
Abstract
Catholicism is the most restrictive world religion in its position on assisted reproductive technologies (ARTs). The opposition of the Church, combined with the widespread acceptability of ARTs in the United States, creates a profound moral dilemma for those who adhere to Church doctrine. Drawing on interviews from 33 Catholic women, this study shows that devout women have different understandings of these technologies than women from treatment-based studies. These differences are rooted in devout women’s position of navigating two contradictory cultural schemas—“religious” and “secular”—regarding the meaning of reproductive technologies. Religious schemas provide devout women with different cultural resources that help them to avoid using ARTs while still reckoning with the ideal of biological parenthood. I show how devout women draw on religion to find value and meaning in their suffering, move beyond biological motherhood, and achieve a moral femininity. While religion increases the burden of reproduction for devout women, it also provides the cultural resources to resist the financial, emotional, and physical difficulties experienced by women who use ARTs.
Sexuality, gender, and reproduction are sites in which what is “natural” and “morally acceptable” are perpetually contested. Advances in assisted reproductive technologies (ARTs) such as in vitro fertilization (IVF) pose a challenge to the idea of “natural” procreation. For some, this challenge has been largely overcome. While ARTs were not widely accepted 30 years ago, they have become part of the normal means by which life can be created (Becker 2000). Their use has doubled in the last decade, underscoring the importance of biological 1 motherhood (Becker 2000; Centers for Disease Control and Prevention 2012). Studies on the experience of infertility show that one’s identity as a woman is often defined by the ability to have a biological child (e.g., Becker 2000; Greil, Slauson-Blevins, and McQuillan 2010; Ireland 1993; Ridgeway and Correll 2004), which is “reified as the gold standard of motherhood” (Martin 2010, 540). This results in a “cataclysmic role failure” for women who desire but are unable to have children (Greil, Leitko, and Porter 1988, 191). Women with access to ARTs thus often feel compelled to use them (Sandelowski 1991). But some are still unable to bear a child, because they may not have access to ARTs (Bell 2009), the treatments may fail (Becker 2000; Throsby 2002), or they may not pursue ARTs at all. These women must then work to “redefine normalcy” (Becker 2000) via other forms of parenthood or by expressing other forms of “normative femininity” when childless (Throsby 2002).
Missing from the literature on infertility in the United States is any consideration of how religion shapes the process of negotiating infertility and gender. Yet religion is replete with beliefs and teachings about reproduction, gender, and sexuality. For many, religion matters and plays a potentially critical, unexplored role in how women navigate messages about infertility and gender. Importantly, religious women negotiate not only wider cultural messages about gender, infertility, and ARTs but also their religion’s positions on these issues. The Catholic Church provides an especially critical case for examination because it venerates motherhood and family but is the most restrictive world religion in its position on ARTs, creating potential moral dilemmas for those who adhere to Church doctrine. Devout women are members of a pronatalist society that supports the use of ARTs, but they are also members of a religion that emphasizes motherhood while restricting the technological means for achieving it. How do these women reconcile being outsiders who do not meet the expectations of their religious and secular communities?
Given the importance of religious considerations in determining the moral acceptability of ARTs, it is surprising that neither sociologists of religion nor medical sociologists have addressed how this potential site of conflict between two institutions of authority—medicine and religion—may affect women’s experiences of infertility. Numerous studies have examined the medicalized experience of infertility (Becker 2000; Franklin 1997; Greil 1991; Greil, Slauson-Blevins, and McQuillan 2010; Modell 1989; Sandelowski 1993; Thompson 2005), but these studies primarily examine people after they have already decided to pursue treatments and thus fail to capture the experiences of those who refuse treatments. Thompson describes the only person who left treatment (for nonfinancial, nonmedical reasons) as having the “unusual commodity” of religion (Thompson 2005, 94).
Medical anthropologists have written extensively on religion and ARTs, but these studies are primarily limited to non-Western contexts. We know little about how religious people experience ARTs in the United States—a country with uniquely high levels of religiosity and a thriving IVF industry. The United States is thus a fruitful site for examining the intersection of religion and medicine—institutions that both have distinct views on how life can legitimately be created. This study asks: Given the widespread acceptability of infertility treatments forbidden by the Catholic Church, what strategies do devout women use to negotiate their religious beliefs and their desire for a child? How does religion shape their efforts to make sense of ARTs, infertility, and gender identity?
The study highlights devout women’s distinctive understandings of ARTs and experiences of infertility. In comparison with the women in most treatment-based studies, I argue that devout women occupy a unique position of navigating two sometimes contradictory cultural schemas (Sewell 1992) regarding the meaning of ARTs in the United States. Drawing on both religious and secular schemas, devout women’s experiences of infertility are both medicalized as a biomedical problem (Greil 1991) and infused with religious meaning. Religion allows devout women to refuse technologies, but it also allows them to rework their sense of what it means to be a Catholic woman who is unable to have a biological child—a process I describe as achieving a moral femininity. Devout women attain this by embracing suffering as meaningful and constructing alternative maternal identities. Their rejection of ARTs becomes a testament of their devotion to God that results in a deepened piety. They become “moral guardians” working to protect the natural social order as ordained by God. Thus, while religion increases the burden of reproduction for devout women, it also provides the cultural resources to resist the financial, emotional, and physical difficulties experienced by women who use ARTs.
The Catholic Church and Assisted Reproductive Technologies
The Catholic Church’s opposition to ARTs is articulated in the instruction Donum Vitae (Respect for Human Life in Its Origin and on the Dignity of Procreation). First, marriage is a sacrament—a ritual signifying God’s presence—and procreation within marriage is a sacred act in which couples co-create with God (Congregation for the Doctrine of the Faith 1987). Children are considered a gift from God created when the corporeal and spiritual unite during intercourse. In the laboratory, the divine nature of procreation is ruptured, as scientists supplant God as the creators of life. In contrast to embryo formation within the womb, the laboratory environment is not considered respectful to human dignity or divine intention (United States Conference of Catholic Bishops 2009).
The Church is not entirely opposed to science and technology. Artificial insemination is not prohibited as long as it does not replace the conjugal act. The Church permits the use of a perforated condom to collect semen during intercourse that can later be used for insemination. In addition, NaPro (Natural Procreative Technology), developed by a Catholic doctor, is a Church-sanctioned infertility treatment that teaches women to monitor their cervical mucus and track fertility. Surgical procedures such as laparoscopic diagnostic techniques, hormonal therapies, and medications are also permitted to address imbalances.
Unlike Judaism and Islam, Catholicism does not privilege biogenetic kinship (Inhorn 2003; Kahn 2000), and thus infertility is not a legitimate reason for divorce. Biological reproduction remains the cultural ideal, but it is not mandated and alternatives such as adoption are valued.
Religious Schemas and Reproductive Dilemmas
I build on Sewell’s (1992) “schemas” in order to understand how devout women develop understandings of ARTs distinct from those of women in previous treatment-based studies. I categorize schemas as “religious” and “secular” for analytical purposes, but acknowledge they can overlap, complement, or contradict each other. Religious schemas are understood as interpretive frameworks that shape how people experience and act in the social world (Ogland and Bartkowski 2014). Sociologists of religion have used schemas to understand how religion influences people’s views on sociopolitical issues, moral judgments, and behaviors (e.g., Bartkowski et al. 2012; Hoffman and Bartkowski 2008; Ogland and Bartkowski 2014). But studies of religious people’s attitudes reveal little about how beliefs are put into practice by people actually experiencing moral dilemmas, or how the salience of schemas may vary throughout the course of these dilemmas. In this study, I show how devout women use religious schemas to reason through dilemmas that extend beyond a discrete moment in time.
We also lack research examining how gender shapes the process of moral reasoning. Decisions about using reproductive technologies are shaped by gendered ideologies that link womanhood to the ability to bear children, and reproductive technologies that are particularly invasive toward women’s bodies. This study expands our understanding of the role of religious schemas by moving beyond attitudinal and behavioral measures and incorporating gender not simply as a variable but as actually shaping the process of moral reasoning. I show how devout women navigate secular and religious schemas that inform their understanding of what it means to be a woman, their infertility, and their relationship with God.
To understand how religion shapes one’s experience with infertility, I draw on studies of religion and gender, literature on the experience of infertility, and studies on religion and ARTs.
Religion and Gender
Sociological studies of religion and gender challenge stereotypes of religious women as “doormats” (Stacey and Gerard 1990) by showing how women strategically use religion to find solace from the contemporary demands of modernity, empower themselves through reinterpreting doctrine, and navigate their workplace and family life (e.g., Chong 2008; Davidman 1991; Gallagher 2003; Griffith 1997). Avishai cautions, however, that efforts to highlight religious women’s agency still often fail to recognize “religiosity for the sake of religiosity” as agentic (Avishai 2008, 429). Building on Mahmood’s (2005) concept of “pious agency”—cultivating a pious self through religious practice—Avishai develops the “doing religion” framework to understand religious conduct as a “mode of being, a performance of religious identity” where agency is expressed as compliance toward religious ends (2008, 410).
This approach challenges Western secular-liberal conceptualizations of agency rooted in the rational, self-interested, autonomous liberal subject, either unmoored from or actively resisting institutionalized authority (Avishai 2008; Mahmood 2005). Yet many religious people simultaneously share these Western, liberal desires for autonomy and individualism while also seeking self-transcendence and a relationship with God. These sometimes contradictory desires must be reconciled, and people synthesize religious and secular schemas in meaningful ways that make distinguishing religious from extrareligious ends difficult. In this study, I extend our understanding of religion and gender by examining how devout women navigate religious and secular schemas to construct their identity as devout women experiencing infertility in the United States.
Medicalized Experiences of Infertility
Most studies of infertility in the United States capture the experiences of those already pursuing treatments (Becker 2000; Franklin 1997; Greil 1991; Modell 1989; Sandelowski 1993; Thompson 2005). These studies describe ARTs as having a “pulling” effect on infertile women that “compels” their use, even when unsuccessful, given the highly valued possibility of a biological child (Franklin 1997; Greil 1991; Sandelowski 1991). Women who can afford treatments feel compelled to use them, and experience shame for not “trying” if they do not (Sandelowski 1991, 32).
A few of these treatment-based studies (Greil 1991; Sandelowski 1993) reference religion. Sandelowski found that religion was most meaningful for less advantaged women who were less treatment-oriented and believed conception was “in God’s hands” (1993). Greil (1991) found that people in his study were unable to draw on religion in meaningful ways to make sense of their infertility. Thompson’s (2005) ethnography of infertility clinics is one U.S.-based study that noted the dilemmas religious people face with ARTs. She describes the rare refusal of infertility treatments by a Mormon woman, and an Orthodox Christian couple who invited a priest to the clinic to discuss how IVF could be carried out in accordance with religious teachings. These important but limited glimpses into religious people’s experiences with ARTs point to a gap in our understanding and highlight the need for more focused research.
Religion and ARTs
Depictions of religion and science as conflicting have been challenged by scholars examining their intersection in the practices of assisted reproduction around the globe (e.g., Bharadwaj 2006; Inhorn 2006; Inhorn and Birenbaum-Carmeli 2008; Kahn 2000; Paxson 2004; Roberts 2012; Teman 2010; Thompson 2005). In Israel, religion and science work together to fulfill pronatalist policies. With Rabbinical laws that accommodate the use of ARTs and government-sponsored IVF treatments, Israelis are the highest per capita users of IVF (Inhorn and Birenbaum-Carmeli 2008; Kahn 2000). Roberts (2012) shows how IVF in Ecuador is not only accepted by Catholics but that religion is invoked as a form of assistance in “God’s laboratories.” Likewise, Inhorn’s work in the Muslim Middle East shows how religious prohibitions raise concerns about being a “good Muslim” when considering ARTs (Inhorn 1994, 2003). Paxson (2004) shows that despite the Greek Orthodox Church’s religious prohibitions, women “naturalize” IVF by transforming their suffering into expressions of atonement. These studies reveal that religion and science interact with each other and other systems of meaning and belonging in everyday life. This study builds on these analyses in order to understand how religion, gender, and science intersect in the experiences of devout Catholics in the United States.
Methods
To understand how Catholic women experience infertility and ARTs, I conducted in-depth, semistructured interviews with 33 Catholic women 2 who experienced infertility. I recruited participants who responded to flyers posted at fertility clinics, cafes, Catholic Social Services, and grocery stores; and online via Craigslist, infertility blogs, and forums. I limited recruitment to Catholic, infertile women ages 18–50 3 who had considered infertility treatments. One non-Catholic woman who was married to a Catholic man asked to participate and was included.
Thirty-two of the respondents were U.S citizens from across the country. One interviewee was from Latin America. The median age of interviewees was 33. Thirty of the respondents identified as Caucasian, one as African American, and two as Hispanic. Twenty-eight women were employed and five were stay-at-home mothers. The sample is predominantly middle- to upper-class, white, college-educated women from the United States. Apart from the three nonwhite respondents the demographic profile of my sample is similar to that of clinical samples from prior research (Chandra and Stephen 2010). In this study, I focus on the majority of the sample that is devout (n = 20). Any comparison between devout and nondevout women is limited because nondevout women experienced infertility for a significantly shorter time (median = 2 years) than devout women (median = 5 years). When appropriate, however, I include experiences of the nondevout women as a point of comparison.
Sociologists of religion agree that religiosity is multidimensional and complex. Commonly used measures of religiosity are beliefs, salience, and practice (Pearce, Foster, and Hardie 2013). In this study, I used three measures of religiosity that reflect one’s commitment to the Church and the strength of one’s Catholic identity (D’Antonio et al. 2001): frequency of Church attendance; frequency of confession, 4 which is the sacrament of reconciliation; and response to an open-ended question on the importance of religion in one’s life. Comparing women in the sample using these measures resulted in two groups that I describe as devout and nondevout. Women were classified as devout if they attended Church at least once a week, confessed at least once a year, and used words such as “very” or “extremely” to describe the importance of religion in their lives. All but one devout woman reported that they attend confession at least once a year; this woman self-identified as devout in a follow-up questionnaire. Women who were classified as nondevout either never attended mass, attended on holidays, or attended monthly. Only one nondevout woman participated in confession, but she attended mass only monthly and described religion as “somewhat important.” One nondevout woman identified religion as “very important” to her, but also described herself as “not strongly religious.” She attended church monthly and did not participate in confession. Nondevout women typically described themselves as “not very religious,” “casual,” “moderate,” or “nonpracticing” Catholics.
To further verify my classification, I sent a follow-up questionnaire to participants to allow them to self-identify as devout Catholics or not. I asked, “Would you consider yourself to be a devout Catholic?” and provided room for an open-ended response. Twenty-three people responded to the follow-up, with all confirming my classification except one subject, whose classification I adjusted accordingly.
I conducted 30 of the 33 one- to two-hour interviews by telephone. I asked participants about their family backgrounds and the importance of religion in their lives, their experience with infertility, marriage, interactions with doctors, and their thoughts on ARTs. After each interview, I asked participants to complete a short demographic questionnaire.
All interviews were transcribed verbatim. I read the transcripts and identified major themes: artificial/natural, marginalized experience, children as gifts, God’s plan, suffering, reconciling strategies, and Catholic identity. Within these themes, I used ATLAS.ti software to create codes. I used both open and focused coding (Emerson, Fretz, and Shaw 1995). The coding process was iterative, as I used the data to develop initial ideas in combination with initial “hunches” I formed during the interview. These ideas were written and developed in memos.
At the end of the interviews, I was often asked if I was Catholic and infertile. I responded that I am a nonpracticing Catholic who grew up in a Roman Catholic family and that I have not tried to conceive. I was also sometimes asked what I was “looking to prove.” When I explained that I was looking to understand their experience, many seemed relieved. They expressed concern about being portrayed in a negative light, with some even saying, “I’m really not stupid” when describing their reluctance to use ARTs. Other than within their online community, devout women often felt misunderstood and utterly alone and were delighted that someone wanted to hear their story.
The research process was sometimes perplexing, and my experience of it is difficult to articulate. These women have political and religious beliefs different from my own. But their openness quickly dispelled any anxiety on my part about being a “different kind of woman,” and I even found myself questioning and reconsidering some of my own beliefs. In Contested Lives, Ginsburg puts my own experience into words: “Doing research . . . often felt schizophrenic. . . . Like internal tectonics, the layers of my own thought and unexamined beliefs began to shift and collide and take new shape in relation to the people I was struggling to understand” (Ginsburg 1998, xxxiv). This experience assisted in understanding these women and the common struggles and contradictions we experience in our daily lives that transcend religious and political affiliations. These women are negotiating their life “disruptions” within the constraints of their particular situation. I hope I can relay their stories as meaningfully as they related them to me.
Devout Women’s Narratives of Infertility
Women in this study and prior studies on infertility share a strong desire for children and a confidence in scientific progress and medical technologies. Both groups of women typically begin their infertility journeys by seeking medical solutions. But when the next line of treatment involves technologies that the Church forbids, devout women’s treatment trajectories become distinct. I show how devout women draw on religious schemas in order to avoid the use of ARTs, while also achieving a moral femininity not rooted in biological motherhood. First, I show that the Church’s veneration of motherhood and its silence regarding infertility amplifies the suffering of those who are without children. Those who refuse ARTs feel isolated from the broader society in which their use has become normalized, even expected. Second, I show how devout women draw on religious teachings about procreation to construct some reproductive technologies as artificial and others as natural. Third, religious schemas provide a means to critique the commodification of reproduction by understanding children as a gift from God, as opposed to a right. Fourth, by attributing their infertility to a “greater plan,” devout women are able to move beyond a strictly biological understanding of infertility and find meaning in their suffering. Finally, they draw on religion to construct alternative maternal identities not defined by biological motherhood.
“All Mothers Must Be Important”
Prior research shows that those who are more religious are less accepting of childlessness and have stronger beliefs regarding the importance of motherhood (Greil et al. 2010). The Church plays an important role in how Catholic women think about motherhood. One devout woman explained, “[Motherhood] is a very important part of life, of femininity, of a marriage. Of actually being a co-creator with God . . . I see it as a very natural part of Catholicism.” Another woman described the Virgin Mary as an exalted model of motherhood: “If the Blessed Mother is important, then all mothers must be important.” Because the Church is family-centered and infertility is rarely acknowledged by their local priests, most women felt like outsiders at Mass. Some felt judged for not having children, as one devout woman described: “People wonder, ‘Are they not really good Catholics? Are they on contraception?’” Women opposed to ARTs must also contend with broader society’s embrace of these technologies, as one woman explained:
You’re living in a society that not only does what you can’t do, but thinks it’s a huge blessing and medical advance and a procedure given to us by God. . . . So you have to deal with that on top of everything. . . . You can’t just go to generic support groups; you can’t go to a generic blog online. . . . You realize, “I’m totally alone . . . everybody else I know can do IVF.”
Devout women are thus in a double bind. They face pressures from society and their religious community to have children, but they feel judged by their Church community and isolated from secular society for refusing ARTs.
“Playing God”: Differentiating the Natural and Artificial
Prior studies on infertility show that women pursuing ARTs struggle with their inability to conceive “naturally” (Becker 2000; Franklin 1997; Greil 1991; Inhorn 2003; Sandelowski 1993; Teman 2010; Thompson 2005). Some naturalize elements of ARTs to achieve desired kin relations and identities—an approach Thompson (2005) terms “strategic naturalization.” I show how devout women construct ARTs as artificial and “strategically naturalize” medical treatments that are compatible with Catholic doctrine. Marilyn, a devout, 34-year-old writer living in a Boston suburb who suffered from primary infertility for four years, described IVF by contrasting it with “natural” procreation:
I just feel like IVF demeans a person so much, because the conception happens not in the throes of love, but rather in a scientific laboratory and it just sounds so disgusting to me . . . they’re not embracing each other, and they’re not participating in this great procreative act.
For Marilyn, IVF eliminates the sanctity of intercourse within the marital union. According to the Church’s instruction of Donum Vitae, this threatens not only “natural” reproduction but also the moral foundation of society (Congregation for the Doctrine of the Faith 1987).
Though opposed to ARTs, devout women do pursue medical treatments that they “strategically naturalize” as facilitating procreation within marital intercourse (Thompson 2005). NaPro, a technology that purports to monitor and maintain a woman’s reproductive and gynecological health, for example, provides a morally acceptable alternative because procreation remains within the bounds of marital intercourse. Margaret, a 30-year-old manager suffering from primary infertility for a year, explained why she prefers NaPro:
I left the reproductive endocrinologist, and that’s one thing I liked about the NaPro doctor. He would never perform any artificial reproductive procedures. He focused on diagnostics and helping me fix the problem from a hormonal and medical kind of way.
Margaret naturalized NaPro by contrasting its “medical” treatment with the reproductive endocrinologist’s “artificial” procedures. Devout women view NaPro as preparing the spousal bodies for procreation through intercourse. One woman explained, “They must make your body so healthy that the result of sex is a baby.” Biomedical and religious frameworks converge and provide a way for devout women to “fuse their modern bodies with their Catholic souls” (Hirsch 2008, 95).
The boundaries between the natural and the artificial are complicated by the fact that while the Church explicitly opposes most ARTs, its position on intrauterine inseminations (IUIs) is undefined. Nonetheless, all but two devout women chose not to use IUIs. Kayla, a 35-year-old banker from New England, suffered from primary infertility for one year. She described an IUI as almost “natural” if using a Church-approved perforated condom to collect semen during intercourse, but even she ultimately decided against the method:
I think the Church is undecided. So I was telling myself that [IUI] would probably be as far as we’d go because we weren’t harming any life. It was not quite natural, but if he used a condom with a hole in it for collection and we had sex, it would still be the act, and you would never really know. So I kind of worked my way around that, but in the end we canceled the appointment. We just weren’t comfortable with it.
But Kayla also expressed doubts about her decision: “After I’ve seen ten women that go on to have IVF and now they have babies, I think, am I making a huge mistake?” Her desire for a child and the cultural acceptance of ARTs by other women contributed to her moral uncertainty.
Audrey, a 40-year-old manager suffering from primary infertility for 12 years, described engaging in “private negotiations” with God (Hirsch 2008). She knelt down to pray before her insemination and held a concealed rosary during the procedure. She explains that an IUI is not “playing God” because it is just moving the sperm “closer.” By having sex postprocedure, it is unclear if the artificially inseminated semen or the semen from intercourse will reach the egg. Conception is still in God’s hands, as Audrey explained: “[IUI is] not really anti-Church. It’s taking his sperm and putting it closer to my egg. You were told to go home and have sex. So was it the sex? Which sperm cell is it?” Audrey’s reasoning resonates with that found in other studies outside the United States on religion and ARTs that similarly emphasize God’s role in the technology’s outcome (Bharadwaj 2006; Inhorn 2003; Paxson 2004; Roberts 2012).
Nondevout women in this study naturalize IVF in ways that are similar to clinic-based samples from prior studies. Christine, who described herself as “not religious,” suffered from premature ovarian failure for one year. She understood IVF as assisting nature: “Basically, [IVF is] just like additional help, right? I would do it. I think we’re very fortunate to have that ability to do that. I wouldn’t even think twice about that.”
Both nondevout and devout women expressed uncertainty about or objected to the use of donor semen and eggs. While devout women framed their objections as “playing God,” some nondevout women described the use of donor egg or sperm as “weird” or “strange.” Adopting an embryo or traditional adoption were considered better alternatives. Christine, who had no misgivings about IVF, was opposed to using an egg donor. But it was her only option, as she described:
I don’t want someone else’s egg. I feel really weird about it and uncomfortable. I don’t like the idea at all. . . . People do what they have to do. I’m one of them. I’m considering something that I would have never ever considered. We do these crazy things so that we can be mothers.
Both devout and nondevout women described feeling it would be unfair—even akin to adultery—to use donor eggs or sperm. They wanted the embryo to be completely genetically related to the couple or not at all. One nondevout couple decided to use their respective siblings as donors so that their child would be genetically related to each spouse. They “strategically naturalized” their siblings’ donor gametes so that each spouse could establish an “equitable” genetic affinity to the child.
Nondevout women were less concerned with the Church’s teaching that procreation must occur within marital intercourse, though they did express concerns about the moral status of the embryo. In response to critiques of “playing God,” nondevout women often cited their good intentions when using IVF. Celeste, an editor from a Midwestern city who was undergoing IVF for male-factor infertility, reflected:
I truly don’t want to be “playing God.” . . . I feel that we’re trying to do things out of love. . . . I really don’t want to destroy life, and I do believe that clearly is life. . . . Not to boil this down to something odd. But it’s like endangered species. . . . Sometimes people have to do things to procreate that maybe weren’t the way it was supposed to happen.
Like many nondevout women, Celeste characterized undergoing IVF as an expression of love for her husband. Nondevout women undergoing IVF also naturalized embryo disposition, as one woman described: “These embryos weren’t killed; they just happened to die, and a lot of embryos die in nature too.” Others limited the number of eggs they would fertilize in order to prevent dilemmas over embryo disposition. Leah, a nondevout scientist who grew up in a devout family, drew on science to reason through embryo disposition: “I think the biologist side of me that thinks they’re just cells—I’m not completely convinced they’re just cells—but they’re not that different from my skin cells.” She uses a scientific framework that is salient in her everyday life to reason through a moral gray area.
The U.S. IVF industry thrives on cultural ideologies of individualism, persistence, and technological progress (Becker 2000). The pursuit of reproductive technologies has become an imperative for many middle-class women (Sandelowski 1991). The ARTs industry has been critiqued by some for commodifying women’s bodies and reproduction, 5 but patients resist such commodification by engaging in objectification and medicalization of their bodies in strategic ways (Becker 2000; Greil 2002; Teman 2010; Thompson 2005). Thompson describes this as “agency through objectification,” wherein technology becomes a tool for patients to achieve their identity as parents (2005, 183).
Devout women critique IVF by defining a child as a gift from God rather than a right. They describe the ART industry as a business that commodifies (future) babies, to which people then feel entitled. Carmela, a devout 34-year-old lawyer from Houston who has primary infertility and has pursued adoption, reflected: “A child is a gift. It is not a given. Because you want a child doesn’t mean that you have to have it, and that you have to do everything to get it and break all of the laws of God and society to do it.” Some secular parents also describe their children as “gifts,” to be sure, but devout women draw a distinction between a divine gift and the right to a child. The concern is that when procreation is delinked from marital intercourse, people are dehumanized in the process and become products in an economic market that focuses on profit and self-interest 6 (Lauritzen 1993). Kayla, like many devout women, perceived her doctor as taking advantage of vulnerable women in order to increase profits: “You tell them that it’s your religion, that this is your moral decision, and they don’t respect it . . . the way I can describe it is like a used car salesman selling me a car when I don’t even need one.”
In their opposition to ARTs, devout women critique the commodification of reproduction, which they believe threatens the sanctity of life. They become guardians of the moral foundation of society, as they understand it. Their beliefs, decisions, and actions produce moral selves by preserving the “natural” mode of reproduction based on Catholic doctrine.
Like women in treatment-based studies, nondevout women described IVF as an undesirable but necessary way to have children. They did not voice strong objections to the industry. Ashley, an executive from Nashville who had an unsuccessful IUI after suffering from primary infertility for a year, explained: “Because we have the technology, the outcome is not something that’s wrong. I honestly don’t think God cares how we get our child. We have the technology and he gave someone the gift to come up with this technology.” For many nondevout women, the technology is described as “God-given” and assisting nature (Modell 1989). Another nondevout woman described having a right to a child: “I just feel like everyone should have their right to have a child or children.” Her statement resonates with prior research in which women described having a right to a family and an obligation to use ARTs to achieve it (Becker 2000; Modell 1989; Sandelowski 1991).
God’s Plan: Suffering for a Greater Purpose
Early in their infertility narratives, devout women have confidence in medical treatments and draw on secular schemas regarding biomedical technologies as successful. Like women in prior studies, devout women described wanting to control every aspect of their infertility. They traveled to consult with doctors, read medical journals, and timed, measured, and tested their own bodies. But when IVF was the only option left, they surrendered their control to God. This transition illustrates how biomedical and religious schemas become salient at different moments. It also shows that religious women can value Western, liberal ideals of autonomy while also accepting limitations on their choices and actions. Anna described her transition:
I’ve always achieved anything I wanted to. . . . And that can give you an ego and make you think that you’re doing all this, and that God really isn’t part of the equation. . . . Now, with this cross, I’ve been humbled to the point where I step back and say, “I understand that I’m not in control of this.”
This shift was also poignantly captured by Audrey:
Earlier it was, “I wish God would let me know what his plan is for me.” Then it was my life is like a tapestry, how one side has the pretty picture and the other side is all ugly with the threads showing. All I can see are the threads. He can see the beautiful parts.
These were common narratives in devout women’s accounts. By eventually locating their infertility within a cosmological order, devout women challenged a strictly biomedical understanding of infertility.
This conceptualization of God’s plan also allowed women to expand their maternal desires beyond biological motherhood. Framed as part of a divine plan, devout women could naturalize their adopted child as meant to be. Rina, a 30-year-old stay-at-home mom who struggled with primary infertility for 12 years, reflected:
We looked at it as there’s a reason, there’s a purpose . . . now that we have our daughter, a friend said, “Thank God you never were able to get pregnant.” She, for me, is . . . that’s the reason that I was waiting for, because I can’t imagine not having her. I wouldn’t trade ten pregnancies for her.
Leah, a nondevout woman and scientist who underwent several cycles of IVF, also questioned the reasons for enduring treatments and why she hasn’t been able to adopt. She explained that a biological child is symbolic of her love for her husband:
We’ll either have a baby or we won’t and then we’ll adopt—it’s simple, right? [laughs] . . . But you’ve spent all of this effort. . . . There must be a reason they’re doing that, right? . . . It’s because I love my husband very much. He has these wonderful qualities, and I want to be able to give him a child.
Leah also struggled to make sense of her infertility, but its meaning does not extend beyond the material world. While devout women’s refusal of ARTs is a testament to their religious devotion, nondevout women’s use of ARTs is often described as a testament of love for their spouse.
Devout women draw on religious texts that provide a language of morality and redemptive suffering to make sense of their infertility. They find solace in biblical stories of infertility, which helps them understand Catholic women’s “vocation to suffering” (Orsi 1998, 87). Georgia, a devout woman, suffered from primary infertility for six years and eventually adopted a child, whom she now views as a miracle. She reflected:
I’m not just blindly following these rules. I do believe in them. . . . Our faith teaches us that Jesus died on the cross, and we are called to carry our crosses. I read a lot about suffering. Almost all of the greatest saints have had the worst things happen in their lives in these very dark times. It taught me that suffering has value in our lives.
Georgia has used religious writings about suffering to realize the value of her own difficult experience. Another devout woman described how infertility was the perfect cross for God to have chosen for her:
What greater suffering can a woman who has always wanted to be a mother have than not being able to have children? So it was the perfect thing for God to have chosen because it allows us to suffer so greatly that we can redeem ourselves. If I had been paralyzed in a car accident, I would suffer greatly. But to me, that wouldn’t to me be as great a suffering as not being able to have children.
Devout women come to understand their infertility as not just a disruption, but as a coherent part of God’s plan 7 for them.
Such religious schemas are not apparent in nondevout women’s accounts or those in prior research. Greil writes, “According to the medical model, suffering is not something to be understood but rather something to be conquered” (Greil 1991, 173). Traditional theodicies were not meaningful for the people in his study. In contrast, devout women in this study not only found their suffering meaningful but also critiqued the notion that all suffering should be avoided. One devout woman argued:
In the modern world everybody is always trying to relieve suffering. Like, you’re suffering from being fat? Try the stomach pill. You can’t see? Do LASIK surgery. I’m not denying that I’m very grateful for modern science, but at the same time, some suffering is meant to be, and it helps you grow as a person.
For some nondevout women, however, religion actually contributed to their suffering. Celeste was undergoing IVF due to male-factor infertility. She described feeling judged by Catholics for undergoing IVF:
Rather than comfort there is judgment and isolation. There is not enough support within the Church for people, and waiting for an unpredictable adoption after we’d been through so much heartache simply seemed cruel. . . . IVF was the shortest way to achieving the family we always dreamed of having.
Religious schemas were thus most meaningful for those who described themselves as more religious. Trusting God’s plan and drawing on women’s vocation to suffering helped devout women transition from desiring only biological motherhood to realizing other forms of maternal identity.
Moral Femininity
Becker (2000) shows that when IVF fails, women must redefine normalcy and rework their gender identities. Devout women refuse ARTs and redefine normalcy by drawing on religious schemas such as Catholicism’s openness to adoption, marriage without children as still meaningful, and a lack of emphasis on biogenetic lineage. These schemas allow them to expand their expressions of maternal identities beyond biological motherhood.
In their infertility narratives, devout women describe achieving a strengthened Catholic identity and an expanded understanding of their gendered identities. I call this coconstruction of their religious and gendered identity a moral femininity, in which infertility and the refusal of ARTs become a combined source of value and self-worth—an expression of Catholic womanhood that brings them closer to God. In using the term moral, I am neither imposing an assessment of one’s morality nor essentializing femininity as “moral.” Rather, I use the term to point to the women’s sense of their own morality. They reflect on their infertility as a journey toward salvation, through which Church teachings enable them to save their marriages, financial security, and bodies from the effects of fertility treatment. One woman explained, “One couple I knew broke up because of infertility . . . we had boundaries that allowed us to focus on each other as opposed to throwing our lives into [ARTs].” Devout women expanded their gendered repertoires by drawing on religion to construct alternative maternal identities when unable to have biological children.
Nine out of 20 devout women in this study eventually adopted or were in the process of adopting (Table 1). But giving up on biological parenthood was a painful process. One devout woman, who suffered from primary infertility for five years, explained, “I had to mourn the loss of my biological child. . . . For the longest time I just couldn’t fathom doing adoption; I almost would rather be childless.” Another woman stated, “Before it was more important to be biological. That was something I had to let go of . . . it’s not that important to be pregnant and give birth. 8 It is important to be a mother. I would be a mother somehow, some way.” Other women noted difficulties even after adopting, as one woman shared, “Maybe you’re fertile in other ways, but that grief is still there. It’s not as painful, but it’s still there.” Even for those who drew on religious schemas, overcoming their desire for a biological child was not always possible. Audrey, one of two devout women who chose an IUI, explained, “I just felt in my heart that I wasn’t ready for [adoption]. I hadn’t exhausted all options. . . . I had to exhaust everything before I felt in my heart that I could do that.” Such statements reveal the powerful idealization of biological parenthood and resonate with women’s experiences from prior studies (Becker 2000; Modell 1989; Sandelowski 1991).
Demographic, Fertility, and ARTs Information
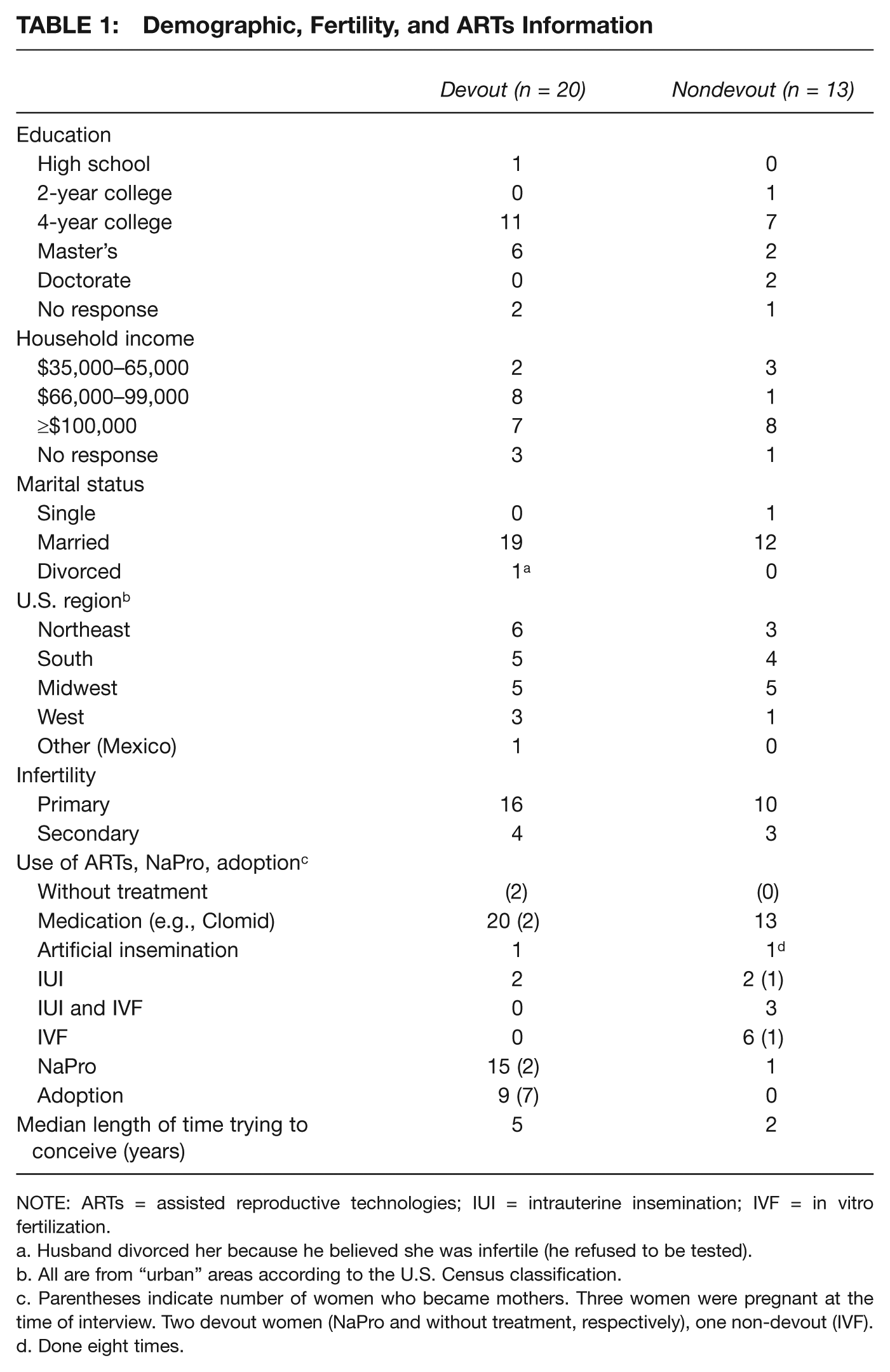
NOTE: ARTs = assisted reproductive technologies; IUI = intrauterine insemination; IVF = in vitro fertilization.
Husband divorced her because he believed she was infertile (he refused to be tested).
All are from “urban” areas according to the U.S. Census classification.
Parentheses indicate number of women who became mothers. Three women were pregnant at the time of interview. Two devout women (NaPro and without treatment, respectively), one non-devout (IVF).
Done eight times.
While the nondevout women in this study were earlier in their infertility journeys, none adopted or were in the adoption process; 12 of 13 had used ARTs (Table 1). Some wanted to try for a biological child first; one woman explained, “We’re open to adoption, but we wanted our own child. We wanted to try to get a biological child.” For some, the experience of pregnancy was most important, while others described the biological connection as being particularly important to their husbands. While nondevout women may eventually adopt, it is possible that the Church’s support of adoption as a religious calling facilitates this transition for devout women.
Devout women were able to construct maternal identities around other forms of parenting, nurturing, and caring. Women drew on Biblical stories of infertility that emphasized women’s value aside from biological motherhood, as one woman explained:
There are women who suffered through infertility in the Bible, and that is a source of comfort: Hannah, Elizabeth, saints, or even nuns that give up their fertility because they have been called for something greater. It makes you feel like your life is still worthwhile even if you are not able to have a biological baby.
Carmela, who had a miscarriage and eventually adopted, challenged a strictly medical understanding of her infertility:
I don’t consider myself infertile in either sense. Neither in the physical sense because I have a baby in heaven that I’m not able to hold, but I was a mother . . . because infertile means you don’t give fruits, and I think I give fruits in many other ways.
These expanded expressions of fertility and motherhood helped devout women repair their gender identities, untethering their femininity and their status as mothers from biology.
Devout women also constructed alternative maternal identities as protectors of life. Elaina, who adopted, explained, “It’s not that the Church is against everything. Actually, we’re promoting life by helping women have their babies, by saving babies of abortion, by saving babies from IVF. It’s very coherent.” Kristine, a 30-year-old scientist from Houston, suffered from primary infertility for six years and eventually adopted a foster child. She described reconceptualizing her own maternal identity: “The key word there is I can be a mother without being pregnant. . . . There are all kinds of kids who need help. I’m always a big advocate. I will always say I’m pro-life. Foster care, NaPro—I’m going to promote it.
Two women became NaPro practitioners in order to teach other couples; they specifically hoped to help others avoid IVF and birth control (to regulate cycles), both of which are understood as threatening the sanctity of life and marriage. As NaPro practitioners and advocates, the women see themselves as guardians of a natural social order promoting procreation according to Church doctrine.
Devout women are also able to achieve a sense of self-worth and value by focusing on what they see as a righteous path. Elaina explains:
Being Catholic has made my life more difficult. On the other hand, it is an amazing source of value. . . . I’m valued because I value life. Very Catholic people know that we’re choosing life by not doing IVF. . . . In that sense, the Church has given me a tremendous source of support.
As “moral guardians of life,” devout women seek to preserve their souls and a divinely informed social order (Congregation for the Doctrine of the Faith 1987). While infertility marks them as potential outsiders in the Church community, their opposition to ARTs and their “bearing of the heavy cross” of infertility transforms them into exemplars of Catholic femininity instead. Women noted, in particular, the recognition of this status within the online community of Catholic infertile women—a place where their suffering, beliefs, and faith were understood.
Conclusion
In both their religious communities and in their social relationships outside of them, devout women contend with cultural interpretations of gender that conflate fertility and femininity. Devout women also experience a disjuncture between cultural expectations for them to use ARTs and a Church doctrine that forbids them to do so. Yet, despite religious traditions often compounding the larger societal pressure for women to be mothers (Greil et al. 2010), devout women value the limitations placed by the Church on the use of ARTs. In many ways, the religious restrictions provide a sense of meaning and stability as women grapple with profound uncertainty. This is not to say that devout women do not still struggle with aspects of their experiences. But they draw on religious schemas to construct moral boundaries around licit and illicit reproductive practices, to come to terms with the failure of medical treatments, and to reconceptualize themselves as feminine women and mothers in ways that transcend biological fertility. In doing so, they are able to recover a sense of womanhood that others experiencing infertility often feel they have lost (Ireland 1993). By “bearing the heavy cross of infertility,” devout women achieve a moral femininity as virtuous women who endure suffering for God’s larger plan.
This study bridges and contributes to three literatures that are rarely in conversation. First, it answers the call to shift the marginalized study of gender and religion to a topic of serious sociological inquiry (Avishai, Jafar, and Rinaldo 2015). In the subfield of the sociology of religion, studies have used the concept of religious schemas primarily to understand how they influence religious people’s attitudes, behaviors, and moral reasoning (e.g., Bartkowski et al. 2012; Hoffman and Bartkowski 2008; Ogland and Bartkowski 2014). But these studies do not examine how religious schemas influence people experiencing actual moral dilemmas. This study thus moves beyond attitudinal and behavioral measures to show how schemas are put into practice. Furthermore, past studies that use gender as a variable obscure how gender itself shapes the process of moral reasoning. Women in this study navigate religious and secular schemas regarding motherhood and womanhood that inform their reproductive desires, dilemmas, and decisions. The effect of religious schemas on shaping their gendered understanding of themselves—from feeling inadequate to becoming exemplars of Catholic femininity—evolves over time.
Second, this study contributes to sociological literature on gender and religion and ongoing debates regarding religious women’s agency (Burke 2012). One group of studies understands agency as the instrumental use of religion toward extrareligious ends. Subsequent studies challenge this approach by including compliance toward religious ends as a form of agency. In keeping with the latter, I show that devout women can value Western, liberal notions of autonomy and individualism while also valuing religious restrictions and surrendering control in pursuit of self-transcendence. They are able to reconcile these sometimes competing ideas by innovatively synthesizing religious and secular schemas into a coherent narrative that makes their suffering and their relinquishing of control meaningful. Prior studies describe women as pursuing either religious or extrareligious ends, but this obscures the ways that religion is intertwined with aspects of one’s life outside of formal religious practice. For the women in this study, their stance against ARTs is not an instrumental use of religion for extrareligious ends; it is understood as a religious act in itself.
Third, this study extends the literature on the experience of infertility and the scholarship on gender, religion, and ARTs. Prior studies on infertility are based primarily on clinical samples and show that it is a cultural imperative for middle-class couples struggling with infertility to use ARTs (Sandelowski 1991). Religion does not appear to be meaningful for most couples in these studies (Greil 1991; Sandelowski 1991); this is likely because those who are most conflicted about ARTs never make it to the clinic, or leave (Greil et al. 2010; Thompson 2005). This study thus captures a group being overlooked by current research, and reveals that for some people experiencing infertility, religion matters profoundly. Though they still desire to be mothers and are confident in medical technology, devout women are not “compelled” to use ARTs (Sandelowski 1991). In their own medical treatment, they limit their embrace of technology once it impinges on procreation within the sanctity of marital intercourse. Prior studies show that couples “strategically naturalize” ARTs (Thompson 2005); devout women also engage in these strategies but draw their boundaries differently. They ultimately embrace their suffering as meaningful—a response not captured in the existing literature. Indeed, neither biomedicine nor U.S. culture at large accord much attention to suffering, other than attempts to eliminate it (Greil 1991). Religion allows Catholic women not only to say “no” to technologies promising a much desired outcome, it also expands their gendered repertoires to include alternative maternal identities. By delinking motherhood and fertility from strictly biological definitions, devout women reconstruct their identities as women, even though the conflation of fertility and femininity remains.
Ultimately, religion is a multilayered and dynamic part of these women’s lives. It contributes to the pain of infertility in various ways, but also offers cultural resources that help devout women construct meaningful, alternative maternal identities. Like their secular counterparts, devout women display admirable strength in facing the pain of infertility, but their religious beliefs enable them to locate their experiences within a larger cosmological order where God—not the individual—determines one’s destiny. This relinquishing of control is, itself, a meaningful form of agency.
Footnotes
Acknowledgements
I am grateful to Renee Anspach, Danielle Bessett, Natalja Czarnecki, Kim Greenwell, Robert Jansen, Mushfeq Khan, Karin Martin, Alexandra Murphy, Rachel Rinaldo, Elizabeth Roberts, and Geneviève Zubrzycki for their very helpful feedback. This article has benefited from participants in the Graduate Writing seminar; the Medical Sociology workshop; the Qualitative Methods seminar; the Culture, History, and Politics workshop; and the Gender & Sexuality workshop at the University of Michigan. I am also grateful to Joya Misra and the editors and four anonymous reviewers for their insightful comments. I am indebted most of all to the women in this study who shared their experiences with me.
Funding for the research was provided by the Rackham Graduate School and the Department of Sociology at the University of Michigan.
Notes
Danielle Czarnecki is a doctoral candidate in sociology at the University of Michigan. Her dissertation examines how Christian women experiencing infertility navigate gender, religion, and science when trying to have a child.