
Abstract
Background:
Breastfeeding is a global priority. To provide culturally appropriate evidence-based lactation support, healthcare professionals need training. Different levels of training are available post registration; however, the impact of in-depth breastfeeding training, such as that leading to the International Board-Certified Lactation Consultant certification, has not been studied.
Research Aims:
To expand understanding of how in-depth training can assist healthcare professionals in gaining knowledge and skills, and improve breastfeeding related outcomes.
Methods:
A systematic review following PRISMA and Joanna Briggs Institute guidelines was conducted. Six electronic databases were searched between 2023 and 2024 and updated in August 2025. Studies were eligible for inclusion if participants where healthcare professionals, and the training was post-registration lasting longer than 20 hours and examined the impact on outcomes such as breastfeeding knowledge and skills, breastfeeding rates, hospital practices, healthcare professionals’ experiences, motivation, and learning needs, and women's experiences of support from healthcare professionals who had undertaken in-depth training. Study selection, data extraction and quality appraisal were conducted independently by two reviewers. Findings were synthesised narratively.
Results:
Three quantitative studies were included. All showed improved knowledge and skills following in-depth training. One study reported an increase in breastfeeding rates and another identified learning needs. No other outcomes were addressed. All studies had methodological limitations.
Conclusion:
The evidence-base for the provision and impact of in-depth breastfeeding trainings is extremely limited. Given that breastfeeding and lactation support is a public health imperative, this knowledge gap sets a priority for future research, including trainings leading to the IBCLC qualification.
Key Messages
No systematic review has explored in-depth breastfeeding trainings (defined in this review as being longer than 20 hours duration, taking place post-registration, and not being United Nations Children’s Fund [UNICEF]-Baby Friendly Hospital Initiative [BFHI] training) with regards to any of these outcomes: breastfeeding knowledge and skills, breastfeeding rates, hospital practices, women’s perceptions of breastfeeding support from health care practitioners (HCPs) who have attended in-depth training, and HCPs’ motivation, learning needs, and training experiences.
This review found that in-depth breastfeeding training improved healthcare professionals’ breastfeeding knowledge. No studies explored women’s perceptions of breastfeeding support from HCPs who attend in-depth breastfeeding training, and HCP’s motivation to attend in-depth lactation training, learning needs, and training experiences.
There is a paucity of research related to in-depth breastfeeding trainings, including those which lead to the IBCLC credential. Given that breastfeeding support is a crucial public health target, this gap in knowledge sets as a priority for future research.
Background
Improving breastfeeding rates is a global public health priority requiring a multi-factorial approach which targets sociocultural and health system changes (Rollins et al., 2016). As part of this multi-factorial approach, healthcare professionals (HCPs) among others, play a crucial role in supporting the initiation, establishment, and continuation of breastfeeding (Ikobah et al., 2020). To provide culturally appropriate evidence-based breastfeeding support, HCPs need education that enhances their knowledge and skills and improves their practice (Yang et al., 2018). Lack of education and inconsistency in information given to families can translate into early cessation of breastfeeding (Hauck et al., 2011; Khoury et al., 2002; Pérez-Escamilla, 2019; Simmons, 2002). This can lead to early introduction of infant formula and an increase in health risks for the mother–infant dyad.
On one side, there is no international consensus on how much and what depth of breastfeeding training HCPs should have (Mulcahy et al., 2022), and on the other, many HCPs do not have enough breastfeeding knowledge. The need for more breastfeeding education for HCPs post registration contrasts with the lack of standardisation of educational opportunities as shown in Mulcahy and colleagues’ (2022) systematic review. In this systematic review, post registration refers to continuous education, further learning, or any qualification a professional undertakes after completing their university degree or gained their license to practice. Exploring data from different levels of trainings, five systematic reviews (Balogun et al., 2017; Beake et al., 2011; De Jesús et al., 2016; Gavine et al., 2017; Spiby et al., 2009) showed a lack of standardisation regarding: hours of education, curricula content, and competency-based frameworks. Gavine and colleagues’ (2017) systematic review urged for high quality studies to inform effective breastfeeding training options. The terms “education” and “training” are often used interchangeably. According to Blair and Serafini (2016) training is more focus oriented and specific, shorter, and provides practical skills. Education has a broader, more formal, connotation and can last several years. “Training” is used in this review because what is studied does not always correspond to formal education.
To provide clarity around the levels of trainings, the Lactation Management Curriculum Guide was developed by Wellstart International. The aim was to integrate breastfeeding management knowledge and skills in the curriculum of medicine, nursing, and nutrition programmes (Wellstart International, 2009), and it defined three levels of professional responsibility. This curriculum guide is not an established way of categorising lactation training and is not widely used. However, it informed our review’s classification given that the current literature has no universally accepted distinction in levels of lactation trainings needed for HCPs. This classification includes training hours and scope of practice. Grounded on Bloom’s revised taxonomy, breastfeeding education should distinguish between levels of thinking or cognitive complexity, which require more structured learning (Bloom, 2014). In addition, as suggested by Ericsson’ theory of deliberate practice, learning incorporates a progression from basic knowledge to practical application and ultimately leads to depth of specialisation (Ericsson, 2008).
Level I (basic) refers to pre-registration/university education for medical students and other HCPs who will not specialise in prenatal or post-natal care but who need to learn the fundamentals of breastfeeding. Level I ensures a minimum competency and should be universal, given to all HCPs who encounter breastfeeding dyads. The length and depth vary with some professionals feeling ill-prepared once they have graduated (Dodgson et al., 2014). Level II (intermediate) refers to training as a subject either during pre-registration or post-registration education and its purpose is consistency of knowledge and skills among HCPs. An example of a Level II training is the United Nations Children Fund (UNICEF) Baby Friendly Hospital Initiative (BFHI), which is 20 hours long (World Health Organisation & UNICEF, 2020) and offers a multidisciplinary programme with supervised clinical work (WHO, 2020). The available breastfeeding training literature makes the distinction between pre-registration and UNICEF BFHI training but does not define in-depth training. As there are no universally accepted criteria for in-depth training, we adopted an “arbitrary” length of more than 20 hours as a cut-off. Level III (advanced) refers to “in-depth” training for those who specialise in breastfeeding care, such as International Board Certified Lactation Consultants (IBCLCs), those who are in charge of delivering UNICEF BFHI training, or Breastfeeding and Lactation Medicine Physicians. Level III HCPs supervise, mentor and teach Level I and Level II staff. Thus, Level III includes trainings greater than 20 hours, defined as the minimum structured hours needed to introduce more advanced knowledge and skills and align with certain competency frameworks. It reflects a shift in cognitive complexity and scope of practice, not just duration.
Globally, there are formal programmes (Master’s degrees or Post Graduate Diplomas in Human Lactation/Infant Feeding) and numerous Level III informal, yet comprehensive trainings. Some serve as preparation to the International Board Lactation Consultants Examiners (IBLCE) examination. IBCLCs are breastfeeding and lactation care experts. The IBLCE examination requires 95 hours of education in addition to 1000 clinical hours (depending on the eligibility pathways) (IBCLC Commission, 2023). Thus, most IBCLC trainings are by definition in-depth.
Pre-registration breastfeeding training (Level I) has been studied widely in medicine and nursing (Mulcahy et al., 2022; Sandhi et al., 2023). An unpublished umbrella review aimed to integrate the results of multiple systematic reviews and meta-analyses into a comprehensive exploration of the impact of interdisciplinary training (formal such as UNICEF BFHI or non-accredited). Numerous systematic reviews have already examined the impact of the UNICEF BFHI training (Level II; Balogun et al., 2017; Beake et al., 2011; De Jesús et al., 2016; Gavine et al., 2017; Spiby et al., 2009; Ward & Byrne, 2011). For these reasons, we conducted a systematic review to expand understanding of how in-depth trainings (Level III) can assist HCPs in gaining knowledge and skills, and improve breastfeeding related outcomes.
Methods
Design
We conducted a systematic review to synthesise evidence on in-depth breastfeeding trainings to better understand what type of trainings HCPs need post registration and which are not the UNICEF BFHI training. The rationale for this review type was to appraise the impact these in depth-trainings have on at least one of the following outcomes: breastfeeding knowledge and skills of those HCPs attending in-depth trainings, breastfeeding rates or changes in hospitals’ practice, women’s perception of support received by those HCPs who have undertaken in-depth breastfeeding training, and HCPs’ experiences, motivation, and learning needs of their in-depth breastfeeding training. This review is reported according to the Preferred Reporting Items for Systematic Review and Meta Analysis (PRISMA) methodology (Tetzlaff et al., 2020). The protocol was registered with the International Prospective Register of Ongoing Systematic Reviews (PROSPERO; Registration number: CRD42023440545).
Sample: Defining the Articles Reviewed
This systematic review used a framework adapted from the Joanna Briggs Institute (JBI; Aromataris & Munn, 2020) comprising a combination of PICO and PICo, that is, PICOS (Population/participants, Interventions/Phenomena of interest, Comparison/Context, Outcomes, and Study type). The pre-determined study eligibility criteria are detailed in Table 1. Studies were eligible to be included if participants were registered HCPs, studies used a pretest post-test and examined any in-depth breastfeeding training. In the absence of an agreed definition of in-depth training (Level III), we defined it as longer than the 20-hour UNICEF BFHI course which can be considered a Level II. Studies from 2003 onwards were eligible to be included to align with the WHO/UNICEF Global Strategy for Infant and Young Child Feeding, which aimed to ameliorate the development and health of children by encouraging optimal feeding practices (WHO, 2003). Full articles that were available in English, Spanish, or French were included; all other languages were excluded.
Inclusion/Exclusion Criteria.
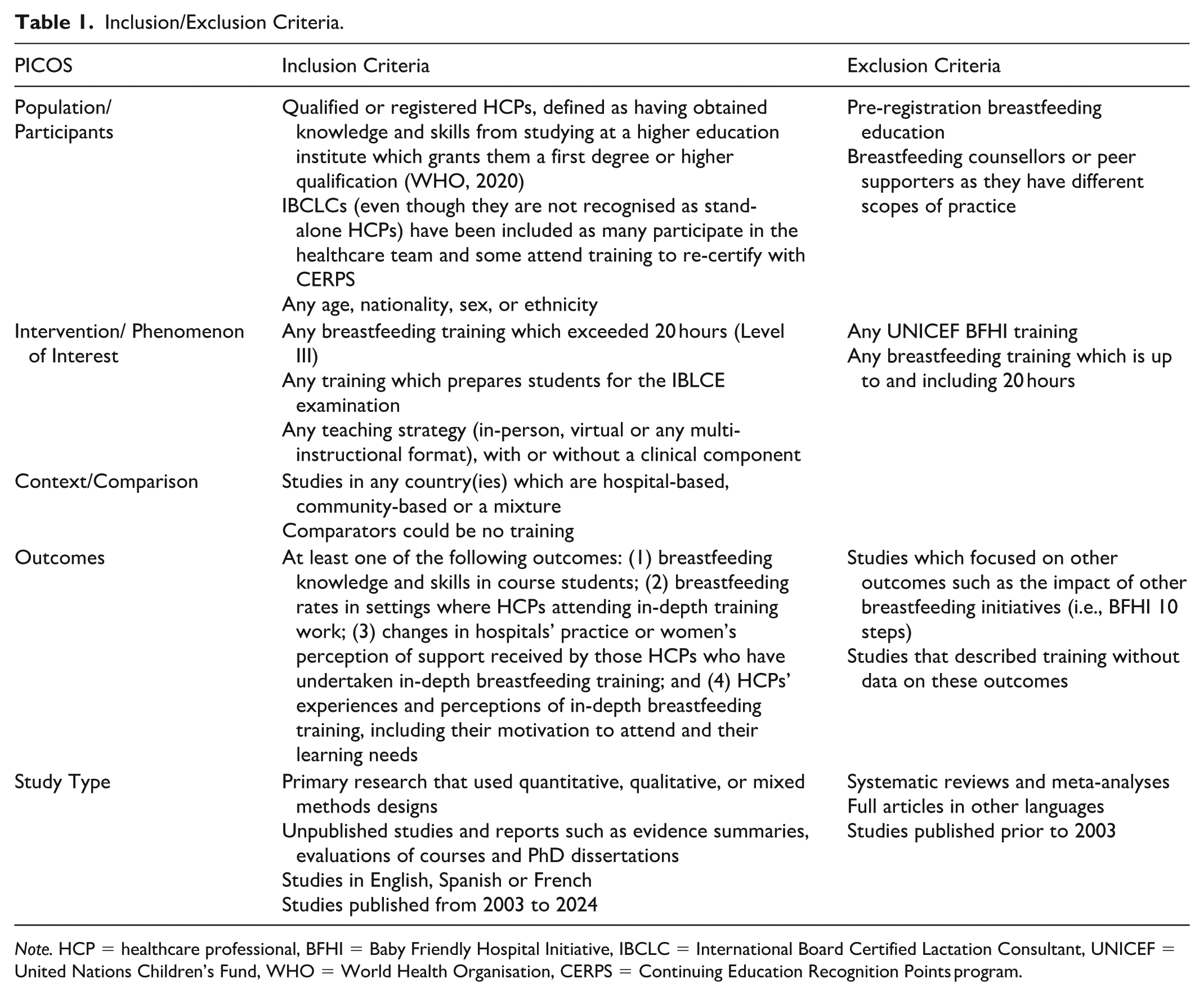
Note. HCP = healthcare professional, BFHI = Baby Friendly Hospital Initiative, IBCLC = International Board Certified Lactation Consultant, UNICEF = United Nations Children’s Fund, WHO = World Health Organisation, CERPS = Continuing Education Recognition Points program.
The electronic searches found 4,394 records (see Figure 1). After duplicates were removed, 2,965 records remained for title and abstract screening of which 2,905 were irrelevant. A total of 59 full texts were retrieved and assessed for eligibility and 56 studies were excluded. No further published material or other references from grey literature were found. Three quantitative studies were included in the review; no qualitative or mixed-methods studies were found. One study (Watkins et al., 2017) involved non-HCPs as well as HCPs, and it was not possible to isolate HCP data. The training met the length of the inclusion criteria, and because most participants were HCPs it was included. Given that the number of studies was small and there was heterogeneity in the outcome measurements, meta-analysis was not possible.
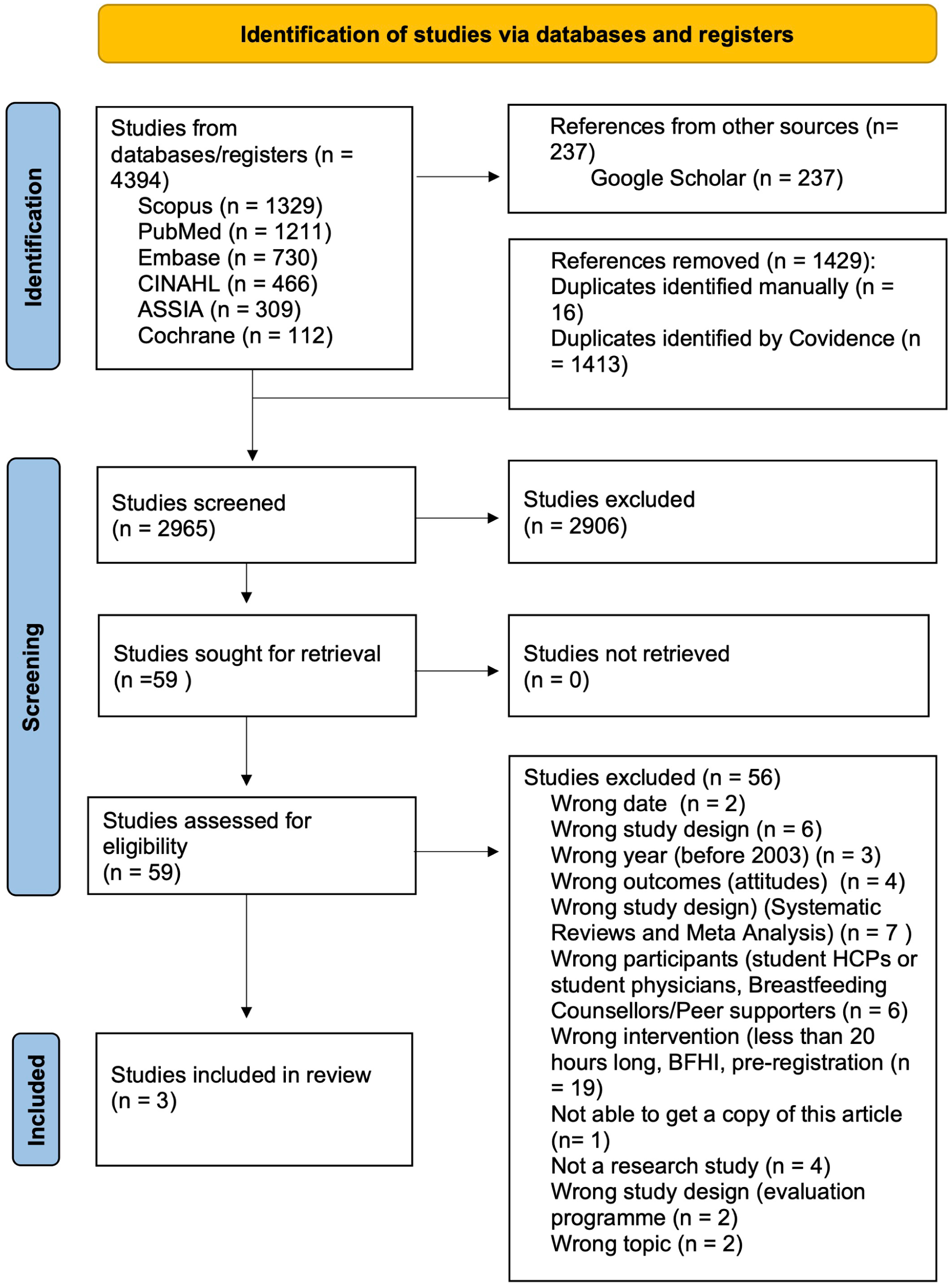
PRISMA flow.
Data Collection: The Search Strategy and Process
Six electronic databases ASSIA (ProQuest), CINAHL Plus (EBSCO), the Cochrane Library, Embase (Ovid), PubMed, and Scopus were searched initially between August 2023 and January 2024, and the search was updated in August 2025. Grey literature searches included the British Library Ethos, Open Access Theses and Dissertations and ProQuest Dissertations and Theses websites, GreyGuide, Open DOAR, CORE and Google Scholar. Hand searching was performed of the journal Clinical Lactation. Forward and backward citation from the included studies was also done. References from relevant systematic reviews were screened to locate further primary studies. In all, 20 IBCLC course providers were contacted via email to ask if they had done any studies on the impact of their trainings.
The search strategy was developed with the support of a librarian. Keywords and their synonyms were combined using Boolean operators. Index and free-text terms were generated and tailored for each database. These search terms mapped to the PICOS search strategy (see Supplementary File 1 in the online supplemental materials for a full search history). The main concepts were: breastfeeding/lactation AND training AND healthcare professionals (nurse, nutritionist, physician, GP, midwife, paediatricians, obstetrician, surgeon, health visitor or IBCLC). All search results were uploaded to the Covidence systematic review software (http://covidence.org) where duplicates were removed. Titles and abstracts were screened for relevance by two reviewers independently. Relevant full texts were retrieved and screened by applying the inclusion and exclusion criteria by two reviewers independently. Any disagreements were resolved by consensus with a third reviewer. Where studies did not include enough information to decide on eligibility, authors were contacted.
Most studies (n = 19) were excluded due to the wrong intervention (i.e., training was 20 hours or less, it was UNICEF BFHI training, or training took place during pre-registration). During the title/abstract phase, several studies did not even specify the length of the training. Thus, full texts were retrieved to find out length and many studies were excluded as the trainings were too short. Many of the excluded studies collected data through feedback forms without assessing outcomes. Nine authors were contacted via email for clarification regarding the exact length of their training. Five responded and one referred us back to the publication which was unclear. Six providers from the international IBCLC trainings who were contacted responded but none had formally evaluated their trainings.
Measurements
In-depth training was defined in this review as any training taking place post registration, which was not UNICEF BFHI training and was longer than 20 hours, either non/accredited or in/formal. In the absence of an accepted universal definition, the 20-hour UNICEF BFHI training was chosen as the cut-off point as it was considered a Level II training. The outcomes measured were any one of the following: breastfeeding knowledge and skills of those who participated in in-depth training, breastfeeding rates in hospitals where those participating in in-depth training worked, hospital practices (or other settings in which course participants worked), women’s perception of support from healthcare professionals who had undertaken in-depth training, and healthcare professionals’ motivation, learning needs, and experiences of participating in in-depth training.
The Knowledge, Attitudes and Practice (KAP) instrument which assesses what is known (knowledge), believed (attitude), and done (practiced; Andrade et al., 2020) was used in two studies. One study assessed a problem-based learning curriculum and used the terms “skills and practice” interchangeably. A skill refers to the ability to apply knowledge and use know-how to complete tasks and solve problems (Cedefop, 2024), and practice means the application of a skill when providing breastfeeding support. Thus, “practices” and “attitudes” were considered as to be part of the “knowledge and skills” outcome in our review, as it was not possible to isolate them.
A bespoke data extraction template addressing the review questions was developed and piloted. It included demographic population information, sample characteristics, study design interventions, outcomes measured, and timescales and key results. The findings served to populate the tables requested in the submission guidelines. The Template for Intervention Description and Replication (TIDieR) was used (Hoffmann et al., 2014) to extract specific information about each training. The TIDieR framework facilitates adequate reporting of health interventions which permits replication, evidence synthesis and wider evaluation. Data were extracted by one reviewer and checked by a second reviewer.
Data Analysis
Methodical steps were employed for data analysis. Using Covidence, data were extracted and tabulated to allow comparison of the baseline characteristics of the sample. The data extracted is summarised in Tables 2 and 3. Table 2 presents the setting, the study design, the aim of the study and sample size as well as type of HCPs. Table 3 summarises training type, outcomes measured and how these were measured. The methodological robustness of each study and the risk of bias were measured. The quality of studies was examined with validated tools. The Mixed Methods Appraisal Tool (MMAT; Hong et al., 2018) was used to appraise the quality of studies, as it allows for the evaluation of empirical studies (qualitative, RCT, non-RCT studies, quantitative descriptive and mixed-methods studies).
Characteristics of Included Studies.
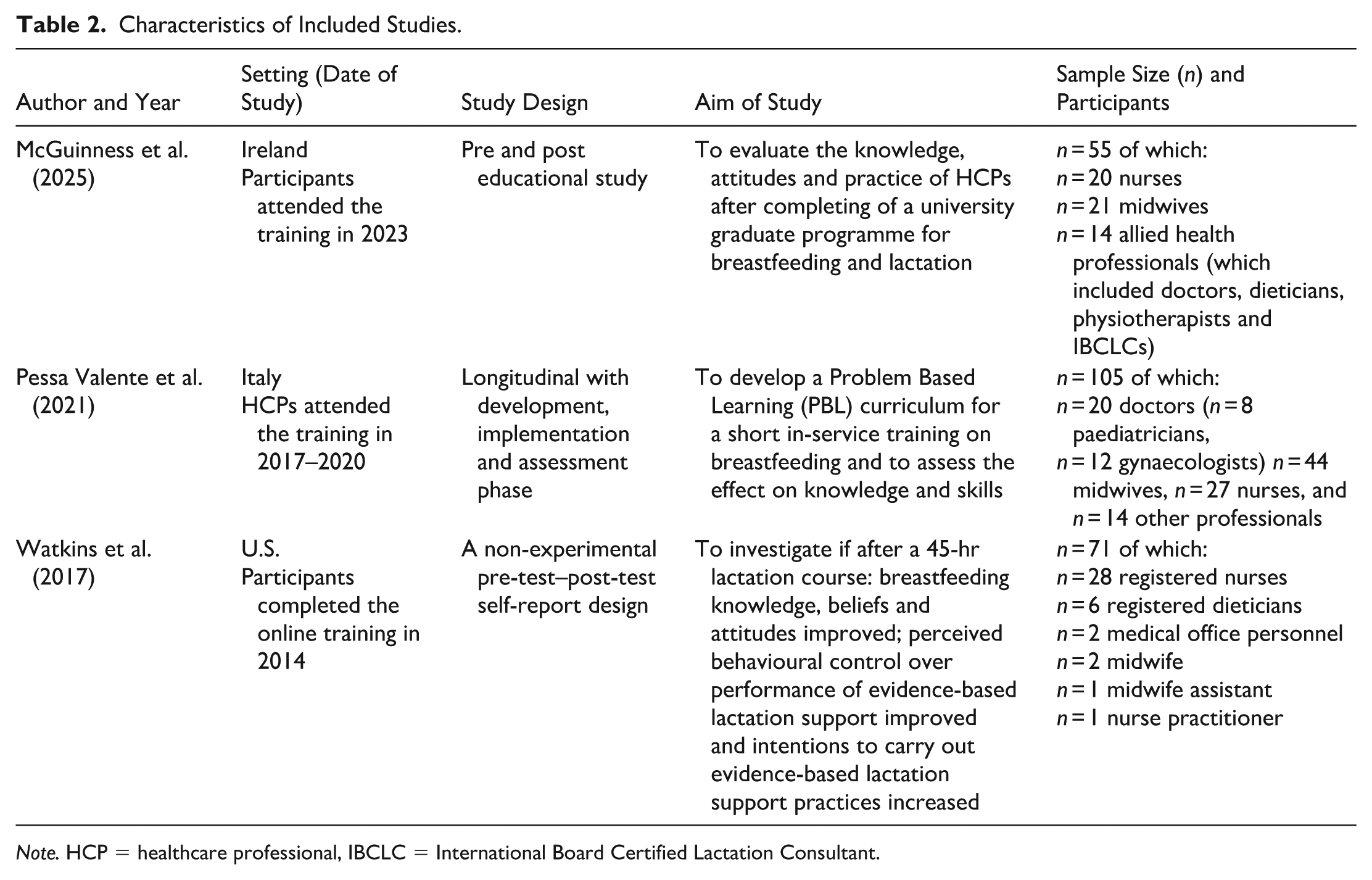
Note. HCP = healthcare professional, IBCLC = International Board Certified Lactation Consultant.
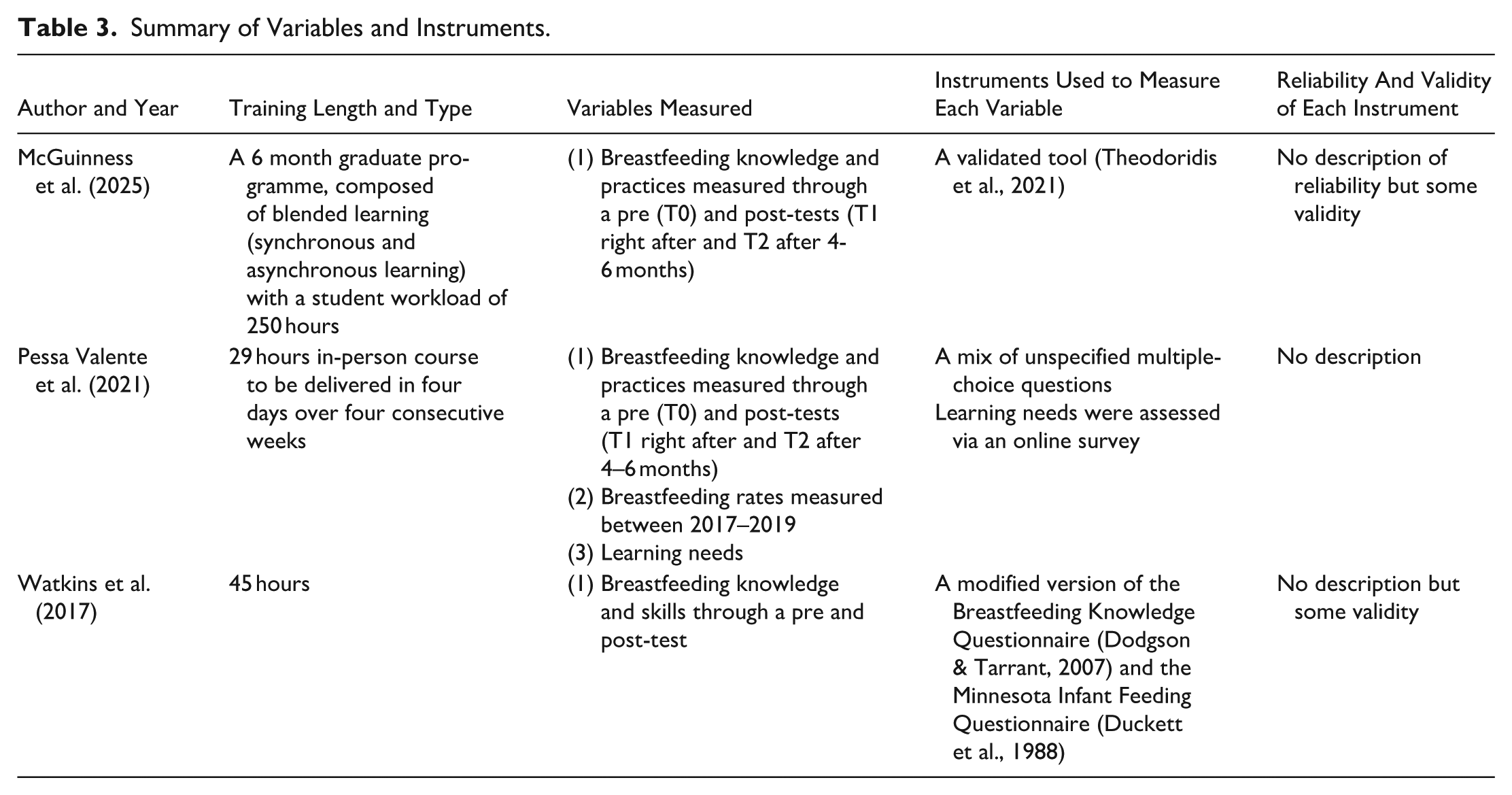
Summary of Variables and Instruments.
The JBI checklist for quasi-experimental studies (non-randomised experimental studies) was used to assess the risk of bias (Tufanaru et al., 2020). Quality appraisal of all studies was conducted by one reviewer and checked by a second reviewer. The results of quality appraisal were not used to exclude studies but to report on the overall quality of the evidence. The last phase involved contrasting and interpreting the results found across the studies. A narrative synthesis supported this as it helped facilitate the investigation of differences and similarities, evaluate the strength of evidence, and provide a summary of knowledge based on the review questions (Lisy & Porritt, 2016).
Results
Characteristics of Studies
Three studies were included (see Table 2), all were published between 2017 and 2025 and written in English. All were from high-income countries (World Bank, 2022), the United States (Watkins et al., 2017), Italy (Pessa Valente et al., 2021), and Ireland (McGuinness et al., 2025).
Participants, Setting, and Recruitment
The total number of participants was 231. McGuinness et al. (2025) and Watkins et al. (2017) presented some baseline population characteristics which included: age, sex, marital status, personal experience breastfeeding, having children and how many, and attendance to previous lactation trainings. The McGuinness and colleagues’ (2025) study had female students and the Watkins and colleagues’ (2017) study included one male out of 56. Only the Watkins and colleagues’ (2017) study reported on ethnicity (white, Latina/Hispanic or other) where 44% were white. The age range of students was 20–60 years old (McGuinness et al., 2025) and 22–68 years old for the Watkins and colleagues’ (2017). Watkins et al. (2017) reported that three quarters of students were parents (range = one to six children) and 44% had breastfed. The Pessa Valente and colleagues’ (2021) study only reported on the students’ professional background.
Sampling in the studies differed. Watkins et al. (2017) used convenience sampling and explained that HCPs attended the training for professional development reasons or as an employment requirement. Pessa Valente et al. (2021) did not give details of sampling. McGuinness et al. (2025) explained that all students were invited to participate in the study. Students had different professional backgrounds including midwives, nurses, nurse-midwives, doctors (paediatricians, gynaecologists, and GPs), allied healthcare professionals (dieticians and physiotherapists) and other unspecified professionals. In the study by Watkins et al. (2017) physicians were invited to attend the training, but none accepted the offer, and no explanation was given of why.
The Intervention
The variables measured and instruments to measure these are presented in Table 3. The length of each training and delivery modes varied. The training for the Pessa Valente et al. (2021) study was 29 hours, delivered in person. The Watkins et al. (2017) was 45 hours long and took place through an online platform. The McGuinness et al. (2025) study was 250 hours long and used a blended learning approach.
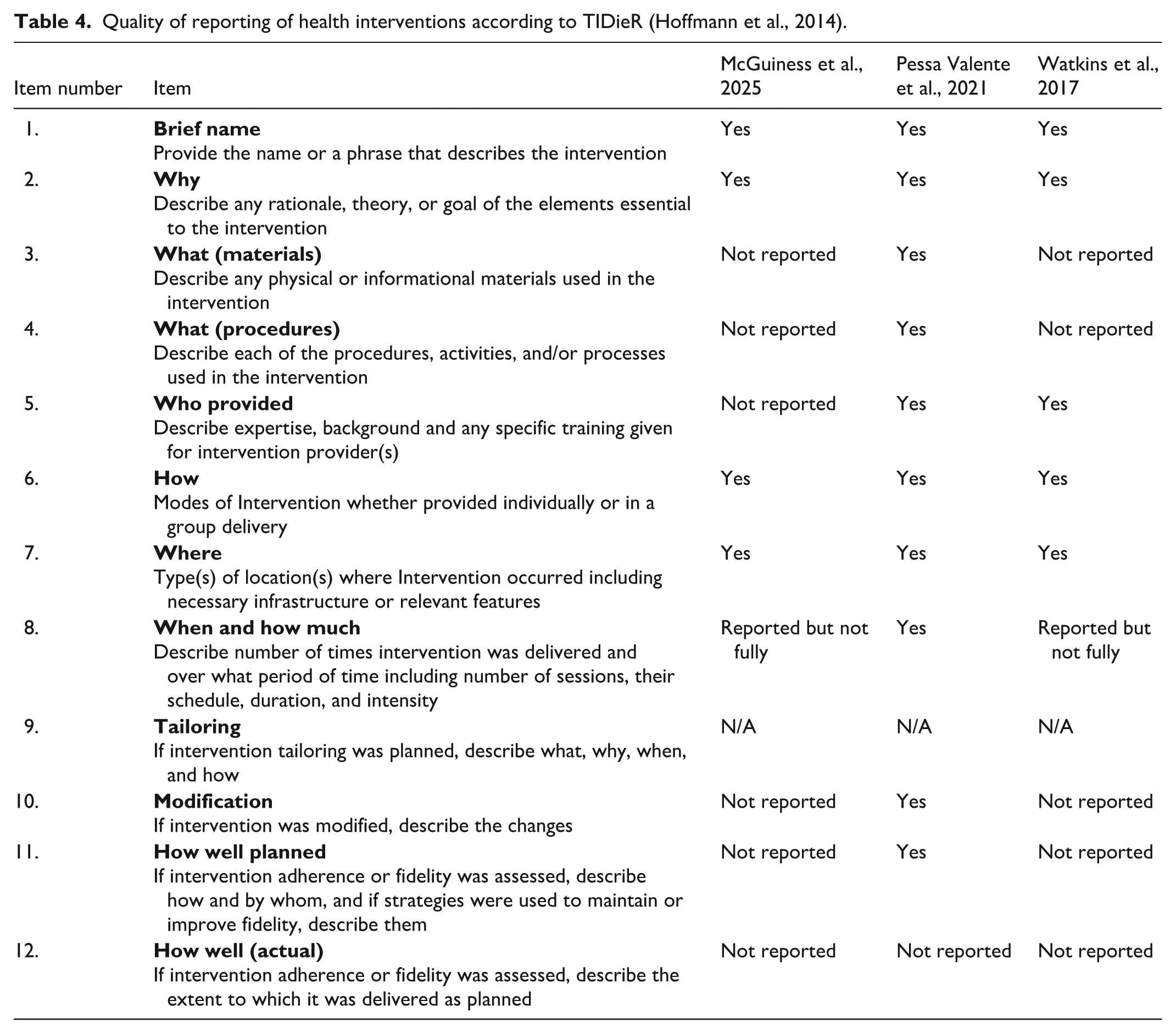
The TIDieR framework evaluated in-depth the quality of reporting (see Table 4). Overall, there was either a lack of data or insufficient reporting from most studies, which is necessary for a comprehensive exploration. Despite being the shortest training, the Pessa Valente and colleagues’ (2021) study gave detailed information on the materials used as well as the learning activities and was the only study that specified the use of a pilot course to test the curriculum, timetable, manuals, and learning materials. Watkins et al. (2017) described in detail their syllabus. The McGuinness et al. (2025) only stated the main themes (see online Supplementary File 2). These two studies (McGuinness et al., 2025; Watkins et al., 2017) did not report whether the intervention was modified or adhered to once it was delivered. None of the studies described if and how the trainings were evaluated by the team delivering them and if improvements were identified for future cohorts.
Quality of reporting of health interventions according to TIDieR (Hoffmann et al., 2014).
Knowledge and Skills
To measure the “knowledge and skills” (or practice) outcomes different tests were used for each study. The study by Watkins et al. (2017) used a modified version of the Breastfeeding Knowledge Questionnaire (Dodgson & Tarrant, 2007) and the Minnesota Infant Feeding Questionnaire (Duckett et al., 1988) for its test. The study by Pessa Valente et al. (2021) used a mix of unspecified multiple-choice questions. The McGuinness and colleagues’ (2025) study tested lactation knowledge with a set of statements from a validated tool reported in a preprint (Theodoridis et al., 2021). This tool was developed in Greece, it was administered mainly to midwives, nursing and medical students (Theodoridis et al., 2021). Several of the statements used in this tool to test knowledge and practice seem more suited to test basic (Level I) training in the McGuinness and colleagues’ (2025) study. For example: “formula milk is easier to digest than maternal milk,” “a mother with mastitis should stop breastfeeding,” “breastfeeding mothers need to night wean at 6 months.” In addition, having “yes” and “no” answers can allow for guessing. The McGuinness and colleagues’ (2025) study also mixed knowledge questions with self-reported confidence. Although knowledge and confidence are both important components of learning, testing confidence can be subjective and does not always translate into improved knowledge.
The first post-test showed a statistically significant improvement in knowledge for all studies. For the Pessa Valente and colleagues’ (2021) study at the pre-test the median was Mdn = 17.00 and at the first post-test the Mdn = 19.00, for the Watkins and colleagues’ (2017) study the pre-test mean was 11.32 (SD = 2.55) and post-test the mean was 12.45 (SD = 1.44). The McGuinness and colleagues’ (2025) study had no aggregate results of the pre- post-tests. Instead, it presented the results for each of the statements. Given the heterogeneity in the way the knowledge outcome was measured comparison among results was not possible.
Breastfeeding Rates
The study by Pessa Valente et al. (2021) was the only one that examined breastfeeding rates. This study measured exclusive breastfeeding rates at discharge from maternity ward over 3 years reporting rates of: 75% in 2017, 81% in 2018, and 81% in 2019 (Pessa Valente et al., 2021). It also reported breastfeeding rates at four/five months old of 31% in 2017, 33% in 2018, and 37% in 2019 (Pessa Valente et al., 2021). However, the trainings took place from 2017 to 2020, which does not align exactly to the dates breastfeeding rates were reported. The definition of “exclusive breastfeeding” was not provided by the authors. An accurate definition is crucial for a better understanding of lactation research (E. Chetwynd, 2024; Noel-Weiss et al., 2012). The authors did not report any contextual factors in the setting that may have influenced the rates other than the training implementation. McGuinness et al. (2025) implied that by increasing HCPs’ knowledge, attitudes and practices breastfeeding rates would be improved, but did not measure this.
Learning Needs
Pessa Valente et al. (2021) asked participants about their training needs prior to developing the curriculum. Through an online survey, training needs were identified and included: (1) effective communication strategies (49%); (2) effective support practices (41%); and (3) maternal and neonatal reflexes (31%; Pessa Valente et al., 2021). The study by Watkins et al. (2017) mentioned that their course was responding to previously identified learning needs without specifying what these were. McGuinness et al. (2025) did not gather information pre training regarding training needs.
Quality Appraisal
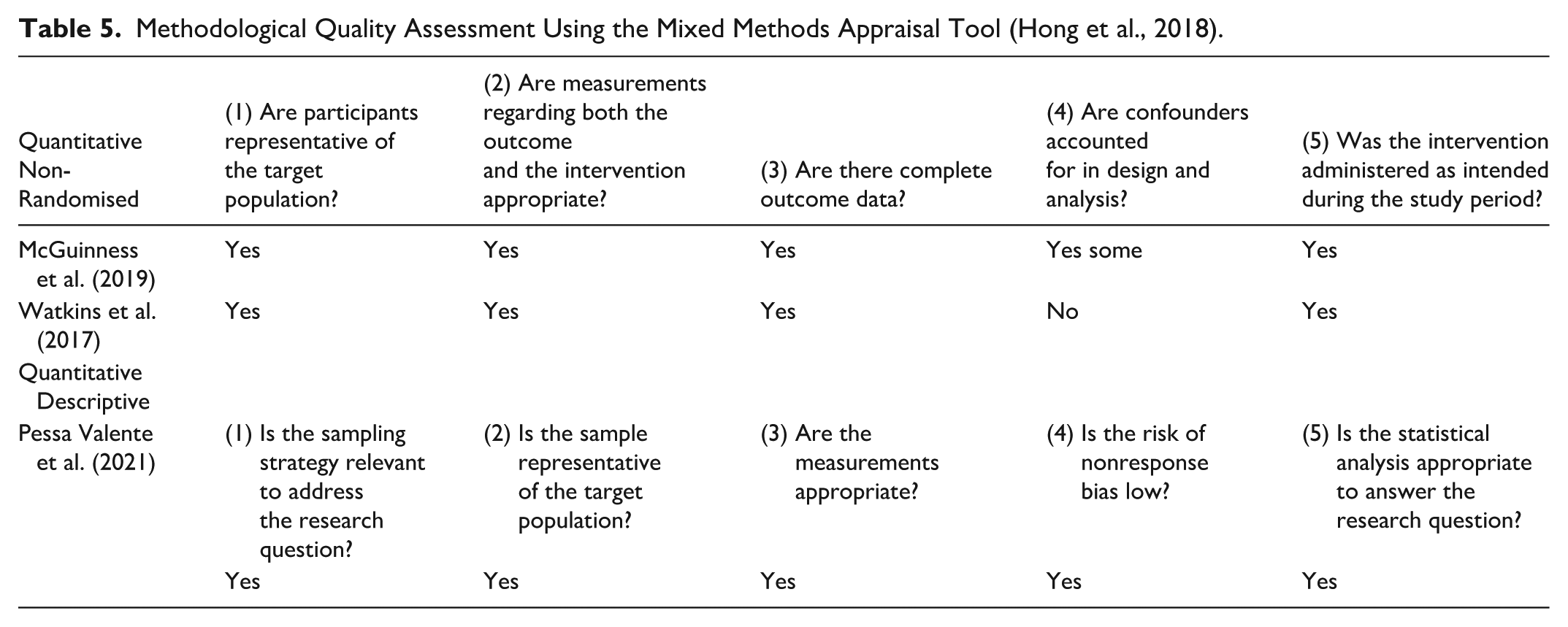
The quality of the study methodology is essential to permit conclusions to be drawn from the outcomes (Hong et al., 2018). The results from the MMAT are in a summary in Table 5. The study by Pessa Valente et al. (2021) used an adequate sampling strategy; the sample was representative of the target population; the measurements and statistical analysis were appropriate. For these two studies (McGuinness et al., 2025; Watkins et al., 2017) either confounders were not accounted in the design and analysis or they were not complete.
Methodological Quality Assessment Using the Mixed Methods Appraisal Tool (Hong et al., 2018).
The JBI critical appraisal checklist showed how the risk of bias differed across the different domains (see Figure 2). There was no ambiguity in terms of the temporal relationship, between “cause” and “effect.” There is a risk of selection bias when randomisation is not used. Random selection could have made the studies more robust, but the samples seem representative. The validity of the causal inferences was weak for most studies. No study used a control group. Only the Pessa Valente and colleagues’ (2021) study had two post-tests’ measurements and this is important to measure knowledge retention. Not all participants in the three studies (McGuinness et al., 2025; Pessa Valente et al., 2021; Watkins et al., 2017) completed the post-test, which represents a threat to the internal validity and potentially attrition and analysis bias (Cherry et al., 2024). Given how knowledge and skills were tested the outcome measurements could be unreliable. Only the Pessa Valente and colleagues’ (2021) study declared funding from the Regional Health Authority of Friuli Venezia Giulia. Thus, it is not possible to ascertain if there could be funding bias for the other two studies. The overall risk of bias for all studies was high.
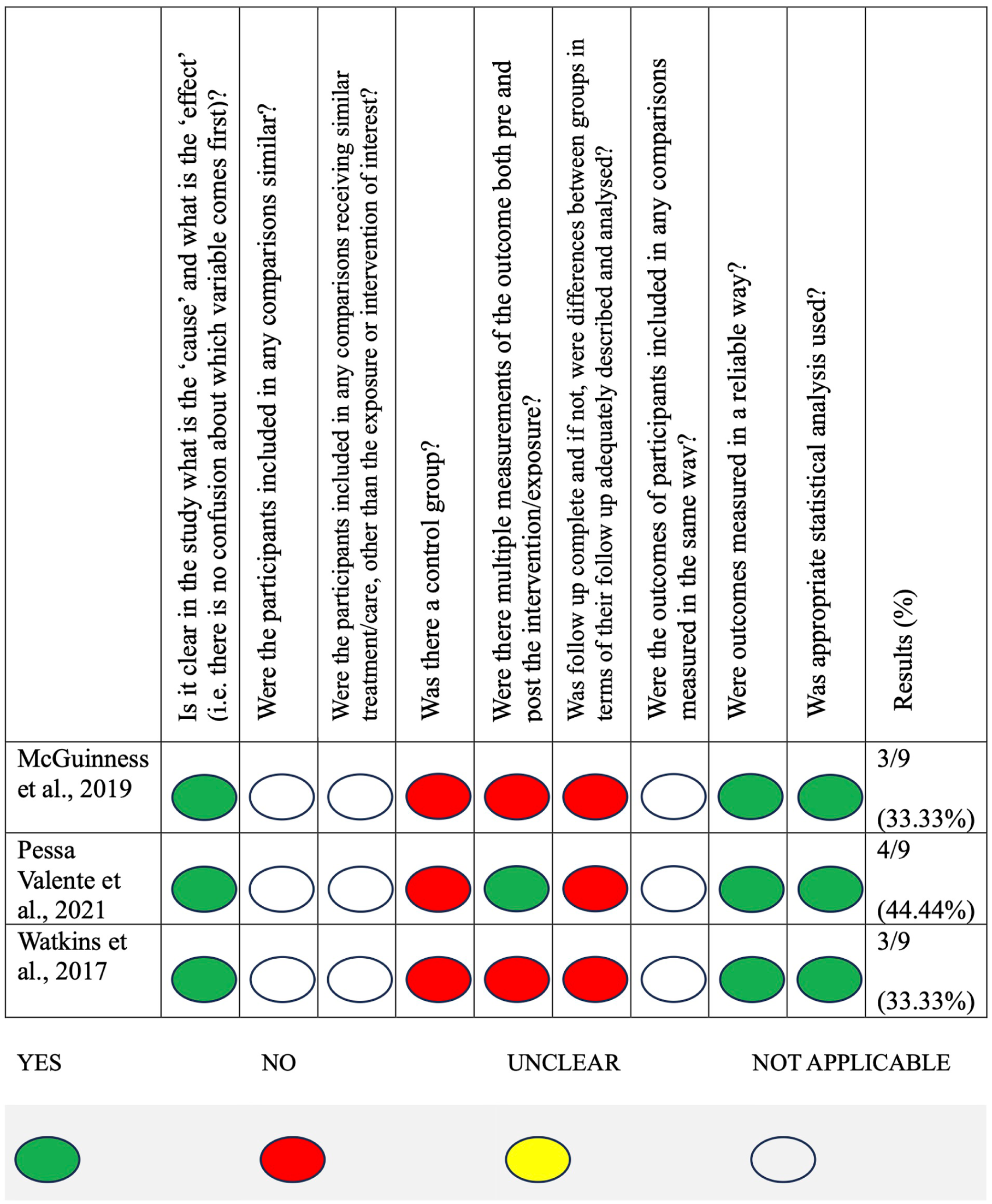
Summary risk of bias.
Discussion
The fact that this systematic review only found three studies to include shows that more research is urgently needed in regard to in-depth breastfeeding training. Given the small number of studies and the limitations, these results must be interpreted with caution. No randomised controlled trials (RCTs) were included in this review, and these could provide stronger evidence. Balogun and colleagues’ (2017) Cochrane review proposed randomisation for a UNICEF BFHI training between staff taking and not taking training, and this could be done similarly for in-depth breastfeeding trainings.
Overall, in-depth training was found to increase course participants’ knowledge as well as their skills. Studies in our review focused mainly on knowledge acquisition. No studies evaluated the impact that HCPs who attend in-depth training might have on hospital practices. Murphy et al. (2019) argued that the aim of HCP’s training is to increase knowledge, improve self-efficacy, and apply knowledge into practice. Watkins et al. (2017) warned that all layers of the organisation need to be involved so that education is not a bandaid to promote evidence-based practice. For HCPs to apply this new knowledge into practice, institutional changes are needed including changes in the philosophy of the wards. Spiby and colleagues’ (2009) systematic review demonstrated that this change must take place. Hannula and colleagues’ (2008) systematic review showed that HCPs need to be supported by their organisations to be able to practice and cement knowledge assimilation and long-term retention.
Breastfeeding rates were only measured in one study. The influence of training on breastfeeding rates is difficult to isolate from other factors. Training as a stand-alone intervention is not the only reason for improvement in breastfeeding rates (Gavine et al., 2017). Other factors such as: BFHI 10 steps implementation (Fallon et al., 2019), personal breastfeeding experience (Brodribb et al., 2008), and sociodemographic factors, may have contributed. A systematic review (Mulcahy et al., 2022) showed that it is essential to measure at different timepoints, as this can reflect measurable outcomes in terms of breastfeeding rates. The paucity of data in our review implies that it was not possible to assess the impact of in-depth training on breastfeeding rates.
No qualitative studies were included, showing a knowledge gap around women’s perception of support received by those HCPs who undertake in-depth training, as well as HCPs’ experiences of and motivations to attend in-depth trainings. To study the levels of satisfaction in families who received lactation care from HCPs with in-depth training (for example IBCLCs or Breastfeeding Medicine specialists) would be important for all families but also for clinically complex cases. Clinically complex breastfeeding dyads sometimes have been seen by many HCPs who have not been able to resolve their issues. A study by Glassman et al. (2022) collected qualitative data of mothers’ perception of support by a paediatrician/IBCLC in a medical home and reported high levels of satisfaction. In addition, the importance of training participants being able to discuss their own positive or negative breastfeeding experiences (personal and professional) was not raised in the studies. However, other research suggests that this can have a significant impact on parental satisfaction. When HCPs participate in breastfeeding training where there is an allocated space to debrief and reflect about their own breastfeeding experiences, their attitudes can be improved and parental satisfaction increases (Ekstrom et al., 2012, Ekstrom & Thorstensson, 2015).
In this review, only the Pessa Valente and colleagues’ (2021) study reported that, through the pre-education phase, HCPs were encouraged to co-create and define their learning needs. There is an intimate interplay between learning needs and motivation to learn (Filgona et al., 2020). People are motivated to attend training because of certain learning needs, or on some occasions the employer might have identified learning deficits. Little is known on what HCPs want or need to learn when they join in-depth breastfeeding training.
This review did not find any studies which addressed the outcome related to HCPs motivation to attend in-depth training. There has been little research on motivational factors, or their relevance to breastfeeding training (Pérez-Escamilla et al., 2016). Having the motivation to join in-depth training is a behaviour influenced by a multitude of intrinsic and extrinsic factors (Ryan & Deci, 2000). Intrinsic motivation examples include: interest/passion (in the topic), mastery (seeking professional improvement), lactation qualification (becoming an IBCLC) or challenge (facing complex breastfeeding cases). Extrinsic factors include: work requirement, material rewards, professional recognition, career progression, or social respect. Self-determination theorists explain that rather than being one or the other, motivation exists along a continuum (Barta, 2024). Within breastfeeding education research, neither intrinsic nor extrinsic motivational factors have been studied for in-depth training.
No study explored the relationship between the demographic characteristics and the outcomes. Unreported or not evaluated characteristics can act as potential confounders. Only McGuinness and colleagues’ (2025) study specified having two groups (IBCLCs and non-IBCLC students) which were compared. IBCLCs can choose to attend in-depth training when they need to recertify. Having attended lactation trainings and being an IBCLC can be an advantage in terms of knowledge and practice. Cantrill et al. (2003) showed in their Australian study that midwives’ knowledge was significantly correlated to three predictors: holding a lactation qualification, having breastfed for more than 3 months, and having substantial clinical experience.
In the three included studies, in-depth lactation training was multidisciplinary. This has advantages to single or bi-profession training as it can ensure that all HCPs “speak” the same language, promoting true continuity of care (Bernstein et al., 2022) and breaking down disciplinary barriers (Morrison & Chamberlain, 2024). Mulcahy and colleagues’ (2022) systematic review recommended an interdisciplinary approach to be used when delivering breastfeeding skills-based training. A systematic review found that when BFHI Step 10, which emphasises “coordination among HCPs at discharge” was implemented it helped mothers maintain breastfeeding (Pérez-Escamilla et al., 2016). In addition, if HCPs have the same knowledge base and follow BFHI Step 10, this can have a greater impact on health outcomes.
This review has highlighted poor reporting and reporting is essential to assess pedagogical robustness. The information reported regarding many trainings can be scant, vague, or merely descriptive (Navarro et al., 2021). The length, the curriculum content, the delivery mode, the professional background of the teaching faculty, and whether there is a clinical component, are some examples. Not all studies in this review specified the trainer’s professional background or teaching experience. Spiby and colleagues’ (2009) systematic review urged investigation of the differences in outcomes based on the delivery of training by trainers with different backgrounds. Pérez-Escamilla (2025) stressed that IBCLCs play a key role in building and creating human resources in lactation as they provide breastfeeding education at all levels. Balogun and colleagues’ (2017) systematic review underlined the difficulty in adopting a universal breastfeeding curriculum due to the huge variation in training materials, and this certainly applies to in-depth trainings too. Boss and colleagues’ (2021) systematic review suggested publishing an online manual which would describe in more detail the intervention development process, which could permit replicability.
This review found only one study which examined an in-depth training that could be considered given its length as a stepping stone for the IBCLC credential (McGuinness et al., 2025). However, the number of in-depth IBCLC training courses has most likely grown around the world for these two reasons. First, there is a clear need to fill the gap in knowledge for those who specialise in breastfeeding. Second, the number of IBCLCs around the world keeps increasing; currently 38,154 in 134 countries (IBLCE, 2025). Yet, there is no international directory of these in-depth trainings. IBCLE’s Preferred Provider is a directory which advertises continuous education (CERPS) programmes. In the United States, the Lactation Education Accreditation and Approval Review Committee (LEAARC) has a directory of its accredited programmes (LEAARC, 2020).
Future research should focus on finding out why HCPs are attending in-depth trainings (including IBCLCs trainings) around the world, who they are, if minority groups are accessing them and to what extent, and who funds the training (employers or individuals). Given IBCLCs’ key role in maternal and infant health, investigating the impact of IBCLC trainings sets a research priority. Pérez-Escamilla (2025) stressed that IBCLCs need to be included in all healthcare systems (Pérez-Escamilla, 2025). E. M. Chetwynd and colleagues’ (2019) systematic review showed that face-to-face support by an IBCLC increased rates of breastfeeding at 6 months. Pascual and colleagues’ (2025) systematic review and meta-analysis found that IBCLC support offered during hospitalisation and continued through the post period could improve breastfeeding outcomes. In Italy, having one IBCLC in a medical centre increased initiation rates by 10% and maternal satisfaction by 33% (Chiurco et al., 2015).
Further studies could reveal which professions seek IBCLC training, for what reasons and what motivates those who already hold a degree and sometimes have many years of experience in maternity care to pursue the IBCLC qualification. The IBCLC qualification has not yet been recognised as a stand-alone credential and IBCLCs are not considered allied HCPs around the world. Studying the impact of IBCLCs in-depth trainings could lead to more effective use of resources by providing an evidence-based curriculum for in-depth training for HCPs. In the long run it could facilitate the integration and recognition of IBCLCs as allied HCPs.
Limitations
This review has several limitations. Given the novel scope of the research topic, the number of studies included in the review was limited. Meta-analysis could not be achieved as there was insufficient or dissimilar data. None of the qualitative questions were answered due to a lack of studies. HCPs need different breastfeeding training (including content, length, and depth) based on their scope of practice and professional responsibility. Another limitation is that there are no universally accepted criteria for in-depth training and therefore we used an “arbitrary” length of more than 20 hours as a cut-off. Data extraction was not performed in duplicate, but it was checked by a second reviewer (due to limited resources). There was language bias as full articles which were not available in English, Spanish, or French, were not considered so we may have missed publication in other languages.
Conclusion
As far as we were aware, this was the first systematic review to assess in-depth breastfeeding training globally. Only three quantitative studies were found. All three studies looked at breastfeeding knowledge as an outcome. Based on the findings of this review, we cannot make recommendations other than to highlight the urgent need for further research. International consensus is needed on different levels of lactation training required by HCPs depending on how much contact they have with breastfeeding dyads. Future research should address the methodological and conceptual limitations of the studies found. Future studies should also measure a wider range of outcomes and use validated tools to test knowledge. Given that lactation support is a crucial public health target, the gap in knowledge is a priority for future research of in-depth trainings, including those leading to the IBCLC qualification.
Supplemental Material
sj-docx-1-jhl-10.1177_08903344261446138 – Supplemental material for In-Depth Breastfeeding Training for Healthcare Professionals: A Systematic Review
Supplemental material, sj-docx-1-jhl-10.1177_08903344261446138 for In-Depth Breastfeeding Training for Healthcare Professionals: A Systematic Review by Indira López-Bassols, Joan Cameron, Camila Biazus-Dalcin and Alison McFadden in Journal of Human Lactation
Footnotes
Acknowledgements
The main author would like to acknowledge the support of Scott McGregor, librarian at the University of Dundee.
Author Contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The lead author is currently undertaking a PhD at the University of Dundee. This systematic review is part of her doctoral studies, which are partly funded by the Central London Community Healthcare NHS trust and the Centre for Breastfeeding Education and Research.
Declaration of Conflicting Interests
The authors disclose the following with respect to the research, authorship, and/or publication of this article: Indira Lopez-Bassols is currently undertaking doctoral research under the supervision of Professor Alison McFadden, Dr. Joan Cameron, and Dr. Camila Biazus-Dalcin. Indira Lopez-Bassols is the Director of the Centre for Breastfeeding Education and Research which hosts the Art and Science of Breastfeeding course, a training which leads to the IBCLC qualification.
Supplemental Material
Supplementary Material may be found in the “Supplemental material” tab in the online version of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.