
Abstract
This article examines the regulation of Latina youth sexualities in the context of sexual and reproductive health care provision. In-depth interviews with health care providers working in two Latino-serving community health centers are analyzed for how they interpret and respond to the sexual and reproductive practices of their low-income Latina teen patients. The author finds that providers emphasize teenage pregnancy as a social problem among this population to the exclusion of other dimensions of youth sexualities and encourage Latina girls’ adherence to a life course trajectory that conforms to middle-class, heteronormative ideals as a solution to this problem. By relying on such understandings, providers construct meanings of sexual citizenship that require participation in bourgeois heteronormativity. These findings suggest that Latino-serving community health centers, their providers, and their teen patients could benefit from questioning the assumptions that inform providers’ appraisals of Latina youth and developing a more inclusive approach to Latina youth sexualities beyond a discourse of pregnancy prevention. Such efforts could allow community health centers to actively participate in disrupting the structural inequalities that shape their young patients’ lives.
Latina 1 youth 2 now constitute the largest group of girls of color, at 15.2 percent of the total number of girls under age 18 in the United States (Denner and Guzmán 2006); however, there are surprisingly few studies that critically examine Latina youth sexualities. While significant for sociological understandings of youth, the limited research on this topic emphasizes the school setting or Latina girls’ personal narratives (e.g., Asencio 2002; Bettie 2003; Garcia 2009, 2012; Hurtado 2003). This article, in contrast, focuses on the production of Latina youth sexualities in the context of sexual and reproductive health care provision and expands upon contemporary feminist scholarship on the regulation of young women’s sexualities. In-depth interviews with 15 health care providers working in two Latino-serving community health centers in a mid-Atlantic city in the United States are examined for how providers interpret and respond to the sexual and reproductive practices of their teenage clients. In line with recent queer theorizations of heteronormativity (Brandzel 2005; Ferguson 2004; Garcia 2009; J. Ward 2008), this article explores how dominant discourses of gender, race, class, sexuality, and age intersect in providers’ narratives, and advances the argument that such discourses and practices constitute, following from the work of Judith Butler (1993), a regulatory regime of bourgeois heteronormativity that is productive of sexual citizenship.
Community health centers provide important comprehensive health care services that economically disadvantaged Latina youth (and others) would not otherwise receive. At the same time, these health centers enact a form of heteronormativity that prescribes a middle-class, heterosexual life course trajectory, constructed historically as a white racial formation, as the only pathway to adulthood that is constitutive of full sexual citizenship. These discourses and practices of sexual and reproductive health care provision communicate that nonnormative sexual and reproductive practices among Latina youth must be prevented in order to produce the ideal “girl citizen” who completes her education and is a full participant and consumer in the “new economy,” unencumbered by children and autonomous from the (welfare) state. At the same time, providers occasionally disrupt this regulatory regime of bourgeois heteronormativity in their accounts, suggesting that community health centers are potential sites of intervention in the production of complex inequalities structured through intersections of race, class, gender, sexuality, and age.
Feminist scholars have long focused on health care and medicine as key sites in the regulation of women, particularly in terms of the medicalization of pregnancy and childbirth (e.g., Bridges 2011; Mamo 2007; Martin 1987; Riesmann 1985; Rothman 1989). Less attention has been paid to how young women’s sexualities are regulated—and thus produced—through sexual and reproductive health care provision, but those that do tend to focus on the perspectives of pregnant and parenting young women of color vis-à-vis reproductive health care (Brubaker 2007; Greene 2006) or focus exclusively on family planning clinics (Joffe 1986). Community health centers are particularly fruitful sites of analysis of the regulation of young women’s sexualities because they cast bourgeois heteronormative meanings and practices of sexual citizenship into bold relief and reveal the workings of power in an institutional context typically regarded as benevolent. Community health centers’ discourses and practices of regulation, reflected through providers’ narratives, produce Latina youth sexualities through discourses of deviance and normalization. These seeming contradictions speak to the mix of indifference and trepidation with which the broader U.S. culture regards Latina girls. As other scholars of Latina sexualities have noted, Latina girls are constructed in the U.S. as inherently “at risk” for early pregnancy and motherhood due to poverty, Latino culture, and racialized sexual stereotypes (Garcia 2012; González-López 2010; Hurtado 2003; Zavella 2003). Such hypervisibility leads to an overwhelming emphasis on pregnancy prevention at the expense of other dimensions of sexuality, while at the same time rendering Latina girls as “lost causes.” This social context informs what health care providers and the broader U.S. society consider thinkable about Latina teens and their sexual and reproductive practices.
Intersectionality and the Regulation of Young Women’s Sexualities
Nearly three decades ago, Michelle Fine (1988) argued that young women’s sexualities in the United States are monitored and managed through the promotion of several normative discourses of gender and sexuality that are often co-constituted with discourses of race, class, and age. These include discourses of female sexual victimization and male sexual predation; the privileging of middle-class, procreative, married heterosexuality over other sexualities; the obfuscation of a discourse of adolescent female sexual desire; and a focus on “negative consequences” associated with young women’s engagement in heterosexual sexual activity. These discourses structure what is conceivable about young women’s sexual and reproductive practices, desires, relationships, and identities, and they do little to facilitate the development of young women’s sexual subjectivities (Fields 2008; Fine 1988; Garcia 2012; Tolman 2002, 2005). The concept of sexual subjectivity, which refers to a “person’s experience of herself as a sexual being, who feels entitled to sexual pleasure and sexual safety, who makes active sexual choices, and who has an identity as a sexual being” (Tolman 2002, 2), has been central to feminist interventions in dominant discourses of young women’s sexualities. More recently, scholars have attended explicitly to how power operates through the intersections of gender, race, ethnicity, class, sexuality, disability, and geography to differentially situate young bodies and prescribe restricted forms of sexual expression for young people, limiting their access to knowledge, skills, and safe discussion while encouraging shame, guilt, ignorance, and silence across multiple social fields (Fields 2008; Fine 1988; Fine and McClelland 2006; García 2009, 2012; Harris 2005; Lawson and Rhode 1993; Lesko 2001; Levine 2002; Luker 1996, 2006; Nathanson 1991; Pascoe 2007; Patton 1996; Schalet 2010, 2011; Tolman 2002).
The limited critical work on Latina youth sexualities focuses on the school setting (Bettie 2003; Garcia 2009, 2012; Mendoza-Denton 2008) or teenage pregnancy prevention programs (Erickson 1998), and interrogates the dominant perception of Latina teenagers as girls who make “poor choices and who will likely drop out of school, become a teenage mother, or be the girlfriend of a gang member” (Denner and Guzmán 2006, 1). In her study of school-based sex education, Lorena Garcia (2009) found that educators instruct Latina youth to be “good girls” by abstaining from sex and refraining from displaying knowledge or curiosity about sex in the classroom while simultaneously assuming that Latina girls are culturally predisposed to be “bad girls” (e.g., the pregnant Latina teen or the sexually promiscuous Latina). In documenting how heteronormativity, sexism, and racism operate together, Garcia argues that sex education lessons curtail Latina girls’ access to information about sex, reproduction, and nonheterosexualities, thereby adversely affecting the development of their sexual subjectivities. In a related vein, Pamela Erickson (1998) found that teenage pregnancy prevention programs targeting Latina teenagers are informed by white middle-class ideals about the transition to adulthood and the timing and sequencing of events such as high school graduation, marriage, and first birth, which ignore or discount that, as others have consistently shown, practices of early childbearing are shaped by structural inequalities, limited opportunities, and normative cultural expectations, and, further, are not necessarily detrimental to young women living in high-poverty areas (Edin and Kefalas 2005; Furstenberg 2007; Geronimus 2003; Luker 1996; Nathanson 1991; M.C. Ward 1995). Nonetheless, the interpretation of teenage childbearing as a social and medical problem in need of prevention remains dominant, shaping the perceptions and practices of school-based sex education, family planning programs, and related sites, such as community health centers, where low-income, teenage girls of color are often the focus of such messages.
Sexual and Reproductive Health Care as a Site of Regulation
Among the significant body of feminist scholarship on medicalization cited here, few studies examine the provision of sexual and reproductive health care to young women. One exception is Carole Joffe’s ethnography of family planning clinics in which she finds that “family planning workers play a crucial role in the cultural shaping of sexuality . . . by imparting a certain view of acceptable ways to conduct a sexual life” (Joffe 1986, 4). By regulating female patients’ sexual morality and access to sexual and reproductive knowledge in ways that may be constraining, emancipatory, or a combination of both, Joffe observes that family planning clinics are contested arenas of sexual regulation, which resonates with the analysis provided here, though this study departs from Joffe’s by focusing on community health centers rather than family planning clinics and exclusively examining sexual and reproductive health care provision to Latina teenage girls.
Community health centers serve over 20 million people in more than 7,000 clinic sites nationally and claim to provide culturally and linguistically appropriate care, regardless of a patient’s ability to pay (California HealthCare Foundation 2012). Community health centers typically receive government funds as well as private foundation grants and individual donations to provide health care services, including sexual and reproductive health care services through Title X of the Public Health Service Act of 1970, the nation’s only family planning program. Importantly, community health centers are not typically understood as “state agents”; rather, they are seen as charitable organizations that are part of the “voluntary sector,” which is increasingly responsible for the provision of social welfare in light of the rapidly shrinking U.S. welfare state (Duggan 2003; Wolch 1990). Because of their contractual relationship with the state in the implementation of public policy, it is plausible to conceptualize community health centers as doing the work of the state and thus as ancillary “state agents.”
This article foregrounds the perceptions and practices of health care providers working in community health centers and examines how such organizations and those who work for them are central to the state’s regulation of low-income Latina youth’s sexualities. The analysis herein is not intended to judge individual providers but, rather, locates their views and actions in the institutional contexts that make their work both possible and circumscribed. Guiding questions include the following: How do health care providers working in community health centers make sense of the sexual and reproductive practices of the Latina youth they serve? How might these perceptions inform their practices of sexual and reproductive health care provision? How are dominant meanings of race, class, gender, sexuality, and age articulated or subverted in providers’ narratives? How might providers’ perceptions and practices in their narratives of sexual and reproductive health care provision be theorized through the lens of sexual citizenship, as part of an effort to intervene in the (re)production of complex inequalities and reimagine what is thinkable about Latina youth sexualities?
Data and Methods
This article is based on a larger study of the regulation of youth sexualities in the United States conducted between 2006 and 2009. The study included discourse analysis of public policy formation, ethnographic fieldwork, and in-depth interviews with health care providers (Mann 2010). This research focused on how the state and community health centers that contract with the state to implement public policy make sense of young people’s sexualities and seek to shape their sexual and reproductive practices in accordance with prevailing social norms. I recruited health care providers through administrators at two Latino-serving community health centers and presented the research as a study of adolescent health care provision. The organizations are located in the same neighborhood in a mid-Atlantic city that, during the 1980s and 1990s, experienced an influx of Latino immigrants. More recently, some Latino residents have been displaced to working-class suburbs as a result of gentrification processes, but often still travel to the organizations to receive services. Over the past 30 years, the clinics have grown significantly to serve many thousands of people each year, both achieving the status of “federally qualified health center,” which allows them to receive Medicaid reimbursements. Each clinic is staffed by fully bilingual (Spanish/English) providers and administrators, operates within a model of cultural competency, has a majority low-income, Latino clientele, and provides low-to-no-cost comprehensive health care services. These community health centers are particularly vital for Latino immigrants who would otherwise not have access to health care because they lack insurance coverage through paid employment or government programs, or because other area health clinics do not guarantee language accessibility and related dimensions of culturally competent care.
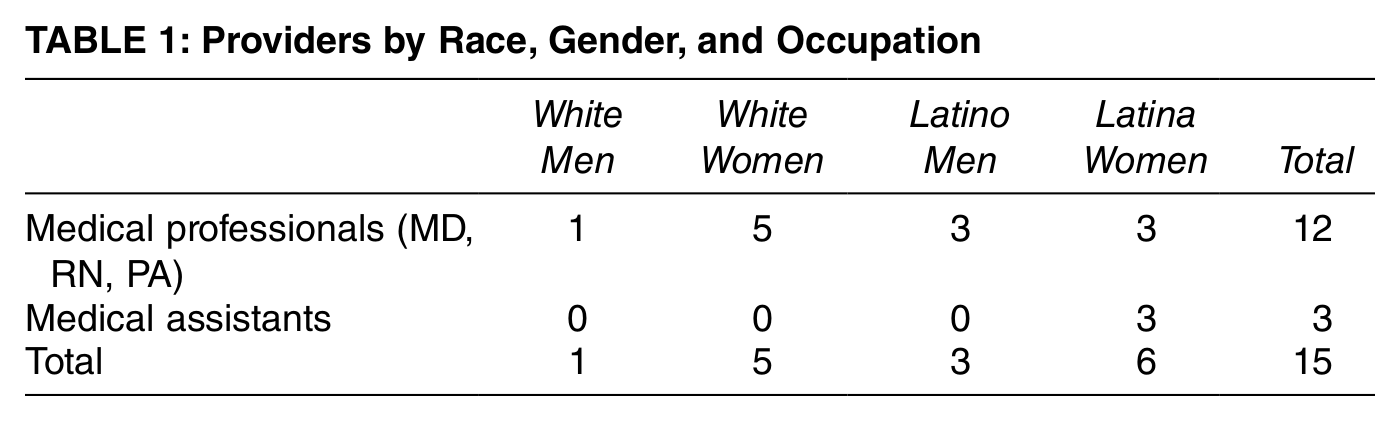
In order to ensure the confidentiality of the interview participants and the anonymity of the organizations for which they work, I do not identify the organizations or providers by name or provide other potentially revealing details. Further, I treat the interviews with health care providers from both organizations as part of a single case study of Latino-serving community health centers because they serve a similar client population, are geographically proximate to each other, engage in collaborative work, and contract with the state to implement Title X, the nation’s only federally funded family planning program. My sample includes 15 health care providers (6 white and 9 Latina/o) and represents a range of health care occupations (see Table 1). I conducted one interview with each provider and, with two exceptions, all interviews occurred in private rooms at the organizations. Interviews lasted approximately 60 minutes, were recorded, and followed a semi-structured interview guide during which I asked providers about their views of the needs and concerns of their Latina teen patients in terms of sexual and reproductive health and how they addressed these needs and concerns during patient visits. I examine how providers talked about their perceptions of Latina youth, focusing on their sexual and reproductive practices, and how they narrate their practices of health care provision in relation to these perceptions.
Providers by Race, Gender, and Occupation
Each interview was transcribed and analyzed using Atlas.ti, a qualitative data analysis software program. Using critical discourse analysis, I drew on insights of feminist, queer, and intersectionality theories to interpret and examine how providers deployed discourses of race, class, gender, sexuality, and age in their narratives of sexual and reproductive health care provision. Discourse here refers to “language in use,” including word choice, arguments, claims, and motives (Clarke 2005, 148). Discourses are both representatives of “reality” and the process by which reality is produced, as well as bodies of knowledge constituting sets of practices through which power/knowledge operates (Clarke 2005, 149). Because discourses are social practices that constitute the conventional meaning structures of social life and thus “social structure” itself, they are important sites of analysis (Jaworski and Coupland 1999). By focusing not only on who produces the discourse but also which social group(s) or social world(s) they are about, critical discourse analysis uncovers politically and ideologically salient features that are constitutive of power relations, which are often unknown or at least unacknowledged by those producing the discourse.
Findings
My findings reveal three interrelated patterns in health care providers’ perceptions and practices vis-à-vis the Latina youth they serve: (1) Latina teenage pregnancy was constructed as an inherent problem in need of prevention; (2) Latina girls’ ambivalence or intentionality about pregnancy was treated with confusion and disdain; and (3) relationships between Latina teen girls and Latino adult men were seen as a central cause of the problem of early pregnancy. In these narratives, providers privileged an “age-appropriate” model of middle-class, procreative, married heterosexuality over other sexualities and intimate relationship configurations. By positioning their Latina teen patients’ sexual and reproductive practices as deviant and problematic, providers implicitly questioned girls’ capacity to be sexual citizens who engage in “good girl” behavior by managing their sexualities, delaying motherhood, engaging in full-time paid work, and participating in consumer capitalism (Harris 2004). At the same time, providers demonstrated empathy for Latina teen patients who depart from the bourgeois heteronormative script by attributing their sexual and reproductive practices as outside their control—because of their youth, poverty, Latino culture, and predatory older men. Such expressions of empathy can be seen as attempts to normalize Latina youth’s perceived deviance while concomitantly encouraging Latina youth to modify their own behavior in order to adhere to this script.
Constructing Latina Teen Pregnancy as a Problem
In their responses to how they viewed the needs and concerns of their Latina teen patients, most providers highlighted teenage pregnancy, doing so in ways that reinforced the dominant perception that teenage pregnancy is a social problem that is particularly prevalent among low-income Latina youth. Providers addressed this issue by recounting the various ways in which they sought to encourage pregnancy prevention among their Latina teen patients. Besides yearly checkups for school, many girls came into the community health centers for, in the words of one white woman provider, “family planning and either to get the pills or get condoms or to get education about it.” Another white woman provider agreed, lamenting that it’s “usually after the fact, but they come.” Among girls who asked for contraception, providers often noted that girls wanted something that could not be easily detected by parents, other family members, or boyfriends. One Latina provider explained, “Well, the majority [of girls] like to go on the Depo [the shot] because then they don’t have to take a pill in front of their parents, and, you know, their parents won’t have to know.”
This approach to birth control made sense to providers because it enabled the girls they serve to accomplish two goals: (1) prevent pregnancy without depending on the cooperation of their male partners, and (2) conceal their sexual activity from their families. Providers generally viewed both goals as normative, although some lamented what they viewed as a lack of communication between Latino parents and their sexually active teen daughters. None of the providers commented on the apparent lack of male partners’ involvement in preventing early pregnancy, highlighting only situations in which male partners appeared to encourage it. Providers perceived Latina girls who adopted this strategy toward contraception positively because they were taking personal responsibility to prevent pregnancy, regardless of what the important people in their lives thought about adolescent sexual activity, contraceptive use, and/or early pregnancy and parenthood.
This appraisal reflects a bourgeois heteronormative script that includes an emphasis on women’s personal responsibility to engage in family planning by delaying childbearing until the completion of education, entry into marriage, and achievement of financial independence (or dependence on a breadwinning husband). The emphasis in this discursive regime is on Latina girls making “good choices.” Such choices are not value-neutral nor are they inherently “true”; they are sanctioned both by dominant U.S. culture and the providers in this study and reflect white, middle-class values about the relationships among the normatively gendered individual, the family, the market, and the state. As Arline Geronimus notes, the public “damning” of early childbearing in the United States, particularly in urban, low-income black and Latino communities, ignores the fact that while delaying childbearing is generally beneficial to white, middle-class women, that is not necessarily the case for socioeconomically disadvantaged women of color who lack the same opportunity structures (Geronimus 2003, 82). Furthermore, intense opposition to early childbearing can perpetuate white middle-class Americans’ cultural dominance and concomitant social inequalities (Geronimus 2003).
Interpreting Latina Girls’ Pregnancy Intentions: Discourses of Class and Culture
Providers’ efforts to prevent pregnancy among their Latina teenage patients often involved accounts of struggles to convince girls to use any kind of birth control at all, indicating a disconnect between providers’ views about pregnancy prevention and girls’ apparent ambivalence or intentionality about pregnancy. One white woman provider lamented that, despite what she saw as extensive effort on her part, some of her teen patients became pregnant because they weren’t using any method of birth control. When asked why she thought this was, she asserted, “They just don’t want [the birth control] to be found . . . there are just so many.” Absent in the provider’s interpretation are alternative explanations for why some girls aren’t using birth control. One of these interpretations was offered by a different white woman provider, who asserted, “I think most of them decide . . . a lot of them want to be pregnant.” Another provider, the only white man in the sample, echoed this observation, narrating an account of how a typical visit goes between him and a Latina teen patient:
Maybe you ought to think about using birth control . . . so you don’t have a kid. Finish school, get a job, then have the kid. You don’t want one now. Although we have people come in and ask me—they want a baby, they’re surprised they’re not pregnant. So it’s more . . . talking about, you know, taking the approach of . . . if you are, or if you have multiple partners you do increase your chance, using protection, but trying to prevent pregnancy [rather] than preventing sex. If they haven’t started [having sex] . . . then sort of joking, you’re too young anyway.
The assumption that Latina youth who become pregnant do so intentionally is reflected in many of the white providers’ narratives as well as the social science literature (Frost and Driscoll 2006). Notably, some providers responded to such intentions with explicit discouragement, as evidenced in the previous quote, where the provider tells the hypothetical Latina teen patient, “You don’t want [a baby] now.” Further, the provider encourages the girl to engage in a heteronormative life course trajectory that is informed by a bourgeois ideology—first school, then work, then a child. Notably, marriage as part of this sequence is not mentioned, perhaps reflecting that marriage is no longer seen as the “master event” that determines sexual activity, adult work life, and the transition to parenthood that it once was (Brandzel 2005; Coontz 2005; Edin and Kefalas 2005).
Like the white male provider quoted earlier, other providers recounted cases of Latina girls who wanted to know if they were able to become pregnant. For example, one white woman provider claimed in an incredulous tone that it was not unusual for a girl to say during a primary care visit, “I think I’m infertile, my boyfriend and I have been having sex and I’m not pregnant yet.” Similarly, a Latina provider noted, “Even my niece, she come here and she born here and she got pregnant, because she just want to know if she can get pregnant. And I told her, ‘That is stupid. Why you want to get pregnant when you have your whole life to?’” These providers made it clear they think becoming pregnant in order to confirm one’s fertility is foolish, and did not explore why some Latina teen patients might be concerned about their ability to become mothers. For example, cultural norms associated with the valorization of motherhood may lead some young Latinas to fret about their capacity to meet the cultural expectation that they become mothers even if they do not intend to become mothers during adolescence (Arreola 2010; Erickson 1998).
Providers also framed their observations and explanations about pregnancy intentions in terms of poverty and culture, although how they did so varied by racial/ethnic identity, with white providers focusing on social class and Latina/o providers focusing on culture. For example, the one white male provider compared his low-income Latina teen patients to their more affluent and (implicitly) white counterparts:
That’s more common, I would say [among my patients], as opposed to if you went to the average private high school in [an affluent, predominantly white suburb], you wouldn’t see girls trying to get pregnant. I mean, there’s a lot of similarities; there’s still a lot of sexual activity, that’s similar, there’s a lot of drugs, and they’re still using a lot of drugs, they still have the same issues about identity, development, social adaptation, sexuality, just looks.
This provider observed that there are distinct class differences in pregnancy intentions between the teenage girls he sees at the community health center and those at “the average private high school.” He was careful, however, to avoid any explicit mention of race while also softening his class analysis with claims about age-related sameness among teenage girls, regardless of other social differences. Further, he implicitly drew on a racialized comparative frame that positions Latina girls as deficient when compared to white girls in their choices about the timing of pregnancy and parenthood. This narrative implies that it’s possible that white providers harbored racialized explanations for their observations about Latina teen pregnancy but were reluctant to disclose them because of the dominance of colorblind racial discourse, which dictates that any talk of race renders the speaker “racist” (Bonilla-Silva 2006). Instead, as evident in the quotes presented here, white providers relied on a discourse of class to explain the perceived phenomenon of intentional pregnancy among low-income Latina girls.
While white providers avoided invoking explicit discourses of race, Latina/o health care providers were far more likely to explain their observations about early pregnancy among Latina teen patients using a discourse of culture while also claiming a Latino identity to bolster their interpretations. In one representative example, a Latino provider noted:
I am Latino, so in some ways I can . . . say that I know some traits of the Latino culture. I know that we tend to be very . . . uhm . . . shy or, I don’t know, another word would be better than that—but we don’t like to talk about sexual health. Most of the Latino parents, especially the ones that were born in their own countries, like El Salvador or Mexico, chances are they’re not going to be very forthcoming in terms of talking to the kids about reproductive health. They’re not going to be talking about problems, they’re not going to be talking about [birth control] pills or anything like that. In fact, they would probably prefer for [their daughters] not to use any . . . or not to have that information in the hopes that they won’t have sex.
This view, which attributes the prevalence of early pregnancy among Latina teens to cultural norms about sex and reproduction in Latino families, is also widely represented in the public health literature (Arévalo and Amaro 2010; Arreola 2010; Erickson 1998; Romo, Nadeem, and Kouyoumdjian 2010). However, some studies contest the assumption that Latina/o parents and their children do not communicate openly about sex (Guzmán, Arruda, and Feria 2006), and others have challenged the assumption that such patterns fully explain the incidence of pregnancy among Latina youth (Garcia 2012). The Latino provider quoted here further elaborated on his observation by stating that the most important way that the community health center could counteract what he viewed as a problematic patterned cultural practice was to provide Latina/o teenagers with medically accurate information about pregnancy and sexually transmitted infections. In other words, he asserted that, since research shows that open parent–child communication about sex can lead girls to either delay the onset of sexual activity or to be more likely to use birth control if sexually active, and Latina/o parents weren’t communicating with their kids about sex, the community health center should take on this role so as to prevent early pregnancy among Latina youth.
Separating the Men from the Girls: Age Differences in Heterosexual Relationships
Accounts of significant age differences between Latina teen girls and their male partners emerged as another noteworthy pattern in providers’ narratives. In these cases, a discourse of female victimization and male predation emerged, with providers attributing blame for teenage pregnancies to older male partners’ manipulations while expressing concern about the well-being of the girls in such relationships. In a representative observation, one white woman provider stated:
This is a classic upfront: “I came in to have a physical exam ’cause my boyfriend wants me to have a baby.” And the boyfriend’s 24, and she’s 15, and she’s, like, the youngest 15 you’ve ever seen. She’s, like, 12 going on 12. . . . [A]nd it’s more like “What do YOU want from your life, what do you want to do?”
This narrative, which was more prevalent in interviews with white providers than with Latina/o providers, is one that is produced through the federal policy-making process, particularly on welfare reform (Cocca 2002; Erickson 1998; Smith 2007), and is also reflected in liberal feminist discourses of teen pregnancy prevention (Luker 1996, 2006). The Latina teen girl in this account can be understood as an archetype, or a composite that is representative of a pattern the provider observes among the girls who come to the community health center for services. At the same time, this archetype can also be understood as a “threatening specter” whose status as an abject subject is constituted through repudiation (Butler 1993, 3; see also Pascoe 2007). The Latina teen girl is constructed as an abject subject through the convergence of discourses of gender, race, class, sexuality, and age. The provider is concerned that the girl has adopted the desire of her male partner as her own, and thus she perceives the girl’s desire to have a child as inauthentic. For the provider, the desire to have a child at the age of 15 could not possibly be authentic because that is not what girls (are supposed to, according to the bourgeois heteronormative script) want for their future; therefore, it must be the older boyfriend’s influence. Further, her desire is also not perceived as authentic because of her age, thereby drawing on a dominant discourse of age to suggest that a teenage girl can’t possibly know what she really wants because of her youth. That these discourses appear to be in conflict—a girl should know what she wants but can’t possibly know what she wants yet—obscures their compatibility. The provider is repudiating the girl in two ways: first, for adopting her boyfriend’s desire as her own, and second, for failing to adhere to a middle-class life course strategy in terms of the timing of sex, marriage, and reproduction in relation to educational attainment and economic self-sufficiency. It is a repudiation that accommodates a conservative discourse that promotes “abstinence until marriage” and a liberal, feminist discourse that promotes the prevention of “negative consequences” of teens’ sexual activity (Fields 2008; Luker 2006). While these may seem to make for strange discursive bedfellows, they work together to produce Latina youth sexualities through a regulatory regime of bourgeois heteronormativity.
While many providers explicitly invoked such normative discourses of gender and age, the absence of a substantive understanding of both Latina girls’ agency and complex inequalities was also noteworthy. For the most part, providers presumed that their Latina teen patients who wanted to become pregnant did so because they wanted to please their boyfriends and because they didn’t know any better. This interpretation relies on racialized gender stereotypes about Latina teen girls, such as the assumption that sexually active Latina girls are prone to early pregnancy because of passivity, ignorance, and sexual irresponsibility (Garcia 2012). Further, these discourses indicate a lack of attention to how Latina girls’ diverse sexual and reproductive practices, which in some cases diverge from culturally dominant ideals in the United States, are shaped by complex power relations (Fields 2008). As Julie Bettie (2003) demonstrates in her ethnography of white and Mexican American high school senior girls, while most older teenage girls across class and race are sexually active, unlike middle-class girls, working-class girls by and large do not have college and careers to look forward to; for them, “motherhood and the responsibility that comes with it can be employed to gain respect, marking adult status” (Bettie 2003, 69). Thus, for some economically disadvantaged young women, there is no convincing reason to postpone parenthood since structural inequalities limit their opportunities regardless of when they have children (Edin and Kefalas 2005; Furstenberg 2007; Geronimus 2003). Nonetheless, motherhood as a route to adulthood in adolescence runs counter to middle-class sensibilities about the heteronormative life course. The response to the assertion of such desires is prevention, which was evident in many of the narratives offered by providers in this study.
In one account, a Latina provider reflected Bettie’s (2003) observations by offering a more structural analysis of why she sees “kids coming in at 15 that say I want to have a baby,” thereby intervening in some of the more individual-level explanations encountered in other interviews:
That’s all they see that they can do in their life, you know, for whatever reason. And so that tells us that teen pregnancy prevention has to begin at pre-K. Where you don’t talk about getting pregnant, but you talk about opportunities, hopes, dreams. A lot of our kids don’t, can’t—because of their reality and because of how they’ve grown up and how their parents have grown up—don’t think beyond the day. Food on the table at night. It’s just the way it is. And so for you to say, “Okay, let’s talk about you going to college for four years,” I mean, that’s just, like, an impossible thing. Which is why when we talk a lot to our kids, it’s like, you can go to school and work part time. Because then that makes a little more sense. The idea of just going off to college and not working is, like, who’re you talking to, you know? So we do it in a way where even if you just take one course, you know, and it takes six years instead of four years, then you’re going to have your degree.
While this provider acknowledges that inequalities structure the opportunities available to the young Latinas to whom she provides health care services, her response to this structural constraint is to focus on a positive, promoting achievement in the domains of work and school, rather than a negative, teen pregnancy prevention. This narrative is noteworthy because it acknowledges how social structure impacts her patients’ lives. At the same time, the response to these circumstances is to communicate the message that Latina girls, while constrained, can still fulfill normative expectations in terms of educational attainment and economic self-sufficiency, provided they delay childbearing. In a social context in which many low-income Latina teens’ opportunities and outcomes are structured through complex inequalities, this well-intentioned message indicates the difficulty providers have in looking beyond early pregnancy prevention as a necessary dimension of ameliorating such inequalities.
Producing Sexual Citizens through a Regulatory Regime of Bourgeois Heteronormativity
In their discourses and practices of sexual and reproductive health care provision, providers foregrounded early pregnancy and childbearing among some Latina teen patients as a social problem in need of intervention. Providers drew heavily on discourses of bourgeois heteronormativity to produce Latina youth sexualities as, in the words of Roderick Ferguson (2004), a nonheteronormative racial formation. By repeatedly framing Latina girls’ sexual and reproductive practices as nonnormative, problematic, and in need of prevention, providers produced a regulatory regime of heteronormativity in which the assertion of gender, sexual, and age-specific norms intersected with dominant racial and class ideologies, rendering bourgeois heteronormative ideals universal while constructing young minoritized subjects as outside the bounds of sexual citizenship.
Sexual citizenship has primarily been theorized as a collection of sexual rights and responsibilities that are bestowed or denied though laws and policies or, more broadly, as the processes by which participation in normative heterosexuality secures access to citizenship in terms of belonging, respect, and recognition within a national community (Bell and Binnie 2000; Evans 1993; Richardson 2000). Not only is sexual citizenship constructed as heterosexual through laws and policies, rendering nonheterosexualities outside its boundaries, it is also contingent on participation in “age appropriate” monogamous relationships and, more specifically, procreative monogamous marriage (Brandzel 2005). A heteronormative construction of sexual citizenship works to marginalize and exclude myriad groups of people by virtue of their social location in power relations of race, class, gender, and sexuality because it “promotes the norm of social life as not only heterosexual but also married, monogamous, white and upper-middle class,” positioning those who embody this ideal as synonymous with “Americans” (Brandzel 2005, 190; see also Somerville 2005). Thus, sexual citizenship is not accessible simply on the basis of heterosexuality because not all heterosexualities are regarded equally (Richardson 2000), particularly when they do not adhere to the white bourgeois heteronormative script.
While U.S. public policy on youth sexualities, including abstinence education and family planning, do provide normalizing lessons in sexual citizenship for young people (Fields and Hirschman 2007; Mann 2010), there are other power relations at work in the regulation of Latina youth sexualities described here. Writing against Fine’s (1988) original thesis that a discourse of adolescent female sexual desire is missing from sex education and other sites of sexual regulation, Anita Harris (2005) argues that a discourse of young women’s sexual desire has, in fact, emerged in recent years, albeit linked to consumerism and participation in the new economy. Harris claims that this discourse of desire has regulatory effects because it is linked to ensuring young women’s availability as flexible labor in the “new economy.” Since the 1990s, this discourse has produced young women as new kinds of citizens that heretofore were not understood as such—as unencumbered workers and consumers. Harris refers to this ideal young woman as the “can do” girl who devotes herself to full-time paid work and performs normative femininity through the display of a consumer lifestyle (Harris 2004, 21). An intrinsic element of a girl’s “can do” experience is delaying motherhood until her thirties or forties and only then having one or two children. While Harris locates this discourse in relationship to disciplining the bodies and desires of economically privileged young women, she notes their regulation necessarily exists in relationship to the discourse of the “at risk” girl, who is constructed as a “failure” and “vulnerable by [her] circumstances,” which involve being marginalized by intersections of race, class, and gender (Harris 2004, 25). This is the only lens through which “at risk” girls are seen, informing what is even thinkable about them, their desires, and their life course. Further, when “at risk” girls are linked to teenage motherhood, they are seen as wasteful—a drain on social resources and a destroyer of their own and future generations (Harris 2004, 30). The vilification and punishment of teenage motherhood in public discourse serve to recruit young women to “good girl” behavior while encouraging them to distance themselves from “bad girls.” This helps justify the shrinking of the U.S. welfare state and the curtailing of the social rights of citizenship while simultaneously emphasizing young women’s individual responsibility to the nation to make every effort to conform to the ideal “can do” girl citizen, regardless of their circumstances.
The construction of girls’ “good citizenship” in relation to carefully monitored sexuality, delayed motherhood, full-time paid work, and participation in consumer capitalism and, by contrast, the “bad citizenship” of girls who do not assimilate to this ideal is apparent in the discourses and practices of the health care providers at the center of my analysis. While providers’ narratives about their Latina teen patients cast prevailing bourgeois heteronormative meanings and practices of sexual citizenship into bold relief, they also reveal how power operates in well-meaning institutional contexts. As such, providers’ narratives produce Latina youth sexualities in ways that circumscribe Latina girls’ access to sexual citizenship through providers’ seemingly failed attempts at normalization. The apparent ambivalence toward contraception among some girls and intentional pregnancy among others were constituted in the eyes of providers as problems that can be solved only by the girls themselves. As Harris notes, these prescriptions “may well be out of step with the reality of young women’s lives and the possibilities that exist for them to actually enact [sexual] citizenship” as it is currently constructed (Harris 2004, 71). Thus, sexual citizenship—for youth in general and Latina youth in particular—is structured in a limited fashion not around sexual and reproductive rights but, rather, sexual and reproductive responsibilities, privileging conformity to the bourgeois heteronormative script at the expense of alternative understandings. The notion that Latina girls could have the capacity for legitimate agency in terms of their sexual and reproductive practices appeared to be unimaginable among the providers in this study.
Conclusion
This analysis has several implications for theories of heteronormativity, intersectionality, and sexual citizenship and for practices of sexual and reproductive health care provision to low-income Latina youth. First, by exploring bourgeois heteronormativity as a regulatory regime structured through intersections of dominant discourses of race, class, gender, sexuality, and age, this article demonstrates the utility of integrating feminist theories of intersectionality with queer theory. This contribution is in line with more recent calls to queer intersectionality theory and to demonstrate the relationship between intersectionality and processes of normalization in specific institutional contexts and in relation to state power (Ward 2008). Second, by using sexual citizenship as a heuristic device through which to make sense of the productive power of bourgeois heteronormativity, the exclusion of young people marginalized at the intersections of race, class, and gender from full membership in the national community becomes newly visible and calls into question providers’ attempts to shape their Latina teen patients’ sexual and reproductive practices in accordance with norms that reflect contemporary relations of ruling. Thus, the understanding of sexual citizenship advanced here through attention to intersectional structural inequalities expands upon previous theoretical analyses by focusing on the sexual regulation of Latina girls, who are so often constructed as inherently “at risk” and as a threat to the nation (see Chavez 2008).
Although the health care providers interviewed for this study did not engage in interpretations or practices that appeared to facilitate the development of what could be conceptualized as full, democratic sexual citizenship for Latina youth, the findings presented nonetheless suggest that community health centers have the potential to become spaces that foster young people’s sexual subjectivities by adopting a social justice approach to health care provision, particularly with respect to sexual agency and reproductive justice. As Garcia notes in her study of sexually active Latina girls, “Young women are afforded very little space to explore and experience sexuality in ways that are empowering to them and, especially, that privilege their sense of desire and pleasure” (Garcia 2012, 150). At the same time, the feminist “empowerment paradigm” so often applied to young women needs to critically engage how racism, sexism, classism, and heteronormativity work together to marginalize those whose perceived or actual sexual and reproductive practices diverge from normative prescriptions (see Schalet 2009). By reimagining what is thinkable about Latina youth sexualities in light of the theoretical and empirical insights offered here, community health centers and the providers who work in them could realize the social justice efforts they purport to pursue in the context of providing allegedly “culturally sensitive” care. In order to encourage the adoption of such a paradigm shift, however, more research is needed, not only with health care providers but also with Latina youth themselves. By situating sexual and reproductive health care provision in terms of the structural contexts that both Latina youth and health care providers navigate, questioning the cultural deficit model that informs providers’ negative appraisals of Latina teenagers’ sexual and reproductive practices, and developing a more inclusive understanding of and approach to youth sexualities beyond a discourse of pregnancy prevention, community health centers could more actively participate in disrupting the complex structural inequalities that shape their young patients’ lives.
Footnotes
Author’s Note
The author would like to thank Laura Mamo, Meyer Kestnbaum, Sonja Mackenzie, Patrick Grzanka, Anthony Hatch, Michelle Corbin, Leticia Marquez-Magana, the three anonymous reviewers, and Joya Misra for their thoughtful and thorough comments on earlier drafts of this article. This research was supported in part by the Dr. James W. Longest Memorial Award of the Graduate School of the University of Maryland, College Park.
Notes
Emily S. Mann is a visiting assistant professor of sociology at the University of Nevada, Las Vegas. Her research interests include gender, sexuality, race/ethnicity, reproduction, and youth.