
Abstract
Social scientists have expended substantial effort to identify group patterns of deviant behavior. Yet beyond the ill-conceived treatment of sexual minorities as inherently deviant, they have rarely considered how gendered sexual identities (GSIs) shape participation in deviance. We argue for the utility of centering theories of gender and sexuality in intersectional deviance research. We demonstrate how this intentional focus on gender and sexuality provides important empirical insights while avoiding past pitfalls of stigmatizing sexual minorities. Drawing on theories of hegemonic masculinity, emphasized femininity, and minority stress together with criminological general strain theory, we demonstrate how societal expectations and constraints generate strains among GSI groups that may lead to distinctly patterned deviance, using the case of prescription drug misuse during sex. We employ thematic analysis of 120 in-depth interviews with people who misuse prescription drugs, stratified by GSI. We identify six themes highlighting distinct pathways from strain to misuse during sex for different GSI groups: intimacy management, achieving sexual freedom, regulating sexual mood, performance confidence, increased sense of control, and managing sexual identity conflict. In this article, we demonstrate the empirical and theoretical importance of centering gender and sexuality in deviance research and provide a roadmap for theoretical integration.
Social scientists have long sought to understand differing group patterns of deviant behavior. Yet, scholars rarely consider sexuality as an identity that shapes deviance. Aside from the historical treatment of sexual minority identity as deviant in and of itself (Woods 2014), deviance research has limited the inclusion of sexual identity largely to victimization and intimate partner violence (e.g., Perry and Alvi 2012; Ristock 2011). Although these are crucial topics, we must also strive to understand how sexuality influences participation in a variety of deviant behaviors. We can deepen these understandings by considering how gendered sexual identity (GSI) shapes deviance, because the intersection of gender and sexuality is particularly important in shaping numerous behavioral patterns (Byrd et al. 2015; Hunt and Antin 2019; Parry and O’Neal 2015).
In this article, we integrate scholarly understandings of GSI with deviance research. Specifically, we center GSI in an examination of motivations for and pathways to deviance in the context of substance use. Drawing on the theories of hegemonic masculinity (Connell 1995; Connell and Messerschmidt 2005), emphasized femininity (Connell 1995; Schippers 2007), and minority stress (Brooks 1981; Meyer 1995) and the criminological theory of general strain (Agnew 1992), we demonstrate how societal expectations and constraints generate strains among GSI groups that ultimately lead to patterned deviance by considering a specific example of deviance: prescription drug misuse 1 during sex.
We use the term gendered sexual identity (GSI) to simultaneously center the importance of a person’s sexual identity and underscore how its expression is fundamentally tied to a person’s gender and a society’s broader gender structures. These expressions of identities are also tied to other core identities, such as race and class, as the discussions of intersectional experiences (Collins 1991; Crenshaw 1991) and later works (e.g., Bowleg 2008; Collins 2004; Townsend et al. 2010) highlight. While we mention these additional identities and stress their importance for further research, our analyses focus on GSI to prevent disaggregating categories beyond analytic viability and because GSI is highly salient in the site of analysis: sexual experiences. 2
In this article, we demonstrate pathways from GSI-related strain to prescription drug misuse during sex via strain’s manifestation in sexual anxiety and other negative emotions during sexual encounters. In doing so, our analysis supports the need to center GSI in deviance research (Kahle, Rosenbaum, and King 2018; Peterson and Panfil 2014). We selected prescription drug misuse as a deviant behavior that is both practiced within this context and of heightened concern due to high prevalence of misuse and dependence (Kantor et al. 2015). The goal of this study is twofold. First, we aim to illuminate how GSI shapes deviant behaviors that have both societal and individual consequences. Second, we do so in a theoretically cohesive way that can anchor future studies of sexuality-stratified participation in deviance without pathologizing sexual minorities. We begin by introducing general strain theory. Subsequently, we integrate hegemonic masculinity and emphasized femininity as well as minority stress to demonstrate how GSI shapes distinct types of strain across these identities. We then briefly situate prescription drug misuse during sex within its wider context.
Theoretical Background
General Strain Theory
General strain theory posits that various types of unpleasant experiences—collectively termed strain—lead to deviant behavior. Merton (1968) introduced strain theory by proposing that a mismatch between societal goals and legitimate means to achieve them drove crime. Agnew (1992) broadened the definition of strain to predict deviance on an individual level. Although everybody experiences strain, not everybody responds to strain with deviant behavior. An individual’s likeliness of deviance depends primarily on overall exposure to and severity of strain, personality and disposition, and access to positive coping mechanisms (Agnew 1992).
Agnew (1992) defined three categories of strain: failure to achieve positively valued goals, removal of positively valued stimuli, and introduction of negative stimuli. Strain within a sexual or romantic context can fall into each of these categories. For example, inability to perform in sexual situations or achieve a pleasurable experience, as well as rejection in romantic pursuits, constitutes failure to achieve positively valued goals. When an individual exits a cherished relationship, they experience strain via removal of positively valued stimuli. Last, introduction of negative stimuli can result from experiences of sexual assault, exposure to sexually transmitted diseases, and fears of unplanned pregnancies. Using this framework, strain generated in anticipation of or during sexual situations may lead an individual to commit a deviant act, such as substance use. While we provide these examples generally, we argue that sexual sources of strain are intimately linked with an individual’s GSI, necessitating differentiation of pathways to deviant behavior by distinct identities.
Importantly, emotions mediate the relationship between strain and deviant behavior, whereby strain creates unpleasant emotions, and individuals sometimes respond by engaging in deviant behaviors, either to cope with the emotion or eliminate the strain’s origin (Agnew 1992). Although early empirical examinations focused on anger (Agnew 1992), other emotional responses to strain, such as depression and anxiety, can also lead to deviant acts, particularly inwardly directed deviance such as drug use (Preston 2006). We extend this line of inquiry to focus on sexual anxiety specifically as a negative emotion likely salient during sex.
According to Awada et al. (2014, 567), sexual anxiety is not considered a disorder. Rather, it is a phenomenon whereby anxiety is experienced in relation to sexuality, often in the context of sexual difficulties and/or relational hardships. It is best described as a dimension, most people having felt some anxiety associated with their sexuality, but only a minority experiencing it as an impairment.
As this definition relates anxiety to sexuality, it can be a response to a variety of GSI-related strains. However, research on sexual anxiety is limited. Early research examined arousal experiences among sexually anxious women (Chambless and Lifshitz 1984; Wishnoff 1978). More recent research examined fears of sexual inadequacy leading to sexual anxiety (Dèttore, Pucciarelli, and Santarnecchi 2013) or risky sexual behaviors (Philaretou and Allen 2003). Beyond physical performance, sexual anxiety may manifest in a range of ways, including discomfort with intimacy, concerns over partner choice, and anxieties about others’ perceptions.
Beyond consideration of emotions, Agnew (2008) recognized that while general strain theory can identify group differences, especially by gender, it cannot explain why those differences exist. Rather, he stressed that explanations lie in macro-level theories, and scholars must integrate these theories, including feminist theories, into general strain to explain group differences. Building on this, researchers have engaged with feminist criminology to establish general strain theory’s explanatory power for women (Eitle 2002) and sexual minorities (Button and Worthen 2017), suggesting potential broad applicability beyond the traditional subject of criminology: heterosexual men. This research demonstrates how gender- and sexuality-based discrimination and victimization results in negative outcomes, including substance use and crime (Button and Worthen 2014; Eitle 2002). Further, it highlights the importance of considering gender and sexuality through an intersectional framework by delineating the different victimization and offending behaviors of sexual minorities (Button and Worthen 2017). Building further on these macro-level explanations, we consider how relevant gender theories can be further integrated to explicate GSI differences in strain.
Sources of GSI-Related Strain Processes
There are multiple sources of strain that may disproportionately or uniquely affect people of different GSIs. Because sex is our analytic site, we focus on how hegemonic masculinity, emphasized femininity, and minority stress create GSI-divergent romantic- and sexually related strains. Importantly, gender and sexual identity are intersectional in nature (Shields 2008), and thus the experiences of sexual encounters—including those related to strain—fundamentally depend on how gender and sexuality intersect. Such GSI-divergent sources of strain can be conceptualized through a paradigm that highlights the socially constructed nature of gender and the systems of social rewards that undergird gender conformity (for a recent overview, see Levant and Powell 2017). In this section, we draw on hegemonic masculinity and emphasized femininity as key structural mechanisms that can create strain.
According to Connell (1995), hegemonic masculinity is a key mechanism that creates and sustains gender stratification between men and women and among men themselves. The theory posits that although multiple masculinities exist, societies have a virtually unattainable masculine ideal—hegemonic masculinity—toward which many men nonetheless orient their behavior and identity. Hegemonic masculinity is not a stable attribute that one can possess, but rather a space inhabited by continually negotiating behaviors and expressions (Connell 1995; West and Zimmerman 1987). The confines of this space are historically and culturally contingent and intersect with other identities, such as race/ethnicity (Collins 1991, 2004; Connell 1995). Although not all men desire to fully inhabit this space, they often benefit from its existence; and at different points, most men feel pressured to behave in ways that afford them access to all or parts of it.
Sex is a crucial site where hegemonic masculinity may feel highly salient. As Segal (1994) discusses, sex is a principal element of Western masculinity and centers on penetration as domination, in part because of its pairing with compulsory heterosexuality. In a classical definition of a heterosexual encounter, men’s expected role is an active one of penetration. As a result, men may feel pressure to perform, as well as experience constraints around passivity, sources of pleasure, and emotional intimacy (Bird 1996). Inability to fulfill a performance role in sexual interactions can disrupt masculine identities (Fergus, Gray, and Fitch 2002). Thus, hegemonic masculinity shapes the experience of anxieties, albeit in distinct ways for heterosexual men and sexual minority men.
Emphasized femininity operates relationally with hegemonic masculinity (Schippers 2007). 3 While emphasized femininity dominates other femininities, it remains subordinate to masculinities, and its contents consist of less-valued traits that lend validity to men’s domination. In contemporary Western culture, these traits include passivity, emotionality, and deference. During sexual interactions, women may feel strain related to a sexual double standard. On the one hand, they are expected to remain sexually “pure” (Valenti 2009), while on the other hand they are expected to provide pleasure and to show deference to their partner’s wishes (Currier 2013). In heterosexual encounters especially, women may feel reluctant to advocate for their wants or needs. Indeed, women may experience strain concerning power-imbalanced situations, including past experiences with or fear of future sexual assault 4 (Acierno, Resnick, and Kilpatrick 1997).
Importantly, as suggested above, hegemonic masculinity and emphasized femininity are foundationally heterosexual (Connell 1995; Schippers 2007). Any nonheterosexual interaction necessitates divergence from one’s hegemonic gendered expectations, which itself can be a source of gendered strain. Sexual minorities may lean into subordinate masculinities and femininities, inherently giving up some power in the process, or alternatively may feel increased pressure to perform in ways that afford access to some hegemonic masculine or feminine spaces. For instance, sexual minority women may either attempt to access or consciously reject emphasized femininity, shaping their encounters through subtle conformity or resistance to these ideals. Either strategy may introduce strain in sexual interactions, and women may choose different strategies in different situations, such as with male or female partners.
Emerging directly from the embeddedness of compulsory heterosexuality (Rich 1980) within hegemonic masculinity and emphasized femininity, this strain is tied to experiences of minority stress. Minority stress theory suggests that members of minority groups experience elevated levels of stress related to their minority status (Brooks 1981; Meyer 1995). Not only do sexual minorities experience the acute and chronic stressors to which all people are exposed, but they experience stressors uniquely linked to their sexuality (Frost, Lehavot, and Meyer 2015; Meyer 1995). This stress is chronic because it comes from relatively constant social and cultural structures.
There are numerous reasons to expect that GSI will affect the sources of minority stress experienced by sexual minorities during sex. First, compulsory heterosexuality defines other sexualities as atypical (Rich 1980). Sexual minorities may therefore experience strain due to structural and cultural invalidation of their sexual identities, unlike straight individuals. Relatedly, sexual minorities may experience stress related to internalized homophobia (Boone, Cook, and Wilson 2016), translating the distal stressor of compulsory heterosexuality into a maximally proximal stressor. Bisexual men and women may experience additional invalidation of their sexual identities owing to mono-sexism (Roberts, Horne, and Hoyt 2015), whereas individuals questioning their sexuality may experience strain related to this uncertainty.
In sum, we identify multiple gendered sexual constraints and expectations that may create differential GSI-related strains for men and women of varying sexual identities. In turn, this strain may manifest in sexual anxiety, to which individuals may respond with deviant behaviors. We study this pathway by examining prescription drug misuse during sex.
Prescription Drug Misuse
Although strain and resulting sexual anxiety may lead individuals to engage in deviant acts, including substance use, prescription drug misuse during sex is a useful case because it has been a major drug trend of concern, and the effects are wide ranging. Misused prescription drugs exist in three primary classes—pain relievers, stimulants, and sedatives—and have variable effects across these classes, which collectively mirror the effects of various other substances. Although numerous individuals use prescription drugs legally for medical purposes, others misuse these drugs by intentionally consuming them without a prescription or for a recreational purpose (Compton and Volkow 2006).
Prescription drug misuse has seen a troubling surge since the 1990s, particularly among young adults, as physicians have dramatically increased their prescribing (Compton and Volkow 2006; Kantor et al. 2015; Rigg, March, and Inciardi 2010). These trends not only concern health professionals but also are of interest to deviance scholars. We add to the literature on prescription drugs by looking at misuse occurring specifically during sex. Research shows that substance use before and during sex increases the odds of risky sexual behaviors and poor sexual health outcomes (Benotsch et al. 2011; Wells et al. 2015).
Although these studies reveal adverse outcomes, less is known about the motivations underlying prescription drug misuse during sex. We extend this line of research by interrogating whether strain, as expressed through sexual anxiety, is an important motive for this behavior. Further, we examine whether distinct relational patterns between strain and misuse during sex exist for different GSI groups, given that GSI directly affects sexual interactions and the likely sources of strain. While contributing to needed theoretical development addressing deviance and gendered sexual identity, we also consider practical elements for prevention and health promotion. In what follows, we analyze in-depth interview data to reveal dimensions of sexual anxiety that operate differently based on GSI and how this process shapes deviance.
Methods
The research team generated a sample of nightlife-involved young adults in New York via time–space sampling, which adds random variation to samples of venue-based populations (Parsons, Grov, and Kelly 2008). The team established a diverse list of venues with significant young adult patronage through fieldwork. Venues were assigned a number, and a random number generator yielded monthly sampling schedules varying by time and day. Research staff screened patrons, intending to approach all young adults present. Those who consented (75.0 percent) completed a brief screening survey. Eligibility was determined based on age (18–29 years) and prescription drug misuse on three or more occasions during the previous six months, with at least one instance in the past three months. If subjects were eligible (9.4 percent of those screened), staff distributed a study description and collected contact information. All participants completed a quantitative survey, and half (n = 214) completed semistructured qualitative interviews.
We took a GSI-stratified random sample of qualitative interviews. We were attentive to diversity among sexual minorities, given that bisexual and questioning individuals may have different experiences from those of gay and lesbian individuals (Marshal et al. 2008). Thus, we took all available interviews from bisexual and questioning individuals, resulting in 11 bisexual and 4 questioning women, and 8 bisexual and 1 questioning men. We then randomly selected 15 lesbian/queer women and 21 gay/queer men, for a total of 30 sexual minority women and 30 sexual-minority men. Together with 30 random straight women and men each, the analytic sample consists of 120 young adults. While this strategy provides an equal number of straight and sexual minority individuals of each gender, we were careful not to lump the experiences of all sexual minorities together. One hundred twenty interviews provide a large qualitative sample to achieve theoretical saturation across groups within the analysis (Charmaz 2006; Guest, Bunce, and Johnson 2006). Basic sample demographic characteristics are defined in the Online Appendix Table A1.
Interviews were conducted privately. For participants indicating prescription drug misuse during sex, interviewers asked about influences on sexual desire and their effects during sex. Interviews employed critical incident measures, which reduce recall bias and provide context by asking respondents to detail specific events (Leonard and Ross 1997). This technique provided data on respondents’ impressions of prescription drug misuse during sex, and motivations for, experiences of, and reflections on those experiences.
We analyzed the interviews iteratively, initially using inductive techniques to search for patterns of misuse during sex, particularly those that indicated motivations. We began by reading all 120 interviews to isolate data where respondents discussed sexual activities. We then reread this subset of data to get sufficiently familiar with it. Subsequently, we coded the data descriptively (e.g., performance concerns). Over time, we used both inductive and deductive techniques, via open and axial coding, which allowed building theory through the data while having a theoretical foundation to expand upon (Charmaz 2006). We reread the coded data multiple times, condensing the descriptive codes and searching for emerging patterns and concepts (Charmaz 2006; Miles, Huberman, and Saldaña 2013). After multiple discussions and recoding, six themes emerged. Our conceptualization was based on the most salient themes across respondents; thus, the quotations below represent larger patterns, not isolated expressions.
Before describing our results, we briefly note methodological limitations. Prescription drugs are a particularly useful case to study because their varied effects across classes—painkillers, stimulants, and sedatives—mimic the effects of a range of other substances, including licit substances such as alcohol and illicit ones such as cocaine. Yet young adults may view prescription substances, even when misused, in a more positive light because of their association with medical settings. Further, because participants were recruited at nightclubs, findings are more representative of experiences of socially active young people. Finally, disaggregating groups across too many intersectional identities creates further challenges, and we return to the theoretical implications of this in our discussion.
Results
Analyses revealed unique motivations toward and experiences with prescription drug misuse during sex, with different patterns based on the intersectional nature of GSI. While we include information about respondents’ self-defined parental class and race/ethnicity owing to their importance in intersectional identities, again, we cannot further disaggregate the results by these categories; we return to this point in the discussion.
Narratives provide contextualized information on sources of strain that manifest for GSI groups and are influenced by hegemonic masculinity, emphasized femininity, and minority stress. Our results focus on pathways to prescription drug misuse during sex and subsequent experiences under the influence, while highlighting conclusions about strain, sexual anxiety, and deviant behavior. Among all GSI groups, some respondents claimed that prescription drugs did not affect sexual experiences, even when they had sex under their influence. However, many respondents described distinct motivations toward prescription drug misuse during sex that demonstrate GSI-divergent experiences of strain. We discuss six themes: intimacy management, achieving sexual freedom, regulating sexual mood, performance confidence, increased sense of control, and managing sexual identity conflict.
Respondents in all GSI categories expressed a generalized theme about the alleviation of strain from sexual anxiety: Prescription drugs lowered sexual inhibitions. However, the meanings of lowered inhibitions differed across groups. For heterosexual men, misusing prescription drugs to lower inhibitions was fundamentally about intimacy management. Across women of varying sexual identities, lowered inhibitions related to experiencing a sense of sexual freedom. For sexual minority men, lowered inhibitions resulted in sexual mood regulation. These interrelated themes constitute the first three themes.
Intimacy Management
Heterosexual men discussed lowered inhibitions related to physical and verbal intimacy, which hegemonic masculine ideals constrain. After taking painkillers, one white man from an upper-middle-class background claimed that “you just sometimes feel more like you kind of just want to touch someone or be with someone.” Similarly, when asked about the last time he had sex on sedatives, a middle-class straight white man described: I think it was just more cuddly than normal, ’cause I’m not much of a cuddler. . . . I was feeling very relaxed because I was on it, and I kind of just wanted to cuddle and then that led to sex (laughter). Yeah, who knows, I might have had sex either way whether I was on it or not, but I definitely was more in the mood. . . . It’s not like energetic sex, it’s more like calm sex, and it definitely feels better when I’m under the influence.
Other respondents described similar effects from painkillers and sedatives. Prescription drugs appear to facilitate physical intimacy during sexual encounters for these men and may also increase ease of verbal intimacy. For example, an upper-middle-class white man explained that “even after the sexual act there’s an ease with your partner . . . I don’t know, it’s just easier to talk too and the pillow talk is better.”
These examples suggest that some straight men hesitate to be physically or verbally intimate with their partners. Discomfort related to intimacy may be a source of strain related to expressing emotion resulting in sexual anxiety. In response, some straight men find that prescription drug misuse lowers inhibitions, allowing them to desire and experience intimacy more freely. To the extent that intimacy taps into deep emotions, it may prevent men from accessing hegemonic masculinity, which demands that men exercise emotional restraint (Connell 1995). Thus, the perceived need to restrain intimacy may be a negative stimulus that triggers sexual anxiety, resulting in prescription drug misuse to facilitate a desired type of sexual experience.
Achieving Sexual Freedom
Straight women often described lowered inhibitions, frequently expressed as an increased willingness to experiment during sex. Heterosexual women who felt fewer inhibitions tended to see these effects positively. For example, one middle-class straight white woman explained: If I’m sober, doing something sexually that normally might make me a little bit nervous, it’s not something that makes me nervous because I don’t want to do it, it’s more of, I want to, but I’m timid or something. . . . So I think Adderall kind of just takes me out of my shell a little bit. So it’s all things that I’m okay with, even when I evaluate it sober, but I just feel more out of my shell and willing.
Another middle-class white woman agreed that she is “more willing to experiment with different things” because “it’s part of being relaxed. . . . I’m not feeling rigid about what I normally do . . . when you’re relaxed, you’re probably just more willing to go with the flow.” In a third example, a straight, upper-middle-class Latina woman discussed a new sexual partner, explaining “the first time that I went with him to one of the shows, I took Xanax because it was a new situation. I wasn’t really sure what things were going to be like. And we did have sex but I guess it made me feel more comfortable around him and in the situation, so that we would go home together.”
In these examples, heterosexual women claimed prescription drugs allowed them to move beyond inhibitions and experiment with new sexual acts or partners. However, these were not later regretted; the women viewed lowered inhibitions as empowering. Thus, straight women may experience strain because of a reluctance to engage in desired or more experimental sex. Through prescription drug misuse, they overcome reluctance, a source of a negative stimulus strain driven by the ideals of emphasized femininity. Women hold less permissive views than men across a range of sexual attitudes and behaviors, likely reflecting the internalization of divergent gendered sexual expectations (Oliver and Hyde 1993). Prescription drugs may thus be a tool for heterosexual women to overcome sexual anxiety and more fully enjoy sexual experiences.
Sexual minority women described a lowering of inhibitions in ways mirroring heterosexual women’s experiences of sexual freedom, despite not always having gendered power imbalances. One bisexual, upper-middle-class white woman claimed that sedatives “loosens me up more. . . . I feel as though I’m more open about things and I’m more responsive in kind of different ways. . . . I’m more of the sexual partner that I want to be, but I’m a little too afraid to be when not on a sedative.” A queer, middle-class white woman echoed these sentiments, attributing the following to prescription drug misuse: “just being able to let my inhibitions go a little bit more, being able to achieve orgasm easier, and just generally being less embarrassed.” Like the straight women, sexual minority women described prescription drug misuse as facilitating positive and freer sexual experiences. These women describe “fear” and “embarrassment” during sex while sober, but they can be “more of the sexual partner [they] want to be” when under the influence. Therefore, women, regardless of sexual identity, may experience sexual strain related to engaging in sexual acts aligned with emphasized femininity and embracing themselves as sexually active women. This strain may lead to sexual anxiety, managed by prescription drug misuse.
Regulating Sexual Mood
The third theme, unique to sexual minority men, is prescription drug misuse facilitating a particular sexual mood. Often, sexual minority men described using stimulants to achieve an “aggressive” sexual appetite. However, there were also several instances of men using sedatives to relax and fulfill a passive role during sex. First, these men described stimulants as positively heightening sexual appetite, repeatedly using the term “aggressive.” When asked how stimulants affected his sexual desire, one bisexual, middle-class white man replied “it’s more aggressive for sure, so I’d probably be more likely to come on to someone or be aggressive in bed.” Similarly, a Black, queer, middle-class man explained that, regarding stimulants, “it’s waking you up and making you extremely aggressively horny.”
These descriptions demonstrate a strong relationship between stimulants and “aggressive” sex drive for sexual minority men, tapping into masculine ideals of performance. Interestingly, this relationship was not present for straight men, although it may be related to their concerns about performance or sexual minority men’s capacity to be sexually aggressive without an erection during receptive intercourse. Nonetheless, there was an exclusive focus on cultivating a high sex drive among sexual minority men. Some respondents explicitly compared themselves to straight men. For example, one working-class Latino gay man described himself by saying “I’m very much a normal sex drive gay man . . . which is above sex drive straight man.” Another queer, middle-class mixed-race man explained the relationship between prescription stimulants, sex, and sexuality: painkillers were far more abused in my straight circles of friends. Especially the ones that kinda stayed at home. . . . Maybe they use it as escape, or some kind of fun. Whereas I find in the gay world there’s a heatedness to it. There’s this definite link to sexuality and sexual goings-on. . . . It’s more for the sex fiends.
These respondents suggest that sex drive is a crucial component of sexual minority male identity among those who misuse prescription drugs. Some explicitly compare their sex drive to that of straight men, suggesting that prescription drug misuse serves a nonsexual purpose among straight men. Therefore, sexual minority men may experience strain from attempting to meet perceived normative expectations of a high sexual threshold.
Alternatively, some sexual minority men described prescription drugs’ ability to achieve an opposite sexual mood: relaxation and passivity. For example, one white, middle-class gay man described a sexual experience with his boyfriend after taking a Xanax: If I’m more relaxed, I’m more likely to do a little more. . . . Physically my muscles are relaxed, so I find that getting head or receiving anal, it’s just easier and therefore more enjoyable when on sedatives.
Another mixed-race, middle-class Latino gay man explained that after taking sedatives, “the physical tactile sensation is different. Again, like the feelings of being at peace or being contented or relaxed.” In both cases, sedatives allowed respondents to physically and mentally relax during sex. Overcoming a potential source of strain that may result in sexual anxiety, the ability to relax is an important motivator for prescription drug misuse during sex, particularly for sexual minority men in instances when they are receptive partners. These motivations may also tie into masculine ideals about performance. However, with regard to the negative effects of misuse for sexual minority men, there is a potential feedback loop of strain caused by substance use, a point to which we return later.
Performance Confidence
The fourth theme, unique to straight men, was that prescription drugs increased respondents’ confidence about sexual performance. For these men, confidence largely related to physical performance, and they almost unanimously lamented that sedatives and painkillers make it more difficult to get an erection. However, when they do obtain an erection, they praise these drugs for allowing extended performance without orgasming, enhancing the potential to please their partner, and thus overcoming strains related to achieving positively valued goals by more closely embodying the ideals of hegemonic masculinity. One upper-middle-class white man described this when he said “it sucked that I couldn’t get it up but then once I did get it up and lasted a while, then that was good.” Another white, middle-class respondent described the same phenomenon, reporting: It wasn’t as passionate . . . it lasted longer though because I lasted longer. . . . I couldn’t feel as much but it was good. I mean overall if you gave me the choice . . . take a painkiller and have sex or don’t take a painkiller . . . I would usually take it. I’d say nine times out of ten. So I would say it’s a preferable experience in that sense.
In this latter case, concern with performance took priority over the respondent’s own physical pleasure. Despite sex on painkillers being less “passionate” and the respondent not “feel[ing] as much,” he prefers sex under the influence because prescription drugs allow him to last longer. A third Black, middle-class man expressed similar sentiments with stimulant misuse, claiming “I was just more focused [during sex]. So it definitely helped me out.” This suggests that confidence and prowess are powerful motives for prescription drug misuse, and straight men may experience strain because of performance concerns. Performing heterosexuality is crucial to straight men’s assertion of their masculinity (Connell 1995), and thus a linkage between preoccupation with sexual performance and prescription drug misuse emerges for straight men.
Increased Sense of Control
Some prescription drugs, especially stimulants, increased respondents’ sense of control during sexual situations. This theme was unique to straight women, many of whom expressed that stimulants gave them more control over their sexual experiences. Largely, these scenarios emerge from gendered power imbalances that women experience during heterosexual encounters. Gendered power imbalances create experiences in which some women feel strain related to an inability to achieve their goals by asserting themselves. Prescription stimulants allow these women to circumvent the strain of passivity expectations entrenched within emphasized femininity. For example, one middle-class white woman said, “I think with any stimulant, you have, or at least you believe you have, more control over your outcome.” Another white, upper-middle-class woman remarked that “it makes you more like oh, my God, you gotta wear a condom. There’s no way I’m doing that. I feel like it makes me more aware, actually, if it’s just Adderall.” A third middle-class white woman expressed similar sentiments, claiming: I also actually felt courageous in being strong-willed and only doing what I wanted to do. Sometimes being sober, I feel like I can be talked into doing something . . . probably nothing dangerous, but . . . on Adderall, I feel a little bit more strong-willed and self-determined, and I am determined to be safe, you know? So I’m not wanting to get pregnant or have an STD.
These responses reveal that women feel more control over sexual encounters and an increased ability to advocate for desired sex. This is important because young women typically have lower sexual self-efficacy than men, which can lead to unwanted or unsafe sexual situations (Phillips 2000). These women described their increased sense of control positively, using phrases such as “strong-willed,” “self-determined,” and “more aware” to capture the effect of stimulants during sex. Without stimulants, straight women may feel less able to control aspects of sexual encounters, especially those relating to safe sex. Lack of control is thus a potential source of strain, and gaining sexual control provides a strong motivation for misusing prescription drugs. Interestingly, no members of other GSI categories mentioned an increase in control due to stimulants, suggesting that straight women may uniquely face strain from sexual gendered power imbalances.
Sexual Identity Conflict
The final theme, exclusive to sexual minority men and women, was misusing prescription drug to address conflicts about sexual identities. These strains stem from negative stimuli emerging from compulsory heterosexuality accentuated by both hegemonic masculinity and emphasized femininity. Such strain was based explicitly within the context of these gender ideologies producing minority stress. For example, in describing regrettable sexual experiences, one white, middle-class lesbian explained, most of the mistakes that I’ve made with Xanax were with men and I’m really, I’m gay, so gay, and I think that I was in denial about it, about a lot, and that’s why I didn’t enjoy sex with men. . . . Sober sex or fucked up sex with men was never good for me, it’s never been good for me, it’s never been a pleasant thing, it’s never been something I want to do, so the majority of times it happens is when I’m fucked up and I don’t care.
This respondent had dated men until adulthood, when she began dating women exclusively, as she was “in denial” about her sexual identity. Although it was “never . . . a pleasant thing” for her, she frequently had sex with men after misusing prescription drugs, particularly Xanax. Although she regretted these encounters, she misused prescription drugs to attempt to manage strain from her sexual identity conflict. Yet these encounters may have contributed to that very same strain, again pointing to the feedback mechanism described below. Additionally, this respondent echoes sentiments expressed by sexual minority men regarding the appropriateness of their sexual partners, with additional pressure to have a partner of a different sex.
In a contrasting example, a bisexual, lower-class Latino man explored his sexuality while misusing prescription drugs, rather than misusing them to suppress questioning. He explained that “drugs definitely had a bearing on my sexuality and if I never would have done any of these drugs, I would have identified myself as a heterosexual man.” Earlier, the respondent described himself as previously being “completely homophobic,” refusing to acknowledge that he was bisexual. He could only accept sexual advances from other men and explore his bisexuality under the influence. In the earlier example, the woman continued to have sex with men while misusing drugs to maintain her denial about her sexuality. In contrast, this man misused prescription drugs to overcome internalized homophobia and explore his bisexuality. Therefore, both respondents misused prescription drugs to navigate strain from conflicts about their sexualities in divergent ways. This theme suggests that sexual minorities may respond to compulsory heterosexuality with internalized homophobia or refusal to acknowledge their sexual identity, and that misusing prescription drugs plays a role both in perpetuating these responses or overcoming them. Thus, for some sexual minority young adults, strain may stem from sexual identity conflict and drive prescription drug misuse.
Strain Feedback Loop
Prescription drug misuse during sex was generally described positively as a strain-alleviating behavior. However, some interviewees described such experiences as generating strain. Prescription drug misuse during sex may reduce strain in the moment but increase strain afterward. In this manner, a strain feedback loop may emerge for some—but not all—who engage in these practices. While not a theme per se, these processes are nonetheless noteworthy.
Although some women described lowered inhibitions as positively enabling sexual freedom, other women described them as prompting impaired judgment, leading them to engage in sexual acts or to be sexually involved with somebody that they otherwise would not have. One middle-class white queer woman explained that “it’s more like who I’m having sex with that my judgment would be impaired. I would be more likely to have sex with somebody than I would consider not having sex in the first place.” A Black, upper-middle-class bisexual woman echoed this sentiment: I think it’s because I’m just a lot more open. . . . I definitely have not turned anyone away . . . this is one of those instances where I end up hooking up with my friend and we had a Xanax and a codeine and we have been drinking and we ended up totally thinking it’s a great idea to not only hook up but sleep with another man we just met that night.
Therefore, women had both positive and negative responses to prescription drug misuse during sex, though negative experiences could ultimately generate rather than ameliorate strain. In these examples, respondents expressed that prescription drugs impaired judgment and led to sex with people that they would not have had sex with sober. Although these women had negative responses, their regret likely relates to the inhibitions expressed by the women who described positively overcoming them. Whereas other sexual minority women focused on sexual acts, these women focused on their partners’ identities. Because of expectations that women remain sexually “pure” (Valenti 2009), they may feel more pressure to choose certain sexual partners rather than remaining open to a variety of partners or to “hooking up.” Although prescription drugs can help some women overcome strain stemming from adherence to emphasized femininity, for others, loosened inhibitions cause regrettable experiences, resulting in strain.
Similarly, positive effects of sedatives were not universal among sexual minority men. While they generally agreed sedatives allowed them to be more passive and relaxed, many viewed that effect as negative or dangerous. In these cases, men used these drugs in combination with other substances while partying, leading to risky sexual situations. For example, when asked about sedatives, one white, middle-class bisexual man explained that they affect “your mood and temperament because you are super relaxed and probably more passive, so that can potentially be dangerous . . . if you were in a social situation that would be quite bad, but if you’re out at a bar and took a bunch of sedatives that would be really stupid to be more vulnerable.” He then described a situation when he took a Xanax in college and became vulnerable to the advances of another man, who made out with him without consent. Similarly, when describing Klonopin, a mixed-race, middle-class queer man claimed: every time I’d take them . . . I don’t know if it was just the fact that I’m a horny bastard and was drunk and then these things make you just kinda mentally check out and get myself in all kinds of trouble. Sexually, even, but, again, I would never take it and be like, “Ah, I’m horny” . . . it’s just like, bad decision.
By leading to increased passivity and relaxation, misusing prescription drugs could make them “vulnerable” and experience “all kinds of trouble,” increasing their perceived risk for sexual assault. This is a logical perception, given that sexual minority men are at an increased risk for sexual assault (Rothman, Exner, and Baughman 2011). Further, they contrast even with those sexual minority women who describe negative results of prescription drug misuse during sex in terms of regret, because these women’s negative interpretations relate to gendered expectations and not explicitly to fear for safety. Regardless, adverse experiences under the influence may lead to strain in a manner that creates a feedback loop.
Discussion
Deviance research frequently neglects GSI, leading to a crucial knowledge gap (Peterson and Panfil 2014). Our study had two aims in addressing this gap. First, we sought to provide knowledge about how GSI shapes prescription drug misuse during sex, a critical element of a larger crisis with the potential for adverse outcomes at both individual and societal levels (Benotsch et al. 2011; Wells et al. 2015). Second, we intended to provide a theoretical foundation for future studies to broaden examination of how GSI influences deviant behaviors without pathologizing sexual minorities. We address each in turn.
First, although prescription drug misuse has increased, deviance research—particularly that which is theoretically informed—has insufficiently addressed this behavior in general or in conjunction with sexual activity (Kantor et al. 2015; Watkins 2016). Thus, we argue that past, present, or anticipated sexual experiences can be sources of strain, which in turn motivate some people to engage in the deviant act of prescription drug misuse during sex. Studies have shown that prescription drug misuse relates to risky sexual behaviors (Benotsch et al. 2011; Wells et al. 2015). However, researchers had not previously elucidated the processes involved in this relationship nor the motivations behind prescription drug misuse during sex. This article addresses this gap by examining a critical pathway to prescription drug misuse during sex: sexually situated strain via sexual anxiety.
Our results show that GSI shapes this sexually situated strain and resulting misuse. Straight men were the only individuals to discuss using painkillers and sedatives to manage expectations around intimacy and achieve longevity of sexual performance, the first related to overcoming constraints of hegemonic masculinity and the latter related to accessing it. However, sexual minority men also described prescription drug misuse—here, stimulants—to achieve the desired performance goal of an “aggressive” sexual appetite. While describing their goals and motivations differently, and relying on separate classes of prescription drugs, both straight and sexual minority men misuse prescription drugs to achieve performance goals related to hegemonic masculinity (Connell 1995).
Further, we demonstrate that the effects of substance misuse are sometimes positive. Most surprisingly, many straight women in our sample experienced both sexual empowerment and greater control than they otherwise might have following stimulant misuse. Sexual minority women also described freer sexual experiences via drug-induced lowered inhibitions, suggesting that women of all sexualities experience strain related to gendered power imbalances or expectations of sexual purity. Prescription drugs help them challenge this strain and achieve safer and more fulfilling sexual experiences. We also discussed a man who accepted his bisexuality via prescription drug misuse, demonstrating the minority stress of compulsory heterosexuality (Meyer 1995; Rich 1980) and the capacity of prescription drugs to help overcome it. We in no way suggest that prescription drug misuse during sex is unproblematic, and the negative experiences of some in our sample clearly demonstrate numerous adverse consequences. However, these findings suggest that existing literature misses important variation by focusing only on potential dangers of misuse during sex, and that strain theory may more broadly focus too exclusively on deviance as negative. In addition to theoretical growth, our findings hold relevance for practitioners who treat issues of substance misuse by stressing the need for training that is inclusive to all GSI groups and practices that discover motivations for drug misuse, because our findings suggest that similar-seeming behaviors can have very different roots.
Our results also highlight the possibility of a feedback mechanism within general strain theory, which is an important theoretical contribution to deviance literature that counters the positive strain-relieving effects noted above. For sexual minority men, prescription drug misuse for sexual mood regulation may cause new strain, such as regrettable sexual situations and safety fears. Similarly, for prescription drug misuse to manage strain associated with sexual identity conflict, the resulting behaviors—such as for the lesbian woman who had sex with men after using sedatives—risk exacerbating this strain, further driving anxiety and prescription drug misuse. In this manner, the linkages among strain, sexual anxiety, and prescription drug misuse imply a recursive process. Notably, we were surprised that no straight women discussed regret around sexual experiences following prescription drug misuse, although some respondents may have avoided discussing unpleasant or traumatic experiences. Additionally, we did not observe feedback loops for straight men, which may be related to privileges associated with hegemonic masculinity.
The fruitfulness of centering theories of gender and sexuality in analyses of deviance leads to our second main contribution. Given the dearth of research examining how GSI shapes participation in deviant behavior, we have provided a theoretical template for application to future explorations of the relationship between GSI and strain. For illustrative purposes, we have synthesized the data-driven theorization into a process-oriented model depicted in Figure 1, which may also prove useful for future quantitative research within this framework.
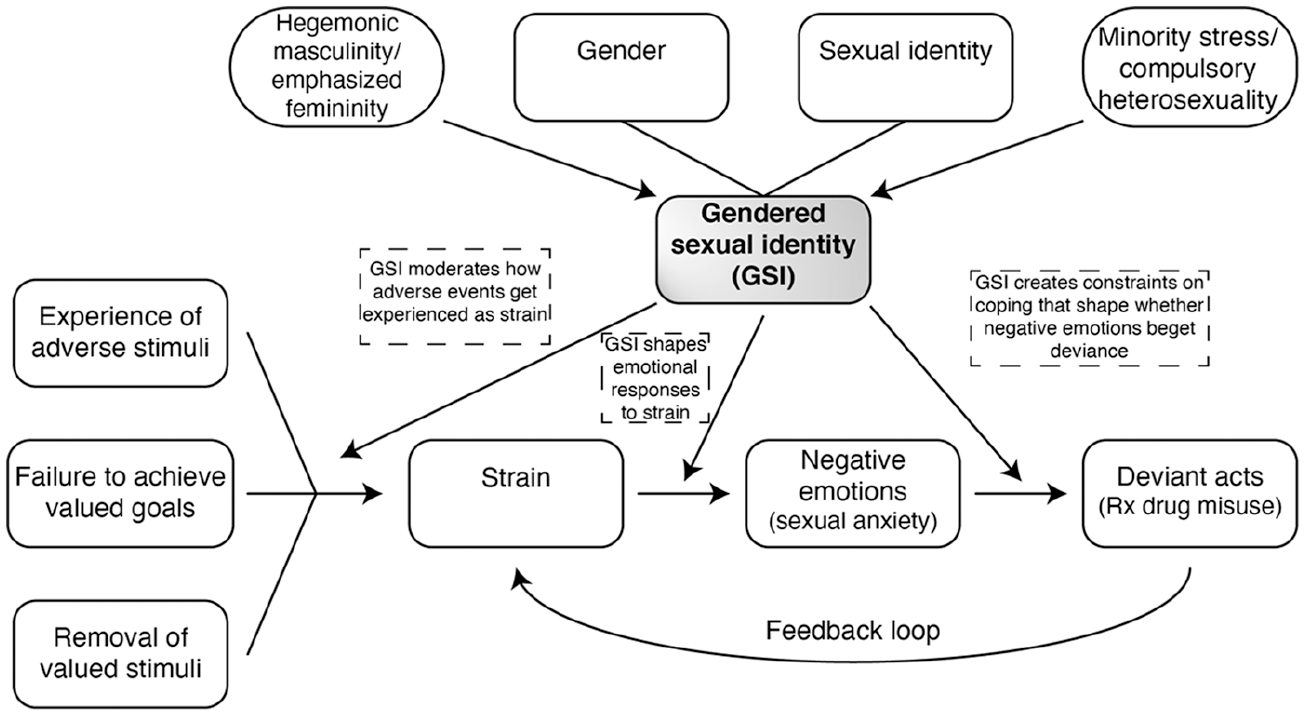
Theoretical Model
On the top of Figure 1, we show how gender and sexual identity are core identity components contributing to one’s GSI, such that we represent these relationships without arrows. Importantly, however, the structural and cultural forces involved in hegemonic masculinity/emphasized femininity (Connell 1995; Connell and Messerschmidt 2005; Schippers 2007) and compulsory heterosexuality (Rich 1980), along with exposure to minority stress (Brooks 1981; Meyer 1995), also influence how GSI is experienced and expressed. On the bottom left, we show how three types of events (adverse stimuli, failure to achieve valued goals, and removal of valued stimuli) can lead to strain that shapes negative emotions (here, sexual anxiety), which in turn can lead to deviance (here, prescription drug misuse during sex) (Agnew 1992).
The top and bottom of our figure are connected by crucial pathways through which GSI may moderate each step, and these connections demonstrate the theoretical integration of gender and sexuality theories with criminological theories. First, GSI moderates how adverse events are experienced as strain, such as a homophobic slur more likely experienced as an adverse stimulus by a sexual minority (Meyer 1995). Second, one’s GSI may shape the production of particular emotions experienced following strain, such as sexual anxiety. Third, GSI facilitates or constrains different types of coping mechanisms that shape whether negative emotions beget deviance. Finally, we highlight how participation in deviant acts can create a feedback loop leading to increased strain, such as in our examples of regretting sexual partners or exposure to unsafe sexual situations.
The theoretical model illustrated in this figure thus demonstrates that researchers can—and should—draw from core gender and sexuality theories when considering deviant behavior, because theories such as general strain can identify group differences but cannot explain why they exist without additional macro-level theories. In our case, we have shown how hegemonic masculinity, emphasized femininity, and minority stress shape the types of strain faced during sex. In turn, these strains produce sexual anxiety, and respondents turn to prescription drug misuse to either manage that emotion or address the original source of strain. By considering structural sources of strain and how they influence and constrain all individuals, including heterosexual men, we can understand the participation of GSI minorities in deviant behavior without the pathologizing of earlier deviance research.
Although centering GSI in this analysis fills a crucial knowledge gap in the criminological and substance use literatures, other axes of identity are also imperative for these processes. This particular analysis cannot account for differences that may stem from other identities, such as race and class. These axes are fundamental in how people construct their senses of self, and they are equally relevant to the types of societal forces, constraints, or privileges one experiences, which are also central to the way people construct, identify, and experience their gender and sexuality (Bowleg 2008; Collins 1991, 2004; Crenshaw 1991; Townsend et al. 2010). Further, privileged expressions of gender not only are influenced by race and social class, but can be utilized as tools of domination (Hamilton et al. 2019), which no doubt shape deviance processes. Our sample cannot thoroughly account for these important axes of identity, although our themes did exist across diverse members of GSI groups. Therefore, we implore others to build on our research in ways that account for how additionally diverse GSI groups experience strain processes. Importantly, the experiences of those with nonbinary genders should be incorporated, theoretically and empirically, into future work.
Although we focused on general strain theory and deviance occurring during sex, we do not imply either that sexual identity should only be incorporated into a single criminological theory, or that sex is the only analytic site in which to explore the unique effects of GSI. Rather, we highly encourage future sociological research that seriously incorporates sexual identity into theories that consider crime and deviance more generally. For instance, scholars should consider how GSI differentially shapes the role of marriage or employment within control theory, or how GSI differentially shapes peer influence within differential association theory. In considering these, scholars should think about how gender and sexuality theories at different levels of analysis might inform each of these criminological theories, from socialization theories to doing gender to gender as institution.
We ultimately view our study as an important step in an emerging literature that centers sexuality in deviance studies (e.g., Peterson and Panfil 2014). As we show, even a single topic comprising strain, sexual anxiety, and prescription drug misuse exhibits differing pathways for those of various sexual identities. A focus on GSI more generally will produce many analytic insights that will assist in tailoring prevention, intervention, and counseling efforts that are sensitive to sexual identity, while simultaneously informing theory.
Footnotes
Notes
Laura C. Frizzell is a PhD Candidate and Presidential Fellow in the Department of Sociology at The Ohio State University. Her research centers on the experiences of racial/ethnic, gender, and sexual minorities within the criminal legal system, from involvement in crime and substance use to reentry after incarceration.
Mike Vuolo is an Associate Professor in the Department of Sociology at The Ohio State University. He is the current Editor of Sociological Methodology, the official methods journal of the American Sociological Association. His research interests include crime, law, and deviance; health; work and education; substance use; the life course; and statistics and methodology.
Brian C. Kelly is Professor of Sociology at Purdue University. His research focuses on contextual influences of young people’s health, mainly on substance use, sexual health, and mental health.