both MIDUS and MIDJA participants. First, the 7-items for each subscale were summed. For items with a missing value, the mean value of that participant’s completed items was imputed. Sum scores were computed for participants who responded to at least four items for a given subscale. Participants who responded to fewer than four items for a given subscale received a missing value for that subscale. Then, we computed the average of the six subscales for a total score with a possible range of 7–49. Nine-year test–retest reliability between MIDUS Time 1 and MIDUS Time 2 was .72 and 4-year test–retest reliability between MIDJA Time 1 and MIDJA Time 2 was .78.
Perception-Congruent Wellbeing
To measure perception-congruent wellbeing for the item “sense of purpose,” we used the purpose in life subscale of the Ryff Psychological Wellbeing Scales (Ryff, 1989a). Nine-year test–retest reliability between MIDUS Time 1 and MIDUS Time 2 was .64 and 4-year test–retest reliability between MIDJA Time 1 and MIDJA Time 2 was .63.
To measure perception-congruent wellbeing for the item “autonomy,” we used the autonomy subscale of the Ryff Psychological Wellbeing Scales (Ryff, 1989a). Nine-year test–retest reliability between MIDUS Time 1 and MIDUS Time 2 was .66 and 4-year test–retest reliability between MIDJA Time 1 and MIDJA Time 2 was .72.
To measure perception-congruent wellbeing for the item “continual learning and growth,” we used the personal growth subscale of the Ryff Psychological Wellbeing Scales (Ryff, 1989a). Nine-year test–retest reliability between MIDUS Time 1 and MIDUS Time 2 was .66 and 4-year test–retest reliability between MIDJA Time 1 and MIDJA Time 2 was .67.
To measure perception-congruent wellbeing for the item “loving and caring for myself,” we used the self-acceptance subscale of the Ryff Psychological Wellbeing Scales (Ryff, 1989a). Nine-year test–retest reliability between MIDUS Time 1 and MIDUS Time 2 was .70 and 4-year test–retest reliability between MIDJA Time 1 and MIDJA Time 2 was .76.
To measure perception-congruent wellbeing for the items “positive relationships with family” and “positive relationships with friends,” we used the positive relations subscale of the Ryff Psychological Wellbeing Scales (Ryff, 1989a). Nine-year test–retest reliability between MIDUS Time 1 and MIDUS Time 2 was .66 and 4-year test–retest reliability between MIDJA Time 1 and MIDJA Time 2 was .69.
To measure perception-congruent wellbeing for the item “relaxation, peacefulness, and contentment,” we used the item “During the past 30 days, how much of the time did you feel calm and peaceful?”. In MIDUS, participants responded on a scale from 1 (All the time) to 5 (None of the time). In MIDJA, participants responded on a scale from 1 (None of the Time) to 5 (All the time). We reverse-scored the item in MIDUS such that higher values reflect more frequent experiences of calm and peacefulness. Nine-year test retest between MIDUS Time 1 and MIDUS Time 2 was .46, and 4-year test–retest reliability between MIDJA Time 1 and MIDJA Time 2 was .56.
To measure perception-congruent wellbeing for the item “positive attitude,” we used the optimism subscale of the Life Orientation Test (Scheier & Carver, 1985). Three items were assessed on a 1–5 scale, and then summed for a possible range of 3–15. Nine-year test–retest reliability between MIDUS Time 1 and MIDUS Time 2 was .59 and 4-year test–retest reliability between MIDJA Time 1 and MIDJA Time 2 was .52.
Physical Health
We used three indicators of physical health: self-evaluated physical health, chronic health conditions, and mortality.
To assess self-evaluated physical health, participants responded to the question “In general, would you say your physical health is excellent, very good, good, fair, or poor?”. Response options ranged from 1 (Excellent) to 5 (Poor). We reverse-scored participants’ responses such that higher values indicated better self-evaluated physical health. Nine-year test–retest reliability between MIDUS Time 1 and MIDUS Time 2 was .55.
To assess chronic health conditions, participants reported whether they had each of 29 listed chronic conditions (e.g., stroke, diabetes) in the past 12 months and the conditions were summed. At MIDUS Time 1, 77.5% of participants reported at least one chronic health condition. At MIDUS Time 2, 82.1% of participants reported at least one chronic health condition. Nine-year test–retest reliability between MIDUS Time 1 and MIDUS Time 2 was .58.
To assess mortality, mortality status was collected using several methods, including National Death Index reports conducted in 2006, 2009, and 2016, and longitudinal sample maintenance through 2019. Survival time was calculated by subtracting the MIDUS Time 1 interview month and year from the month and year of death.
Analytic Approach
Data were analyzed using R, version 4.2.0 and the following packages: MASS (Venables & Ripley, 2002), pscl (Jackman, 2020), psych (Revelle, 2020), stats (R Core Team, 2013); survival (Therneau, 2023).
Cultural differences in perceptions of a good life.
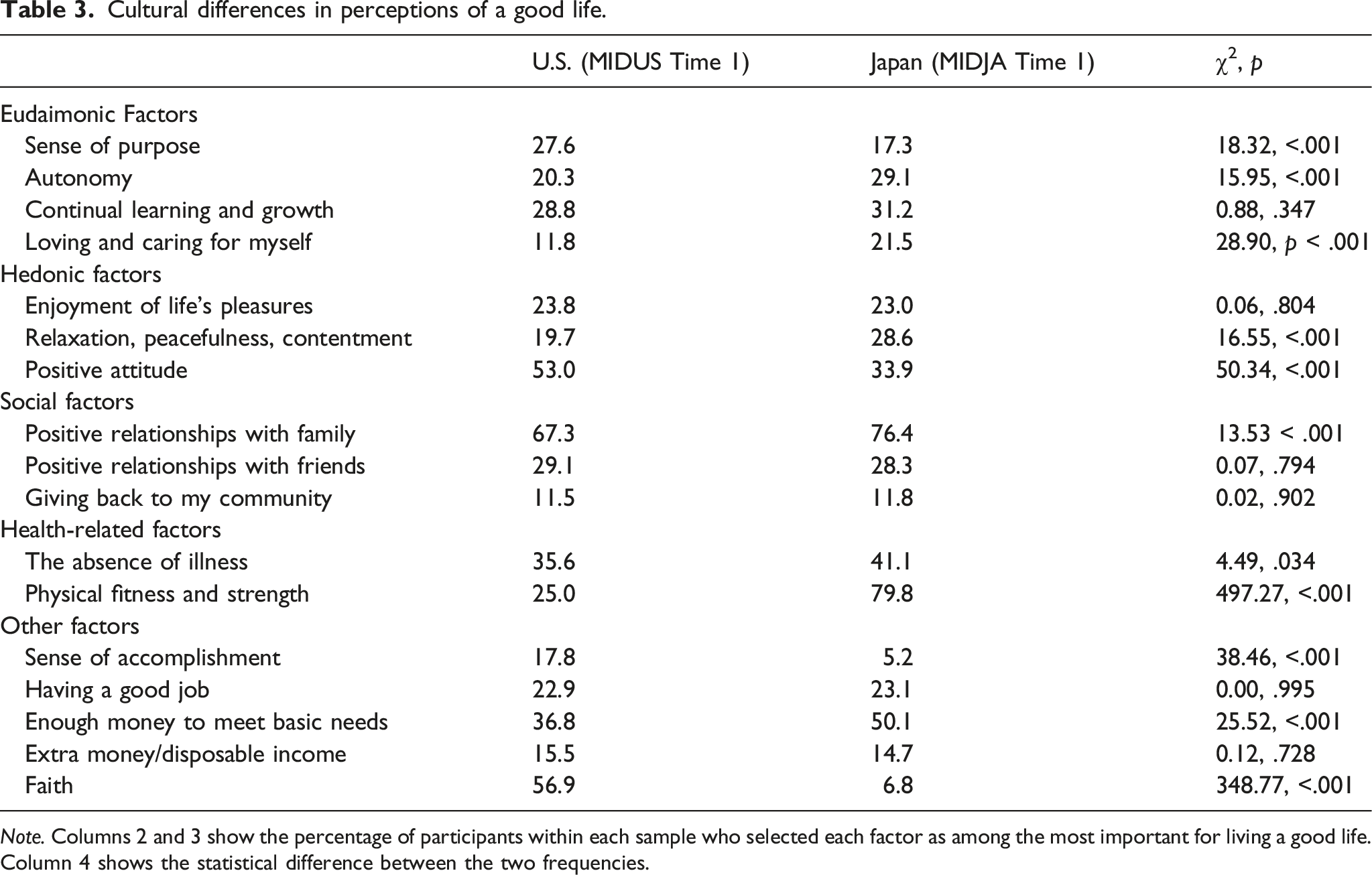
Note. Columns 2 and 3 show the percentage of participants within each sample who selected each factor as among the most important for living a good life. Column 4 shows the statistical difference between the two frequencies.
Age differences in perceptions of a good life.

Note. 99% confidence intervals are shown. Effect sizes are Cohen’s d. “Younger” indicates people who selected the factor as among the most important for living a good life tended to be younger. “Older” indicates people who selected the factor as among the most important for living a good life tended to be older.
†Effect was statistically different from zero when using FDR correction and an alpha level of .05, rather than uncorrected p values and an alpha level of .01.
Concurrent Associations between Perceptions of a Good Life and Psychological Wellbeing.

Note. 99% confidence intervals are shown. Effect sizes are Cohen’s d.
†Effect was statistically different from zero when using FDR correction and an alpha level of .05, rather than uncorrected p values and an alpha level of .01.
Concurrent associations between perceptions of a good life and perception-congruent wellbeing.

Note. 99% confidence intervals are shown. Effect sizes are Cohen’s d. The perception-congruent measure of wellbeing is shown in parentheses after the good life item in Column 1. – = No appropriate measure of perception-congruent wellbeing. Health-related and “other” factors were excluded from Aim 3b.
Prospective associations between perceptions of a good life and change in perception-congruent wellbeing.
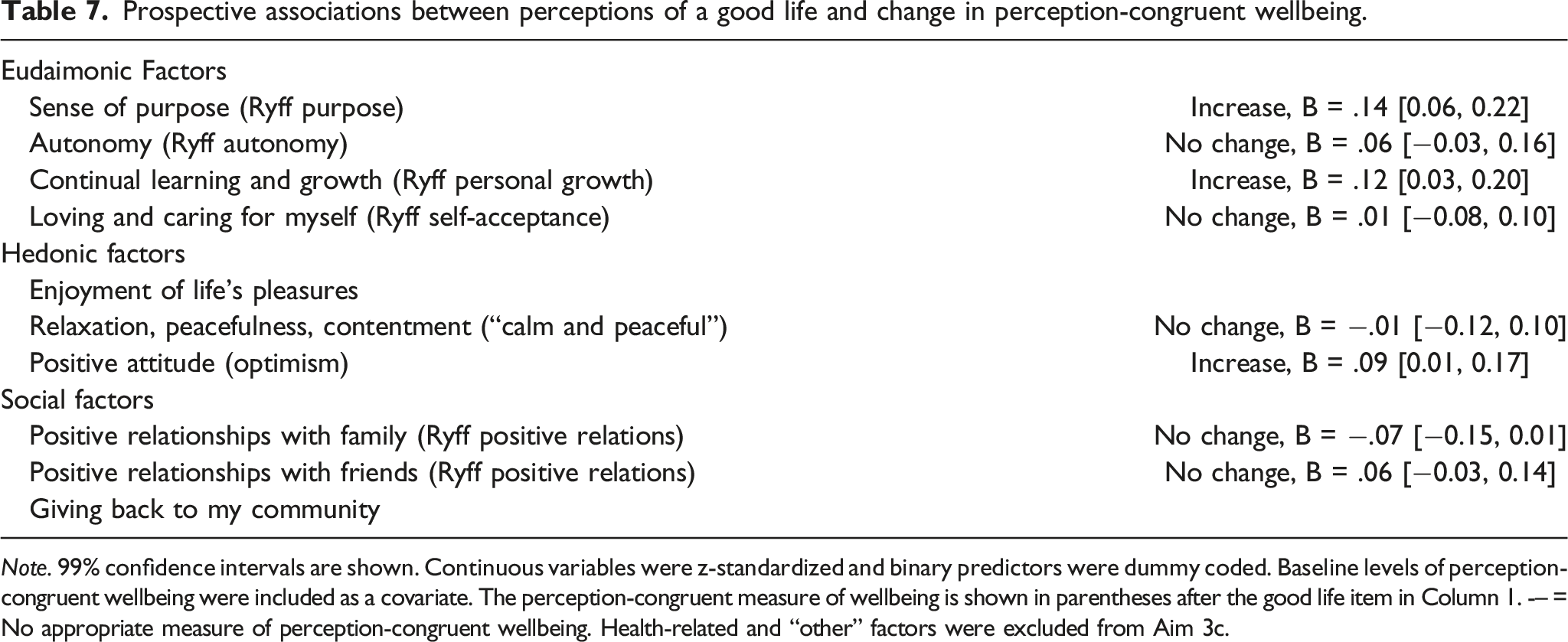
Note. 99% confidence intervals are shown. Continuous variables were z-standardized and binary predictors were dummy coded. Baseline levels of perception-congruent wellbeing were included as a covariate. The perception-congruent measure of wellbeing is shown in parentheses after the good life item in Column 1. -– = No appropriate measure of perception-congruent wellbeing. Health-related and “other” factors were excluded from Aim 3c.
Aim 1: Cultural Differences in Perceptions of a Good Life
Participants were included in analyses for Aim 1 if they completed the measure of perceptions of a good at in MIDUS Time 1 (N = 4041) or MIDJA Time 1 (N = 381). Given the sample size in each group and our alpha level of .01, we had 80% statistical power to detect a small effect (h = .18 or larger). First, we computed the percentage of participants within each sample that selected each factor as among the most important for living a good life. Then, we rank ordered the factors based on their frequency within each sample. We report the top five most commonly endorsed factors in the U.S. and Japan. Next, we used a series of 17 Chi-square tests of independence to compare the proportion of participants the U.S. to the proportion of participants in Japan who selected each of the 17 factors as among the most important for living a good life.
Aim 2: Age Differences in Perceptions of a Good Life
Participants were included in analyses for Aim 2 if they completed the measure of perceptions of a good life at MIDUS Time 1 (N = 4041) or MIDJA Time 1 (N = 381). Given the sample size and our alpha level of .01, we had 80% statistical power to detect small age differences in MIDUS (d = .08 or larger) and medium age differences in MIDJA (d = .25 or larger). We used a series of 17 Welch’s t-tests within each sample to compare the mean age of participants who selected each of the 17 factors as among the most important for living a good life to those who did not.
Aim 3: Perceptions of a Good Life and Wellbeing
Participants were included in analyses for Aims 3a and 3b if they completed the measure of perceptions of a good life and the wellbeing measure(s) at MIDUS Time 1 (N = 4026) or MIDJA Time 1 (N = 381). Participants were included in analyses for Aim 3c if they completed the measure of perceptions of a good life at MIDUS Time 1 and measure(s) of wellbeing at MIDUS Time 1 and MIDUS Time 2 (N = 2693). Given the sample size and our alpha level of .01, we had 80% statistical power to detect small concurrent associations with wellbeing in MIDUS (d = .08 or larger) and medium concurrent associations with wellbeing in MIDJA (d = .25 or larger) (Aims 3a and 3b). Given the sample size and our alpha level of .01, we had 80% statistical power to detect small prospective associations between perceptions of a good life and wellbeing change in MIDUS (standardized regression coefficient = .08 or larger) (Aim 3c). Because we expected these associations to be small, we did not have sufficient power to test Aim 3c in MIDJA.
To address Aim 3a, we used a series of 17 Welch’s t-tests within each sample to compare the mean psychological wellbeing of participants who selected each of the 17 factors as among the most important for living a good life to those who did not select that factor.
For Aim 3b, we focused on the 10 factors for which we had congruent measures of wellbeing. We used a series of 10 Welch’s t-tests within each sample to compare the mean perception-congruent wellbeing of participants who selected each of the 10 factors as among the most important for living a good life to those who did not select that factor. For example, we compared the mean sense of purpose for participants who selected “sense of purpose” as among the most important factors for living a good life to those who did not select “sense of purpose” as among the most important factors for living a good life. This included all of the eudaimonic factors, two of the three hedonic factors (i.e., “relaxation, peacefulness, and contentment”, “positive attitude”), and two of the social factors (i.e., “positive relationships with family”, “positive relationships with friends”). We did not have congruent measures of wellbeing for “enjoyment of life’s pleasures” or “giving back to my community.”
To address Aim 3c, we used a series of 10 general linear models in MIDUS to examine the effects of people’s perceptions of wellbeing on longitudinal change in perception-congruent wellbeing. In each model, perception-congruent wellbeing assessed at MIDUS Time 2 was the outcome variable. A binary variable indicating whether the factor was selected as among the most important for living a good life as MIDUS Time 1 was the focal predictor. Perception-congruent wellbeing at MIDUS Time 1 was included as a covariate so that the models were predicting residualized change. Continuous variables were z-standardized to aid in interpretation of effect sizes.
We also conducted sensitivity analyses for Aims 3a-3c adjusting for age, sex, and years of education. These sensitivity analyses were not preregistered and are reported in the Supplementary Online Materials. The direction and statistical significance of results remained the same with two exceptions, which are noted in text.
Aim 4: Perceptions of a Good Life and Physical Health
Participants were included in mortality analyses for Aims 4a–4c if they completed the measure of perceptions of a good life at MIDUS Time 1 (N = 4041). Participants were included in the other analyses for Aim 4a if they completed the measure of perceptions of a good life and the concurrent measurement occasion of self-evaluated physical health and/or chronic health conditions at MIDUS Time 1 (N = 4041). Participants were included in the other analyses for Aims 4b and 4c analyses if they completed the measure of perceptions of a good life at MIDUS Time 1 and the self-evaluated physical health and/or chronic health conditions measure at MIDUS Time 1 and MIDUS Time 2 (N = 2900). Given the sample size and our alpha level of .01, we had 80% statistical power to detect small concurrent and prospective associations (equivalent to r = .06 or larger) with self-evaluated physical health and chronic conditions in MIDUS. Given the sample size, our alpha level of .01, and the mortality rate of 14.5%, we had 80% statistical power to detect hazard ratios of 0.69 or smaller (or the inverse, 1.45 or larger). Because we expected associations with health outcomes to be small, we did not have sufficient power to test Aim 4 in MIDJA. In addition, mortality data was not available in MIDJA.
To examine associations with self-evaluated physical health, we used ordinal regression to account for the ordinal nature of the outcome variable. To examine associations with number of chronic health conditions, we used zero-inflated Poisson regression to account for the count nature of the outcome variable. This type of model provides estimates for the effect of the predictor on the number of conditions (the count model) and a separate estimate for the effect of the predictor on the likelihood of having at least one condition (zero-inflated model). To examine associations with mortality, we used Cox proportional hazards regression to account for the survival nature of the outcome variable.
For concurrent associations (Aim 4a), we examined perceptions of a good life, self-evaluated physical health, and number of chronic health conditions at MIDUS Time 1. Because the concurrent associations are descriptive in nature, we did not adjust for any covariates.
For prospective associations (Aim 4b), we examined perceptions of a good life at MIDUS Time 1, self-evaluated physical health and number of chronic health conditions at MIDUS Time 2, and mortality through 2020. In the prospective models predicting self-evaluated physical health, we adjusted for baseline self-evaluated physical health, and potential sociodemographic confounders (age, sex, and years of education). In the prospective models predicting number of chronic health conditions, we adjusted for baseline chronic health conditions, and the same sociodemographic variables. In the models predicting mortality risk, we adjusted for baseline self-evaluated physical health, baseline chronic health conditions, and the same sociodemographic covariates.
To test whether perceptions of a good life moderated the effects of wellbeing on physical health (Aim 4c), we included perceptions of a good life in MIDUS, perception-congruent wellbeing at MIDUS Time 1, and their interaction as predictors of self-evaluated physical health and chronic health conditions at MIDUS Time 2, and mortality, adjusting for the same covariates as described in Aim 4b.
Results
Aim 1: Cultural Differences in Perceptions of a Good Life
The percentage of participants in the U.S. and Japan that selected each factor as among the most important for living a good life are shown in Table 2. In the U.S. sample, the top five most commonly endorsed factors in descending order were “positive relationships with family” (67.3%), “faith” (56.9%), “positive attitude” (53.0%), “the absence of illness” (35.6%), and “positive relationships with friends” (29.1%). In the Japanese sample, the top five most commonly endorsed factors in descending order were “physical fitness and strength” (79.8%), “positive relationships with family” (76.4%), “enough money to meet basic needs” (50.1%), “the absence of illness” (41.1%), and “positive attitude” (33.9%). Thus, three of the top five factors were shared across the two samples, whereas two of the top five factors were unique across the two samples.
Next, we considered whether statistically significant differences existed between the two samples. Relative to participants in the US, participants in Japan were less likely to perceive “sense of purpose,” “positive attitude,” “sense of accomplishment,” and “faith” as among the most important factors for living a good life. Moreover, participants in the Japanese sample were more likely to perceive “physical fitness and strength,” “having enough money to meet basic needs,” “loving and caring for myself,” “autonomy,” “relaxation, peacefulness, and contentment,” and “positive relations with family” as among the most important factors for living a good life.
Aim 2: Age Differences in Perceptions of a Good Life
Age differences in perceptions of a good life are shown in Table 4. One finding was consistent in the US and Japan. In both samples, people who perceived “absence of illness” as among the important factors for living a good life tended to be older. Several additional age differences were observed in the US sample, but not in the less well-powered Japanese sample. People who perceived hedonic factors, such as “enjoyment of life’s pleasure” and “relaxation, peacefulness, and contentment,” as among the most important factors for living a good life tended to be younger. Results were more mixed for eudaimonic factors. People who perceived “sense of purpose” and “loving and caring for oneself” as among the most important factors for living a good life tended to be younger, whereas people who perceived “autonomy” as among the most important factors for living a good life tended to be older. Only one age difference was observed for social factors: people who perceived “positive relationships with friends” as among the most important factors for living a good life tended to be younger. Finally, people who perceived “having a good job” as among the most important factors for living a good life tended to be younger, and people who perceived “absence of illness,” “having enough money to meet basic needs” and “faith” as among the most important factors for living a good life tended to be older.
In exploratory analyses suggested during the review process, we calculated the correlation between the vector of ds in MIDUS and the vector of ds in MIDJA. Age differences in MIDUS were moderately positively correlated with age differences in MIDJA (r = .42). This suggests that the pattern of age differences observed in MIDUS was somewhat similar to the pattern of age differences observed in MIDJA.
Aim 3: Perceptions of a Good Life and Wellbeing
Table 5 shows concurrent associations between perceptions of a good life and psychological wellbeing. No statistically significant associations were observed in the less well-powered Japanese sample. However, in the larger U.S. sample, perceiving eudaimonic and hedonic factors as among the most important for living a good life showed mixed associations with overall wellbeing. Some factors were associated with greater wellbeing (“sense of purpose,” “continual learning and growth,” and “positive attitude”), some factors were associated with slightly lower wellbeing (“loving and caring for myself,” “relaxation, peacefulness, and contentment”), and two factors were not associated with wellbeing (“autonomy” and “enjoyment of life’s pleasures”).
Perceiving social factors as among the most important for living a good life was associated with greater wellbeing, across all three social factors.
Finally, perceiving “absence of illness,” “having a good job,” and both money-related factors, as among the most important factors for living a good life was associated with worse wellbeing, whereas perceiving “faith” as among the most important factors for living a good life was associated with greater wellbeing.
Table S3 shows the results of sensitivity analyses adjusting for age, sex, and years of education. The direction and statistical significance of all associations remained the same, with the exception of sense of purpose. In sensitivity analyses adjusting for sociodemographic covariates, perceiving sense of purpose as important for a good life was no longer associated with psychological wellbeing.
In exploratory analyses suggested during the review process, we calculated the correlation between the vector of ds in MIDUS and the vector of ds in MIDJA. Psychological wellbeing associations in MIDUS were strongly positively correlated with psychological wellbeing associations in MIDJA (r = .73). This suggests that the pattern of associations with overall psychological wellbeing observed in MIDUS was highly similar to the pattern of associations with overall psychological wellbeing observed in MIDJA.
Table 6 shows concurrent associations between perceptions of a good life and perception-congruent facets of wellbeing. Like with overall psychological wellbeing, the following statistically significant associations were observed in the larger U.S. sample, but not in the smaller and less well-powered Japanese sample. People’s perceptions of a good life were generally positively related to their experiences of perception-congruent wellbeing. For example, people who perceived “sense of purpose” as among the most important factors for living a good life tended to report a higher sense of purpose. This pattern was observed for “autonomy,” “continual learning and growth,” “positive attitude,” “positive relationships with family,” and “positive relationships with friends.” However, this was not observed for “loving and caring for myself” or “relaxation, peacefulness, and contentment,” where associations with perception-congruent wellbeing were null. In the smaller Japanese sample, this pattern only held for “continual learning and growth.”
Table S4 shows the results of sensitivity analyses adjusting for age, sex, and years of education. The direction and statistical significance of all associations remained the same.In exploratory analyses suggested during the review process, we calculated the correlation between the vector of ds in MIDUS and the vector of ds in MIDJA. Perception-congruent wellbeing associations in MIDUS were moderately positively correlated with perception-congruent wellbeing associations in MIDJA (r = .36). This suggests that the pattern of perception-congruent wellbeing associations observed in MIDUS was somewhat similar to the pattern of perception-congruent wellbeing associations observed in MIDJA.
Table 7 shows associations between perceptions of a good life and longitudinal change in perception-congruent wellbeing. Consistent with our hypothesis, people experienced increases in sense of purpose, personal growth, and optimism when their perceptions of a good life included “sense of purpose,” “continual learning and growth,” and “positive attitude,” respectively. This pattern was not observed for autonomy, positive relationships with others, self-acceptance (i.e., “loving and caring for myself”), or experiences of calm, and peace (“relaxation, peacefulness, contentment”).
Table S5 shows the results of sensitivity analyses adjusting for age, sex, and years of education. The direction and statistical significance of all associations remained the same, with the exception personal growth. Perceiving “continual learning and growth” as important for a good life was no longer associated with increases in personal growth.
Aim 4: Perceptions of a Good Life and Physical Health
Concurrent associations between perceptions of a good life and physical health.

Note. 99% confident intervals are shown. Effect sizes are odds ratios (OR) and incident risk ratios (IRR).
Concurrent associations between eudaimonic perceptions of a good life and physical health were mixed. People who perceived “sense of purpose” and “continual learning and growth” as among the most important factors for living a good life tended to have better concurrent self-evaluated physical health. In contrast, people who perceived “loving and caring for myself” as among the most important factors for living a good life tended to have worse concurrent self-evaluated physical health and more chronic health conditions. Further, people who perceived “autonomy” as among the most important factors for living a good life tended to have more chronic health conditions.
Concurrent associations between hedonic perceptions of a good life and physical health were similarly mixed. People who perceived “positive attitude” as among the most important factors for living a good life tended to have better concurrent self-evaluated physical health and fewer chronic health conditions. In contrast, people who perceived “relaxation, peacefulness, and contentment” as among the most important factors for living a good life tended to have worse concurrent self-evaluated physical health and more chronic health conditions.
Only one statistically significant association was observed between social perceptions of a good life and physical health. People who perceived “positive relationships with family” as among the most important factors for living a good life tended to have fewer chronic health conditions.
Regarding health-related factors, people who perceived “physical fitness and strength” as among the most important factors for living a good life tended to have better concurrent self-evaluated physical health and fewer chronic health conditions. In contrast, people who perceived “absence of illness” as among the most important factors for living a good life tended to have more chronic health conditions.
Interestingly, people who perceived “having a good job” and “faith” as among the most important factors for living a good life tended to have worse concurrent self-evaluated physical health but fewer chronic health conditions. Finally, people who perceived “enough money to meet basic needs” as among the most important factors for living a good life tended to have worse concurrent self-evaluated physical health and more chronic health conditions.
Prospective associations between perceptions of a good life and physical health.
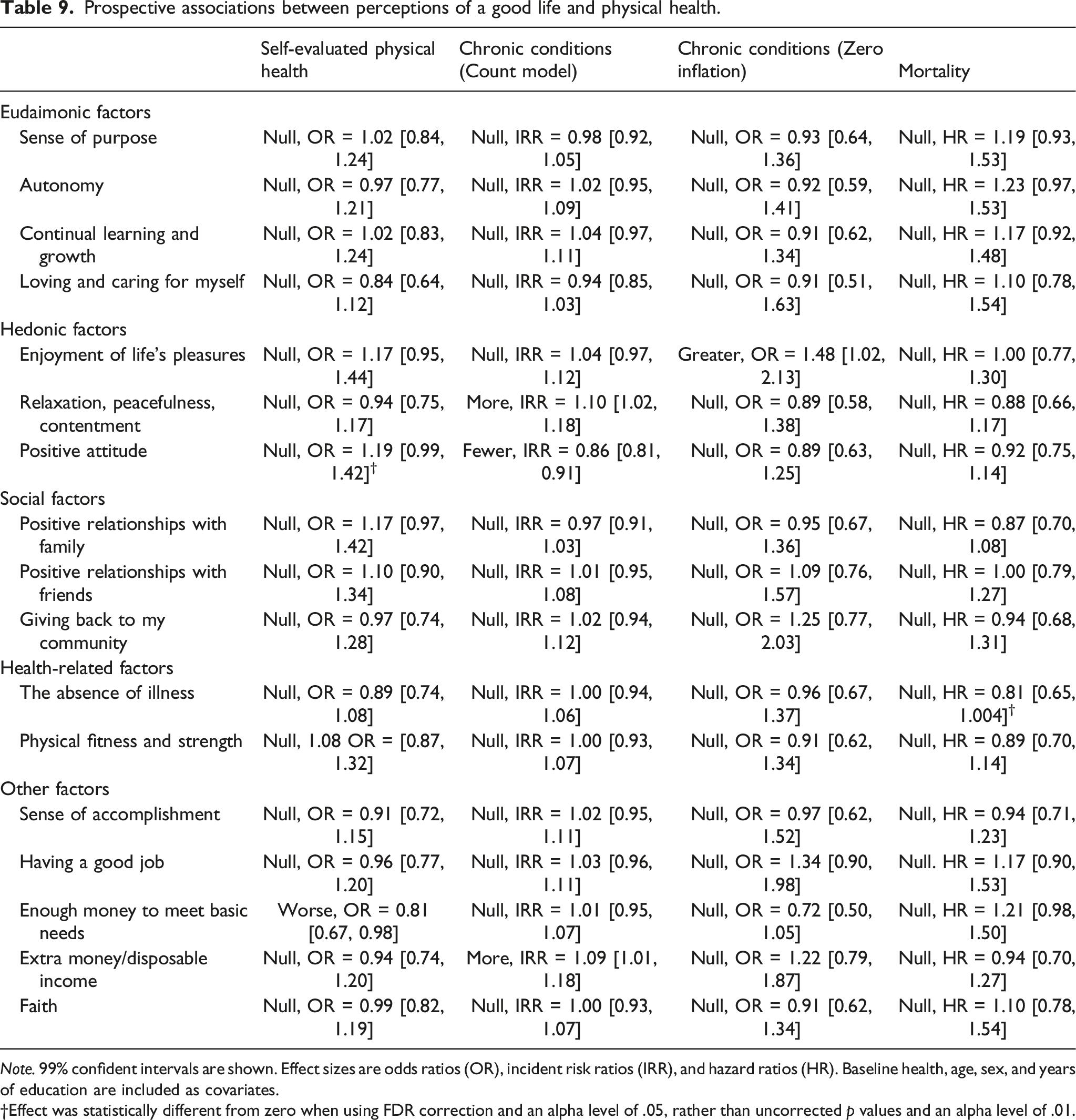
Note. 99% confident intervals are shown. Effect sizes are odds ratios (OR), incident risk ratios (IRR), and hazard ratios (HR). Baseline health, age, sex, and years of education are included as covariates.
†Effect was statistically different from zero when using FDR correction and an alpha level of .05, rather than uncorrected p values and an alpha level of .01.
None of the eudaimonic, social, or health-related factors were prospectively associated with any of the health outcomes.
All of the hedonic factors were prospectively associated with number of chronic health conditions. Perceiving “enjoying life’s pleasures” as among the most important factors for living a good life predicted greater likelihood of at least one chronic health condition 9 years later, and perceiving “relaxation, peacefulness, and contentment” as among the most important factors for living a good life predicted more chronic health conditions 9 years later. In contrast, perceiving “having a positive attitude” as among the most important factors for living a good life predicted fewer chronic health conditions 9 years later.
In addition, perceiving “having enough money to meet basic needs” as among the most important factors for living a good life predicted worse self-evaluated physical health 9 years later and greater mortality risk, and perceiving “having extra money/disposable income” as among the most important factors for living a good life predicted more chronic health conditions 9 years later.
Supplementary Table S6 shows the results of multiple regression models in which the interaction of perceptions of a good life and experiences of wellbeing predicted physical health outcomes. Contrary to our hypothesis, optimism was associated with fewer chronic health conditions, but this association was attenuated for individuals who perceived “positive attitude” as among the most important factors for living a good life. Similarly, positive relationships with others was associated with fewer chronic health conditions, but that association was attenuated for individuals who perceived “positive relationships with friends” as among the most important factors for living a good life.
Discussion
The present research examined similarities and differences in people’s perceptions of a good life, and implications of those perceptions for wellbeing and physical health. People’s perceptions of a good life included a combination of eudaimonic (e.g., “sense of purpose”), hedonic (e.g., “enjoyment of life’s pleasures”), social (e.g., “positive relationships with family”), health-related (e.g., “absence of illness”), and other (e.g., “faith”) factors. Some factors were generally perceived to be important in both the U.S. and Japan, such as “positive relationships with family,” “positive attitude,” and “absence of illness.” Other factors were substantially more common in the U.S. (e.g., “faith”) or in Japan (e.g., “physical fitness and strength”). In addition to these cultural differences, we observed age-related similarities and differences in several factors related to meaningful lifespan developmental priorities. For example, family relationships were generally perceived to be important by both younger and older adults, whereas older adults tended to perceive “absence of illness” as among the most important factors for living a good life and younger adults tended to perceive “having a good job” as among the most important factors for living a good life. In addition to these group-level similarities and differences, individual differences in several aspects of perceptions of a good life were concurrently and prospectively related to wellbeing and physical health. Below, we discuss implications of these findings for our understanding of what people think of as “a good life.”
Perceptions of a Good Life
We classified factors into eudaimonic, hedonic, social, health-related, and “other” categories for descriptive purposes and aid in interpretation of findings. In both the U.S. and Japan, people’s perceptions of a good life included factors from all five categories (e.g., eudaimonic, hedonic, social, health-related, and “other”). In fact, the top five most commonly endorsed factors in both countries spanned all categories except for eudaimonic constructs. This suggests that people’s perceptions of a good lifespan many different aspects of life. When considering the proportion of people who selected each factor as important for living a good life, interesting patterns emerged. For example, “positive relationships with family” was among one of the most commonly endorsed factors, but “giving back to my community” was among one of the least commonly endorsed factors. This suggests that while people perceive others as important to living a good life, fostering personal relationships may be viewed as more important than giving back, or close others may be considered more important than distal others. The emphasis on personal relationships, particularly with one’s family, is consistent with prior research showing that family is the most prominent source of meaning in life across 17 distinct countries (Pew Research Center, 2021).
Overall, people’s perceptions of a good life tend to include factors that are well-represented in prominent models of wellbeing, but also include factors that are often considered causes rather than components of wellbeing, such as faith and money. Just as wellbeing definitions are debated among contemporary wellbeing theorists, there were instances in which a given factor could have been classified into more than one category. Most notably, we classified “positive relationships with family,” “positive relationships with friends,” and “giving back to one’s community” as social factors. However, prior research has considered contributions to others to be a eudaimonic conception of wellbeing (e.g., McMahan & Estes, 2011b), and Ryff’s (1989) model of eudaimonic wellbeing includes positive relationships with others. Further, we classified “positive attitude” as hedonic. However, the closely related construct of optimism has both eudaimonic and hedonic components (Bouchard et al., 2017). Despite these complexities, the 17 factors largely mapped onto existing models of wellbeing and captured a broad spectrum of personal attributes and life circumstances.
Importantly, the measurement instrument used to assess perceptions of a good life constrained the possible conclusions that we could draw about those perceptions. It is possible that important factors were omitted from the list of 17 possible factors, limiting our ability to detect those elements of people’s perceptions of a good life. In addition, all participants were instructed to select exactly five factors. If participants were given the freedom to select any number of items, we may have come to a different set of conclusions. Finally, future research should consider individual differences in the relative importance of different factors, as well as in combinations of multiple factors. For example, future research could benefit from asking participants to rank order items, rate the importance of each item, or select as few or as many items as they wished.
Cultural Differences in Perceptions of a Good Life
The present findings are consistent with the notion that perceptions of a good life contain both shared and culturally distinct elements. The most pronounced differences were a greater emphasis on “faith” in the US and a greater emphasis on “physical fitness and strength” in Japan. The greater emphasis on faith in the U.S. is consistent with a 2009 Gallup poll showing that more than two-thirds of people in the U.S. but less than one-fourth of people in Japan consider religion to be an important part of their daily lives (Crabtree, 2010) and that more people in the U.S. compared to Japan consider faith a source of meaning in their lives (Pew Research Center, 2021). Similarly, the greater emphasis on physical fitness and strength in Japan is consistent with the integration of exercise into daily life in Japan (e.g., at the workplace; Jindo et al., 2019).
Prior research on cultural differences in lay conceptions of wellbeing has found a greater emphasis on social factors in Eastern cultures relative to Western cultures (Ford et al., 2015; Lu & Gilmour, 2004; Uchida & Kitayama, 2009). We did not observe strong evidence for this pattern in the present research. Participants in Japan were somewhat more likely to perceive “positive relationships with family” as among of the most important factors for living a good life, but this factor was commonly endorsed in both countries. The other two social factors that we examined—“positive relationships with friends” and “giving back to one’s community”—were equally common in the U.S. and Japan. Some prior research has also found that people in the US are more likely to incorporate positive emotion and personal achievement into their conceptions of wellbeing (Lu & Gilmour, 2004; Uchida & Kitayama, 2009). We found mixed evidence for these differences in perceptions of a good life. For example, there was no difference between the U.S. and Japan in perceptions of “enjoyment of life’s pleasures” as among the most important factors for living a good life and perceiving “relaxation, peacefulness, and contentment” as among the most important factors for living a good life was more common in Japan. However, “positive attitude” was more commonly endorsed in the US Regarding personal achievement, US participants were more likely to perceive “sense of accomplishment” as among the most important factors for living a good life, but specific achievement-related factors such as “having a good job” did not differ between the two countries.
An important limitation of Aim 1 is that we drew inferences about cultural similarities and differences based on country of data collection without assessing individuals’ cultural values. This approach provides initial insight into the nature and magnitude of similarities and differences between the two cultures, but future research should investigate relationships between perceptions of a good life and the cultural values of individuals within each culture, as there is more variability in cultural values within cultures than between them (Hamamura, 2012). Further, although we discussed differences in Western and Eastern philosophy, values of collectivism and individualism, and differences in religious trends, we cannot conclude from these data alone that these factors underlie the observed differences in perceptions of a good life. Indeed, the dominance of individualistic and collectivist values within the US and Japan has been debated (Heine et al., 2002; Oyserman et al., 2002). Observed differences may also be due to other features of the samples and research design, rather than due to cultural differences. For example, the US sample was a national probability sample, whereas the Japanese sample was drawn from a major metropolitan area. Thus, observed differences could be attributed to differences in urbanicity or relative social status (e.g., Takahashi et al., 2018).
Age Differences in Perceptions of a Good Life
Of the differences that were observed, most were only statistically significant in the larger US sample. This is not surprising given that the smaller Japanese sample was underpowered to detect the majority of the observed effect sizes. The vector of effect sizes for age differences in the US sample was moderately positively correlated with the vector of effect sizes for age differences in the Japanese sample, suggesting that many of the age differences observed in the US may replicate in a more well-powered Japanese sample.
The largest age differences were for “absence of illness” and “having a good job.” People who perceived “absence of illness” as important for living a good life tended to be older, perhaps because illness is more salient in older adulthood when health problems are most prevalent. This finding is also consistent with prior research which found that older adults were more likely to rate the avoidance of negative experiences as important for wellbeing (McMahan & Estes, 2011a). People who perceived “having a good job” as among the most important factors for living a good life tended to be younger. This is consistent with selection, optimization, and compensation theory (Baltes, 1997; Baltes & Baltes, 1990; Freund & Baltes, 1998, 2002) which suggests that older adults deprioritize achievement-related goals. Moreover, the life tasks literature (Havighurst, 1972; Hutteman et al., 2014) suggests that achieving satisfactory work status is a critical developmental task of middle adulthood, whereas older adults focus more on the transition from the workplace. As such, future research should consider following participants longitudinally to consider whether perceptions of the good life change to reflect the primary developmental tasks of the given period.
Although socioemotional selectivity theory suggests that older adults tend to value emotional meaning and enjoyment of the present moment (Carstensen, 1993, 2006, 2021; Carstensen et al., 1999), we did not find evidence for a greater emphasis on emotion experience in older adults’ perceptions of a good life. In fact, people who perceived “enjoying life’s pleasures” and “relaxation, peacefulness, and contentment” as among the most important factors for living a good life tended to be younger. This is consistent with prior research which found that younger adults were more likely to rate the experience of pleasure as important for wellbeing (McMahan & Estes, 2011a). Prior research also found several factors that were common components of wellbeing conceptions across the adult lifespan, such as an others-orientation. Our findings are partially consistent with this observation. For example, neither “positive relationships with family” nor “giving back to my community” differed by age.
An important limitation of Aim 2 is that we examined cross-sectional associations between perceptions of a good life and age, rather than examining whether perceptions of a good life changed within individuals as they age. Specifically, we compared the average age of participants who perceived a particular factor as among the most important for living a good life to those who did not select that factor. We took this approach because the dichotomous nature of the perceptions of a good life measure made longitudinal within-person comparisons difficult. Thus, we cannot conclude from the present research whether age differences were driven by cohort effects or the aging process. For example, younger adults were more likely to include “loving and caring for oneself” as among the most important factors for living a good life. It is unclear whether this is because people tend to place less emphasis on loving and caring for themselves as they age, or because younger adults grew up during a time period in which there was greater societal emphasis on loving and caring for oneself. Future research should track longitudinal change in perceptions of a good life to disentangle age, period, and cohort effects.
Perceptions of a Good Life and Implications for Wellbeing
Perceptions of a good life were associated with concurrent wellbeing and longitudinal change in wellbeing. Like with age differences, the majority of statistically significant effects were observed in the larger US sample, and not in the smaller Japanese sample which was underpowered to detect the same effect sizes. However, the vectors of effect sizes observed in the US sample were strongly positively correlated with the vectors of effect sizes observed in the Japanese sample, providing some evidence that the associations may be similar in both countries. Consistent with prior research on lay conceptions of wellbeing (e.g., McMahan et al., 2013), certain eudaimonic perceptions of a good life tended to be associated with greater overall eudaimonic wellbeing (e.g., “sense of purpose” and “continual learning and growth”). The only hedonic factor that was associated with greater overall eudaimonic wellbeing was “positive attitude,” which has both hedonic and eudaimonic features.
The present research also builds on prior work by examining a broad range of factors that people might perceive as important for living a good life. Consistent with research on social support and wellbeing (e.g., Weston et al., 2021), social perceptions of a good life were consistently related to greater wellbeing, perhaps because people who perceive social factors as important for a good life are more likely to invest in their social relationships. For health-related factors, perceiving “absence of illness” as among the most important factors for living a good life was associated with lower wellbeing. This may be driven in part because people living with health conditions may be more likely to recognize the importance of good health and may also have lower wellbeing. Alternatively, the association with lower wellbeing may be driven by the emphasis on avoiding a negative experience or perhaps by the emphasis on a factor that is often outside of an individual’s control. Finally, an emphasis on job and money-related factors was consistently associated with lower wellbeing. This is consistent with prior research demonstrating that valuing materialism (Dittmar et al., 2014) and linking wellbeing motives to financial goals (Garđarsdóttir et al., 2009) are both associated with lower wellbeing.
Across several types of wellbeing, perceptions of a good life were associated with higher levels of perception-congruent wellbeing. For example, people who perceived “sense of purpose” as among the most important factors for living a good life tended to be higher in sense of purpose. These findings may be explained by perception-behavior links, which have been found in prior research on lay conceptions of wellbeing (McMahan et al., 2013). For example, people who perceive “sense of purpose” as important may be more likely to engage in purposeful activities, and experience greater sense of purpose as a result. We found indirect evidence for this possibility in longitudinal analyses examining perceptions of a good life and subsequent changes in wellbeing. People experienced increases in sense of purpose, personal growth, and optimism when their perceptions of a good life included “sense of purpose,” “continual learning and growth,” and “positive attitude,” respectively. This may suggest that people are motivated to pursue elements of wellbeing that they view as particularly important. Future research should test this possibility by examining motives, behaviors, and wellbeing alongside perceptions of a good life in longitudinal designs.
Perceptions of a Good Life and Physical Health
We observed several statistically significant concurrent associations between perceptions of a good life and physical health, but most did not hold prospectively when adjusting for baseline health and sociodemographic characteristics. A key exception was the hedonic factors. Perceiving “enjoyment of life’s pleasures” and “relaxation, peacefulness, and contentment” as among the most important factors for living a good life was prospectively associated with worse physical health. These findings may suggest that certain hedonic perceptions of a good life are associated with health-detrimental behaviors (e.g., inactivity or indulgence). In contrast, perceiving “positive attitude” as among the most important factors for living a good life was associated with better physical health. Coupled with the observed positive association between perceiving “positive attitude” as among the most important factors for living a good life and optimism, this finding is consistent with research demonstrating the health benefits of optimism (e.g., Bouchard et al., 2017; Trudel-Fitzgerald et al., 2019). Additionally, perceiving “having enough money to meet basic needs” as among the most important factors for living a good life predicted worse physical health. One potential explanation is that people whose basic needs are not being met are more likely to perceive “having enough money to meet basic needs” as important for living a good life and are also at greater risk for poor health. Future research should additionally consider more health-related perceptions, such as “being in good health” or “living a long life.” Such health-related perceptions may be more strongly associated with actual physical health.
We also observed two unexpected interactions between aspects wellbeing, perceptions of a good life, and physical health. Specifically, the protective effects of optimism and having positive relationships with others were attenuated for people who perceived those factors as among the most important for living a good life. One possibility is that experiencing these types of wellbeing and perceiving them as important for living a good life are similarly beneficial for health, but the benefits are not cumulative. However, because we only observed this pattern for two factors and given the counterintuitive nature of the pattern, we caution against overinterpretation without replication.
An important consideration in Aims 3 and 4 is the use of self-report questionnaires to assess perceptions of a good life, as well as wellbeing and health. Although self-report is arguably an ideal method to assess people’s subjective perceptions and experiences, shared method effects and self-report biases may have inflated the observed associations. Our physical health measures ranged from more subjective (i.e., self-reported health), to less subjective (i.e., chronic conditions), to objective (i.e., mortality). We found a similar number of statistically significant associations with self-reported health and chronic conditions, but no associations with mortality. This may suggest that people’s perceptions of a good life are more important for their subjective experiences of wellbeing and health, relative to more objective health outcomes.
In addition to shared method effects, third variable confounders such as personality traits and life circumstances could impact perceptions of a good life as well as wellbeing and health. This is particularly important for interpreting concurrent associations, which should not be interpreted as causal. In prospective analyses predicting wellbeing and health, we controlled for baseline levels of wellbeing and health, respectively. This means that any potential third variable confounder would have to causally affect perceptions of a good life at Time 1, and causally affect wellbeing or health at Time 2 independent of its effects on wellbeing or health at Time 1. This is possible in the case of a life circumstance proximal to Time 1 that had an immediate effect on perceptions of a good life, but that took longer to impact wellbeing and health. For example, a recent argument with a family member could immediately impact perceptions of the importance of family relationships, but strained family relationships may take longer to impact wellbeing and health. In contrast, relatively stable dispositions like personality traits would be less likely to explain the observed prospective effects.
Constraints on Generality
The present research was conducted within the US and Japan between 2004 and 2016. A subset of study aims, including associations between perceptions of a good life and perception-congruent wellbeing, and perceptions of a good life and physical health were only conducted in the larger U.S. sample only. Just as perceptions of a good life contain both shared and distinct elements across cultures, there are likely to be both cultural similarities and differences in the wellbeing and health correlates of perceptions of a good life. Thus, the extent to which the present findings generalize outside of the cultural contexts in which they were studied remains an open empirical question. Perceptions that are associated with better wellbeing and health in the US may have different relationships to wellbeing and health in countries and cultures that place more or less value on those same factors.
It is also important to consider the historical context in which the present data were collected. For example, in MIDUS, Time 1 took place before the Great Recession (i.e., 2004–2006), and Time 2 took place after the Great Recession (i.e., 2014–2016). Perceptions of factors related to one’s job and income, as well as the wellbeing and health correlates of those perceptions could have been influenced by this historical context. In MIDJA, Time 1 took place before (i.e., 2008–2010) the largest earthquake ever recorded in Japan, and Time 2 took place after this event (2012–14). Research is mixed on the influence of natural disasters on individual differences such as personality (Damian et al., 2021; Milojev et al., 2014), and it remains an open question whether such major events influence people’s perceptions of a good life. In short, it is unlikely that perceptions of a good life can be completely extracted from the cultural and historical contexts in which those perceptions are held.
Concluding Comment
The human instinct to satisfy needs and strive toward a better life has led scholars and philosophers to focus on what makes for a good life. The current findings provide clear evidence that while some perceptions of a good life are shared by most people (e.g., positive family relationships), individuals also differ in their perceptions of what a good life looks like. How we view the good life may depend on our culture, our age, and our health and wellbeing. These findings point to an intricate interplay between perceptions of the good life and actually trying to live one—namely, we may strive toward congruence with what we think makes a good life, which could change over time. As such, our findings speak to two important implications. First, individualized programs to promote healthy development need to start by asking what people want in their lives. Second, researchers need to test whether these perceptions yield behavioral changes, which in turn may shape wellbeing and health.
Supplemental Material
Supplemental Material - Perceptions of a good life: Associations with culture, age, well-being, and health
Supplemental Material for Perceptions of a good life: Associations with culture, age, well-being, and health by Emily C Willroth, Gabrielle N Pfund, Daniel K Mroczek and Patrick L Hill in European Journal of Personality
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute on Aging (R01AG047154). Preparation of the manuscript was supported by a National Institute of Aging grant awarded to Daniel K. Mroczek (R01AG018436). The content is solely the responsibility of the authors and does not represent the official views of the National Institutes of Health.
Open Science statement
The present research involved secondary analysis of two public datasets. Thus, sample size was predetermined and sensitivity power analyses are reported in the “Analytic Approach” section of each aim. We also report inclusion criteria and all data exclusions in the “Analytic Approach” section of each aim. We report all measures that were analyzed as a part of the present investigation. Data and a complete list of measures included in the MIDUS and MIDJA studies can be found on the study website [https://www.icpsr.umich.edu/web/NACDA/series/203]. Analysis preregistration and statistical code can be found on OSF (https://osf.io/kn9vp). Analyses were preregistered in three separate preregistrations. Preregistration 1 was published on OSF (https://osf.io/u5jpt) first in August 2021. After analyses for Preregistration 1 were completed and results were known, Preregistrations 2a and 2b were drafted to address additional aims and follow-up questions. Preregistrations 2a (https://osf.io/dmp4e) and 2b (https://osf.io/tr6ud) were published on OSF simultaneously in September of 2021. Aims 1 and 2 were descriptive in nature and we did not make specific hypotheses. Aims 3 and 4 included descriptive aspects, as well as preregistered hypotheses. See Supplementary Table 1 for a mapping of study aims (Aims 1–4) onto preregistrations (Preregistrations 1, 2a, and 2b), and for documentation of additional non-preregistered analyses and one preregistration deviation. Analysis preregistration and statistical code can be found on OSF [![]() ].
].
Supplemental Material
Supplemental material for this article is available online.
Note
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.