
Abstract
Background
Recognizing early clinical signs of dementia is key to optimizing emerging therapies, including monoclonal antibodies. Mild behavioural impairment (MBI) characterizes later-life emergent and persistent nropsychiatric symptoms linked to greater dementia risk, representing a behavioural manifestation of the underlying neurodegenerative disease for some. The association of MBI with functional ability may therefore reveal subtle functional decline as an additional early risk marker in cognitively unimpaired (CU) older adults.
Methods
Baseline data from 1714 CU participants from the CAN-PROTECT study were analyzed. MBI was assessed using the MBI Checklist (MBI-C) (continuous and dichotomized, MBI+ ≥8). Functional ability was assessed using the SAGEA scale capturing instrumental and basic activities. Negative binomial models examined associations between MBI and function, adjusting for demographics, cognition, and physical/sensory limitations.
Results
Higher MBI-C scores (count ratio [CR] = 1.07; 95%CI: 1.06-1.07) and MBI+ status (CR = 2.64; 95%CI: 2.36-2.95) were associated with greater global and domain-specific functional impairments.
Conclusion
Findings highlight the importance of assessing both behavioural and functional changes in CU adults to identify at-risk individuals for timely interventions.
Plain Language Summary
Treatments for Alzheimer disease are most effective when started early, before clear memory and thinking problems develop. Identifying early warning signs is therefore critical. One potential early sign is mild behavioural impairment (MBI), which refers to new and persistent changes in mood, motivation, or personality that begin later in life. Another potential early sign is subtle difficulty with everyday activities. Although these mild difficulties do not interfere with a person’s independence, they may still represent an early signal of future cognitive decline. If we can capture both early behavioural changes and subtle difficulties in daily activities together, we may be able to better identify those at higher risk for dementia.
In this study, we examined 1714 older adults without cognitive impairment. We investigated whether individuals with behavioural symptoms also experienced subtle difficulties in everyday activities, such as managing finances, organizing tasks, or performing basic self-care. We found that individuals with more behavioural symptoms were more likely to have subtle challenges in daily functioning, even though their cognitive abilities remained normal. These differences were not explained by physical health, sensory limitations, or cognitive performance. These findings suggest that behavioural changes, together with subtle functional difficulties, may represent early indicators of increased dementia risk. Importantly, both can be assessed easily, cost-effectively, and remotely. This approach could help identify individuals earlier, when emerging treatments designed to slow Alzheimer disease may be most beneficial.
Introduction
Recent advances in Alzheimer disease (AD) therapeutics have shifted the field toward disease-modifying strategies, with emerging treatments targeting the underlying pathophysiology. Among these, the anti-amyloid monoclonal antibody (mAb) therapies are particularly promising, as they target amyloid-beta accumulation, a hallmark of AD pathology, with the potential to slow or modify disease progression.1,2 Evidence indicates that the effectiveness of such therapies is greatest when administered at the earliest stages, underscoring the urgent need for timely detection and accurate identification of early clinical symptoms. 3 Yet, identifying individuals at high risk remains challenging, as subtle cognitive deficits often appear after pathological changes are already underway. This challenge has prompted growing interest in non-cognitive clinical symptoms, such as neuropsychiatric symptoms (NPS) and mild functional changes, which may serve as early markers of risk for subsequent cognitive decline.
NPS, including depression, anxiety, apathy, agitation, and psychosis, are highly prevalent across the AD continuum4,5 and are increasingly recognized not only as accompanying features of dementia but also as early markers of underlying neurodegenerative processes. In this context, the mild behavioural impairment (MBI) construct has emerged as a valuable framework for capturing later-life onset and persistent (≥6 months) NPS that can represent early manifestation of neurodegeneration. 6 MBI has been consistently associated with greater risk of cognitive decline and progression to dementia, even among those with subjective cognitive decline or even cognitively unimpaired (CU) older adults.7-12 In addition to predicting clinical outcomes, MBI has been linked to a range of AD-related biomarkers, including amyloid-beta and tau accumulations13-19 and structural brain changes,20-23 highlighting its potential role as an early indicator of underlying neuropathology. Less is known, however, about subtle functional changes that may co-occur with MBI in the absence of measurable cognitive impairment. Identifying such early behavioural and functional changes together could improve risk stratification.
Functional ability, measured through activities of daily living (ADL), represents a critical outcome in aging, closely tied to independence, quality of life, and ultimately dementia diagnosis. ADL are broadly divided into basic (BADL) and instrumental ADL (IADL). BADL include fundamental physical activities such as feeding, bathing, dressing, and mobility, while IADL encompass more complex activities including managing finances, using transportation, organizing medications, preparing meals, and navigating social or community settings. 24 IADL require the integration of multiple cognitive domains including memory, executive function, attention, and visuospatial skills. Thus, decline in IADL tends to appear earlier than BADL in the course of neurodegenerative disease, sometimes preceding measurable deficits on standard neuropsychological tests.25-28 Recent studies further highlight that persistent impairment in IADL, ie, mild functional impairment, in the early stages is associated with an elevated risk of cognitive decline and dementia, 29 as well as greater amyloid-beta and tau pathology as measured in the CSF. 30 Importantly, prior research also shows that NPS are significantly associated with global functional decline in mild cognitive impairment (MCI) and dementia.31-35 However, the association between NPS and functional decline specifically among CU older adults has received less attention. Establishing such associations would highlight the importance of capturing subtle functional declines that may accompany MBI, providing an additional non-cognitive marker of risk for subsequent cognitive decline and progression to dementia.
The existing evidence on the association between NPS and functional decline in CU older adults is limited and has yielded inconsistent findings. A large longitudinal study reported that NPS were associated with subsequent decline in IADL performance. 36 However, NPS were measured with instruments that did not account for MBI core criteria of later-life symptom emergence and persistence. Thus, transient, reactive, and/or lifelong NPS unrelated to neurodegeneration were likely included. In contrast, a cross-sectional study of individuals with subjective cognitive decline used the MBI Checklist (MBI-C), 37 which operationalizes MBI criteria, and found no association between NPS and IADL. 38 Yet a more recent study using the MBI-C, reported associations between higher MBI-C scores and greater IADL impairment in CU individuals. 39 Thus, whether MBI is associated with functional difficulties in CU older adults, particularly at the level of specific ADL domains, is in question.
Here, we investigated whether MBI, assessed both as a continuous severity score and as a dichotomized status, was associated with global and domain-specific ADL performance in CU older adults. By establishing links between MBI and early functional changes, we sought to enhance risk stratification for individuals to be investigated with AD biomarkers, identifying those most likely to benefit from emerging therapies, such as mAbs, and to underscore the importance of integrating both behavioural and functional assessments for timely intervention.
Methods
Study Population
Participant data were obtained from the July 2025 data release of the Canadian Platform for Research Online to Investigate Health, Quality of Life, Cognition, Behaviour, Function, and Caregiving in Aging (CAN‐PROTECT). 40 CAN-PROTECT is an online, longitudinal, observational cohort examining brain aging in dementia‐free, community‐dwelling adults. All residents of Canada age ≥18 years are eligible for enrolment. Participants are excluded if they have an established diagnosis of dementia or cannot provide informed consent. Participants and their study partners complete annual assessments covering demographics, health, cognition, behaviour, function, lifestyle, and other domains. Ethics approval for this study was granted by the Conjoint Health Research Ethics Board at the University of Calgary (REB21‐1065). A detailed description of the CAN‐PROTECT study design and procedures has been published previously. 40
Participant Selection
From the initial cohort of 3202 participants, 2338 had completed the neuropsychological test battery at baseline, meeting the prerequisite for access to other study components. Among these participants, those aged <50 years (n = 278), with a diagnosis of MCI (n = 19), and missing data on assessments of daily function (n = 286), or behaviour (n = 41) at baseline were excluded, resulting in a final sample of 1714 participants (Figure 1). Flowchart demonstrating the participant selection process. MBI-C, mild behavioral impairment checklist; MCI, mild cognitive impairment; SAGEA, standard assessment of global everyday activities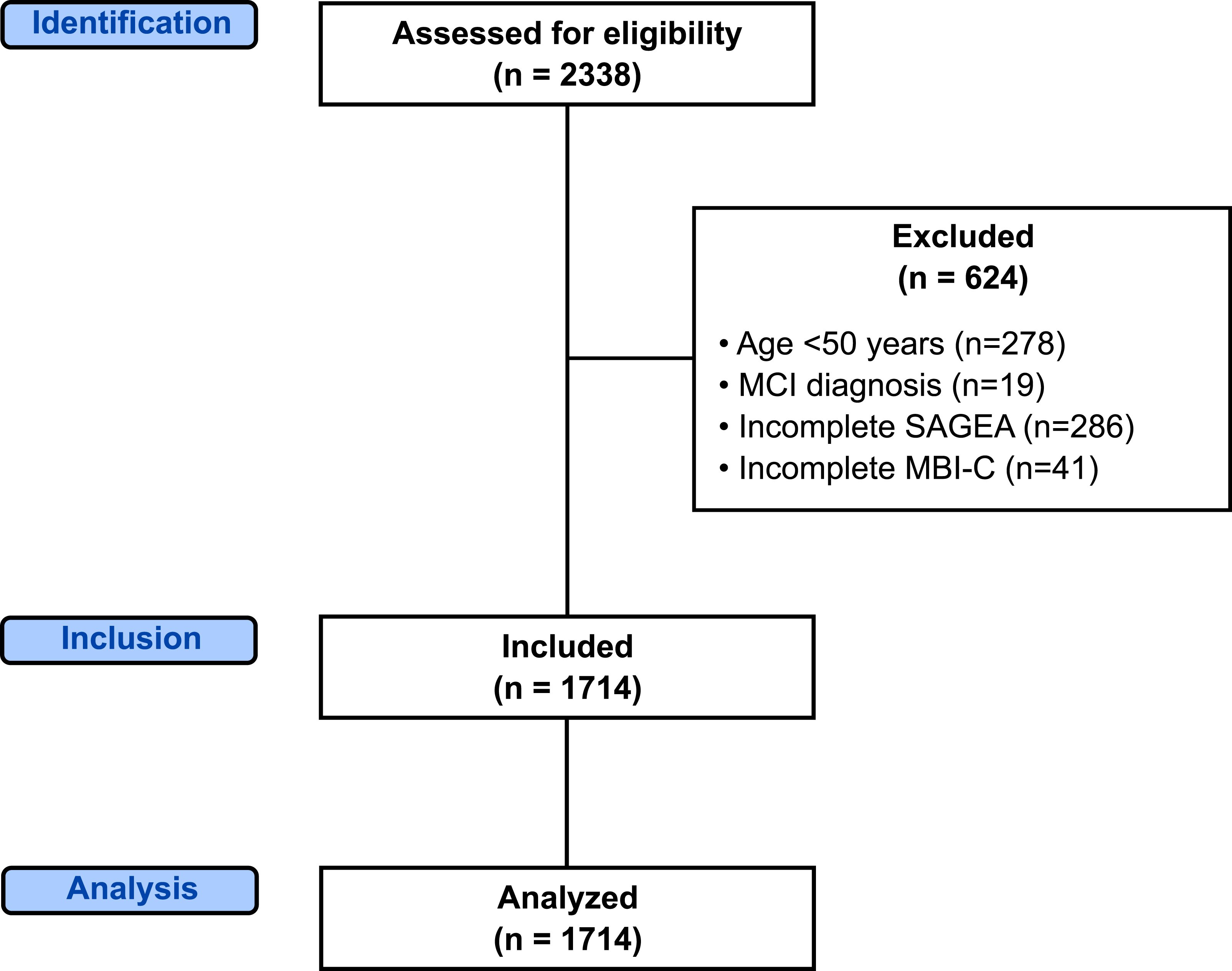
Measures
MBI Operationalization
MBI symptom severity was measured using the self-reported MBI-C 37 . The MBI-C was developed to assess later-life emergent NPS in individuals without dementia, consistent with the International Society to Advance Alzheimer’s Research and Treatment–Alzheimer’s Association (ISTAART-AA) research diagnostic framework for MBI. MBI-C consists of 34 items grouped into five domains: decreased motivation (6 items), affective dysregulation (6 items), impulse dyscontrol (12 items), social inappropriateness (5 items), and abnormal perception/thought content (5 items). For each item, participants first indicated whether the symptom had been present for at least 6 months and was different from their usual long-standing behaviours or past psychiatric conditions, fulfilling the MBI case definition. If endorsed, severity was rated from 1 (mild) to 3 (severe). Domain scores were calculated as the sum of item ratings, and the global score (range 0-104) was obtained by summing across domains. In line with prior work in pre-dementia cohorts, participants with a total score ≥8 were categorized as MBI+.41,42
Daily Function
Daily function in performing ADL was captured using the Standard Assessment of Global Everyday Activities (SAGEA) scale, 43 which evaluates the level of self-reported difficulty in performing ADL over the past month across five domains: (1) cognitive ADL (eg, maintaining attention in conversation, remembering recent events, multitasking), (2) applied cognitive ADL (eg, playing concentration-based games, navigating new environments, organizing trips or social activities), (3) instrumental ADL (eg, managing finances, medications, house chores, transportation, driving), (4) basic ADL (eg, dressing, bathing, toileting), and (5) mobility (eg, walking, using stairs). Each item is scored from 0 (no difficulty) to 3 (severe/stopped due to difficulty). Scores within each domain were summed to generate domain-level scores, which were then summed across all domains to yield an ADL total score (range 0-45), with higher scores indicating greater functional impairment.
Cognition
Cognitive performance was assessed using the CAN-PROTECT neuropsychological test battery, which encompasses the following tests: Trail Making B (visual attention and task switching), Switching Stroop (visual attention and task switching), Self‐Ordered Search (spatial working memory), Paired Associate Learning (visual episodic memory), Verbal Reasoning (general intelligence and grammatical reasoning), and Digit Span (working memory).40,44-46 The total z-score was calculated as the sum of standardized scores across all tests, with higher scores indicating better cognitive performance.
Physical/Sensory Limitations
To help differentiate ADL difficulties related to underlying neurodegeneration from those stemming from physical or sensory impairments, we incorporated the SAGEA questionnaire item asking whether, over the past month, any of the following problems limited the participant’s ability to perform activities (yes/no): physical injury, vision loss, arthritis, unsteadiness, and chronic pain.
Statistical Analysis
All statistical analyses were performed in RStudio version 2024.09.0 + 375 (R version 4.2.2). Sample characteristics included baseline age, sex, education years, neuropsychological test scores, MBI-C total scores, MBI status, total and domain-level SAGEA scores, and presence or absence of physical/sensory limitations to perform ADL. All baseline characteristics were summarized across MBI status groups (MBI+ vs MBI-) using means and standard deviations (SDs) for continuous measures and percentages for categorical measures. For overdispersed continuous measures, medians and interquartile ranges (IQR) were also reported. Group comparisons were conducted using two-sample t-tests for continuous variables and Chi-squared tests for categorical variables. Furthermore, demographic characteristics of participants excluded from the analyses due to missing data were compared with those included to assess potential selection bias introduced by the complete-case analysis approach.
Associations between MBI and SAGEA scores were modeled using negative binomial regression from the MASS package, given the right-skewed distribution of non-negative integer SAGEA scores with overdispersion (ie, variance >mean). Results were reported as count ratios (CR), where the exponentiated coefficients represent relative differences in raw counts, along with 95% confidence intervals (CI) and P-values. Separate models were implemented for global and domain-specific SAGEA scores, and parallel models used MBI status (MBI+ vs MBI-) instead of the continuous MBI total severity score. All models were adjusted for age, sex, education years, neuropsychological test score, and physical/sensory limitations to ADL performance, with statistical significance set at P < 0.05 for hypothesis tests. Although all three domains of cognitive, applied cognitive, and instrumental ADL include tasks that rely on higher-order cognitive processes, the cognitive ADL items–such as remembering recent events, sustaining attention, and task-switching–align closely with abilities measured by neuropsychological testing. Including test scores in these models may therefore introduce over-adjustment. For this reason, we conducted sensitivity analyses excluding the neuropsychological test score in models where cognitive ADL served as the outcome.
Interaction effects between MBI and sex were further examined to explore potential effect modification and identify sex-specific patterns in the associations with ADL outcomes.
Results
Sample Characteristics
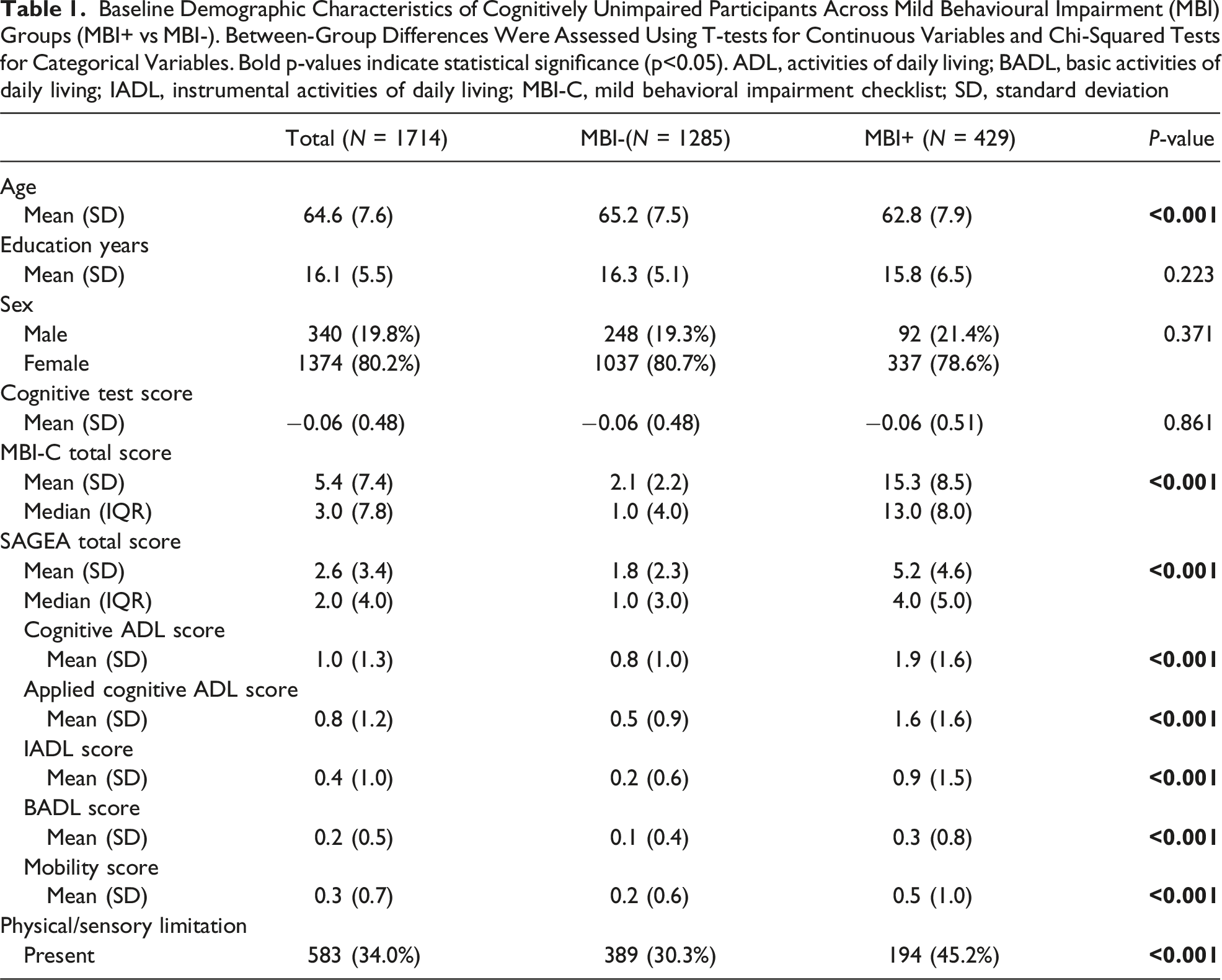
The final sample comprised 1714 CU participants (mean age 64.6 ± 7.7 years; mean education 16.1 ± 5.5 years), of whom 80.2% were females. 25.0% (n = 429) of participants were classified as MBI+, and 75.0% (n = 1285) as MBI-. Compared to MBI- participants, those classified as MBI+ were younger (P < 0.001) and exhibited higher total and domain-specific SAGEA scores across all domains (P < 0.001) (Figure 2). Physical/sensory limitations were also more prevalent in the MBI+ group than MBI- (P < 0.001) (Table 1). No significant differences in demographics were observed between participants included in the analyses and those excluded due to missing data on MBI-C and SAGEA scores (N = 327). Bar plots illustrating the associations between MBI status (MBI+/MBI-) and SAGEA total and domain scores. For each plot, error bars demonstrate 95% confidence intervals. ADL: activities of daily living; BADL, basic activities of daily living; IADL, instrumental activities of daily living; MBI, mild behavioural impairment; SAGEA, standard assessment of global everyday activities Baseline Demographic Characteristics of Cognitively Unimpaired Participants Across Mild Behavioural Impairment (MBI) Groups (MBI+ vs MBI-). Between-Group Differences Were Assessed Using T-tests for Continuous Variables and Chi-Squared Tests for Categorical Variables. Bold p-values indicate statistical significance (p<0.05). ADL, activities of daily living; BADL, basic activities of daily living; IADL, instrumental activities of daily living; MBI-C, mild behavioral impairment checklist; SD, standard deviation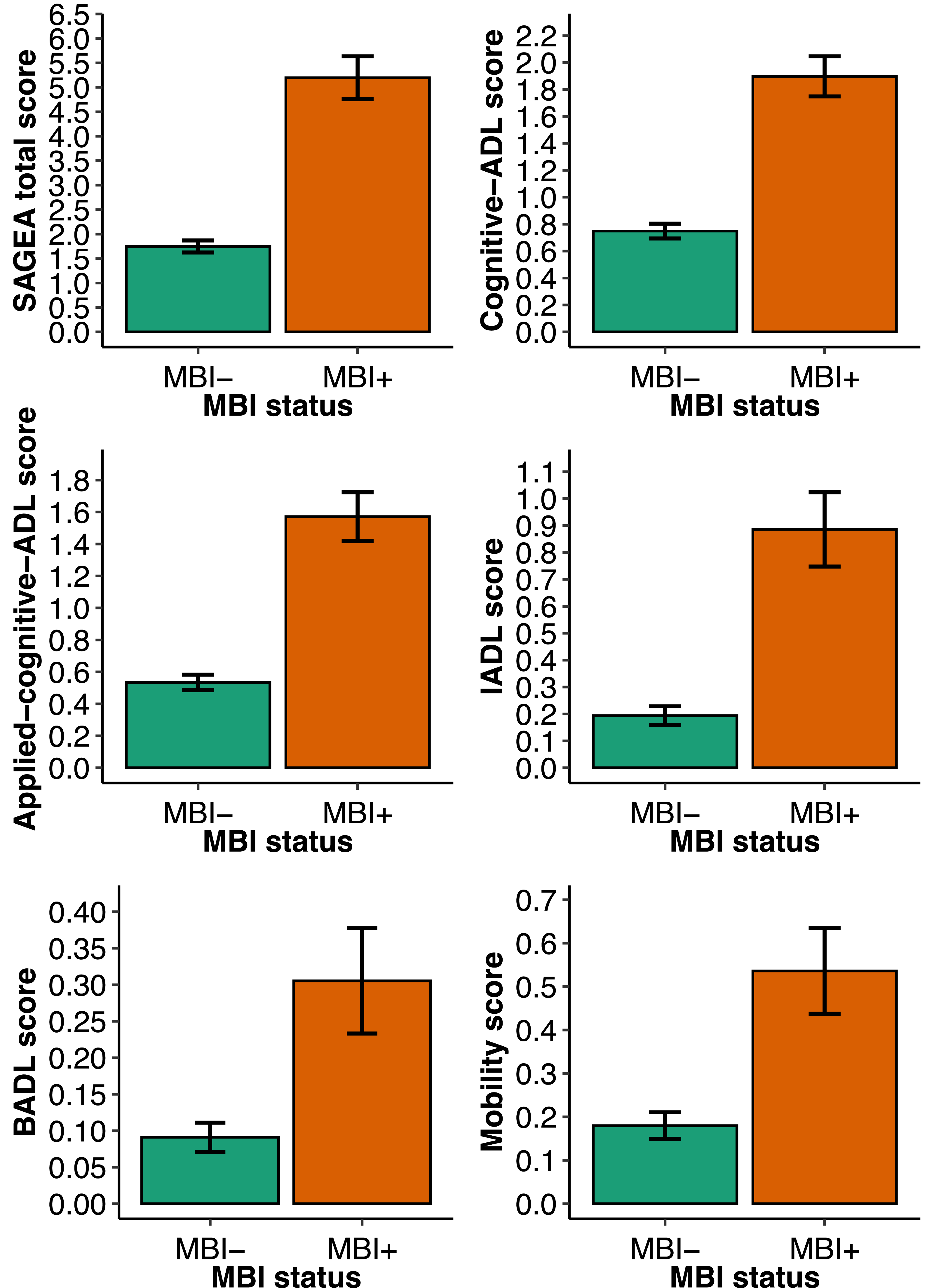
Global ADL and MBI
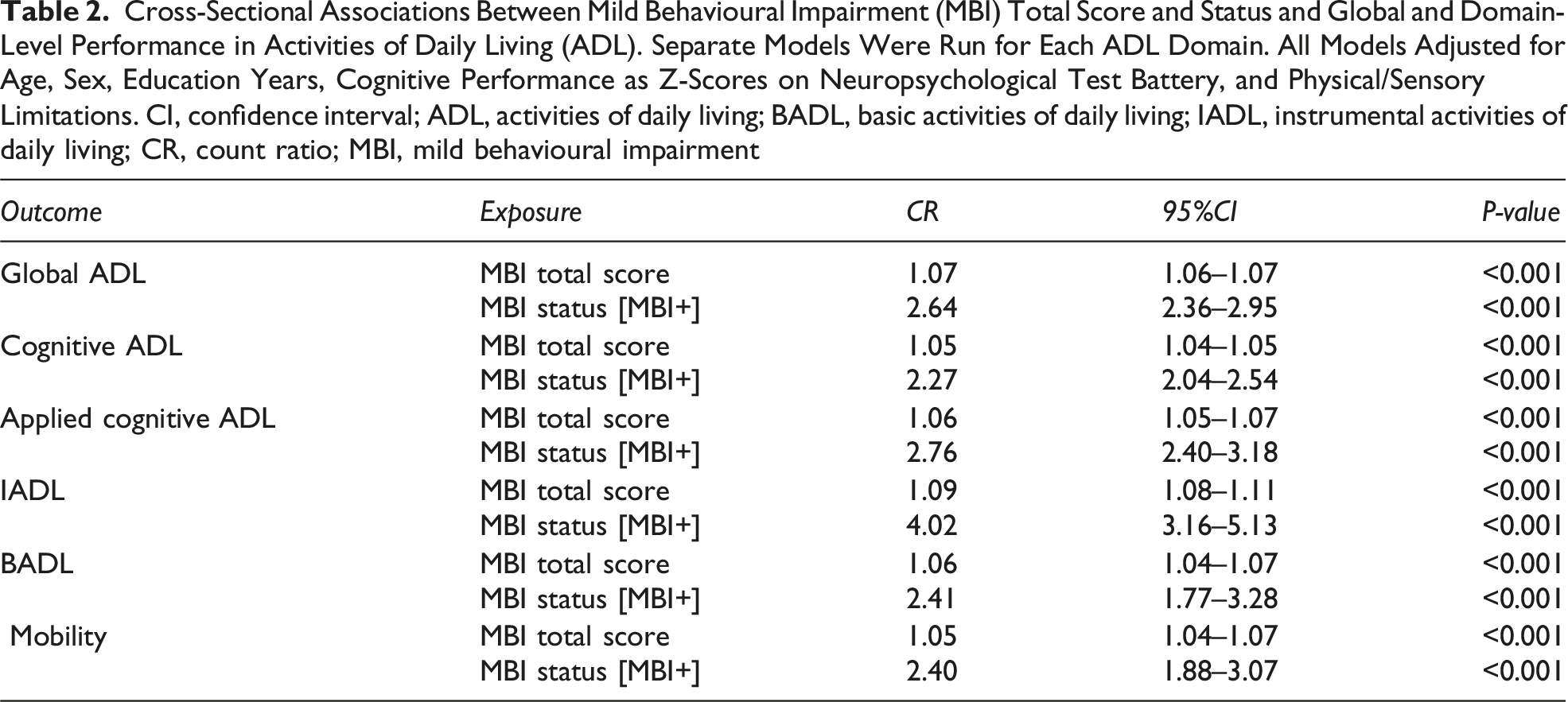
Cross-Sectional Associations Between Mild Behavioural Impairment (MBI) Total Score and Status and Global and Domain-Level Performance in Activities of Daily Living (ADL). Separate Models Were Run for Each ADL Domain. All Models Adjusted for Age, Sex, Education Years, Cognitive Performance as Z-Scores on Neuropsychological Test Battery, and Physical/Sensory Limitations. CI, confidence interval; ADL, activities of daily living; BADL, basic activities of daily living; IADL, instrumental activities of daily living; CR, count ratio; MBI, mild behavioural impairment
Domain-Level ADL and MBI
A one-unit increase in MBI-C total scores was associated with significantly higher impairment scores across all ADL domains: 5% higher cognitive ADL (CR = 1.05, 95%CI: 1.04-1.05, P < 0.001), 6% higher applied cognitive ADL (CR = 1.06, 95%CI: 1.05-1.07, P < 0.001), 9% higher IADL (CR = 1.09, 95%CI: 1.08-1.11, P < 0.001), 6% higher BADL (CR = 1.06, 95%CI: 1.04-1.07, P < 0.001), and 5% higher mobility (CR = 1.05, 95%CI: 1.04-1.07, P < 0.001) impairment. Similarly, in models using MBI status, MBI+ participants had significantly higher domain-specific ADL scores compared to MBI- participants: 2.27 times higher cognitive ADL impairment scores (CR = 2.27, 95%CI: 2.04-2.54, P < 0.001), 2.76 times higher applied cognitive ADL impairment scores (CR = 2.76, 95%CI: 2.40-3.18, P < 0.001), 4.02 times higher IADL impairment scores (CR = 4.02, 95%CI: 3.16-5.13, P < 0.001), 2.41 times higher BADL impairment scores (CR = 2.41, 95%CI: 1.77-3.28, P < 0.001), and 2.40 times higher mobility impairment scores (CR = 2.40, 95%CI: 1.88-3.07, P < 0.001) (Table 2). For the cognitive ADL domain, the sensitivity analysis excluding neuropsychological test scores as a covariate yielded nearly identical results for both the associations with the continuous MBI-C score (CR = 1.05, 95%CI: 1.04-1.06, P < 0.001) and with dichotomous MBI status (CR = 2.30, 95%CI: 2.06-2.57, P < 0.001).
Across other model covariates, better cognitive performance was associated with significantly lower cognitive ADL (CR = 0.85; 95%CI: 0.75-0.96, P = 0.009) and applied cognitive ADL impairment scores (CR = 0.74; 95%CI: 0.63-0.86, P < 0.001), but no associations were observed for IADL (CR = 0.85; 95%CI: 0.65-1.11, P = 0.245), BADL (CR = 1.04; 95%CI: 0.73-1.48, P = 0.836), or mobility (CR = 0.85; 95%CI: 0.64-1.11, P = 0.239) impairment. Physical/sensory limitations were associated with higher impairment scores across all SAGEA domains, with the strongest associations for BADL (CR = 8.17; 95%CI: 5.72-11.93, P < 0.001) and mobility (CR = 7.32; 95%CI: 5.62-9.63, P < 0.001), followed by IADL (CR = 2.20; 95%CI: 1.74-2.77, P < 0.001), cognitive ADL (CR = 1.47; 95%CI: 1.31-1.64, P < 0.001), and applied cognitive ADL (CR = 1.30; 95%CI: 1.13-1.50, P < 0.001). No significant interaction between MBI (continuous or dichotomous) and sex was observed for any ADL domain.
Discussion
In this cross-sectional study of 1714 CU participants, greater MBI symptom burden was strongly associated with higher SAGEA total scores, reflecting greater functional impairment. While the strongest associations were observed for IADL, the associations of MBI persisted across all ADL domains, highlighting the broad relationships between MBI and both complex and basic daily activities. These findings are particularly relevant for emerging therapies, including mAbs, where early identification of individuals with both mild functional and behavioural impairments may be critical for maximizing treatment efficacy.
Several studies have previously demonstrated that NPS are associated with worse ADL performance, although most of the samples comprised of older adults with MCI or dementia. In a cross-sectional study including participants with MCI and AD, NPS were associated with greater BADL and IADL impairments, with stronger effects for BADL in advanced disease and stronger effects for IADL in MCI and moderate dementia. 47 Similarly, another cross-sectional study found higher NPS scores to be associated with worse BADL and IADL performance in AD. 48 Longitudinally, NPS predicted 5-year decline in both BADL and IADL among individuals with AD. 49
At earlier disease stages, findings have been mixed. A memory clinic study of participants spanning normal cognition, MCI, and dementia, found that NPS were associated with worse IADL. 35 Yet, in a cross-sectional study of individuals with subjective cognitive decline, no association between NPS, as measured by the MBI-C, and IADL was observed. 38 In the Mayo Clinic Study of Aging, cross-sectional analyses showed higher Functional Activities Questionnaire (FAQ) total scores to be associated with NPS in participants with either normal cognition or MCI. 34 In longitudinal analyses of the same cohort, baseline NPS were associated with increases in FAQ total scores over time. Notably, stratified analyses by neurocognitive status revealed that this relationship held among CU participants but was not significant in those with MCI. However, the MCI group comprised only 12.5% of the sample and thus estimate imprecision might have accounted for the lack of statistical significance. 36 More recently, a cross-sectional study on CU older adults found an association between higher MBI-C scores and greater IADL impairment, regardless of the source of reports, participants or study partners. 39
Overall, these findings suggest that NPS are meaningfully associated with functional impairment, certainly later on in the disease course, and likely earlier on as well, although informed by only a limited number of studies in CU individuals. The observed variability may reflect limitations in study design or measurement noise due to the use of ADL scales not intended for pre-dementia populations. These scales may not be sufficiently sensitive to detect subtle functional changes. Furthermore, the latest research indicates that, analogous to MBI criteria capturing the natural history of NPS, accounting for the natural history of functional difficulties also provides a more accurate representation of the underlying neurodegenerative disease.29,30 Thus, accounting for new-onset and persistence of changes in function may enrich the sample for those with AD proteinopathies in the early stages of disease, and who are more likely to progress to dementia. Aside from ADL, most studies measured NPS using scales with a short reference period, and little attention to natural history of NPS, potentially introducing noise.
Importantly, the operationalization of MBI criteria allows for the identification of older adults at particularly high risk for cognitive decline and dementia. MBI has been consistently associated with accelerated cognitive decline, increased dementia risk,8,10-12,50 and pathological markers of AD, including abnormal amyloid-beta and tau biomarkers (eg, total tau, p-tau181, and p-tau217),13,15-18,51 as well as structural brain changes such as hippocampal atrophy and cortical thinning.20,21,23,52 This body of evidence supports the utility of MBI as a valuable tool for risk stratification in preclinical populations, highlighting its relevance for both research and potential early intervention strategies. So far, few studies have explored the associations between MBI and ADL, but findings have been mixed. A recent cross-sectional study of CU individuals reported a significant association between higher MBI-C scores and greater IADL impairments. 39 However, another study that used the MBI-C in a sample of participants with subjective cognitive decline, found no link between NPS and IADL, but only unadjusted pairwise correlations were examined. 38 Another recent study of CU participants and those with MCI operationalized MBI from the neuropsychiatric inventory questionnaire (NPI-Q) based on published algorithms and found that higher MBI total and domain scores were associated with higher FAQ scores, indicating greater functional impairment. However, this study likewise did not appear to account for covariate adjustments. 53
Our findings add to the limited body of literature on the association between NPS and functional impairment in CU individuals. We leveraged the MBI-C to capture later-life emergent and persistent NPS that represent a sequala of the underlying neurodegenerative disease process. Notably, by examining ADL domains separately, our analyses provided a more nuanced understanding of how MBI relates to distinct aspects of daily functioning, from basic self-care to more complex instrumental activities. Interestingly, while MBI was significantly associated with decline across higher-cognitive domains, MBI associations extended to basic ADL and mobility domains as well, which are traditionally thought to be preserved in CU individuals. Across all ADL domains, IADL were most strongly associated with the presence of MBI, consistent with evidence that early functional changes often first manifest in more complex activities, preceding declines in cognition and basic self-care activities.25-28 Our findings highlight that higher-order daily activities encompassed in IADL are particularly sensitive to the same conditions associated with early behavioural changes. Thus, both behaviour and function signal elevated dementia risk and underlying neurodegeneration.
Monitoring IADL performance in CU individuals could offer a practical approach for early detection of emerging neurodegenerative changes, enabling timely interventions aimed at preserving independence and optimizing the potential benefit of emerging therapies, including mAbs. To maximize this potential, further research should refine and validate IADL assessment instruments tailored to preclinical populations, ensuring they capture subtle, disease-related changes with sufficient sensitivity and specificity. Further, most existing IADL assessment scales fail to appropriately account for the natural history of functional decline. Similar to NPS assessment, where MBI improves accuracy by using a longer reference frame (6 months) to capture persistent symptoms, IADL measures may also be enhanced. By adopting extended time frames, sustained functional impairments are more likely to indicate underlying disease.29,30
Importantly, in our study, the strong associations between MBI and global and domain-level ADL persisted despite adjusting for cognitive performance and physical/sensory limitations, demonstrating that MBI captures functional vulnerability beyond what is explained by cognition or somatic health. Cognitive performance independently accounted for the greatest variability in cognitive and applied cognitive ADL domains, while physical/sensory limitations strongly influenced BADL and mobility. Yet, the association with MBI remained significant across these ADL domains, highlighting the broad relationship between MBI and daily functioning. Later-life emergent and persistent NPS reflect underlying neurobiological changes that may independently contribute to difficulties in daily functioning, thus serving as a disease marker. 52 Past studies have reported that NPS contribute to functional impairment in early- and late-stage AD,54,55 suggesting that emergent behavioural symptoms may precede functional decline. Thus, MBI may serve as a clinically useful marker for emerging functional vulnerability, potentially preceding measurable cognitive decline. Although evidence for the reverse direction (ie, functional impairment leading to NPS) is limited, it remains possible that emerging functional difficulties could in turn exacerbate behavioural symptoms through increased frustration, loss of autonomy, or reduced engagement. Both behavioural and functional changes may also reflect shared underlying neurodegenerative processes and, when accurately captured, can both serve as early markers of dementia. Multiple studies have demonstrated associations between MBI and AD-related biomarkers in dementia-free populations.13,14,18,20 While the evidence is more limited for functional difficulties, several studies indicate associations between IADL impairment and AD-related biomarkers in these populations. Notably, studies in CU older adults have found significant associations between IADL difficulties and smaller hippocampal volumes, weaker brain network connectivity, 56 and greater amyloid burden. 25 Thus, both behavioural and functional changes may emerge from the underlying pathology. Due to the cross-sectional design of our study, the direction of the association between MBI and functional impairment cannot be determined here. Our findings demonstrate associations but not causations, highlighting the need for longitudinal studies assessing both behaviour and function alongside AD biomarkers to clarify these interrelationships.
The absence of significant MBI by sex interactions in our study might suggest that the impact of MBI on daily functioning may be broadly similar in males and females. However, given that about 80% of our sample was female, these findings should be interpreted with caution. The overrepresentation of females may have limited our ability to detect sex-specific differences, and thus the apparent similarity in functional consequences cannot be considered conclusive. Sex differences have been observed in the prevalence of certain NPS and associations with cognitive decline, 57 which might impact daily functioning differently. Future studies with more balanced samples across sex are required to determine whether the relationship between MBI and daily functioning truly generalizes across both groups or whether subtle sex-specific effects emerge when sample distributions are more even.
Limitations of this study include its cross-sectional design and reliance on self-reported measures of ADL and MBI, which may be subject to reporting bias. Future longitudinal studies are warranted to clarify the directionality of the relationship between MBI and functional decline and to investigate the mechanisms underlying both. CAN-PROTECT also collects study partner–reported SAGEA and MBI-C data, though the current sample size is limited. As the cohort expands, future analyses could leverage these reports to replicate our findings. Future studies should also investigate the association of individual MBI domains with ADL and its domains, as different behavioural domains may be differentially associated with aspects of daily functioning. Another important consideration is that MBI criteria specify that individuals should generally maintain independence in daily functioning, with minimal assistance. 37 As our sample comprised CU older adults, this criterion may have limited the range of functional impairment observed, potentially constraining observable associations between MBI and ADL performance. The requirement for preserved independence in the MBI construct is intended to capture behavioural change prior to overt loss of function as a sign of dementia. Future studies using more sensitive or longitudinal measures of everyday function may better detect subtle changes that occur within the bounds of MBI. Recent work suggests that, mirroring the MBI approach to NPS, capturing persistent functional difficulties over time may provide a more sensitive measure of early functional decline and identify individuals at greater risk for progression and AD-related pathology.29,30 Thus, better characterizing and defining the mild functional impairment at early disease stages can help frame the research agenda in this field. Enhancing the sensitivity of functional assessment tools could also help more accurately characterize the relationship between functional decline and MBI. Nonetheless, future iterations of the MBI criteria will need to consider the emerging evidence on functional impairment in CU individuals. Despite these limitations, our findings highlight the relevance of MBI as an early indicator of functional vulnerability and support the utility of assessing both behavioural and functional changes in preclinical populations.
Despite these limitations, our findings highlight the potential of combining behavioural and functional assessments as early indicators of neurodegenerative risk. By examining ADL domains separately, our study provides a more nuanced understanding of how MBI relates to daily functioning, from basic self-care to more complex instrumental activities. Incorporating subtle functional impairment alongside MBI may help identify an even higher-risk group for incident cognitive decline and dementia, offering a promising avenue for early detection and targeted interventions. Early identification of such high-risk individuals is particularly critical in the context of emerging therapies, including mAbs, where therapeutic efficacy is thought to be greatest before substantial cognitive decline occurs. 3 Importantly, assessing both behavioural and functional markers is simple, accessible, and cost-effective, and can even be conducted remotely, increasing feasibility for broad clinical and research use. Integrating such practical assessments into routine clinical evaluations could therefore not only improve risk stratification but also guide the timing and selection of interventions aimed at slowing or preventing disease progression.
Footnotes
Ethical Considerations
The Conjoint Health Research Ethics Board at the University of Calgary Ethics provided approval for CAN‐PROTECT (REB21‐1065).
Consent to Participate
All participants provided informed consent.
Author Contributions
All authors contributed to data analysis, interpretation, and manuscript preparation. MG and ZI conceived and designed the study. MG led data preparation, conducted the analyses, and drafted the initial manuscript. DG made substantial contributions to data preparation. DG, CB, BC, AC, EP, ES, and ZI provided critical input on the interpretation of findings. All authors had full access to the study data, participated in revising the manuscript, and approved the final version for submission.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: CAN‐PROTECT was supported by Gordie Howe CARES and the Evans Family fund via the Hotchkiss Brain Institute. ZI is supported by the Canadian Institutes of Health Research (BCA527734), Gordie Howe CARES, and the UK National Institute for Health and Care Research Exeter Biomedical Research Centre. The funding sources had no involvement in study design, data collection, analysis, or interpretation, nor in the writing of the manuscript or in the decision to submit for publication.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Z.I. has served as a consultant/advisor for Eisai, Lilly, Lundbeck/Otsuka, Novo Nordisk, and Roche. E.S. has provided consulting (unpaid) to Alnylam, Eisai, and Lilly. Other authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Due to the confidential nature of participant demographic health data, CAN-PROTECT study data are not publicly available on a data repository. However, individual access to the data may be provided upon reasonable request to the corresponding author.