
Abstract
Purpose:
Previous studies have demonstrated the feasibility of bedside placement of ureteral stents in cases of acute ureteral obstruction. However, there is a lack of evidence comparing its efficacy to traditional stent placement in the operating room with fluoroscopy. We compared the clinical outcomes of bedside ureteral stent placement with the current standard of care.
Methods:
A retrospective cohort study included patients with acute obstructive pyelonephritis from July 2023 to July 2024. Exclusion criteria included patients not requiring hospital admission, absence of obstructing ureteral calculi, and absence of sepsis criteria. Baseline demographics, including the degree of sepsis and stone characteristics, were measured. Outcomes included time to decompression, successful stent placement, and hospital duration.
Results:
A total of 55 patients were included, of which 17 underwent bedside ureteral stenting and underwent operative stent placement. No significant differences were found in baseline demographics, sepsis criteria measures, stone characteristics, or degree of hydronephrosis between the groups. Patients in the bedside group had reduced time to stenting (216.0, Q1–Q3: 4.5–408.5 minutes vs 319.0, Q1–Q3: 174–792 minutes, p = 0.040) and achieved higher rates of urine aspirate retrieval (100% vs 76%, p = 0.028) compared with the operating theater group. There were no statistically significant differences in the stent success rates (100% vs 95%, p = 0.344) or complication rates (0% vs 3%, p = 0.500) between the two groups.
Conclusions:
Bedside stent placement offers faster source control and reliable urine aspirate retrieval while maintaining comparable success and complication rates to stenting in the operating theater for patients with obstructive pyelonephritis.
Introduction
Obstructive pyelonephritis or “septic stone” is an acute urologic emergency associated with significant mortality and morbidity if left untreated. 1 Timely renal decompression is critical in the management of obstructive pyelonephritis, either with nephrostomy tube insertion or retrograde ureteral stent insertion. Stent insertion allows for patient stabilization and prevents further complication. Although traditionally performed in an operative environment with fluoroscopy and under general or regional anesthesia, this procedure has also been explored under local anesthesia alone and with adjunctive analgesia and anxiolysis. Ureteral stent placement under ultrasound guidance has been further adopted at our institution, proving to be a safe and feasible option, and several studies have found this approach to successfully alleviate blockage in 70%–100% of patients. 2,3
In the case of acute ureteral septic stones, decompression beyond 48 hours of admission yielded significantly worse patient outcomes when compared with early decompression. 4 In the Canadian context, access to operating room time for performing emergency cases can be challenging. This is especially true in high-volume trauma centers managing many urgent and emergency cases. As a result, delays in upper tract decompression may occur and have been associated with up to 29% increase in mortality. 5 Canadian data suggest that up to 20% of emergency cases experience delays in timely intervention. 6 Delays may also be attributed to the “weekend effect,” caused by limitations in staffing and perioperative resources. 7 Anecdotal evidence from our center, that has widely adopted bedside stenting, suggests that this approach may allow for more expedient time to decompression. However, to date, ultrasound-guided ureteral stent placement is yet to be compared with the standard fluoroscopy-guided approach.
This study aimed to compare the time with upper urinary tract drainage, hospital stay duration, and clinical outcomes of bedside ureteral stent placement without fluoroscopy with the clinical standard of care. We hypothesized that patients presenting with acute obstructive pyelonephritis undergoing ureteral stent insertion at the bedside will have a shorter time to upper urinary tract drainage, shorter hospital stay, and lower mortality when compared with traditional stent placement with fluoroscopic guidance.
Materials and Methods
A retrospective cohort study was performed on patients who underwent ureteral stent insertion for all patient admissions coded for septic stone, obstructing pyelonephritis, or urosepsis at two tertiary care centers. This study was approved by the University of Manitoba Health and Research Ethics Board (HS26677).
Study population and data collection
All patients underwent ureteral stent insertion for obstructive pyelonephritis between July 23 and July 2024 at either of two hospitals, Health Sciences Center and St. Boniface Hospital, in Winnipeg, Manitoba, Canada. Patients were included if they met all the following inclusion criteria: (1) having undergone traditional ureteral stent insertion (in an operating room or in a procedural room under fluoroscopic guidance), bedside ureteral stent insertion in the emergency department, or in an inpatient bed using our previously published procedural protocol, which utilizes point-of-care ultrasound to confirm wire placement 3 ; (2) underwent ureteral stent insertion for sepsis defined as two or more systemic inflammatory response syndrome (SIRS) and/or positive urine culture; and (3) having obstructive ureteral calculi identified on cross sectional imaging (computed tomography scan). Patients were excluded if their stay at the hospital did not involve admission or if they had missing key baseline demographics. Patient baseline demographics included age, setting of stent insertion, sex, Charlson Comorbidity Index (CCI), number of Systemic Inflammatory Response Syndrome criteria, Quick Sequential Organ Failure Assessment (qSOFA) score, maximum recorded temperature (Tmax), white blood cell count on bloodwork, stone characteristics (size, laterality, and location), and degree of hydronephrosis (mild, moderate, or severe). Clinical outcomes included time to upper tract drainage (defined as the time from urologic consultation to ureteral stent placement), successful stent placement (defined by post-procedure X-ray kidney–ureter–bladder), complications (as defined by Clavien–Dindo Classification), whether urine aspirate was successfully obtained, and the duration of hospital stay.
Data analysis
All the data were collected in an anonymized fashion and managed using an encrypted file. Descriptive statistics were used for baseline demographic and clinical outcome data, namely, means and standard deviations, where appropriate. A Shapiro–Wilk test was used to assess for normal distribution among baseline demographics and clinical outcomes. Non-parametric data underwent Mann–Whitney U test for significance (p < 0.05) and results are listed using median and quartiles. Parametric outcomes were assessed for statistical significance using Fisher’s exact test, with a significance level of p < 0.05. For clinical outcomes, differences between cohorts were examined using an independent t-test, with statistical significance set at p < 0.05. Statistical analyses were performed using Statistical Package for the Social Sciences software.
Results
From July 2023 to July 2024, we initially identified 97 patients who underwent ureteral stent insertion for a presumed diagnosis of septic stones, obstructing pyelonephritis, or urosepsis. Of these, 55 were ultimately included in the analysis after the inclusion and exclusion criteria. Patient enrolment is further described in Figure 1 following the Strengthening the Reporting of Observational Studies in Epidemiology guidelines. Seventeen patients underwent bedside ureteral stenting (BS), whereas 38 underwent ureteral stent insertion in the operating theater with fluoroscopy (tS). The mean age was 64.1 ± 16.4 years in the BS group and 61.8 ± 16.1 in the tS group (p = 0.641). Sex distribution was similar between groups, with 11 (65%) females in the BS group and 24 females (63%) in the tS group (p = 0.909). Comorbidities, as measured by the CCI, were comparable, with patients in the BS group scoring a median of 3.0 (Q1–Q3: 1–5.5) points compared with 3.0 (Q1–Q3: 1–4) points in the tS group (p = 0.227). The patient demographics are presented in Table 1.
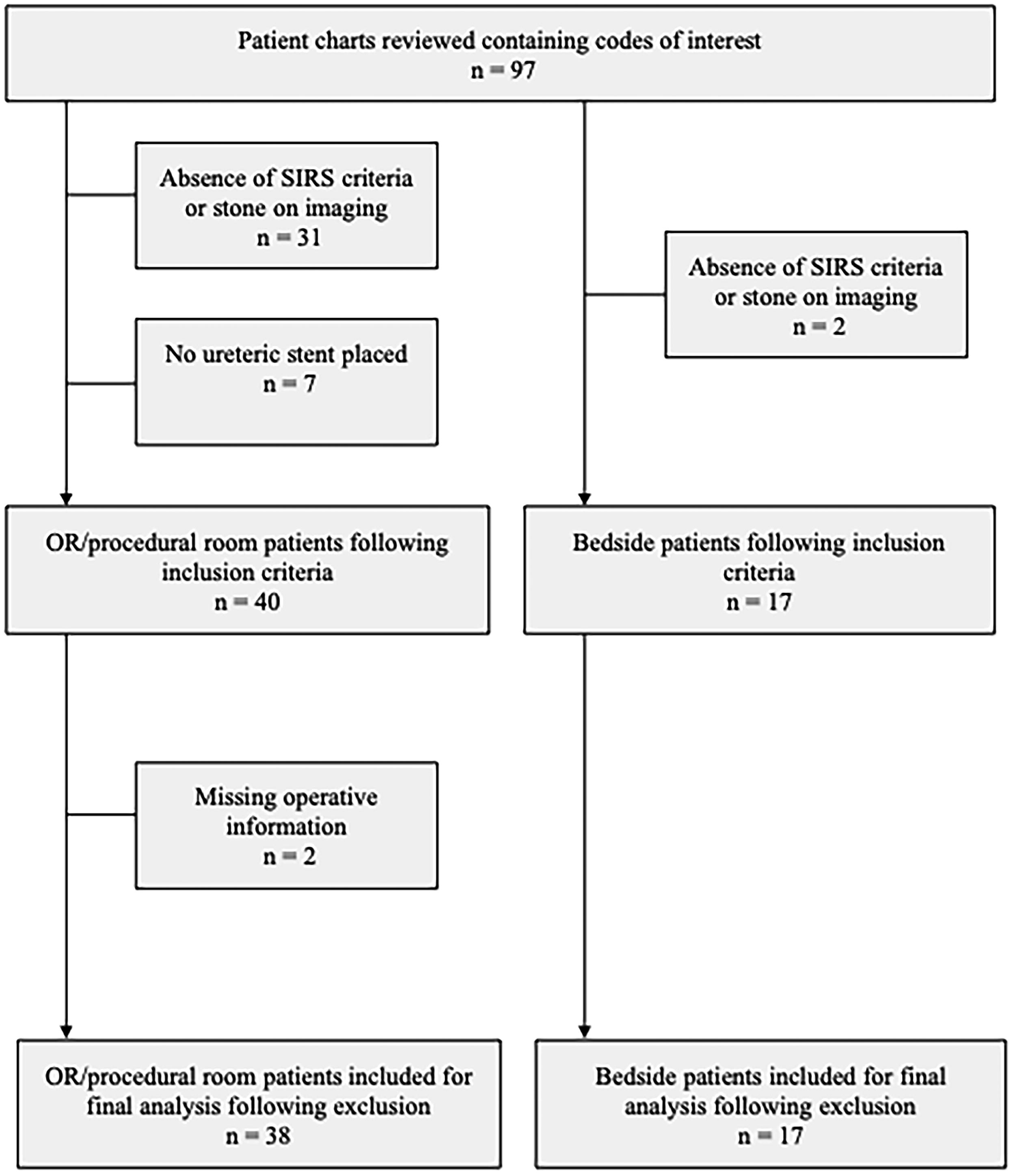
STROBE guideline of included and excluded patients. STROBE = Strengthening the Reporting of Observational Studies in Epidemiology.
Baseline Demographics, Stone Characteristics, and Degree of Hydronephrosis across Both Modalities of Ureteral Stenting
CCI = Charlson Comorbidity Index; qSOFA = Quick Sequential Organ Failure Assessment; SIRS = systemic inflammatory response syndrome; Tmax = maximum recorded temperature; WBC = white blood cells.
There were no significant differences in sepsis parameters between the groups, as measured by the qSOFA score, SIRS criteria, Tmax, and white blood cell count. The median qSOFA scores were 1.0 (Q1–Q3: 0–2) in the BS group and 0.0 (Q1–Q3: 0–1) in the tS group (p = 0.238). The BS cohort had a median of 2.0 (Q1–Q3: 1–3) SIRS criteria compared with 2.0 (Q1–Q3: 2–3) criteria in the tS group (p = 0.740). Tmax on presentation was 37.8 ± 0.9 degrees Celsius in the BS group and 37.5 ± 1.3 degrees Celsius in the tS group (p = 0.387). White blood cell count was 16.1 ± 8.9 × 109 cells/L in the BS group and 17.7 ± 6.3 × 109 cells/L in the tS group (p = 0.472).
The urinary stone characteristics were comparable between the groups regarding size, ureteral location, and degree of hydronephrosis. The average stone size in the BS group was 7.4 ± 3.3 millimeters and 7.61 ± 3.8 millimeters in the tS group (p = 0.873). The location of the obstructing stone did not differ significantly between the two groups (p = 0.297), with approximately half of all patients presenting with proximal ureteral obstruction. The degree of hydronephrosis was also not significantly different between the BS and tS groups (p = 0.831). Stone characteristics can be seen in Table 1.
The rates of successful stent placement (as defined by radiographical confirmation of proper stent placement) were similar between cohorts, with 100% (n = 17) of stents placed successfully in the BS group and 95% (n = 36) in the tS group (p = 0.344). Two patients in the tS group underwent interventional radiology percutaneous nephrostomy tube placement after failed retrograde ureteral stent placement. The median time between presentation and stent placement was significantly shorter in the BS group (216.0, Q1–Q3: 124.5–408.5 minutes) than that in the tS group (319.0, Q1–Q3: 174–792 minutes), p = 0.040. The urine aspirate retrieval rate was significantly higher in the BS group (100%, n = 17) than in the tS group (76%, n = 29), p = 0.028. The length of patient stay was not significantly different between groups, with patients undergoing bedside stenting staying for a median of 4.0 (Q1–Q3: 2–14) days and patients in the tS group staying for 5.0 (Q1–Q3: 4–11) days, p = 0.551. Outcomes between groups can be seen in Table 2.
Clinical Outcomes across Both Modalities of Ureteral Stenting
Statistical significance.
The BS group had no complications, whereas the tS group had one (3%) complication related to stent insertion (p = 0.500). This complication was a small, non-drainable perinephric abscess that was successfully treated after discharge with intravenous antibiotics through the Manitoba Community Intravenous Program. The average resident training year at the time of the stent placement was significantly higher in the BS group with an average of 3.25 ± 0.58 years compared with 2.62 ± 1.00 years in the tS group (p = 0.0075).
Discussion
Our study demonstrated that bedside ureteral stent insertion in patients with septic obstructive urolithiasis is both safe and effective. Since implementing this approach at our institution, we observed a significantly shorter time to urinary tract decompression from presentation in the BS cohort compared with the current standard of care. Importantly, the success rates were comparable between the two groups, in the absence of any significant differences between patient comorbidities, degrees of sepsis, and stone characteristics. This suggests that bedside stenting can be considered as a first-line option for suitable candidates, potentially reducing delays in definitive management without compromising patient outcomes. These findings have important implications for clinical practice, particularly in high-volume trauma centers or during weekend call coverage, where there may be limited staffing and perioperative resources for urologists.
Patients who underwent bedside ureteral stent placement had significantly shorter times to upper tract decompression than those who did not. In current literature, timely decompression of obstructive pyelonephritis has been shown to decrease both in-hospital mortality and length of hospital stay, highlighting the importance of prompt management. 5,8 The benefits of bedside ureteral stenting are amplified within the context of the Canadian public health care system and its limited perioperative resources. Delays in urgent and emergent surgical interventions are prevalent throughout North America at high-volume trauma centers that have a high case load of surgical emergencies. The ability to provide timely care independent from the operating room is particularly valuable in mitigating the “weekend effect,” where limited resources may otherwise delay patient management. 7 Despite the difference in time to stent placement between the two groups having been statistically significant, further investigation is needed to determine its impact on clinical outcomes. However, in a pathology associated with significant mortality and morbidity in the absence of timely decompression, we believe that there may be some clinical benefit with early renal decompression that was not reflected in the present study.
Interestingly, in the BS cohort, two patients had stents inserted after a delay of 10 hours or more. In these two cases, the initial assessment was first completed by a junior, first-year resident who was on call, later being followed by bedside stent insertion by a well-trained senior resident. These delays in intervention can be attributed to the lack of training of the on-call junior residents, underestimating the benefit of the bedside technique in timely decompression. This is further reflected in the higher average resident training level seen in the BS cohort than in the tS cohort, suggesting that earlier hands-on training in this skill may yield some merit.
Our bedside technique for ureteral stenting demonstrated similar success rates, complication rates, and length of hospital stay compared with the traditional operative group. These success rates were comparable to those of a previous study by our group, in which a series of 28 patients who underwent bedside ureteral stenting also had a success rate of 100 percent. 3 Previous studies on traditional ureteral stent placement for intrinsic ureteral obstruction by Wenzler et al. and Yossepowitch et al. showed success rates of 88% and 94%, respectively, which is comparable to the 95% success rate observed in our cohort. 9,10 Additionally, our bedside technique was found to be more reliable in obtaining urine aspiration for culture and susceptibility testing when compared with the operative theater group. It should be noted, however, that all patients underwent traditional urine culture testing prior to their procedures. This does not necessarily indicate that the traditional method is inferior in terms of obtaining urine aspirates. Instead, the observed differences may be attributed to factors such as the omission of culture sampling, time constraints in urgent situations, or variability in ureteral stent insertion techniques among urologists. As previously described by Chung and Ramjiawan, our bedside technique utilizes ureteral catheterization with a 5 French flexible ureteral catheter to detect hydronephrotic drip, confirming proper catheter tip placement proximal to the obstructing stone. 3 Our approach may allow easier integration of urine culture collection into the procedural workflow which could account for the difference in recorded urine aspiration rates. At a minimum, this finding demonstrates that bedside stent placement is not inferior in obtaining upper tract urine cultures when compared with traditional aspiration techniques that are employed in the operating room.
We observed no significant differences in either mortality rates or length of hospital stay between the groups, demonstrating that bedside stenting is non-inferior to the traditional approach in these critical outcomes. Moreover, both approaches managed similar levels of sepsis severity and case complexity, further validating the comparability of the two techniques. However, it is important to acknowledge that detecting differences in mortality and complications may be challenging because of the relatively low event rates typically seen with obstructive pyelonephritis. 9 Nevertheless, we can reasonably infer that the faster drainage times and comparable success rates observed with bedside stenting may translate into benefits, such as reduced mortality and morbidity, as prompt decompression in obstructive pyelonephritis is crucial for preventing septic complications. 8 Although our study was not powered to definitively prove this benefit, it provides a strong rationale for further investigation through a larger scale multi-institutional study.
This study is not without its limitations. First, patient tolerability of the bedside stenting procedure was not formally assessed. Although anecdotal experience from the residents performing the procedures suggested that the procedure was generally well tolerated, a systematic assessment of patient comfort and satisfaction would have provided valuable insights. Second, our institution has a unique system at the Winnipeg Health Sciences Center, which includes access to a urologic procedure suite outside the main operating room. In this suite, we have access to conscious sedation, fluoroscopy, nursing staff, and endoscopic urologic instruments which we utilize to circumvent the operating theater backlog. Patients brought to our procedure suite were included in the tS group, possibly leading to an underestimation of the difference in the time to drainage between groups. Third, patients who were deemed eligible for bedside stent placement were selected based on anecdotal assessment of clinical factors such as stone location, size, and other anatomical factors. This may have led to a selection bias, which would have overestimated our success rates. Because of the retrospective nature of our study, it is difficult to accurately identify the criteria used to determine selection for bedside ureteral stenting, although, when referencing our prospective database of ureteral stenting, almost all patients were offered bedside stenting considering hemodynamic stability and on-call resident comfort with the procedure. Further investigation with randomized clinical trial would be warranted to minimize this bias. Fourth, we were unable to evaluate post-stent complications such as ureteral stricture rate because of the lack of follow-up data on ureteroscopies performed for subsequent definitive stone management. Lastly, although our data are promising, the generalizability of our findings may be limited by our single-institution experience and relatively small sample size. This was partially because of our selective inclusion criteria for determination of a “septic stone,” for which there is no widely accepted definition in the literature, to minimize selection bias. To address these limitations and further validate the efficacy, safety, and tolerability of bedside stenting, future research should focus on larger prospective, multi-institutional studies including randomized clinical trials, quantifying long-term outcomes such as ureteral stricture rate, along with formalizing the definition of this condition. In addition, our group is working to develop and implement a formalized training program using a standardized approach, which could enhance the reproducibility of our results. Such initiatives, combined with more extensive research, may pave the way for bedside stenting to become a more widespread option, potentially leading to significant reductions in the time to drainage for patients with obstructive pyelonephritis with the added benefit of reducing health care costs.
Conclusion
Bedside ureteral stent placement is a safe and reliable method for urinary decompression in patients with obstructive pyelonephritis secondary to urinary stones. Bedside stenting was associated with faster decompression times and consistent urine aspirate retrieval. Further, larger-scale studies are required to confirm whether the benefits of bedside stenting translate to improve patient outcomes, such as morbidity, mortality, and hospital length of stay, while decreasing health care costs.
Footnotes
Authors’ Contributions
S.D., D.C., P.P., and G.H. contributed to the design and implementation of the research. S.D., D.C., and K.X. analyzed the results. S.D., M.F., R.R., and D.C. contributed to the writing of the article. D.C. and P.P. conceived the original and supervised the project.
Ethical Compliance
This study was approved by the University of Manitoba Health and Research Ethics Board (HS26677).
Author Disclosure Statement
P.P. has been an advisory board member for Boston Scientific as well as has received a grant/honoraria from Endo Pharmaceuticals and participated in a clinical trial supported by Zenflow. The remaining authors do not report any competing personal or financial interests related to this work.
Funding Information
The authors received no financial support for the research, authorship, and/or publication of this article.