
Abstract
Drawing on 121 in-depth interviews with first- and second-generation women and men physicians of Indian origin in the U.S. Southwest, I examine the incidence and nature of gender-based discrimination in American medicine. I focus on two aspects: (1) gender discrimination by employers and colleagues against women physicians of Indian origin and (2) the interaction of gender discrimination with race in the professional lives of first- and second-generation physicians. U.S. healthcare has become increasingly dependent on immigrants, in particular women physicians, from the developing world. I document the significant impact gender and race can have in molding the professional trajectories of Indian women physicians. The experiences of these physicians help clarify the interaction of skilled migrant workers with racial/ethnic and gender relations in U.S. workplaces.
There is almost a racial hierarchy that exists. If for the same job there are four-five options available, and it’s not just the race, it’s also gender. So if there is a white male available, that will always be the number one choice. So if you have to go and make a rank order list, in general white male gets preference, and then black male second, then white female, then Indian male, then black females, and then everybody else. And Indian female comes, really, at the bottom. And sometimes equal to or even below the Hispanic. This is just the way they work. And it does not matter whether the person making decision up top necessarily is black or white or Indian. (Piya Jaiswal, first-generation woman)
This study examines how race/ethnicity, gender, and nationality shape the experience of Indian physicians in the United States, and how in the environments of racially different foreign-born medical professionals, gendered and racial dynamics create complex conditions of inequality and disadvantage for women of color. I explore how workplaces are gendered, but also racialized. I further consider how discrimination based on nationality and country of medical training impacts these experiences.
Gender constitutes “an emergent feature of social situations: both as an outcome of and a rationale for various social arrangements and as a means of legitimating one of the most fundamental divisions of society,” often tailoring the limits and the choices of women in the United States (West and Zimmerman 1987, 126). A gendered hierarchy that privileges hegemonic masculinity and subordinates or excludes women is embedded within the assumptions and practices that comprise most contemporary work organizations (Acker 1990). This is achieved by the reproduction of complex inequalities within organizations through gendered relations at work that pattern “advantage and disadvantage, exploitation and control, meaning and identity” in terms of a distinction between men and women (Acker 1990, 146). In fact, professional women of color are at an added disadvantage, being differentially situated in workplaces (Crenshaw 1991). They often find themselves as the sole representative of their demographic group, and more vulnerable to stereotyping because of their extreme visibility as tokens (Browne and Misra 2003; Kanter 1977).
The differential treatment they receive because of their gender and race culminates in second-class citizenship for them (Collins 2001), multiplying the disadvantages of race and gender (Browne and Misra 2003; King 1989). Particularly for first-generation women, the social categories of race and gender merge with nationality to create intersecting systems of oppression that mutually constitute, maintain, and transform each other rather than functioning as independent structures of inequality. This results in a matrix of domination that interlocks privilege and disadvantage (Collins 2000), playing a critical role in shaping the experiences of women physicians of Indian origin in the United States.
Drawing on more than 100 interviews with Indian physicians—both first- and second-generation—as well as interviews with some non-Indian administrators, I explore how gender, race, and nationality intersect in the experiences and perceptions of Indian physicians in the United States. This allows me to paint a rich portrait of how Indian women physicians continue to experience discrimination in the United States in the twenty-first century.
Literature Review
Acker (2006) describes inequality in organizations as differential access between men and women in power in their control over goals, available resources, and their outcome. Organizational practices, in turn, reinforce the segregation of work by gender, widen status and income disparity between men and women, and replicate cultural stereotypes of gender. Gender stereotypes portray women as less competent and better at less valued communal tasks when compared to men, who are viewed as status worthy, instrumental, and agentic. In professional fields that have been culturally perceived as masculine, like management, defense, or medicine, men are evaluated more favorably than women (Ridgeway and Correll 2004). Therefore, even when women perform comparably to men, men are regarded as being more capable at a given task than women, who may have to accomplish more than men to be rated equally (Correll 2004 ).
For instance, women-dominated occupations and whole subsections of U.S. medicine with a high rate of female physicians have less standing in terms of income, prestige, and career opportunities (Heath 2004). Research shows that women in academic medicine earn less than men with similar productivity (Ash et al. 2004). Women are also passed over in rank advancements (Dobson 1997). The glass ceiling in U.S. academic medicine is often seen as hindering the advancement of women into leadership positions despite any tangible barriers (Carnes, Morrissey, and Geller 2008). The present academic structure perceives women as less competitive and with fewer leadership abilities, underrepresenting women in positions of management and leadership (Eagly and Karau 2002).
Academic medicine in particular mirrors the dichotomy between the numerical strength of women in the field versus their underrepresentation in leadership positions and among tenured faculty. Studies show how systematic disadvantages, like the absence of effective mentorship, harsh and sexist work environments, and inadequate job opportunities, limit the career advancement of women in U.S. academic medicine (Carnes, Morrissey, and Geller 2008; Carr et al. 2003). Besides, women are more apt to engage in “institutional housekeeping” and be educators and clinicians instead of being on research-based faculty tracks that lead to management positions (Bird, Litt, and Wang 2004). For instance, in 2005 only 11 percent of department chairs, 15 percent of full professors, and 32 percent of U.S. medical school faculty were women; in academic surgery, women comprised only 2 percent of department chairs, 6 percent of full professors, and 16 percent of the faculty (Kass, Souba, and Thorndyke 2006, 179). Moreover, women comprise 10 percent or fewer of department chairs in psychiatry and pediatrics, fields in which women have constituted at least 50 percent of those workforces for the past two decades (Carnes, Morrissey, and Geller 2008, 6). Women headed only 20 percent of the National Institutes of Health (NIH) in 2006, receiving lesser budget increases than units headed by men (Carnes, Morrissey, and Geller 2008, 6). Even when women attain management positions, research shows that they are closely scrutinized (Bendl and Schmidt 2010). But given the already troubled waters for women physicians in the United States, there is strangely little research investigating how women physicians from ethnic minorities fare in an essentially white male–dominated medical environment.
Academic medicine in particular mirrors the dichotomy between the numerical strength of women in the field versus their underrepresentation in leadership positions and among tenured faculty. Studies show how systematic disadvantages, like the absence of effective mentorship, harsh and sexist work environments, and inadequate job opportunities, limit the career advancement of women in U.S. academic medicine (Carnes, Morrissey, and Geller 2008; Carr et al. 2003). Besides, women are more apt to engage in “institutional housekeeping” and be educators and clinicians instead of being on research-based faculty tracks that lead to management positions (Bird, Litt, and Wang 2004). For instance, in 2005 only 11 percent of department chairs, 15 percent of full professors, and 32 percent of U.S. medical school faculty were women; in academic surgery, women comprised only 2 percent of department chairs, 6 percent of full professors, and 16 percent of the faculty (Kass, Souba, and Thorndyke 2006, 179). Moreover, women comprise 10 percent or fewer of department chairs in psychiatry and pediatrics, fields in which women have constituted at least 50 percent of those workforces for the past two decades (Carnes, Morrissey, and Geller 2008, 6). Women headed only 20 percent of the National Institutes of Health (NIH) in 2006, receiving lesser budget increases than units headed by men (Carnes, Morrissey, and Geller 2008, 6). Even when women attain management positions, research shows that they are closely scrutinized (Bendl and Schmidt 2010). But given the already troubled waters for women physicians in the United States, there is strangely little research investigating how women physicians from ethnic minorities fare in an essentially white male–dominated medical environment.
With race and gender as a foundation for exclusion or for hiring still persisting in many organizations (Acker 2006), gender and racial inequalities are often re-created by interaction practices that are unspoken, subtle, and difficult to document (Acker 2006). Collins (2001) shows that racial/ethnic minority groups encounter a politics of containment, ridden with exploitation of less powerful racial groups for the benefit of more powerful racial groups (Collins 2001). Existing intersectional research on gender and race shows that ethnic minority women unlike their white female counterparts contend additional burdens of gender and race, their achievements are undervalued, and they are assigned less responsibility than they can handle (García-López 2008). Women of color report higher occurrences of being denied opportunities for advancement than did white women (Shrier et al. 2007). Earning differentials still persist across ethnic groups even after controlling for other factors like level of education, region, and occupation (Kim and Sakamoto 2010). Structural arrangements following a racial hierarchy further provide social and economic advantages to whites by offering them better opportunities in terms of “enhanced college admissions, favored job interviews, improved career opportunities, and higher labor market rewards” (Kim and Sakamoto 2010, 935), whereas Asian Americans, despite their professional attainments in the United States, are required to be more educated to receive a similar income to whites (Waters and Eschbach 1995).
Research also shows that Asians are unable to achieve full equality in the U.S. labor market in lieu of fewer economic returns for their level of education when compared to their white counterparts and the glass ceiling that accounts for their absence in top executive positions despite their considerable numbers in such occupations (Espiritu 1997; Kibria 1998; Purkayastha 2005). Despite controlling for individual-level characteristics, substantial differences in the earnings between Asian Indian women and white women persist (Stone, Purkayastha, and Berdahl 2006). Purkayastha (2005) in her research shows that experiences of racialization make even second-generation South Asian Americans who are economically incorporated into U.S. mainstream view themselves as distinct from white Americans and other Asian American groups. More so, when accompanied by discrimination and prejudice, their physical features act as a barrier at the workplace (Portes and Zhou 1993). In fact, Murti (2012) finds that Indian male physicians find greater social acceptance in public on revealing their occupational status, whereas Indian female physicians become more intimidating socially and risk greater social marginalization for seizing high social status reserved for white men.
Gender and racial discrimination thus act as a double bind for minority women in medicine, who, when compared to men, report higher levels of discrimination (Carr et al. 2007). Gray, Gallagher, and Masters (1996) report substantial differences in perceptions for women and minority graduates compared to white male graduates regarding experiences at medical school and the professional medical environment in the United States. Minority faculty members report lower levels of satisfaction (Palepu et al. 2000) and are more likely to leave their academic careers (Hadley et al. 1992). This dissatisfaction can be traced to lower returns on education for first-generation Indians, who are paid well but less than whites in medical and other professions in the United States (Barringer and Kassebaum 1989), and a lower rate of promotion of minority faculties compared to their white counterparts in medicine (Fang et al. 2000; Palepu et al. 1998).
Labor market opportunities and incorporation are further impacted by nationality and citizenship status along with gender, race, and ethnicity (Browne and Misra 2003). However, the interlinked impact of gender, race, and nationality in shaping the career trajectories of Asian American women doctors has largely remained unexamined (Xu and Leffler 1992). Purkayastha (2005) argues that compared to their counterparts with credentials from the developed world, immigrants from former colonies are often held back. Foreign medical degrees act as a “major liability,” enhancing the “difficulty” of “breaking in” even for women who have better access to networks of Indian physicians (Purkayastha 2005, 188). These women also encounter “subtle forms of gender and race marginalization” (Purkayastha 2005, 191). In fact, first-generation immigrant women from ethnic minorities face a triple bind in American medicine, with the addition of bias against foreign medical graduates.
Research shows that foreign medical graduates who are largely first-generation immigrants face added prejudice and are discriminated against very or somewhat significantly (Coombs and King 2005), either overtly or in subtle ways, on the basis of their country of origin, xenophobia, and chauvinistic attitudes (Desbiens and Vidaillet 2010). In fact Coombs and King (2005) in their survey of 445 licensed physicians in Massachusetts found more than 60 percent of their respondents to have reported that discrimination against foreign medical graduates was very or somewhat significant. While 44 percent of U.S. medical graduates reported that discrimination against foreign medical graduates in their present organization was significant. Moreover, there are relatively fewer foreign medical graduates than American graduates in competitive, financially lucrative specialties (Brotherton and Etzel 2010; Ebell 2008). Surgery in particular is infamous for discriminating against foreign medical graduates, with some surgical directors acknowledging external pressure to rank a U.S. medical graduate over a better-qualified foreign medical graduate (Desbiens and Vidaillet 2010).
Focusing on any one category ignores the internal divisions of races along gender and nationality lines, and precludes an understanding of how these categories have a complex, mutually reinforcing or contradicting interaction. I focus on discrimination by race and gender, along with nationality, which has introduced another facet of discrimination through a new visa category (H-1B and J-1) 1 for high-skilled nonimmigrant (temporary) workers in the United States. I argue that workspaces of Indian physicians in the United States are significant social spaces for the perpetuation of gendered, racialized, and ethnicized norms. My primary research question is “How does gender discrimination in U.S. medical workplaces manifest itself in the professional lives of women physicians of Indian origin?” To explore this, I focus on (1) gender discrimination by employers and colleagues against women physicians of Indian origin and (2) how gender discrimination interacts with race and manifests itself in the professional lives of first- and second-generation physicians. Lastly, I explain how analyzing these physicians’ experiences can help us understand the operation of gender and race in the medical workplace in new and important ways.
Method
The racial experiences of Indian physicians in the United States have been studied in a few works (Sethi 2003), and limited primarily to third-person narratives, while there is very limited research on the experiences of Indian women physicians in U.S. workplaces (Murti 2012). My study draws extensively on in-depth interviews addressing the general and specific attitudes of Indian physicians and some administrators toward gender and racial discrimination in the workplace. I used semi-structured interviews, 2 where “two individuals come together to try to create meaning about a particular topic” (Esterberg 2002).
I identified 108 physicians, 43 women and 65 men, 3 whom I interviewed in the summer and fall of 2009 and 2010. 4 Thirteen of these 108 physicians were reinterviewed in 2010, 5 leading to a total of 121 interviews with 108 physicians. Of the total sample size, 55 interviews were carried out with first-generation Indian physicians, 59 with second-generation Indian physicians, and seven with senior faculty in higher administrative positions. 6 The criteria of eligibility for the participants included self-identifying as physicians of Indian origin, being over the age of 18, and engaged in training (residency or fellowship) or employed at the time of the interview. To be categorized as second-generation, participating physicians had to have been born in the United States and have one or two immigrant parents, or have migrated to the United States when they were 10 years old or younger. 7
I conducted my research in a large metropolitan area housing a major biomedical research center, making it a common location for Indian physicians in U.S. Southwest. I established my initial round of participants using a snowball sampling technique by contacting Indian physicians employed or in training, through emails listed on the medical center department websites. Once I established my initial round of participants, I requested referrals to other physicians who might be interested in participating in this study, indicating that I was interested in how Indian physicians experience gender and race relations in the workplace, and racial and gender discrimination, if any, in particular.
Being a first-generation Indian woman, I was unsure if I would be able to inspire the trust needed of second-generation physicians to be candid about their emotions, dilemmas, and fears about discrimination in and out of American medicine. Yet, I found the second-generation physicians to be much more enthusiastic, articulate, and forthcoming participants. However, I did face greater difficulty in securing interviews with first-generation Indians vis-à-vis their second-generation counterparts, which might have less to do with my identity and more to do with their unwillingness “to face the reality of racism,” as Ritika, a first-generation female, put it.
After obtaining the consent of my research participants I audio-recorded each interview. I transcribed every interview verbatim myself. Finally, I coded each of the interviews by organizing all the material thematically and cross-listing pieces that were relevant to more than one area. Given the sensitivity of the subject, and the extent to which the physicians were self-selected, I was able to interview only women and men who were forthcoming about revealing how they experience race and gender relations at work. I have attempted to portray their experiences in this research with the same sincerity and honesty. Table 1 summarizes the characteristics of physicians of Indian origin enrolled in the study.
Characteristics of Physicians of Indian Origin Enrolled in the Study

Immigrants who immigrated at a young age and underwent most of their childhood and adolescent socialization in the United States.
Residents and fellows in training at a university hospital setting.
Academic medical faculty at a university hospital setting.
The following sections address findings of the three major issues that emerged in my interviews.
Gender Discrimination in American Medicine
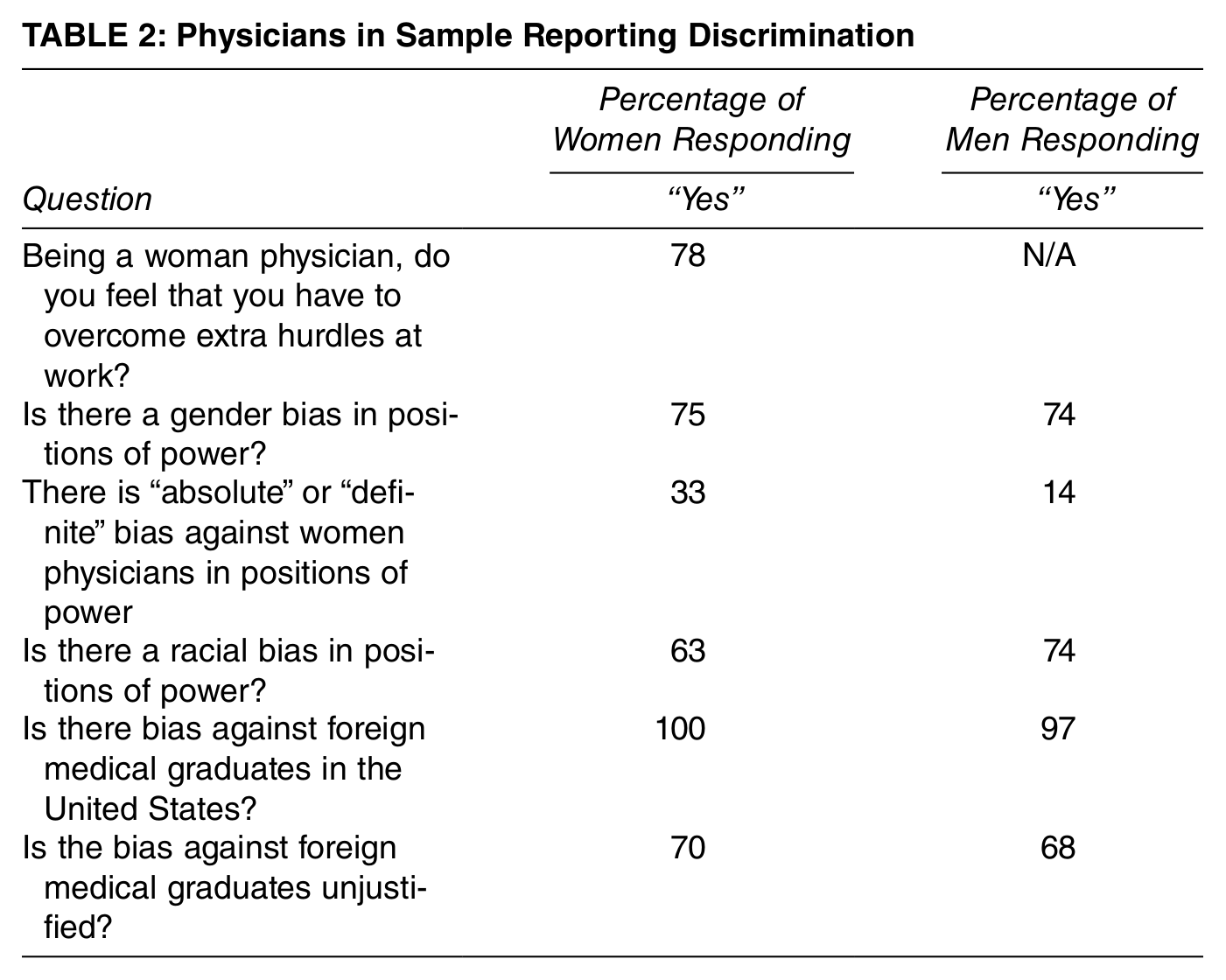
A majority of the Indian women physicians who were interviewed for this research experienced gender-based discrimination at all levels in the medical workplace—as residents and faculty, and in promotions to positions of power. 8 Most women physicians reported experiencing gender-based discrimination (see Table 2), with almost one-third reporting “absolute” or “definite” bias against women physicians who were in positions of power. Several examples of these reports are given in this section to illustrate and elaborate on these cases.
Physicians in Sample Reporting Discrimination
Gender discrimination was visible even in the recruitment process, when women were asked questions about their families unlike their male colleagues, despite such questions being illegal. Shweta, a second-generation female, noting that the same was not true for her male colleagues, recounts about her residency interviews:
I was asked whether I was single, whether I was seeing somebody, whether or not I was serious or married, and if there was any possibility of me having children. These are personal. And in fact the ACGME [Accreditation Council for Graduate Medical Education], ERAS [Electronic Residency Application Service], and all of those institutions will flat out tell you these are illegal questions that are not supposed to be asked during an interview.
The women in my sample also reported that women residents were reprimanded more severely than men residents for the same mistakes.
Both men and women physicians argued that competitive procedure-oriented specialties and subspecialties like general surgery and orthopedics were fields where women physicians faced discrimination. Women noted that both attending physicians and fellow colleagues tried to steer women away from opting for these specialties, suggesting that probable family commitments might impede them from committing the requisite time in these subfields. Women physicians instead reported being steered more towards “less time and labor-intensive specialties” like psychiatry, pediatrics, and family medicine. These branches were also both less remunerative and less competitive. Women residents perceived discrimination from women attending physicians and the nursing staff. Tanuja felt that because women attendings “had a hard time” in medicine and “had more hoops to jump through” they took out their “frustration” on their female residents.
Women also perceived greater challenges for women in being promoted in academic medicine. Lata, a second-generation female, revealed, “Men much more often get promoted than women and get promoted to higher positions more quickly than women. . . . I feel like their [men’s] accomplishments get recognized more often.” When it came to hiring women in leadership positions or promoting them to positions of power, a number of first- (Hemant, David) and second-generation (Mahesh) men faculty voiced similar points to Shweta, who voiced:
it’s kind of an old boys club [in medicine], so if you are a white Caucasian male it’s easier for you than if you are a woman or of color. . . . I mean, you can look at our institution, the head of medicine has been a male for years, I don’t think there’s ever been a female head of medicine.
Previous research has shown that women in traditionally male professions, like medicine, face stereotyping and negative judgments (Williams 1992). Successful women in these jobs may face a double-bind, as they are viewed as “hostile” (Heilman 2001, 667-68) and less “nurturing” (Benard and Correll 2010, 620). Jennifer, a white senior faculty member, revealed that “if a woman is really strong, then people are kind of angry and bitter about that, but if a man is really strong, then he is viewed as a strong leader. . . . I think that sort of perception that a woman is a man-hater, or they use that phrase ‘ball-buster.’” These adverse reactions augment the challenges that women in managerial positions face and also perpetuate the glass ceilings they encounter (Ridgeway and Correll 2004). Sheila, a first-generation female, similarly commented:
One of my attendings [an African American female] in residency told me, “You have to wear balls around your neck. You have to think like a man, and you have to act like a man, otherwise you can’t survive in academics or anywhere.”
Moreover, Shaurya, a first-generation man, argued:
Women physicians [in positions of power] have a harder time than male physicians. . . . [A] lot of women physicians feel like they need to work twice as hard than [sic] their male counterparts to get the same respect. And on the same side, if a male physician is abrasive and authoritative, people are kind of more scared of him and they will get more respect than if the female is the same way and the female will be regarded more as just a bitch.
Overall, both men and women in my sample reflected their perceptions that women physicians faced significant challenges in being seen as leaders or being promoted to upper ranks.
For women physicians, perceptions of possible motherhood, and motherhood itself, exacerbated their discriminatory experiences in the workplace at all levels of their medical training and career (Duffy 2007; Glauber 2007). Status-based discrimination by employers stereotype mothers as “less competent and committed to paid work than non-mothers” (Benard and Correll 2010), and decreases their chances of getting training, winning promotions, or engaging in networking when they work part time (Dick and Hyde 2006; Lawrence and Corwin 2003).
These experiences are reflected in medical training, as well as in jobs and opportunities for promotion. For example, Shweta recollected:
There was one [Indian] girl who was pregnant when she started internship with us. . . . She had kind of planned it so that her vacation would be right around the time of delivery anyway, but they [faculty and administration] were like, “Why can’t you just get induced ’cause you are so close? That way you won’t mess up the call schedule or any of that other stuff.”
Priyanka, a second-generation female, similarly felt that women are “shamed for having a baby [in residency] . . . it’s really a very hostile environment to try to have a baby . . . it’s awful.” Harish, a second-generation male, senior male faculty in dermatology, revealed:
And what I see is that many of them [women faculty] are moms, so if they miss a few things, then instead of giving them support . . . what they do is they penalize them for that, by not giving them certain rank advancements or pay and things like that . . . we only have now two women left on all of our faculty . . . which is bad.
Similarly, Shaurya, a first-generation man noted, “I think there’s more of a stigma of being a woman, there’s a stigma of taking time off to have babies.” Lindsay, a white senior faculty in administration, noted that women physicians who “get on the mommy track . . . lose years of recruitment of seniority or on your promotion track.” With pervasive reservations and discouragement against motherhood in the medical environment, mothers who work part time faced even lower wages and fewer chances of promotions in the workplace.
Overall, both women and men physicians in my sample report fairly substantial gender discrimination from supervisors and coworkers in the workplace. This discrimination shapes each step of their careers, from applying for residencies, to jobs, to promotions. A part of this discrimination seems focused around the potential for motherhood to derail or slow women’s career progress. However, a large part of this discrimination as my findings reveal, is centered on the assumption that women are inherently less capable and hard working than men, and are more “obsessive” about details, hence more suitable for secretarial jobs than leadership positions in academic medicine.
Gender, Race, and Foreign Medical Graduates
Whenever I start a new job, or when I was training for my residency and fellowship, it’s a man’s profession. So number one, being a female you have to jump through extra hoops to establish yourself. And then, when you look like me and when you talk like me you stand out . . . if you are a new member of the team nobody is going to accept you . . . I have to prove myself, right? I have to prove that I am capable of taking care of the 20 patients that I am supposed to take care of. So when you are a female physician, and then you are a female “not Caucasian,” then you are definitely made to prove yourself twice over, before they accept you as one of them. (Deepti, first-generation female)
Gender, when combined with race, acted as a “double hit” for Indian women physicians in the workplace. The additional influence of foreign medical graduate bias in American medicine cumulates in a “triple bind” for first-generation Indian women physicians. All of the women respondents in this study perceived bias against foreign medical graduates in the United States (see Table 2). Jennifer, a white senior administrative faculty, acknowledged, “There is a lot of prejudice against people who trained elsewhere [in South Asia and Africa, unlike foreign graduates who trained in England or other Western European countries].” She explained, “Anytime somebody hears an accent you are immediately, I think, going to be treated differently. I think you are treated with less respect . . . people expect you not to be very good and they are surprised if you are . . . most people by nature are pretty xenophobic, unfortunately.” Likewise, Surbhi, a second-generation female, said, “Even in foreign medical graduates there is a different classification. So if you are from Canada or if you are from Europe you are considered okay on some level, but then if you are from Asia, and I don’t know why that bias is there.”
Ameena, a second-generation female, explained how, in her residency training program (internal medicine), the people who are selected as being chief residents are usually white men, reflecting how race and gender intersect in this selection process:
And if you go back the last five or ten years, there’s very few nonwhite women, or even nonwhite people, selected [as chief] residents. Yet the demographics of the residency class is not white men. White men are actually the minority . . . people [other students] have said, “You know, it’s funny that our chiefs are always white guys when most of the residents are not white guys.”
Harish, a senior faculty in dermatology, noted a similar pattern of selection of chief residents over the years.
Foreign medical graduate Indian women fellows and faculty members reported similar biases when it came to hiring, salary structure, and social incorporation in the workplace. Two-thirds of the women respondents in this study felt discriminated against because of their race/ethnicity at their place of work at some time during their career. An overwhelming proportion (90 percent) of these respondents reported racial bias in positions of power while one-third reported “absolute” or “definite” racial bias in positions of power. Aparna, a second-generation female, agreed with Ameena that “I think that’s across the board, male Caucasian, tall, the demographics of certain people who are more likely to look like [a] professional and be more likely to be hired than the others.”
Lindsay, a white administrator, affirmed that
if you are a black woman or an Indian woman, if you are diminutive, if you are short and slender, you don’t have an imposing physical force, you have the disadvantage of being viewed as someone who would not be in a leadership position and it requires extra effort and artful communication to get people to respect you. It’s a harder job to get them to respect you, to listen to you, do what you say . . . I think it’s harder to get people to cooperate with you.
Lindsay further noted, “It’s not typical, they think, for a woman of color to be in the position of power, that’s not the prototype powerful person in the United States. It’s like I said, a white man in his fifties or sixties.” Second-generation Indian women like Lata also felt that
sometimes achievements are minimized [from Caucasian and African American colleagues, fellow students, fellow students’ parents] because there are so many Indian doctors anyway and of course you are gonna be a doctor . . . there’s almost an anger, like all you Indian people become doctors and kind of take away the spots of everybody else, ’cause you spend all your time studying.
Such sentiments often echo the model minority thesis that is applied to Asian Americans in the United States. Critics argue that the model minority stereotype is not really an indication of increased acceptance of Asians into the U.S. mainstream, but an ideological apparatus to actually create and sustain the racial marginalization of Asians in the U.S. mainstream and brew resentment against Asian achievements (Kibria 1998).
This “Indianness” acts as a barrier in the professional advancements of Indian women. Lata vividly remembered how, during medical school “there was this one professor I remember, this old white guy who was an OBGYN attending . . . one of the things that he specifically said was, ‘You know, you were fine once you got over your natural cultural tendencies of not talking very much and of not being open.’” Rather than being judged on her medical competence, Lata felt that she was judged on racialized and gendered grounds.
Moreover, the stigma of being a foreign medical graduate multiplies the discriminatory experiences of first-generation Indian women physicians in the workplace. Ameena explained that accents lead to differential treatment of foreign medical graduate physicians in the workplace. Foreign graduates like Sheila, a first-generation female, reported having to work harder to gain access into competitive fellowship spots; Sheila was refused a gastroenterology fellowship at an Ivy League U.S. medical university because she was a foreign medical graduate, despite support from the chair of the department. When it came to rank advancement, Nidhi, a first-generation female faculty, felt that it is very hard to get promoted in the workplace “if you are Indian or if you are a foreign graduate.”
Neeraj, a first-generation male faculty, who has sponsored the visas of some first-generation Indian women who were discriminated against in their medical programs yet chose to fight the system, elaborated, “One of the people who were [sic] fired had to leave the country in two weeks. And then they had a provision of hearing, so they put the hearing four weeks later, knowing very well that she is not going to able to attend the hearing . . . that is how their careers are being spoilt.”
In comparing experiences of second-generation versus first-generation physicians, interesting differences as well as similarities were observed (see Table 3). Because of the small sample size, statistical analyses to test for significance were not performed. Second-generation physicians were more likely to perceive discrimination due to their race/ethnicity and gender, and believe that there is gender-based discrimination against women in positions of power. However, a greater proportion of first-generation physicians reported that they had to work harder or prove themselves more at work because of their race/ethnicity. Although all first- and second-generation physicians reported that there is foreign medical graduate bias in the U.S. medical system, first-generation physicians were more likely to feel that it was unjustified, suggesting that second-generation physicians may share some of these biases again foreign medical training.
Comparing Discriminatory Experiences of Second-Generation versus First-Generation Physicians

Discussion and Conclusion
Gender is a fundamental constituent of workplaces, “present in [its] processes, practices, images and ideologies, and distributions of power” (Acker 1992, 567). While feminist scholarship has recognized the gendered nature of workplaces (Acker 1990, 1992, 2006; Britton 2000), it is also important to explore how race and nationality figure into the gendering of workplaces.
My research suggests that many physicians—both women and men—continue to perceive sexist and patriarchal attitudes in American medicine. My women respondents felt that they worked harder to gain the respect of their supervisors and coworkers, while they were also more likely to be steered into less prestigious subfields (Dresler et al. 1996). For example, Raghav, a second-generation male, who is a faculty member in geriatrics, admitted that they “do occasionally hear about older physicians who may have differing expectations of male and female students or may be biased in their evaluations of students and those sorts of things, based on gender.”
Despite the entrenchment of gendered and racialized assumptions and expectations within the practices of these organizations, most research ignores how the gender category is deeply complicated by racial and ethnic differences (Acker 2006). Except for Neeraj, a first-generation man in my sample, who filed and won a racial discrimination lawsuit against an Ivy League U.S. medical school, both the first- and second-generation participants in my sample did not make an active effort to resist discrimination; instead, most were spectators or victims of discrimination. Combating institutionalized discrimination can be mentally taxing and financially draining for individual physicians, as illustrated by Neeraj’s description of the case of a second-generation Indian female physician who won a gender discrimination lawsuit for 1.6 million dollars against a prestigious university hospital in Massachusetts: “After that judge went, they fired her chair and then they [the university] appealed that their [judge’s] judgment is wrong . . . and it is going to go on for a couple of years. And they [the university] have a lot of money. They [lawsuits] cost a lot of money.” Hemant, a second-generation male faculty, aptly summarized the prevalent belief among physicians of Indian origin:
Why would you [complain to the administration if discriminated]? If you were trying to move forward, why would you go and talk to the administration? That would just be counterproductive. You try to work within the system or you leave, go somewhere else, and that’s why some people have left [in his program].
Gendered racism, of course, is not a static phenomenon, but subject to change and transformation. While twenty-first century racial practices in the United States may now be less overt, and more informal (Bonilla-Silva 2000), my research suggests that Indian women physicians continue to face racialized gender discrimination. My findings confirm that, compared to second-generation Indian women physicians, first-generation women who are also foreign medical graduates face particularly troubling racial discrimination by their colleagues, senior faculty, and the medical system at large. Second-generation Indian physicians, who are unaffected by the foreign medical graduate stigma, rigid visa regulations, and accent discrimination, may offer more promise to prospective employers. Yet even this group reports very high levels of gender and racial discrimination, even as they themselves may see discrimination against foreign-trained physicians as justified.
With the health care workforce becoming increasingly dependent on women immigrants from the developing world, more research is needed to understand the interaction of the recent migration of skilled personnel with developing racial/ethnic and gender relations in U.S. workplaces. Such studies will also have policy implications for the flow of professional immigrants between the developing and the developed world. Moreover, given the significant impact gender, race, and nationality can have in molding and restricting the career/migration trajectories of Indian women physicians in the United States, conceptualizations that recognize and inform the impact of discrimination against skilled professionals are imperative.
Footnotes
Authors’ Note:
I extend my gratitude to all the physicians interviewed for this study who took out time from their tight schedules to share their thoughts on this subject with me. Without their generosity of spirit and courage to be forthcoming and honest, this research would not have been accomplished.
Notes
Wasudha Bhatt is a PhD candidate in the department of sociology at the University of Texas at Austin. Her research interests include international migration, gender, and race and ethnicity.