
Abstract
Objectives:
To clarify disease behavior and oncological outcomes as well as the need for ureteroscopy (URS) implementation in patients with clinically suspected upper tract carcinoma in situ (UT-CIS).
Patients and Methods:
In this multi-institutional study, we retrospectively analyzed patients who met three criteria for clinically suspected UT-CIS between 2008 and 2018: positive high-grade cytology from the upper tract, absence of a solid upper tract lesion on imaging, and negative bladder biopsy. Patients who underwent URS were compared with those who did not. Kaplan–Meier curve was used to assess the natural history of treated UT-CIS and the prognostic impact of URS.
Results:
In total, 48 patients with clinically suspected UT-CIS were analyzed, of whom 27 (57%) had a previous history of urothelial carcinoma. Of 28 (58%) patients who underwent URS, pathologically confirmed UT-CIS and UT-non-CIS were detected in 7 (25%) and 6 (21%), respectively. As initial treatment, 23 (48%) patients received upper tract bacillus Calmette–Guérin, while 21 (44%) underwent radical nephroureterectomy (RNU). During a median follow-up of 44.8 months, the most common site that suffered recurrence and progression was the bladder (40% and 17%), followed by the affected (15% and 6%) and contralateral (8% and 4%) upper tract, respectively. Three-year overall, cancer-specific, upper tract-specific, progression-free (PFS), and recurrence-free survival estimates were 88.2%, 94.8%, 100%, 80.8%, and 52.4%, respectively. Survival outcomes were comparable regardless of URS implementation, with the exception of PFS. However, URS implementation resulted in an earlier transition to surgical intervention in 11% and avoided unnecessary RNU in 11%.
Conclusions:
UT-CIS is a pan-urothelial disease and frequently shows metachronous recurrence and progression in any part of the urinary tract, necessitating long-term, meticulous follow-up. Despite the lack of a statistical difference between patients with and without URS, we found that a non-negligible number of patients benefited from URS implementation.
Introduction
Isolated upper tract carcinoma in situ (UT-CIS) is a flat lesion and lacks distinct visualized tumors, generally distinguished from concomitant UT-CIS, which presents as a CIS lesion accompanied by other papillary/nodular tumors. 1 Concomitant UT-CIS has been found to have a prognostic value in patients with upper tract urothelial carcinoma (UTUC) submitted to radical nephroureterectomy (RNU), with an incidence of 26.7% in 1387 patients with UTUC.2,3 In contrast, the incidence of isolated UT-CIS was much lower, ranging from 2% to 4%,4–6 and survival outcomes in previous studies have been reported with varying results. Retrospective data from 55 consecutive patients receiving antegrade bacillus Calmette–Guérin (BCG) through a nephrostomy tube showed a better prognosis, with a 5-year disease-specific survival rate of 95%. 7 Conversely, Hayashida and colleagues described that 50% of patients with UT-CIS progressed and died of the disease. 8 In addition to variability in survival outcomes, even the diagnosis of UT-CIS remains challenging. All but two previous studies did not include ureteroscopic (URS)-based pathological confirmation for the diagnosis of UT-CIS. In this context, the National Comprehensive Cancer Network guidelines do not provide clear recommendations on treatment strategies or diagnostic management of this disease. 9 We presumed that the diagnostic uncertainty related to this rare entity complicates accurate risk assessments of disease recurrence and progression, resulting in variable survival outcomes. Thus, we conducted this multicenter study to clarify the clinical behavior and prognosis of UT-CIS and the significance of diagnostic URS in patients clinically suspected of having UT-CIS.
Materials and Methods
After the approval of each institutional review board, we retrospectively collected data from 12 centers between 2008 and 2018. All patients who met the three inclusion criteria of clinically suspected UT-CIS were included: the presence of positive high-grade cytology from the upper tract, the absence of a solid upper tract lesion on imaging, and a negative bladder biopsy. Patients who had hydronephrosis or imaging findings suspicious for UTUC and who were taking immunosuppressive drugs due to kidney transplantation were excluded. Definitive diagnoses of UT-CIS and UT-non-CIS were confirmed by pathological evaluation based on URS biopsy. Clinical diagnosis of UT-CIS was made following the three criteria mentioned above, without pathological confirmation (either a lack of pathological diagnosis of UC based on URS biopsy [URS group] or no URS implementation [non-URS group]). URS was performed only for diagnostic purposes.
Ureteroscopic management
Our technique for URS procedures was described previously. 10 Briefly, with patients under general anesthesia, a 4.5 Fr semi-rigid ureteroscope (The Needle, Richard Wolf GmbH, Germany) was advanced into the ureteral orifice with a wireless non-touch technique to prevent tumors from dropping or bleeding caused by contact with the guidewire. Further searches of the proximal ureter and renal pelvis were generally performed using either an 8.4 Fr (URF-P5, Olympus, Japan) or a 7.95 Fr flexible ureteroscope (URF-P7, Olympus, Japan) without the use of an access sheath. 11 Biopsies were performed using a 3 Fr biopsy cup forceps (Cook Medical, USA).
Techniques of BCG delivery and ureteroscopic biopsy
Intracavitary instillation of BCG was performed by retrograde catheterization with a 6-Fr Single- or Double-J stent. Our technique for placing a transcutaneous Single-J ureteral stent was as follows: after adequate extension of the bladder, a 19-gauge needle was inserted from the lower abdomen into the bladder under ultrasound guidance. A 0.035 guidewire was inserted through the needle and dilated the entry site up to 6 Fr. Then, a 6-Fr Single-J stent was introduced into the renal pelvis following the guidewire. Retrograde pyelography was performed to ensure the position of the catheter. A solution consisting of 240 mg of BCG (Immunobladder®, Japan BCG Laboratory, Tokyo, Japan) diluted with 120 mL of 0.9% saline was placed 20 cm above the kidney level of the patient’s spine and infused into the renal pelvis at a rate of 1 mL/min for 2 hours. In a Double-J stent, vesicoureteral reflux was confirmed by cystogram, and 80 mg of BCG combined with 39 mL of 0.9% saline was retained in the bladder for 2 hours. Each BCG course consisted of 6 weekly instillations. Complete response to BCG instillation was defined as the absence of high-grade cytology in either selective or voided urine cytology.
Follow-up
Routine follow-up protocol generally involved cystoscopy and urinary cytology every 3 months for the first 2 years after initial treatment; thereafter, patients were followed up every 6 months for 3 years and then annually. Disease recurrence and progression were defined as relapse elsewhere in the urinary tract regardless of tumor stage, and with higher stage (≥T1), respectively.
Statistical analysis
Differences in categorical and continuous variables according to URS were assessed with the chi-square and the Mann–Whitney U test, respectively. Overall (OS), cancer-specific (CSS), upper tract-specific (UTSS) focusing on the affected upper tract, progression-free (PFS), and recurrence-free survival (RFS) were calculated from the date of histological diagnosis to death from any cause, death from urothelial carcinoma (UC) elsewhere in the urinary tract, death from the affected UTUC, first progression, and recurrence, respectively. All P-values were two-sided, and statistically significant differences were defined as P < 0.05. Statistical analyses were performed using Stata/SE 17 statistical software (Stata Corp., College Station, TX, USA).
Results
Following the criteria of clinically suspected of having UT-CIS, 48 patients were included in this study. Table 1 summarizes their baseline characteristics according to the implementation of diagnostic URS. Diagnostic URS was performed in 28 (58%) patients (URS group), of whom definitive diagnoses of UT-CIS and UT-non-CIS were made in 7 (25%) and 6 (21%) cases, respectively (Fig. 1). Of the non-URS group, 95% (19/20) of cases were treated based on a clinical diagnosis of UT-CIS. Previous histories of UC and intravesical BCG administration were observed in 27 (56%) and 21 (44%) cases, respectively. Of 21 patients with no previous history of UC, initial reasons for visiting a urology department included macrohematuria in 9 patients, detection of abnormal urinalysis from medical checkup, etc. in 7, and dysuria and back pain in 4. In total, 92% of cases proceeded with initial treatment: 48% treated with upper tract BCG and 44% treated with nephroureterectomy. Of four patients (8%) who did not undergo any treatment intervention due to the lack of definitive/clinical diagnosis, positive selective cytology findings eventually disappeared, and all are alive without any abnormal findings suspicious for malignancy in the upper urinary tract. Among 21 patients who submitted to RNU as an initial treatment, including 12 with clinical diagnosis of UT-CIS, the final pathological findings revealed UT-CIS in 14 patients and T1 in 3, with a concordance rate of UT-CIS being 67%.
Characteristics of Patients Who Had a Positive High-Grade Cytology from the Upper Tract, the Absence of a Solid Upper Tract Lesion on Imaging, and a Negative Bladder Biopsy
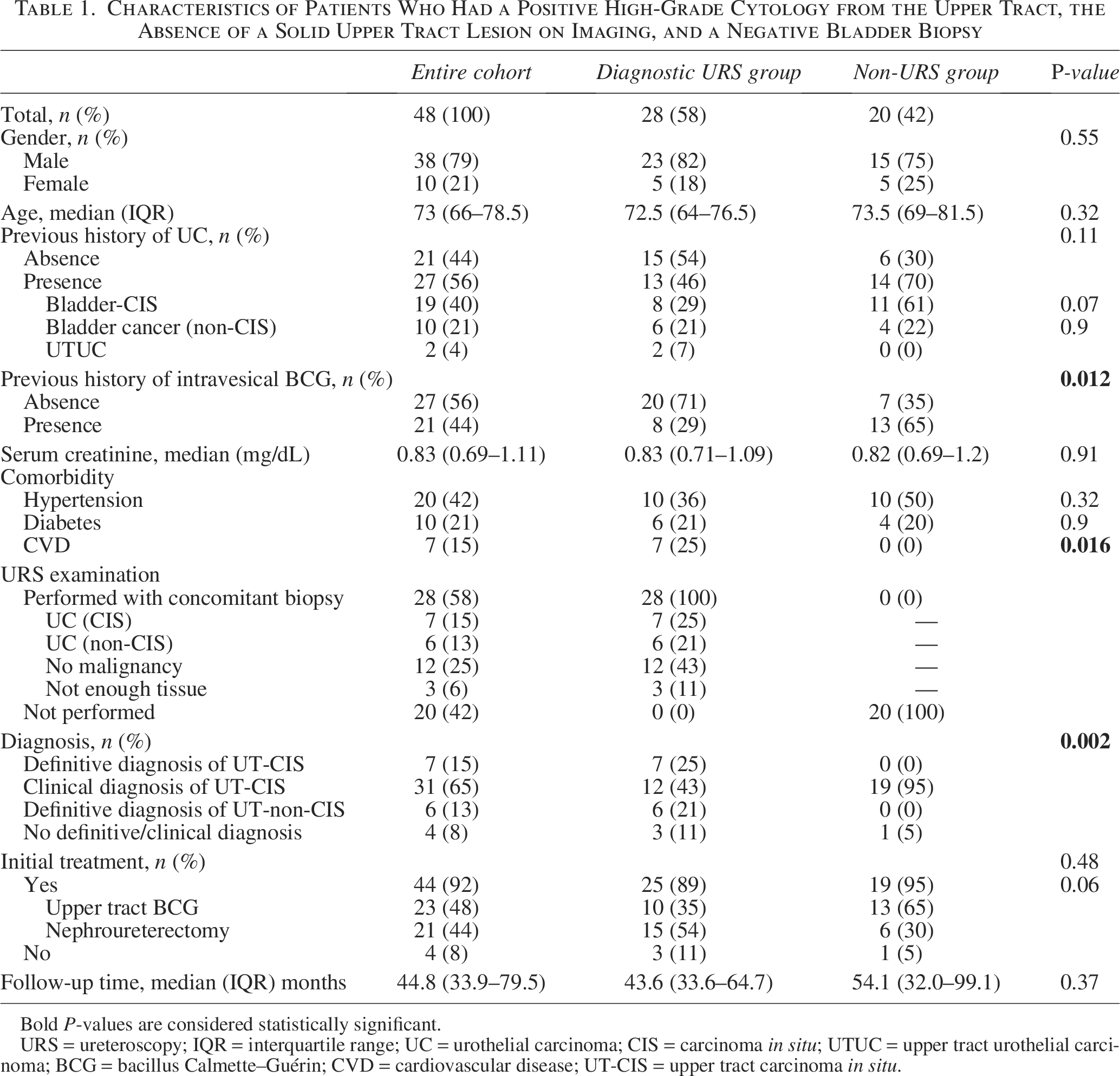
Bold P-values are considered statistically significant.
URS = ureteroscopy; IQR = interquartile range; UC = urothelial carcinoma; CIS = carcinoma in situ; UTUC = upper tract urothelial carcinoma; BCG = bacillus Calmette–Guérin; CVD = cardiovascular disease; UT-CIS = upper tract carcinoma in situ.
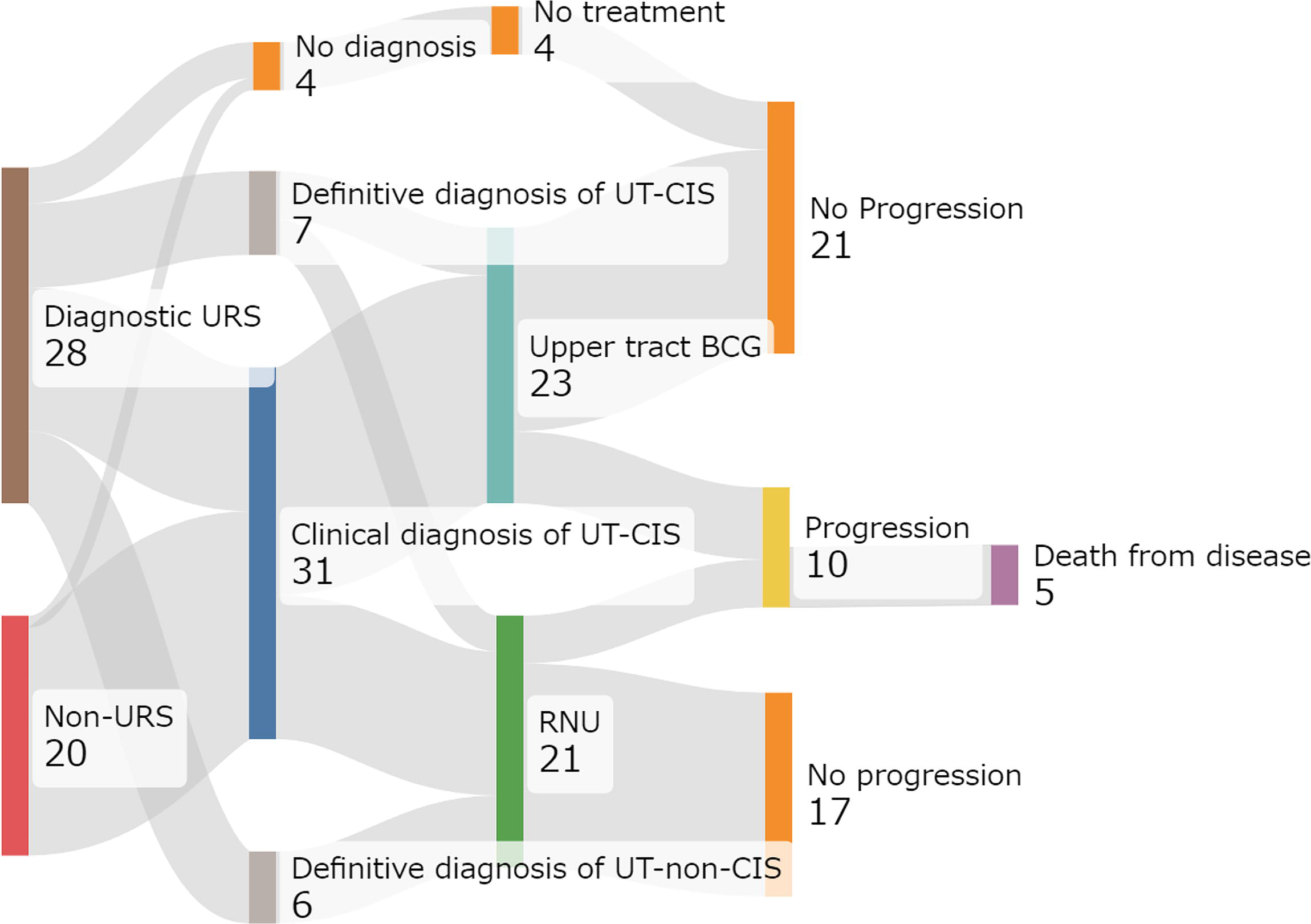
Treatment courses and survival outcomes in patients clinically suspected upper tract carcinoma in situ (UT-CIS).
Patterns of recurrence and progression and survival outcomes
During a median follow-up of 44.8 months (interquartile range: 33.9–79.5), recurrence after initial treatment occurred in 26 cases (54%), with 18 (64%) in the URS group and 8 (40%) in the non-URS group (P = 0.10). Meanwhile, progression occurred in 10 (21%) cases, with 9 (32%) in the URS group and 1 (5%) in the non-URS group (P = 0.022). Details of recurrence and progression sites are shown in Figure 2. Bladder was the most common site that suffered a recurrence (40%) and progression (17%), with six patients eventually undergoing a radical cystectomy. Moreover, recurrence was likely to occur in any part of the urinary tract, including the contralateral upper tract (8%) and urethra (2%).
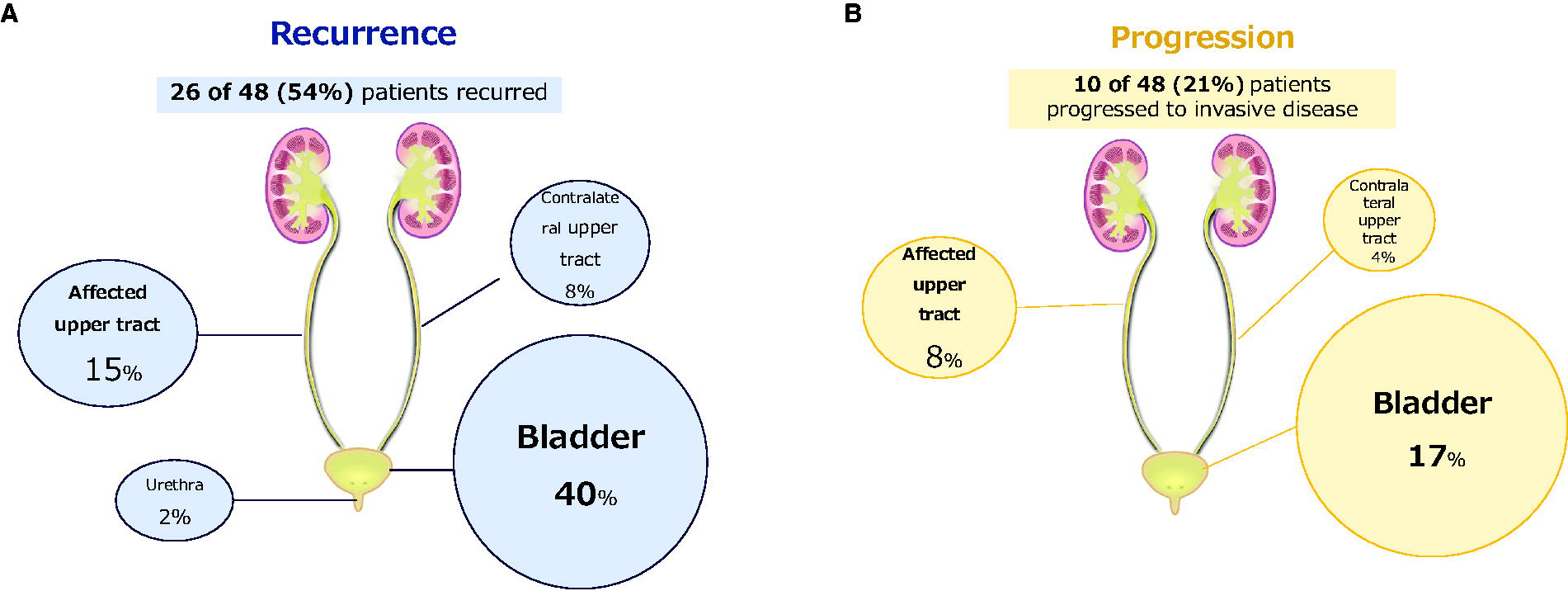
Details of recurrence
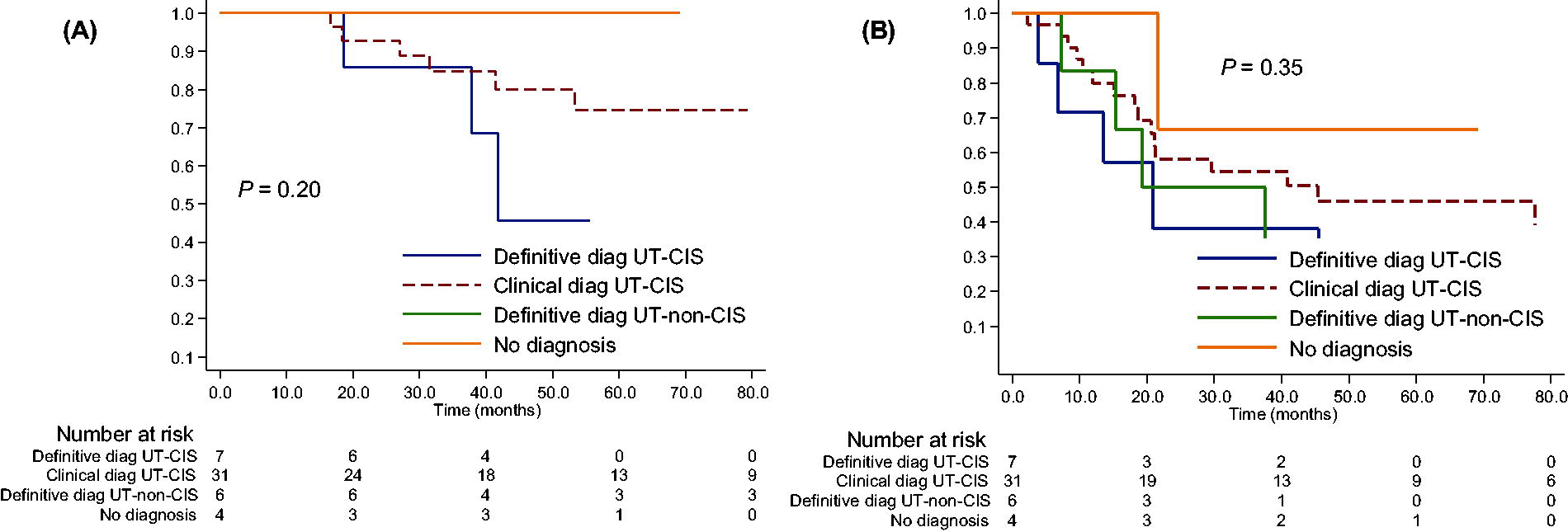
During the follow-up period, nine (19%) patients died, and five (10%) died of the disease. The overall OS, CSS, UTSS, PFS, and RFS estimates were 88.2%, 94.8%, 100%, 80.8%, and 52.4%, respectively, at 3 years, and 75.5%, 84.1%, 96.4%, 76.9%, and 39.7%, respectively, at 5 years (Fig. 3). The median time to recurrence and progression was 18.4 and 20.4 months, respectively. When patients were stratified by diagnostic status, 3-year OS and RFS estimates varied considerably, ranging from 84.8% to 100% and from 38.1% to 66.7%, respectively (Fig. 4).
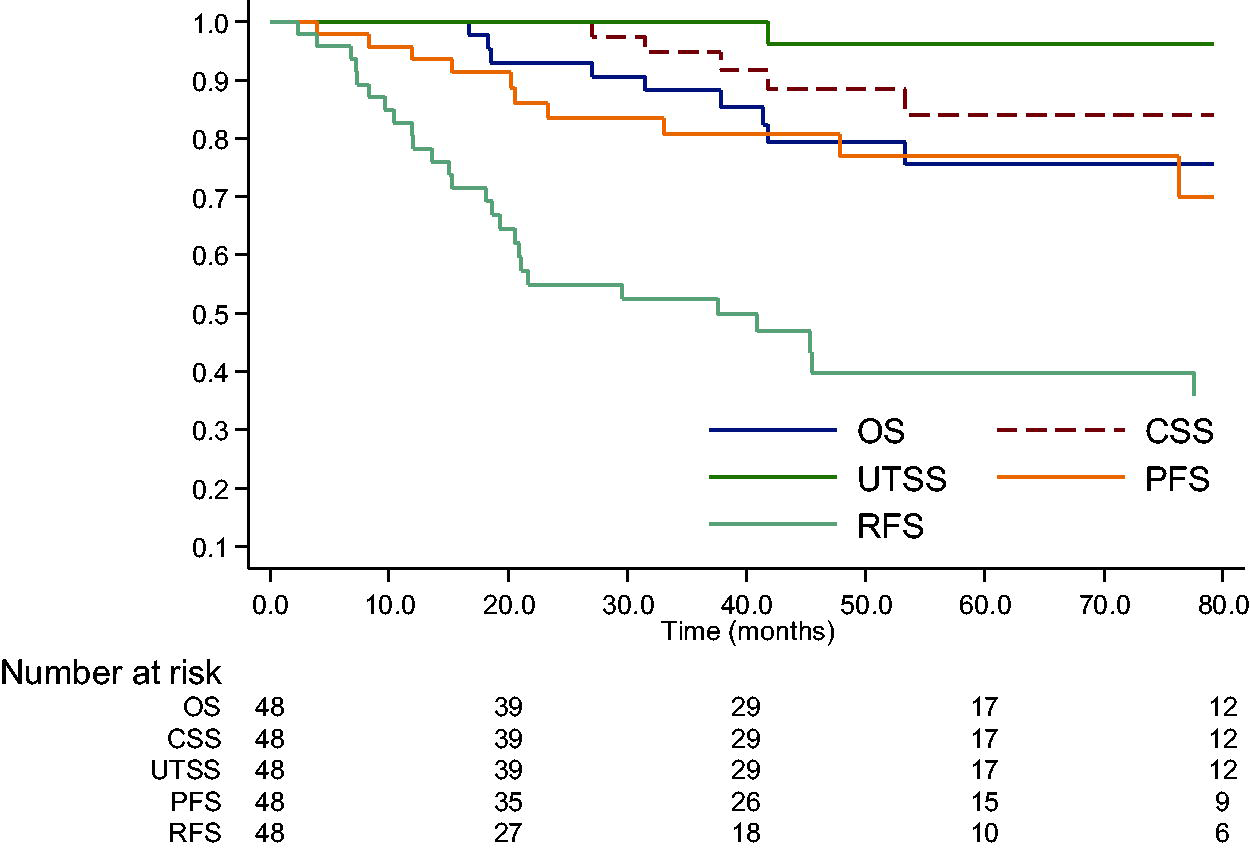
Kaplan–Meier curves of overall (OS), cancer-specific (CSS), upper tract-specific (UTSS), progression-free (PFS), and recurrence-free survival (RFS) in patients with clinically suspected UT-CIS. UT-CIS = upper tract carcinoma in situ.
Kaplan–Meier curves of OS
Oncological impact of diagnostic URS for UT-CIS
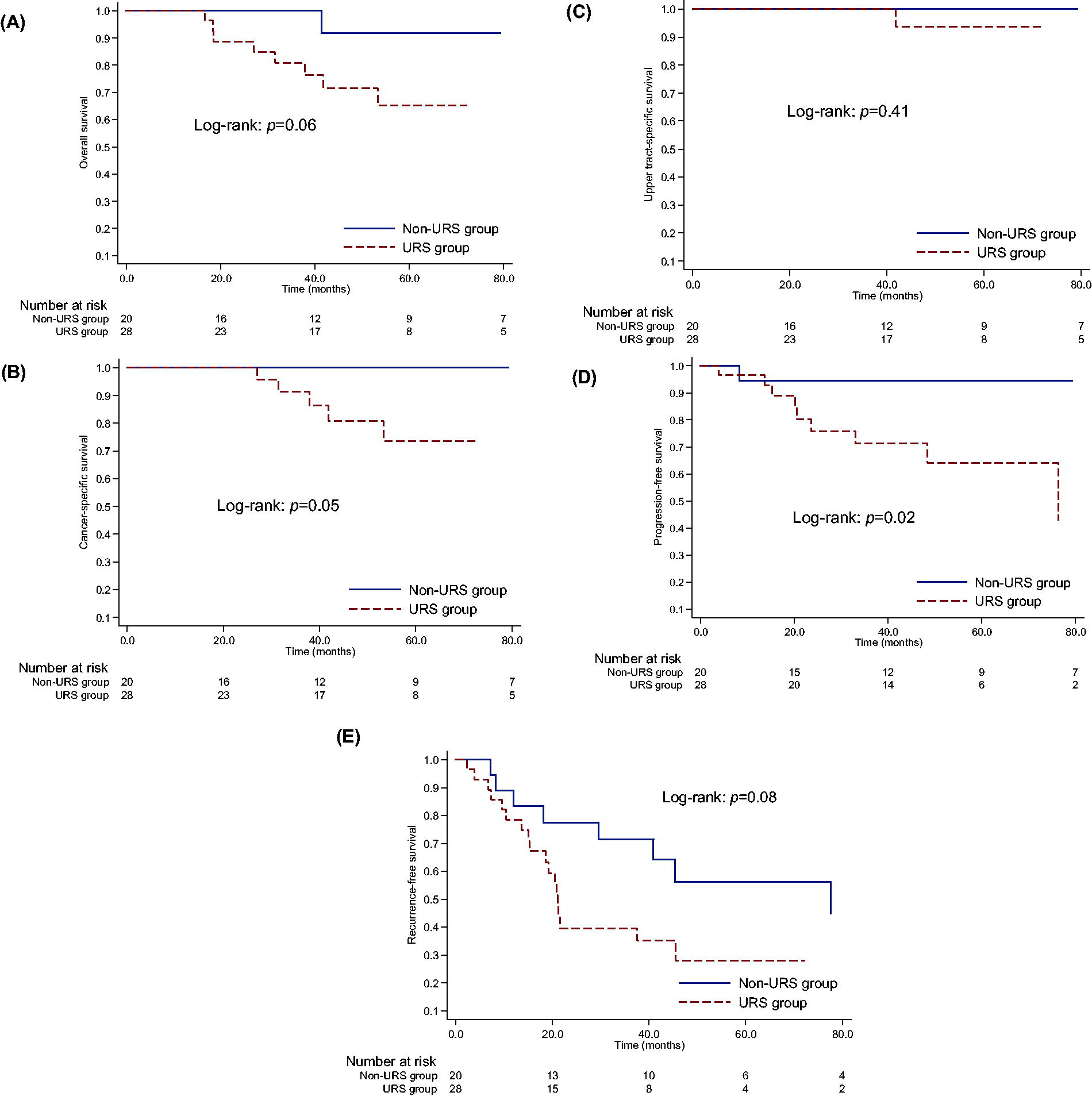
Kaplan–Meier curves showed that no significant differences were observed between the URS and non-URS groups in survival outcomes except for PFS (Fig. 5). Of note, URS-based pathological assessment led to an early definitive diagnosis of UT-non-CIS in three (11%) cases, thereby enabling early treatment intervention with RNU (all three are alive). Moreover, URS implementation also revealed the absence of malignancy in the affected upper tract in three (11%) cases, thereby avoiding misdiagnosis and/or overtreatment, such as unnecessary RNU or upper tract BCG instillation (all are alive without any intervention during the follow-up period). Meanwhile, two patients in the non-URS group and one in the URS group underwent RNU under clinical diagnosis of UT-CIS, but no cancer cells were detected in the final pathology analysis.
Kaplan–Meier curves of overall
Intracavitary BCG instillation to the upper tract
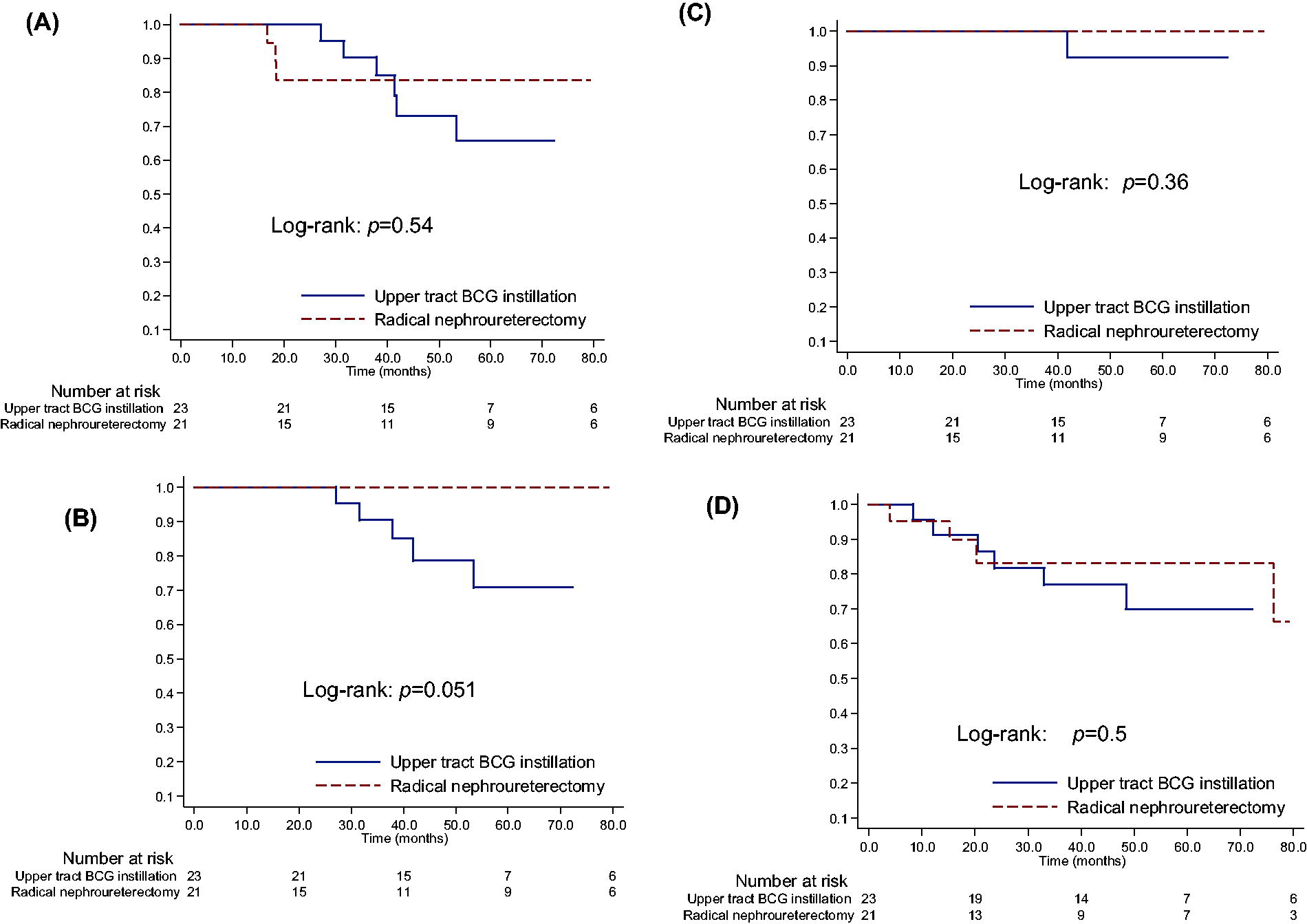
In total, 23 (48%) patients received intracavitary BCG instillation to the upper tract (Table 2). After the weekly BCG instillation, all patients (100%) achieved initial complete response. Afterward, six cases experienced recurrence in the affected upper tract: four in the URS group and two in the non-URS group (P = 0.022). Of them, four patients underwent subsequent RNU after recurrence, with one being found invasive UTUC (pT3). No significant differences were observed between upper tract BCG instillation and RNU in survival outcomes (Fig. 6).
Outcome of Upper Tract BCG Instillation in Patients with Clinically Suspected of UT-CIS
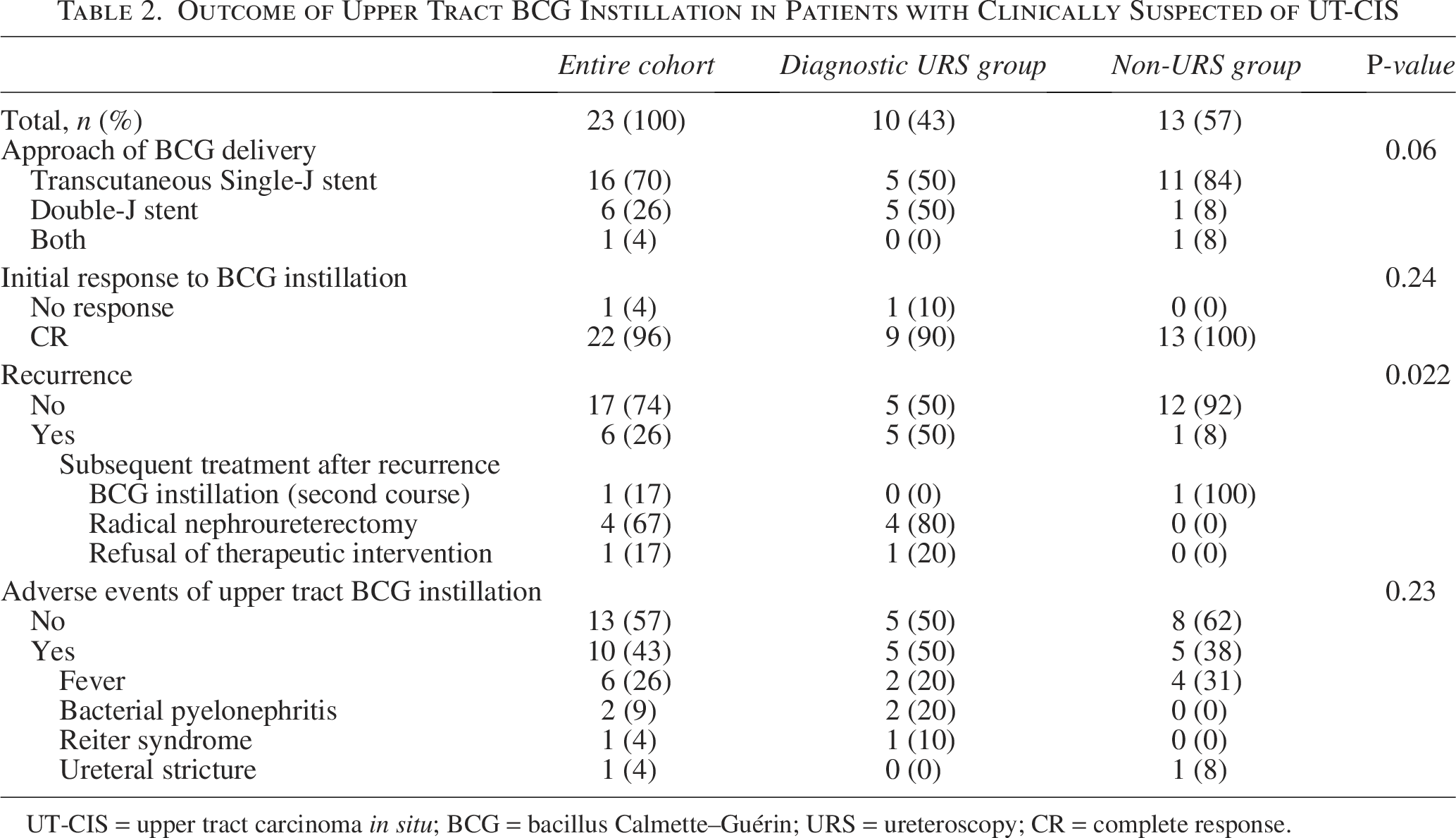
UT-CIS = upper tract carcinoma in situ; BCG = bacillus Calmette–Guérin; URS = ureteroscopy; CR = complete response.
Kaplan–Meier curves of overall
Discussion
We assessed the treated natural history of patients clinically suspected of having UT-CIS. Furthermore, we explored the prognostic impact of URS-based pathological evaluation on survival in this population. We found that clinically suspected UT-CIS frequently recurred and occasionally progressed with unique patterns, ultimately associated with unfavorable prognosis. Furthermore, URS implementation conferred oncological benefits, such as earlier transition to RNU or avoiding the most feared outcome, that is, the absence of malignancy after RNU, associated with no pathological confirmation prior to extirpative surgery, even though it failed to detect a statistically significant difference due to its retrospective nature imposing considerable selection bias.
There are several important implications of the findings of this study. First, the long-term prognosis of clinically suspected UT-CIS may not be as favorable as previously expected. Despite a lack of uniform reporting due to the rarity of this disease, isolated UT-CIS generally has been assumed to have better survival outcomes compared with bladder-CIS, with 5-year CSS and RFS of 83.1% and 54.9%, respectively. 12 However, survival outcomes in patients with isolated UT-CIS have remained debatable, since oncological outcomes reported in available literature have a large heterogeneity in the risk of recurrence and progression.13,14 One possible explanation for this wide range of clinical behavior in UT-CIS is that, due to a lack of a standardized diagnostic assessment, this rare entity possibly harbors various diseases, ranging from progressive UC to the absence of malignancy in the suspected upper tract. In support of this, our analyses revealed that among clinically suspected UT-CIS, URS examination enabled the definitive diagnoses of UT-CIS (15%), UT-non-CIS (13%), and no definitive/clinical diagnosis (8%), resulting in a wide spectrum of oncological outcomes (RFS distributions varied between 38.1% and 66.7%). Therefore, establishment of reliable diagnostic criteria or consensus is urgently required to unveil the true prognosis of this disease. In this context, previous studies focusing on patients with biopsy-proven UT-CIS may provide valuable clues to understand the true prognosis of UT-CIS. 15 A recent study by Fontanet et al. investigating the efficacy of intracavitary BCG for biopsy-proven UT-CIS exhibited that the estimated 5-year PFS and RFS were 72.3% and 49.6%, respectively. 16 These findings, in accordance with our findings, may offer robust evidence showing the potential unfavorable prognosis of this disease with frequent recurrence and occasional progression.
Second, our findings enhance the understanding of recurrence and progression patterns in this disease. It is noteworthy that 56% of patients in our study had previous UC history prior to UT-CIS diagnosis, with 40% having bladder-CIS and 44% having undergone intravesical BCG administration. This is consistent with a large study of patients with UT-CIS treated with intracavitary BCG therapy in which all included patients had a previous history of UC. 7 Cumulative evidence also identified bladder-CIS as an independent risk factor for the development of metachronous UTUC.17,18 Moreover, metachronous recurrence was detected in the urinary tract of 54% of our patients following treatment of clinically suspected UT-CIS, with a median follow-up of 44.8 months. Taken together, these findings indicate that UT-CIS seems to be considered as a certain point in time during the long clinical course of pan-urothelial disease, suggesting a higher likelihood of having either synchronous or metachronous recurrence, or prior UC disease, in any part of the urinary tract. 19 As a possible mechanism to account for distinct recurrence patterns in patients with UT-CIS, a previous study investigating DNA content, p53 immunoreactivity, and proliferative index between urothelial mucosa with and without CIS revealed that CIS was a surrogate marker of a high malignant transformation potential in the surrounding normal urothelium, thereby suggesting CIS to be reflective of a proliferative status underlying field carcinogenesis. 20 Interestingly, 21% of patients in this cohort progressed, with 72% of them being independent of the affected upper tract. Given the frequent recurrence and non-negligible progression rates, meticulous long-term surveillance covering all parts of the urinary tract is needed so as not to miss recurrent UC at an early stage prior to the development of progressive UC, considering that most progress silently.
Third, we first assessed the role of URS implementation for the management of patients with clinically suspected UT-CIS. Although we failed to detect the significance of URS, 21% (6 out of 28 cases) of patients obviously benefited from URS implementation, including the early transition to and avoidance of unnecessary RNU. The possible reason for better PFS in favor of the non-URS group includes considerable selection bias resulting from the difficulty of extracting this rare disease and the small sample size not amenable to multivariable analysis controlling for the effects of possible confounding factors. There may be several concerns related to routine URS implementation, such as a delay in subsequent RNU or suboptimal diagnostic performance of URS for UT-CIS.6,21 However, our data suggest that CSS and UTSS were comparable between the URS and non-URS groups, and pathological confirmation of UC was made in almost half of the cases in the URS group. Moreover, two patients with clinically suspected UT-CIS who omitted diagnostic URS followed by RNU resulted in the absence of cancer cells on the final pathology, and three with high-grade selective cytology eventually disappeared during the follow-up period, suggesting the limited diagnostic reliability of urine cytology to exclude/confirm UTUC. 22 Therefore, we believe that accurate diagnostic workup, including URS with concomitant biopsy, is crucial to detect the presence or absence of malignancy in the suspected upper urinary tract before proceeding with any type of invasive treatment (e.g., BCG or RNU). 1
Our study is not devoid of limitations, most of which are inherent to its retrospective and multicentric nature. First and foremost, it suffers from selection bias. Since clinically suspected UT-CIS presumably represents a certain point in time during the long clinical course of pan-urothelial disease, accurate data extraction of eligible patients who met three inclusion criteria is deemed challenging. In addition, the diagnostic disparity (URS vs non-URS groups) was mainly based on the difference of each institutional diagnostic strategy, not on that of patients’ characteristics, leading to the potential selection bias. Second, due to the nature of multicenter studies, specimens were not reviewed via central pathology, and the follow-up protocol was not standardized. Third, fluorescence in situ hybridization and novel imaging techniques, such as photodynamic diagnosis, were not used in this study, but these technologies may help improve the diagnostic performance of UT-CIS.23–25 Fourth, although bladder was the most common site that suffered recurrence and progression, 56% of patients had experienced previous bladder cancer, suggesting that caution should be exercised regarding the interpretation of this finding.
Nonetheless, advances in understanding the biology of UT-CIS should lead to the development of definitive diagnostic criteria and optimal treatment strategies that will facilitate clinicians to manage this rare disease. We believe that diagnostic URS can assist clinicians in uncovering each patient’s true disease course, thereby helping counsel about his/her prognosis.
In conclusion, we clarified the unique patterns of recurrence and progression in patients clinically suspected of having UT-CIS. This disease frequently recurred and occasionally progressed during a long follow-up period, resulting in an unfavorable prognosis. Given the nature of pan-urothelial disease, meticulous long-term observation covering all parts of the urinary tract is needed. The incorporation of URS into the diagnostic pathway may provide additive value in avoiding overtreatment (unnecessary RNU) for patients harboring cancer cells in another part of the urinary tract and earlier surgical intervention for those with UT-non-CIS, thereby providing firm guidance for treatment strategies. Further studies are warranted to establish diagnostic criteria and unveil the true prognosis of this rare entity.
Authors’ Contributions
S.K.: Conceptualization; N.K., O.F., T.K., T.T., H.H., T.N., R.A., K.U., Y.Y., Y.N., M.T., T.S., K.Y., T.Y., T.K., Y.T., T.S., T.I., S.N., K.E., and Y.K.: Data curation; S.K., T.I., and T.Y.: Formal analysis; K.B., T.K., T.W., and M.A.: Supervision; S.K.: Writing—original draft; M.A.: Writing—review and editing.
Footnotes
Acknowledgments
The authors thank all the urologists at the participating institutions for collecting data and conducting this study.
Author Disclosure Statement
All authors state that they have no conflict of interest that might bias this work.
Funding Information
This study did not receive any kind of funding.
Ethical Approval
This study has been approved by the Institutional Review Board of Okayama University Hospital (approval number: K2009-043).
Availability of Data and Material
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Consent to Participants
In accordance with institutional policy for retrospective studies, an opt-out approach was applied, and information about the study was disclosed on the institutional website to provide patients the opportunity to decline participation.
Consent for Publication
Not applicable