
Abstract
Background:
To ensure the initiation and maintenance of breastfeeding, health systems need qualified professionals who can advise and support women. There was previously no validated tool to assess midwifery students’ confidence in providing breastfeeding support in Türkiye.
Aim:
To adapt the Australian self-efficacy scale for breastfeeding support for midwifery students into Turkish and to psychometrically test its validity among Turkish midwifery students.
Methods:
A scale adaptation approach was used to translate and validate the 34-item scale. The tool was then sent to third- and fourth-year Turkish midwifery students. Psychometric properties were examined using both classical test theory and the Rasch measurement analysis.
Results:
A total of 382 participants completed the survey. The Turkish version demonstrated excellent internal consistency, strong item functioning, and a largely unidimensional structure, confirming its robustness in the Turkish educational context. The findings indicate that Turkish midwifery students generally reported high self-efficacy for foundational breastfeeding support tasks, while more complex, practice-based skills, such as managing infant behavior during breastfeeding, required higher levels of confidence.
Conclusion:
This study provides strong evidence for the validity and reliability of the Turkish version of the Self-Efficacy Scale for Breastfeeding Support. Consistent with prior development and validation works, the scale demonstrated strong psychometric properties. These findings extend the scale’s applicability to a new cultural and educational context. Overall, this Turkish version is a psychometrically sound tool for self-assessing breastfeeding self-efficacy and may be used to inform curriculum evaluation, guide targeted educational interventions and enable cross-cultural comparison.
Key Messages
It is the responsibility of health professionals to provide accurate information and guidance on breastfeeding. Strengthening midwives’ support and counseling skills is essential for maternal and infant well-being and public health.
Midwifery education plays a key role in breastfeeding support. Despite strong evidence of the benefits of breastfeeding and increasing emphasis on evidence-based practice, research shows that many midwives lack sufficient knowledge and skills to effectively support infant feeding.
This paper presents a validated Turkish version of a tool to measure midwifery students’ breastfeeding support self-efficacy. It helps to identify areas of insecurity and supports targeted improvements in education programs.
Background
Breast milk is a nutritional source that meets all the newborn’s needs, supporting healthy growth and development (Lyons et al., 2020). The World Health Organization (WHO) and the American Academy of Pediatrics recommend exclusive breastfeeding for at least 6 months, with breast milk as the sole source of nutrition (Meek & Noble, 2022; WHO, 2020). Beyond its maternal and child health benefits, breastfeeding is an important component of sustainable development and well-being globally.
In 1989, WHO and the United Nations International Children’s Emergency Fund (UNICEF) published the “10 Steps to Successful Breastfeeding” principles to protect, promote, and support breastfeeding in facilities providing maternity and newborn services (UNICEF, 2018). In 1991, the WHO and UNICEF launched the Baby Friendly Hospital Initiative (BFHI), revising the 10 steps and providing implementation guidance for healthcare systems (WHO, 2026).
To ensure the initiation and maintenance of breastfeeding, health systems need qualified professionals who can support, advise, and inform women about breastfeeding (UNICEF, 2018). Step Two of the BFHI recommends “that staff have sufficient knowledge, competence, and skills to support breastfeeding” (WHO, 2026). Institutional support for breastfeeding and support from trained health professionals are important factors in breastfeeding success (Meek & Noble, 2022). However, the extent to which breastfeeding education and training are implemented, and their effectiveness, are largely unknown (Brodribb et al., 2007; Freed et al., 1996; Gavine et al., 2017; Mulcahy et al., 2022).
In 2019, UNICEF released the United Kingdom Baby-Friendly Initiative university standards to enhance university education (UNICEF, 2019). The Baby Friendly University program works to ensure that future generations of health professionals are enabled to incorporate Baby Friendly standards into their practice from the very start of their careers. However, these standards have not been adopted globally. Despite the growing awareness of the benefits of breastfeeding and the need for evidence-based breastfeeding practices, research has found that health professionals continue to lack the knowledge and skills needed to effectively support breastfeeding (Dodgson et al., 2014; Duarte et al., 2022; Gary et al., 2017; Yang et al., 2018).
In Türkiye, the “Program for the Promotion of Breastfeeding and Baby-Friendly Health Facilities” has been actively implemented by the Ministry of Health since 1991 to protect, promote, and support breastfeeding (Ministry of Health of the Republic of Türkiye, 2023). Breastfeeding support is actively provided in primary care facilities and secondary and tertiary care units. According to the 2018 Türkiye Population Health Survey, the exclusive breastfeeding rate for the first 6 months is 41% (Hacettepe University Institute of Population Studies, 2019). While 66% of babies continue to be breastfed at 1 year of age, only 34% are breastfed up to the age of 2. Breastfeeding rates in Türkiye remain below the desired level (Hacettepe University Institute of Population Studies, 2019). Therefore, promoting and supporting breastfeeding remains an important issue in Türkiye.
Midwives and nurses, as the primary providers of maternal and child health services, play a vital role in assisting mothers to initiate and sustain breastfeeding. Studies have reported that undergraduate midwifery and nursing students are not adequately prepared to support mothers in breastfeeding (Altwalbeh, 2021; Freed et al., 1996; Vandewark, 2014; Yang et al., 2019). In addition to knowledge of breastfeeding physiology, health professionals are best positioned when they have a positive attitude toward breastfeeding, the knowledge and skills to overcome breastfeeding challenges, and effective counseling skills to provide adequate support to breastfeeding women (McFadden et al., 2017; Mclntyre & Fraser, 2018; WHO, 2018). Studies emphasize that positive health professional attitudes towards breastfeeding are effective in maintaining mothers’ self-efficacy and breastfeeding behavior (Vandewark, 2014; Yang et al., 2019). However, when breastfeeding is not valued and formula is promoted, early weaning is likely (Duarte et al., 2022; Pérez-Escamilla, 2020). This reinforces the vital need for undergraduate health professionals to receive consistent and effective education in breastfeeding to develop their knowledge, skills, and attitudes to support breastfeeding (Mulcahy et al., 2022).
Midwifery students should develop the belief that they can support breastfeeding mothers through their education before graduation. Research assessing how midwifery students learn to provide breastfeeding support, the impact of learning processes, and students’ perceptions of these processes is limited (Mulcahy et al., 2022). Valid tools to assess the level of health science students’ breastfeeding knowledge and skills are also limited (Yang et al., 2018).
Since 1997, midwifery education in Türkiye has been offered through 4-year, full-time, direct-entry undergraduate programs. Students are admitted after high school based on their performance in a national entrance examination. The midwifery curriculum is implemented uniformly across universities nationwide, encompassing a total of 61 midwifery departments. Oversight and coordination of the program are provided by the Council of Higher Education (YÖK), and the curriculum is structured in accordance with the guidelines of international organizations such as the WHO and the International Confederation of Midwives, as well as the European Union Directive 80/155/EEC (İsbir et al., 2023). In Türkiye, undergraduate midwifery students receive education on breastfeeding and breast milk during their studies within the scope of the National Core Curriculum in Midwifery EBE-UCEP (Council of Higher Education [EBE-UÇEP], 2025). In all midwifery schools, breastfeeding support and counseling are taught as part of compulsory courses. In addition, most schools offer an optional 2 hours of theoretical education, or two credits of theory and two credits of practical training, and students are exposed to breastfeeding support during clinical placement.
Self-efficacy refers to an individual’s confidence in their ability to achieve goals by learning and performing specific tasks (Melchionda et al., 2019). This concept, developed by Bandura, is based on an individual’s expectations regarding their capacity to learn and successfully perform a behavior (Bandura, 1986). Breastfeeding self-efficacy is defined as a mother’s confidence in her own ability to breastfeed her baby, and it influences her thoughts and behaviors regarding the process of initiating and maintaining breastfeeding (Dennis, 1999).
Breastfeeding support self-efficacy, distinct from a mother’s self-efficacy regarding her own breastfeeding experience, refers to a person’s perceived ability to provide support to others. In this context, breastfeeding support self-efficacy can be defined as an individual’s belief in their ability to provide effective support, counseling, and guidance to mothers regarding breastfeeding. For midwifery students and future healthcare professionals, this concept encompasses their perceived competence in providing evidence-based information, offering guidance on breastfeeding techniques, and managing potential challenges that may arise during breastfeeding. Despite the inclusion of breastfeeding content in midwifery curricula, there is limited evidence on how effectively these educational experiences translate into students’ confidence in providing breastfeeding support.
In Türkiye, the absence of a validated instrument to assess breastfeeding-related self-efficacy among midwifery students limits the ability to evaluate educational outcomes and identify areas requiring targeted improvement. To address this gap, the Self-Efficacy Scale for Breastfeeding Support developed by Blackman et al. (2015) was identified as an appropriate instrument for adaptation. Blackman and colleagues’ (2015) tool is based on breastfeeding self-efficacy theory and enables midwifery students to self-assess their self-efficacy in fulfilling their midwifery role in breastfeeding support. It was originally developed in Australia in English, and has since been translated and validated for use in the Italian educational context (Melchionda et al., 2019). This scale enables midwifery students to identify areas where they feel inadequate in providing breastfeeding support, thereby facilitating the development of a curriculum focused on these areas and the implementation of personal learning plans tailored to the students’ needs. Additionally, assessing students’ breastfeeding self-efficacy before and after breastfeeding education sessions can be used to measure the effectiveness of the education. The absence of a measurement tool in Türkiye to assess breastfeeding support self-efficacy is a significant gap. In this context, the aim of the study was to adapt the Australian Self-Efficacy Scale for Breastfeeding Support for Midwifery Students into Turkish and to psychometrically validate it with Turkish midwifery students.
Methods
Study Design
This study was a scale adaptation study to translate and psychometrically validate the Australian Self-efficacy Scale for Breastfeeding Support for Midwifery Students (Blackman et al., 2015) for use in Türkiye. The process is outlined in Figure 1.
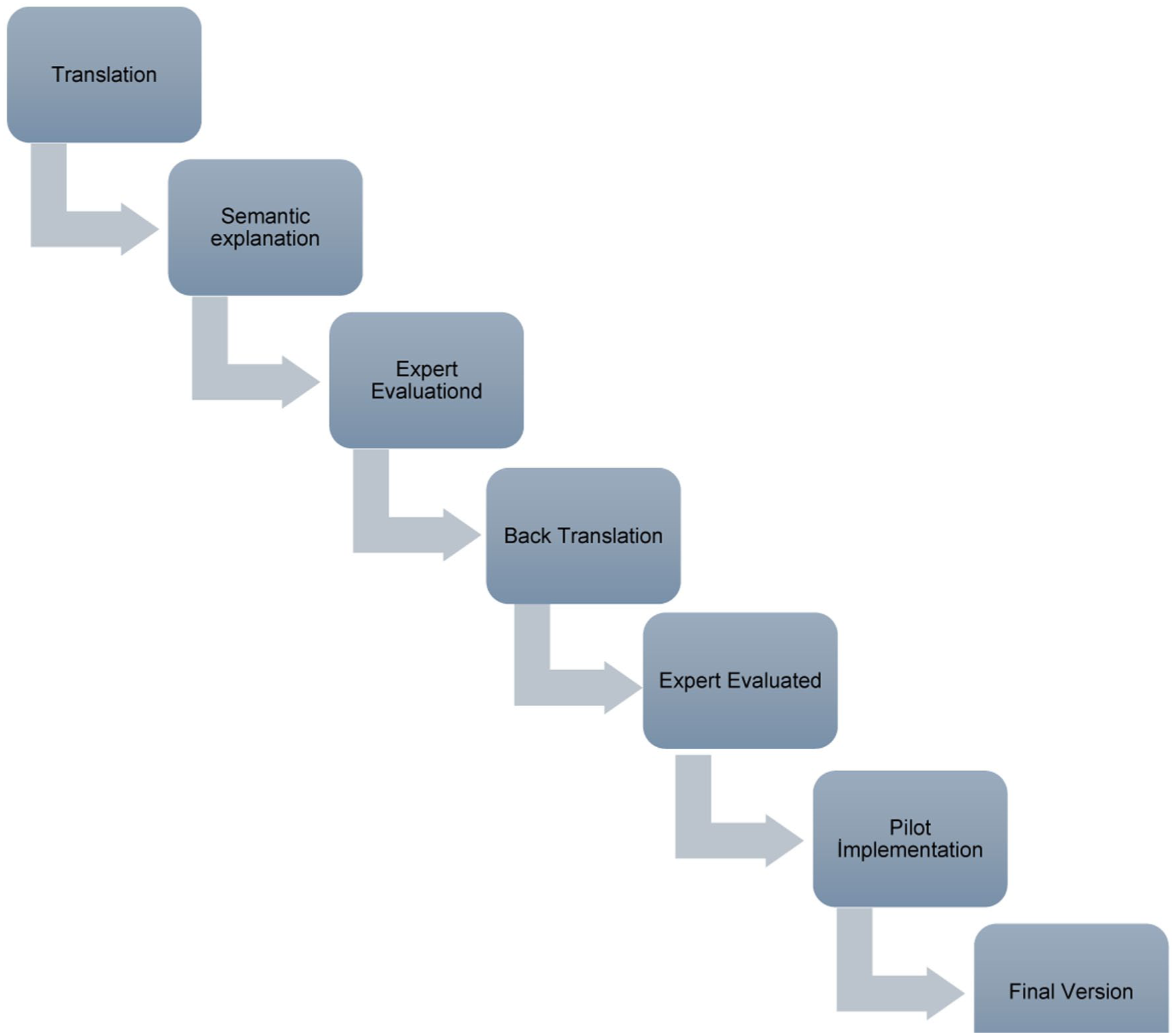
Steps followed in the adaptation process.
Translation and Cultural Adaptation
The adaptation process followed the International Testing Commission (ITC, 2019) guidelines, and used the WHO’s instrument translation protocol (Sousa & Rojjanasrirat, 2011). The original English questionnaire was translated into Turkish by two bilingual PhD-prepared academics specializing in midwifery and women’s health (FAO and EC). Translations were reviewed for semantic, idiomatic, conceptual, linguistic, and contextual (HO). An expert panel then evaluated the draft Turkish version. The expert panel consisted of academics and clinicians working in the field of breastfeeding, including: one professor of midwifery, one professor of child health and disease nursing, one professor of women’s health nursing, three associate professors of midwifery, five assistant professors of midwifery, and four specialist midwives. Although some sources recommend expert opinion after back-translation (Jesus & Valente, 2016), the Sousa and Rojjanasrirat (2011) recommends expert opinion after initial translation. The experts evaluated each item as “not appropriate (1)”; “the item needs to be brought into an appropriate form (2)”; “appropriate, but minor changes are needed (3)”; or “very appropriate (4).” A Content Validity Index (CVI) was calculated as the percentage agreement among the experts’ opinions. Items with at least 80% of experts assigning a rating of 3 or 4 were considered acceptable (Terry & Nguyen, 2025), and the lowest CVI score across all the items was 0.86, indicating good content validity. Revisions were made based on expert consensus to ensure linguistic clarity and cultural appropriateness.
The revised Turkish version of the scale was then back-translated into English by an academic fluent in both languages (HO). The back-translated version was reviewed by one of the researchers who developed the original scale (LS) to evaluate consistency of meaning with the original version. Based on this evaluation, necessary revisions were made, translated back to Turkish, and the final version was then piloted with a small group of six students.
In line with COSMIN recommendations, students were asked to review all items in their final form and provide feedback on clarity, comprehensibility, and relevance (COSMIN, n.d.; Prinsen et al., 2018). No difficulties or misunderstandings were reported, and therefore no further revisions were deemed necessary. Pilot data were not included in the final analysis.
The final Turkish version retained all 34 items of the original instrument, scored on a 4-point Likert scale: 4 = “It is very easy for me to do this”; 3 = “It is easy for me to do this”; 2 = “It is difficult for me to do this”; 1 = “It is very difficult for me to do this”. Higher scores indicate greater self-efficacy in providing that aspect of breastfeeding support. See Supplementary file 1 in the online supplemental materials for both the Turkish and the English back-translated versions of the items.
Sample, Data Collection, and Management
Midwifery students were recruited from universities across Türkiye through social media platforms (i.e., Facebook, WhatsApp, Instagram). Eligible participants were third- or fourth-year midwifery students who ideally had received education on breastfeeding and breastfeeding support as part of their theoretical and clinical curriculum. Data was collected online via Google Forms from January 15 to March 15, 2024.
Data Analysis
Descriptive statistics were calculated to summarize participant characteristics and item distributions. Internal consistency of the scale was evaluated using Cronbach’s alpha, which assesses the degree to which the items measure a single underlying construct. Alpha values above 0.70 are generally considered acceptable, whereas values above 0.90 are regarded as indicating excellent internal consistency (Tavakol & Dennick, 2011). Item-Total Correlations (ITC) were then examined to assess each item’s contribution to the overall construct. Pearson correlation coefficients were computed between each item score and the total scale score. This method is widely used to evaluate the discriminative power of individual test items and their contribution to the overall scale structure (DeVellis & Thorpe, 2021; Nunnally & Bernstein, 1994). ITC values below 0.30 indicate weak association with the scale, whereas values of 0.50 or higher indicate strong internal consistency and good alignment with the latent construct (Wu & Adams, 2007).
For psychometric validation under item response theory, the Rasch measurement model was applied to the 34 Likert-type items to examine unidimensionality, the hierarchy of item difficulty, and response scale functioning on a common logit metric. The Rasch model estimates both item difficulty and respondents’ latent trait levels on the same interval scale, enabling direct comparison of item and person locations (Bond, 2015). The model assumes that a student with a higher latent ability (self-efficacy) has a greater probability of endorsing any item at a higher (easier) category than a student with lower ability. In this study, item difficulty values were normalized and rescaled so that the mean item difficulty was centered at zero. In Rasch analysis, items with higher difficulty parameters are likely to be endorsed only by individuals who possess higher levels of the underlying latent trait (Tennant & Conaghan, 2007; Wright & Masters, 1982). To ensure the Rasch model was appropriate, key assumptions were checked: unidimensionality and local independence. Unidimensionality and local independence were evaluated through Principal Components Analysis of standardized Rasch residuals. The scale was considered essentially unidimensional if the primary Rasch dimension explained a substantial portion of the total variance (ideally > 50%) and the largest secondary dimension (the first residual contrast) had an eigenvalue of less than 2 (Christensen et al., 2024; Stolt et al., 2022). An Essential Unidimensionality Index was also computed, with values above 50% indicating acceptable unidimensionality (Linacre, 2023; Liu et al., 2023).
Item fit was examined using infit and outfit mean-square (MnSq) statistics for each item. These indices reflect the extent to which observed responses match model expectations, with values between 0.5 and 1.5 considered acceptable (Linacre, 2017). Items with values above 1.5 were flagged as exhibiting underfit (unmodeled noise or potential multidimensionality), whereas values substantially below 0.5 indicate overfit (redundancy or deterministic responses). We also inspected the point-measure correlations (PTMEA) for each item, which are the correlations between item scores and the person measures, similar to item–total correlations but on the Rasch metric.
As a Rasch-specific indicator of reliability, the Person Separation Index (PSI) was used to determine the scale’s ability to distinguish between individuals with varying levels of competence. The PSI is computed as the ratio of true person variance to the total variance, and is considered a Rasch-equivalent of Cronbach’s alpha (Tennant & Conaghan, 2007; Wright & Masters, 1982). While PSI values above 0.70 are accepted as sufficient for group-level comparisons, values exceeding 0.85 are deemed appropriate for individual-level decision-making (Tennant & Conaghan, 2007). Additionally, rating scale functioning was assessed by examining category frequencies, average measures, Andrich thresholds, and category fit statistics to confirm order and consistent category use. To facilitate interpretation of the Rasch model outputs, a Wright Map (person–item map) was generated. This map plots the distribution of student self-efficacy measures alongside the distribution of item difficulty calibrations on the same logit continuum. The Wright Map enables a visual inspection of how well the items target the latent traits across different respondent ability levels (Tennant & Conaghan, 2007). All analyses were conducted using SPSS (Version 30) for classical test theory indices, and Winsteps (Version 5.10.2; Winsteps® Rasch Measurement, Beaverton, OR) for Rasch modeling.
Results
Participant Characteristics
A total of 382 participants completed the survey. Of these, 41% (n = 157) were third year midwifery students and 59% (n = 225) were in their fourth year. More than half (53%, n = 204) had completed a course titled “Breastfeeding Counselling,” while 86% (n = 320) had taken an obstetrics course, and 78% (n = 298) had received breastfeeding-support training as part of a child health course. Most participants (94%, n = 358) had provided breastfeeding support in clinical practice, and 78% (n = 296) had delivered breastfeeding support to a family member, friend, or acquaintance outside of clinical practice. Of the 382 respondents, three were excluded from the psychometric analyses due to missing data.
Internal Consistency and Item Analysis
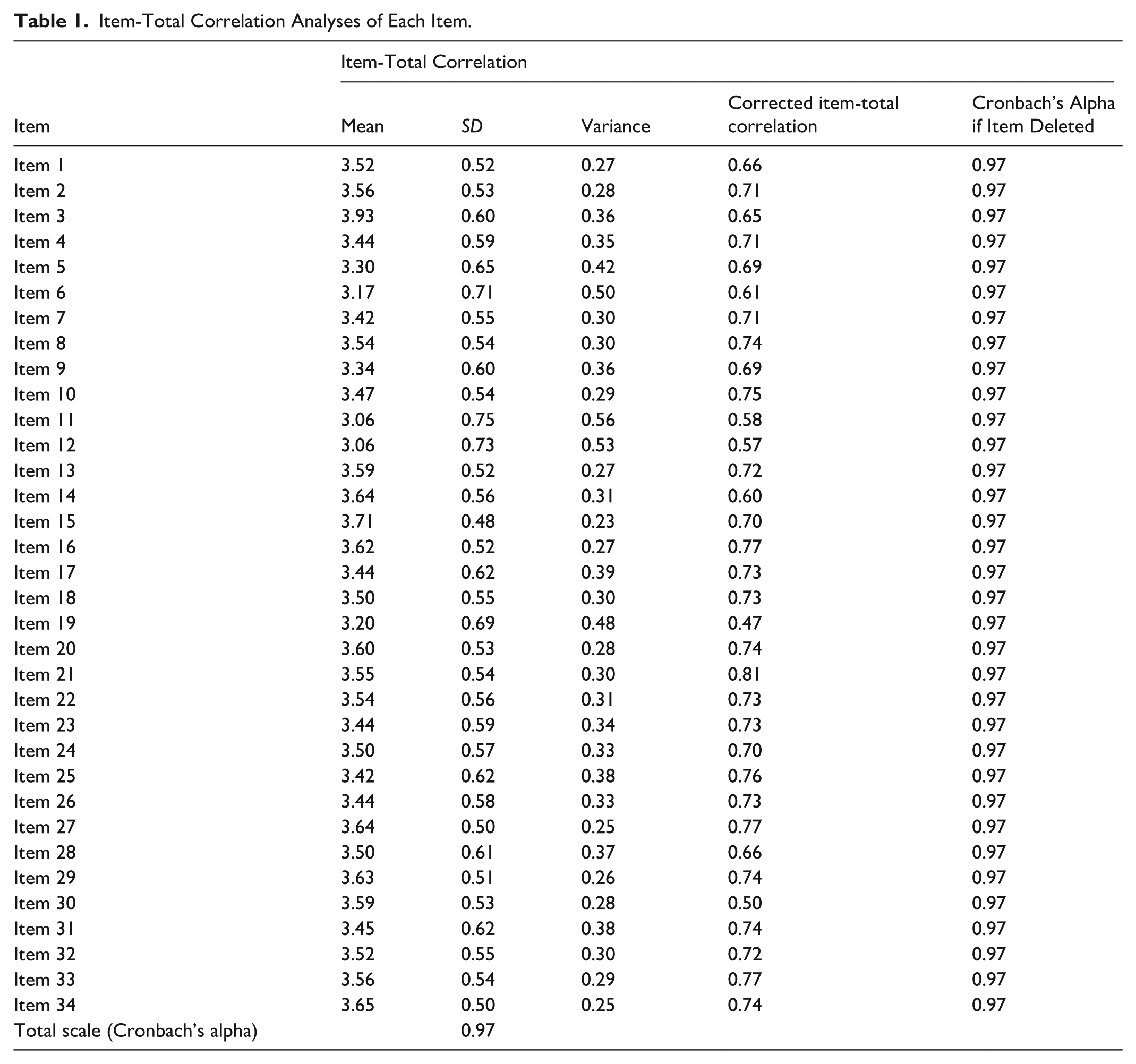
The Turkish version of the 34-item scale demonstrated excellent internal reliability, with a Cronbach’s alpha coefficient of 0.97. Corrected item–total correlations ranged from 0.47 to 0.81, exceeding the minimum acceptable criterion of 0.30. Cronbach’s alpha remained stable when any single item was deleted, with all values remaining at 0.97, indicating that the removal of any individual item did not alter the overall reliability of the scale. Across the 34 items, mean scores on the 1–4 scale ranged from 3.06 to 3.93 (Table 1), with most items clustering around the response category “It is easy for me to do this” (Supplementary file 2). The lowest mean scores were observed for Item 11 and Item 12 (both means = 3.06), while the highest mean score was observed for Item 3 (mean = 3.93; see Table 1).
Item-Total Correlation Analyses of Each Item.
Rasch Model Analysis
Rasch Item Measures, Fit Statistics, and Point–Measure Correlations.
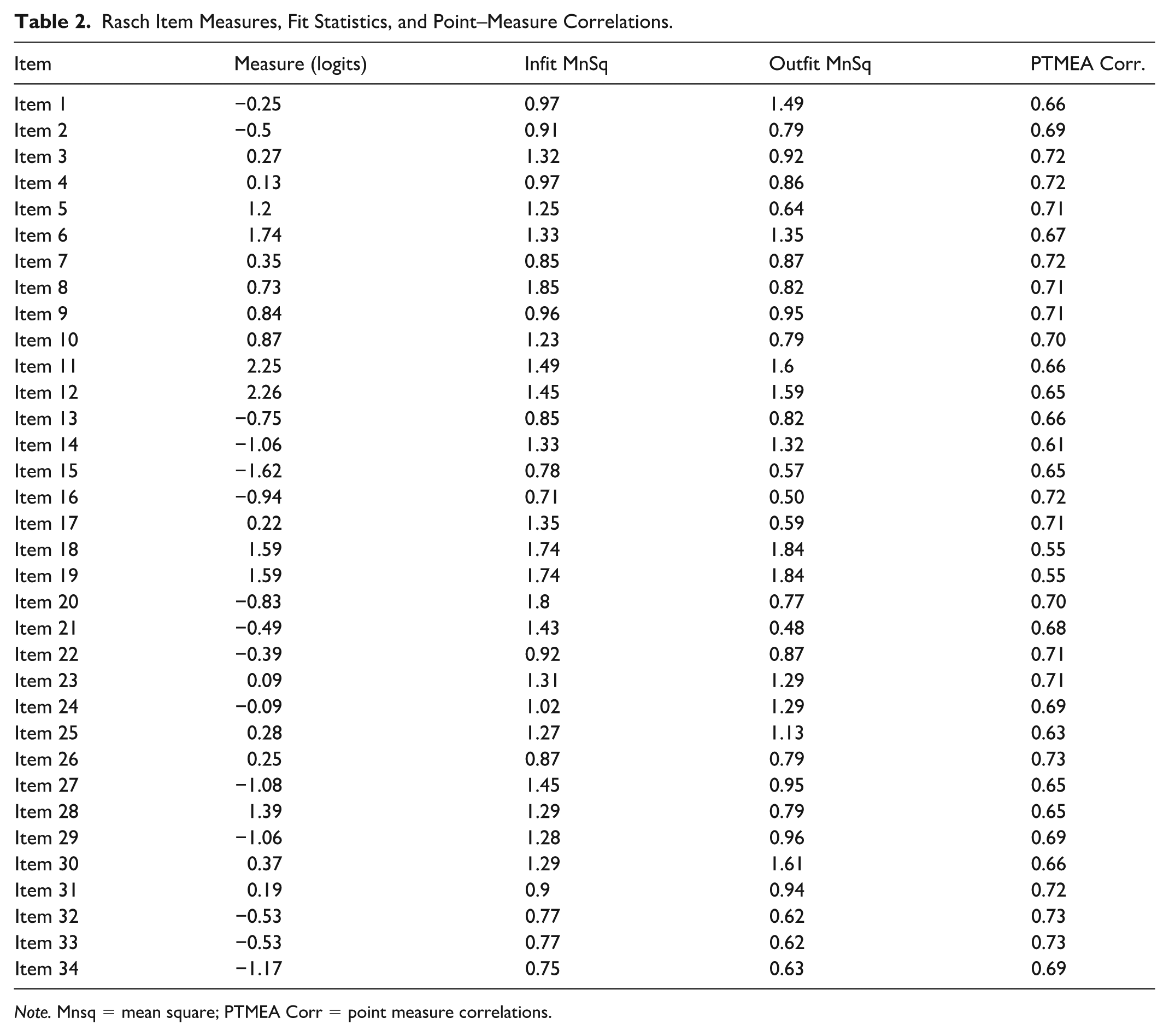
Note. Mnsq = mean square; PTMEA Corr = point measure correlations.
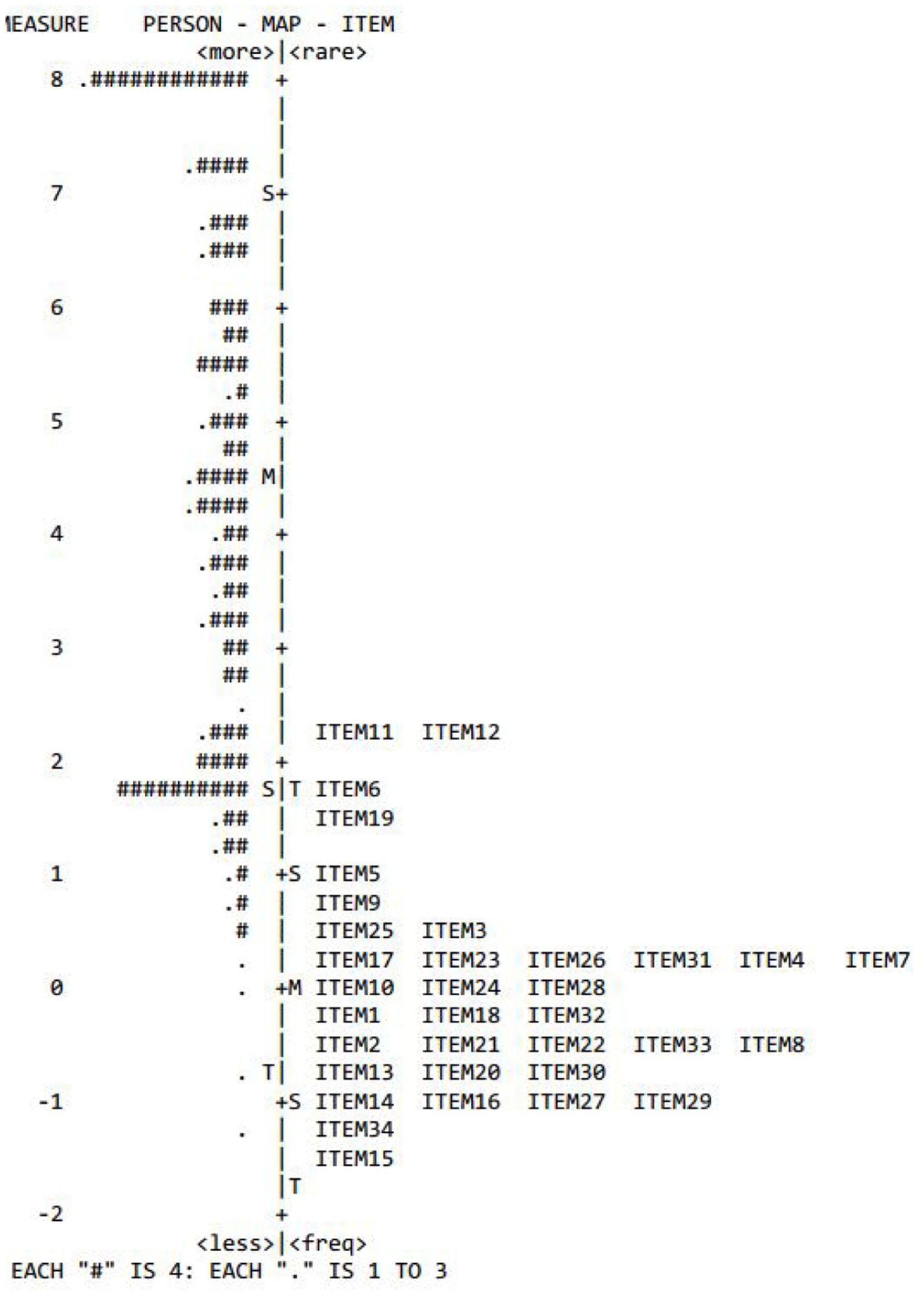
Wright map.
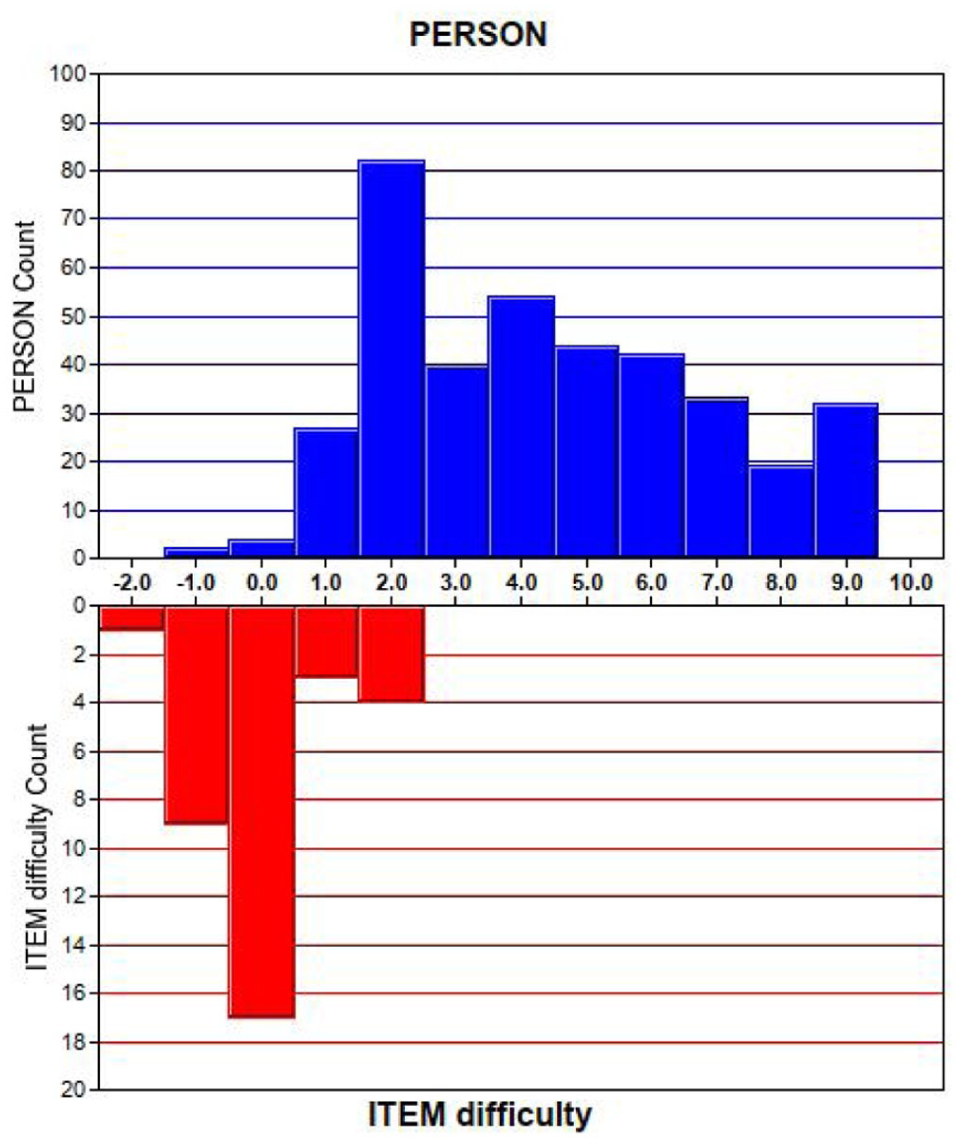
Histogram representation of the distribution of person abilities (upper panel) and item difficulties (lower panel) along the same logit scale.
Discussion
This study provides strong evidence supporting the validity and reliability of the Turkish version of the Self-Efficacy Scale for Breastfeeding Support. Consistent with the original tool developed by Blackman et al. (2015) and the Italian validation study by Melchionda et al. (2019), the scale demonstrated strong psychometric properties when evaluated using both classical test theory and Rasch measurement methods. These findings extend the scale’s applicability to a new cultural and educational context.
In the present study, overall self-efficacy levels were high, with mean item scores clustering around the “It is easy for me to do this” response category. This finding is comparable to those reported among Australian and Italian midwifery students (Blackman et al., 2015; Melchionda et al., 2019), suggesting Turkish midwifery students generally perceived themselves as confident in providing breastfeeding support. This is not unexpected, given that most participants receive breastfeeding support education and have experience providing support in both clinical settings and outside their clinical practice.
Despite generally high self-efficacy scores, the Rasch item hierarchy in the present Turkish study revealed meaningful differences in perceived difficulty across breastfeeding support tasks. Items requiring management of infant behavior during breastfeeding were among the most difficult to endorse. Specifically, the item addressing understanding infant crying in relation to breastfeeding (Item 11) emerged as the most difficult, while maintaining infant alertness during breastfeeding (Item 12) was also located toward the higher end of the difficulty continuum, suggesting that infant support skills were perceived as more demanding than routine breastfeeding guidance. This pattern is also reflected, to some extent, in the Italian study (Melchionda et al., 2019), in which Item 11 similarly appeared among the most difficult items. In contrast, the Australian students reported greater item difficulty across social support and motivational domains, including “gain her family’s support in her decision to breastfeed” (Item 7), “motivate her to breastfeed successfully” (Item 8), and “explain to the mother the benefits of breastfeeding” (Item 27; Blackman et al., 2015).
Conversely, in the current study, items reflecting foundational breastfeeding knowledge and standard counseling messages were among the easiest to endorse. These included advising and motivating exclusive breastfeeding during the early postnatal period (Items 14–16), explaining the benefits of breastfeeding (Item 27)—especially the first breastfeed within the first hour after birth (Item 34)—and promoting skin-to-skin contact within 1 hour post-birth (Item 29) was among the easiest to endorse. This clearly shows that core breastfeeding principles are well embedded in the Turkish midwifery curriculum, whereas more practice-based skills, such as responding to infant behavior and infant support, appeared more challenging, indicating greater difficulty with skills that rely on assessment, attunement, and interaction within the mother–infant dyad. This also aligns closely with the findings of Swerts et al. (2016), who described midwives’ breastfeeding support as being predominantly framed around a “technical expert” role that is breast-centered and task-focused, while the “skilled companion” role, which is woman-centered, relational, and attentive to infant cues and mother–infant interaction, was less prominently enacted in practice. Managing infant behavior, such as responding to crying, feeding cues, or settling difficulties, is a core component of this skilled companion role and requires experiential, integrated learning rather than declarative knowledge alone.
The Rasch person–item targeting indicated some degree of scale mistargeting at the upper end, with several highly confident students exceeding the difficulty range of the items. While this generally confirms high self-efficacy within the cohort, it also suggests that the scale may be less sensitive in distinguishing among students with advanced breastfeeding support skills. Similar targeting issues have been observed in the Australian validation study (Blackman et al., 2015), where students’ ability exceeded item difficulty, particularly at baseline, prior to an educational intervention. Following the education, item difficulty was redistributed, and the range of perceived self-efficacy narrowed, suggesting that this phenomenon reflects a common measurement challenge in self-assessment among well-prepared student cohorts, rather than a limitation unique to the Turkish version.
The validation of the self-efficacy scale for breastfeeding support among Turkish midwifery students provides a valuable measurement tool for students to self-assess their perceived competence in this domain. From an educational and clinical perspective, identifying areas of lower self-efficacy is crucial, as self-efficacy plays a central role in translating knowledge into practice, and influences clinical behavior, persistence, and willingness to engage in complex caregiving tasks (Bandura, 1986). Clinicians are required not only to apply theoretical knowledge but also to rely on practical skills and professional confidence when supporting breastfeeding mothers (Akmeşe & Bay, 2023; Freed et al., 1996; Prepelita et al., 2020). The use of validated self-efficacy measures during undergraduate education may therefore support targeted feedback, enhance reflective learning, and guide curriculum refinement. Studies have shown that structured feedback and skills-based education can improve students’ confidence, motivation, and performance in breastfeeding support roles (Healer, 2015; İlkin et al., 2022; Ward & Byrne, 2011). Given the global emphasis on breastfeeding promotion initiatives such as the Baby-Friendly Hospital Initiative and WHO–UNICEF recommendations (WHO, 2026), ensuring that midwifery students graduate with high self-efficacy in breastfeeding support skills is essential. Instruments that reliably measure students’ perceived competence can improve educational quality and, ultimately, breastfeeding outcomes for mothers and infants.
Several limitations of this study should be acknowledged. First, the use of self-reported self-efficacy may not fully reflect actual clinical competence and may be influenced by social desirability bias. Second, cross-sectional design limits conclusions regarding changes in self-efficacy over time or in response to specific educational interventions. Third, we were unable to reach the third- and fourth-grade midwifery students at all universities in the country. It is thought that it would be more beneficial to include students from all universities to ensure generalizability. Lastly, the study was conducted within a specific educational and cultural context, which may limit generalizability to other settings.
Despite these limitations, the study provides strong support for the validity and usefulness of the Turkish version of the scale in midwifery education and practice. Rasch analysis provided a statistically significant method and enabled validation of the questionnaire in Turkish. Therefore, it was found that the Turkish version of the instrument can effectively assess midwifery students’ perception of self-efficacy in providing breastfeeding counseling to breastfeeding mothers. In this context, providing breastfeeding support education with a measurement- and evaluation-based approach in the learning process for midwifery students will enable objective, comprehensive learning, making it easier to identify when the student feels self-sufficient and when not, and to eliminate any deficiency. Midwifery students should be motivated by enabling them to take part in studies to provide the mother with strategies to meet her baby’s breastfeeding demands and to be more confident providing breastfeeding support.
Conclusion
This study confirms that the Turkish adaptation of the self-efficacy scale originally developed for Australian midwifery students is a valid and reliable tool for self-assessing competence in breastfeeding support. Using both classical test theory and Rasch measurement, the scale demonstrated excellent internal consistency, strong item functioning, and a largely unidimensional structure, confirming its robustness in the Turkish educational context.
The findings indicate that Turkish midwifery students generally report high self-efficacy for foundational breastfeeding tasks, while more complex, practice-based skills, such as managing infant behavior during breastfeeding, require higher levels of confidence. Overall, the validated Turkish version is a psychometrically sound tool for self-assessing breastfeeding support self-efficacy, and may be used to inform curriculum evaluation, guide targeted educational interventions, and enable cross-cultural comparison. Its use may strengthen midwifery education and improve the quality of breastfeeding support for mothers and infants.
Supplemental Material
sj-docx-1-jhl-10.1177_08903344261455174 – Supplemental material for Psychometric Evaluation of the Turkish Version of a Breastfeeding Support Self-Efficacy Scale for Midwifery Students
Supplemental material, sj-docx-1-jhl-10.1177_08903344261455174 for Psychometric Evaluation of the Turkish Version of a Breastfeeding Support Self-Efficacy Scale for Midwifery Students by Filiz Aslantekin Özçoban, Hava Özkan, Esra Çevik, Alemayehu Mekonnen, Amanda Muller and Linda Sweet in Journal of Human Lactation
Footnotes
Acknowledgements
We would like to thank the study participants for their contributions and for sharing their experiences.
Ethical Considerations
The study was conducted in accordance with the principles of good clinical practice (GCP) and the Data Protection Act (2018). Ethical approval from Atatürk University Research Ethics Committee (Ref:2024/01/02) was obtained. The date of approval: 03 /01/2024
Author Contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplementary Material may be found in the “Supplemental material” tab in the online version of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.