
Abstract
Background:
Patients with exstrophy–epispadias complex (EEC) often present with attenuated fascia. Currently, there is no direct comparison of outcomes between percutaneous cystolitholapaxy and open cystolithotomy in this specific patient population. Thus, we sought to evaluate the therapeutic efficacy and associated morbidity of both surgical approaches in patients with EEC.
Methods:
Patients who underwent either their first percutaneous cystolitholapaxy or open cystolithotomy between 2003 and 2023 were identified using an IRB-approved institutional database of 1512 patients with EEC.
Results:
Among 66 patients, 8 (12.12%) underwent percutaneous cystolitholapaxy without augmentation, 31 (46.97%) underwent percutaneous cystolitholapaxy with augmentation, 11 (16.67%) underwent open cystolithotomy without augmentation, and 16 (24.24%) underwent open cystolithotomy with augmentation. Compared with the open approach, the percutaneous approach resulted in shorter operative times: 123 (interquartile ranges [IQR]: 81–151) vs 218 minutes (IQR: 142–281) for patients with augmentation, and 131 (IQR: 115.5–141) vs 196 minutes (IQR: 176.5–287.3) for those without augmentation (p = 0.0002). Hospital stays were shorter with the percutaneous approach: 1 (IQR: 1–1) vs 3 days (IQR: 1–4) with augmentation, and 1.5 (IQR: 1–2) vs 3 days (IQR: 1–4) without augmentation (p = 0.0044). Notably, the percutaneous group had smaller stone volumes (7.15 cm3, IQR: 2.73–24.31 vs 31.04 cm3, IQR: 10.77–107.40, p = 0.0011). Both techniques achieved a 100% stone-free rate (p > 0.99). There were no differences in recurrence (p = 0.20) and cumulative incidence (HR 0.76, 95% confidence interval: 0.39–1.48, p = 0.38) between groups. Postoperative complications revealed that vesicocutaneous fistulas were most common in open surgery without augmentation (n = 5, 45.45%), followed by open with augmentation (n = 1, 6.25%), and none in the percutaneous groups (p = 0.0002).
Conclusion:
Percutaneous cystolitholapaxy provided significant advantages for patients with EEC, including shorter operative times and reduced hospital stays, with equivalent stone clearance. Moreover, open cystolithotomy carried a higher risk of vesicocutaneous fistula formation. These findings suggest percutaneous approaches may offer a safer and more efficient alternative for managing bladder stones in patients with EEC.
Keywords
Introduction
Patients with exstrophy–epispadias complex (EEC) who undergo bladder reconstruction face a significantly increased risk of bladder stone formation, especially if their reconstruction involves bowel augmentation or bladder neck procedures that increase outlet resistance. 1 In fact, 21.6% of patients with EEC with augmented bladders develop bladder stones, with a significant recurrence rate. 2 Managing bladder stones in patients with EEC presents unique and intricate challenges posed by their attenuated lower abdominal fascia, a consequence of the congenital malformation affecting the structural integrity of the abdominal wall. 3 Furthermore, the unique physiological characteristics of their urothelial tissue—notably the markedly reduced expression of Uroplakin-II, a glycoprotein crucial for urothelial integrity—further complicate treatment in this population. 4 These features, combined with the impact of repeated surgical interventions, heighten the complexity of surgical intervention and increase the risk of complications in patients with EEC following repeated mucosal violations. 5 Given the delicate anatomical considerations in patients with EEC, careful selection of the optimal surgical approach is of paramount importance to minimize complications and optimize outcomes.
Stone clearance and recurrence in patients with EEC are strongly influenced by multiple interrelated factors, including total stone volume, bladder augmentation status, and postoperative management strategies such as bladder irrigation. Larger stone burdens are associated with greater operative complexity and longer surgical times, especially for percutaneous approaches. 6 Augmentation using bowel segments such as ileum or colon is a well-established risk factor for stone recurrence, with recurrence rates reported as high as 74%, independent of surgical approach. 2 Additionally, postoperative strategies like bladder irrigation are frequently employed to mitigate recurrence. 7 These variables must be considered when evaluating outcomes between surgical approaches.
Both percutaneous cystolitholapaxy and open cystolithotomy are well-established surgical techniques for the management of large bladder stones.1,8–13 The optimal approach for bladder stone removal in patients with EEC remains unclear. To date, no studies have directly compared the efficacy and safety of these interventions in this unique and complex patient population, leaving a critical gap in the evidence necessary to guide clinical decision-making. We hypothesize percutaneous cystolitholapaxy offers a less invasive alternative, reducing perioperative morbidity while achieving comparable stone-free rates compared with open cystolithotomy.
Therefore, the objective of the current study was to evaluate the efficacy and morbidity of percutaneous cystolitholapaxy vs open cystolithotomy in patients with EEC. The present study aims to evaluate the complications and stone-free outcomes of patients with EEC undergoing either open cystolithotomy or endoscopic percutaneous cystolitholapaxy.
Methods
Study population
Data encompassing patients with exstrophy–epispadias treated with either their first percutaneous cystolitholapaxy or open cystolithotomy between January 1, 2003 and December 31, 2023 were identified using an institutional database of 1512 patients with EEC, which includes all patients with cloacal exstrophy, classical bladder exstrophy, and epispadias. Bladder stones were identified either incidentally during routine ultrasound or upon imaging prompted by clinical symptoms such as hematuria, recurrent urinary tract infections (UTIs), pain, incontinence, or retention. Of note, nearly all patients in the cohort had previously undergone bladder neck transection or bladder neck reconstruction as part of their initial bladder reconstruction, precluding the use of transurethral approaches for stone removal. One patient had an open bladder neck; however, the bladder neck was stenotic, preventing the feasibility of a transurethral approach. For this study, we included patients with bladder stones—both first-time and recurrent—who underwent their first percutaneous or open bladder surgery. Some recurrent stone formers had previously undergone stone removal through their continent stoma but later required percutaneous or open surgery for recurrence. Patients who underwent stone removal exclusively through their continent stoma were excluded, as this approach, which avoids transabdominal entry or mucosal violation, is typically reserved for smaller stone burdens determined by the surgeon at the time of surgery. Further exclusion criteria encompassed patients with incomplete demographic data (i.e., bladder status), as well as those who had bladder stone removal concurrent with another surgical procedure. Eligible patients were followed from the time of their procedure until death, loss to follow-up, or the study endpoint on December 31, 2023. Patients were stratified based on augmentation status (i.e., augmentation vs no augmentation) to assess differences in postoperative outcomes, given prior clinical experience suggesting a higher complication rate in patients with bladder augmentation. This study was approved by The Johns Hopkins University Institutional Review Board.
Pre-procedure management
To optimize patient safety and minimize the risk of bowel or continent stoma injury, preoperative imaging was performed with computed tomography (CT) to assess bowel positioning relative to the bladder. If imaging suggested a high risk of bowel injury, a percutaneous approach was avoided in favor of an open approach. For patients with prior bladder reconstruction, additional precautions were taken to ensure safe access. The bladder was secured to the abdominal wall during initial reconstruction to minimize the risk of bowel interposition.
Surgical technique
For percutaneous cystolitholapaxy, a 10F cystoscope was first used for stoma endoscopic guidance, and the bladder was accessed through the midline lower abdominal wall using an 18-gauge spinal needle under direct visualization. Following skin and fascial incisions, the tract was dilated to 30F using a NephroMax balloon dilation system, and a sheath was introduced. Bladder stones were fragmented using a combination of lithotripsy techniques, including ultrasonic, pneumatic, and Holmium laser lithotripsy, followed by removal with a suction vacuum device to optimize efficiency and minimize residual fragments. For open cystolithotomy, the bladder was initially filled with methylene blue or 0.9% saline through the stoma for improved visualization of the bladder after incision. A midline lower abdominal incision was then made, and the fascia was meticulously dissected. Any adjacent bowel was identified and mobilized away to prevent injury. Once a clear surgical field was established, the bladder was incised, and the stones were manually removed. Both procedures were performed under general anesthesia. It is important to note that there may be variability in the surgical approach, including incision size and technique, depending on surgeon preference.
Post-procedure management
Following percutaneous cystolitholapaxy or open cystolithotomy, patients were managed with a 16F suprapubic (SP) tube placed immediately postoperatively for bladder drainage. The tube was inserted through the rectus muscle, typically on the lateral aspect of the right or left side depending on anatomical considerations. Additionally, a stoma catheter was inserted for drainage immediately after the procedure. Both the SP tube and stoma catheter were irrigated with 0.9% saline to maintain hygiene. The SP tube was removed after 4 weeks. Following the removal of both SP tube and stoma catheter, patients were followed continuously with annual renal and bladder ultrasound imaging evaluations to monitor for recurrence of bladder stones, without a predefined minimal follow-up period. Of note, in patients with EEC, annual renal and bladder ultrasound is standard practice from the time of closure or bladder reconstruction onward, ensuring consistent long-term surveillance.
Variables and outcomes of interest
The primary independent variable of interest was the type of bladder stone surgery (i.e., percutaneous cystolitholapaxy and open cystolithotomy). Patient demographics, including age, biological sex, race, diagnosis (i.e., epispadias, bladder exstrophy, cloacal exstrophy), comorbidities (i.e., chronic kidney disease, nephrolithiasis, spina bifida, paraplegia, hypothyroidism, kidney transplant, obesity), bladder status (i.e., closed native, augmentation [ileal augment and colon augment], neobladder [ileal neobladder, colon neobladder, and combined neobladder]), bladder neck status (i.e., transection, reconstruction, and open), voiding method (i.e., continent catheterizable stoma, urethral voiding, and incontinent), irrigation, fragmentation, primary stone component, and stone size were collected. Obesity was defined as having a body mass index >30. Stone sizes were determined using preoperative imaging (i.e., non-contrast CT, ultrasound, or X-ray) or confirmed postoperatively through pathology reports, with the aggregate stone burden reported as the total maximum diameter and stone volume. The primary outcomes of interest were the complications in each group (i.e., intraoperative and postoperative). The postoperative period was defined as the first 30 days following the procedure. Secondary outcomes of interest included perioperative course measures (i.e., duration of procedure, length of hospital stay, stone-free rates, recurrence rates, duration of follow-up). Stone-free status was defined as the complete removal of bladder stones during the procedures, confirmed through direct visualization. Recurrence was defined as a subsequent surgery to remove stones during the follow-up period or the detection of stones on follow-up imaging exams, including ultrasound or non-contrast CT. For analysis of cumulative incidence of recurrence, a single patient could only be counted as having a bladder stone recurrence once, despite possibly having multiple recurrent episodes of bladder stones over time.
Statistical analysis
Continuous variables were summarized using median values and interquartile ranges (IQR), whereas categorical variables were presented as counts and percentages (%). The Mann–Whitney U test or Kruskal–Wallis test was used to compare continuous variables between treatment groups as appropriate, and the chi-square or Fisher exact test was used to compare categorical variables. Time-to-event analysis was performed using Kaplan–Meier survival curves to estimate cumulative incidence of first recurrent bladder stones. The log-rank test was used to compare stone recurrence between treatment groups. The hazard ratio (HR) for recurrence was calculated based on the log-rank test, with 95% confidence intervals (CIs)—an HR greater than 1 indicates a higher rate of recurrence in the percutaneous group compared with the open group. Censored events occurred at last follow-up or death. All tests were two-sided, and a p value <0.05 was considered statistically significant. Graphs were generated, and statistical analyses were performed using GraphPad Prism version 10.4.0 (GraphPad Software, Inc.).
Results
Patient cohort
The study cohort included 66 patients. Median age was 19.36 years (IQR: 15.32–25.88), 38 (57.58%) were men, and 57 (86.36%) were White (Table 1). The primary underlying diagnoses were bladder exstrophy (n = 53, 80.30%), cloacal exstrophy (n = 10, 15.15%), and epispadias (n = 3, 4.55%). The most common comorbidity was recurrent UTIs (n = 30, 45.45%). A majority of patients had undergone prior bladder augmentation (n = 47, 71.21%), of which 23 (34.85%) were with ileal segment and 24 (36.36%) were with colon. Of the remaining patients, 12 (18.18%) had a closed native bladder, and 7 (10.61%) had a neobladder formed, of which 5 (7.57%) were ileal, 1 (1.52%) was colon, and 1 (1.52%) was a combined neobladder. Regarding bladder neck status, most patients had a bladder neck transection (n = 50, 75.76%), whereas a smaller proportion underwent prior bladder neck reconstruction (n = 15, 22.73%). In terms of voiding method, nearly all patients utilized a continent catheterizable stoma (n = 64, 96.97%). Bladder irrigation was instructed in the majority of patients (n = 51, 77.27%). The median stone volume was 14.59 cm3 (IQR: 3.89–37.59).
Patient Characteristics Relative to Percutaneous Cystolitholapaxy vs Open Cystolithotomy
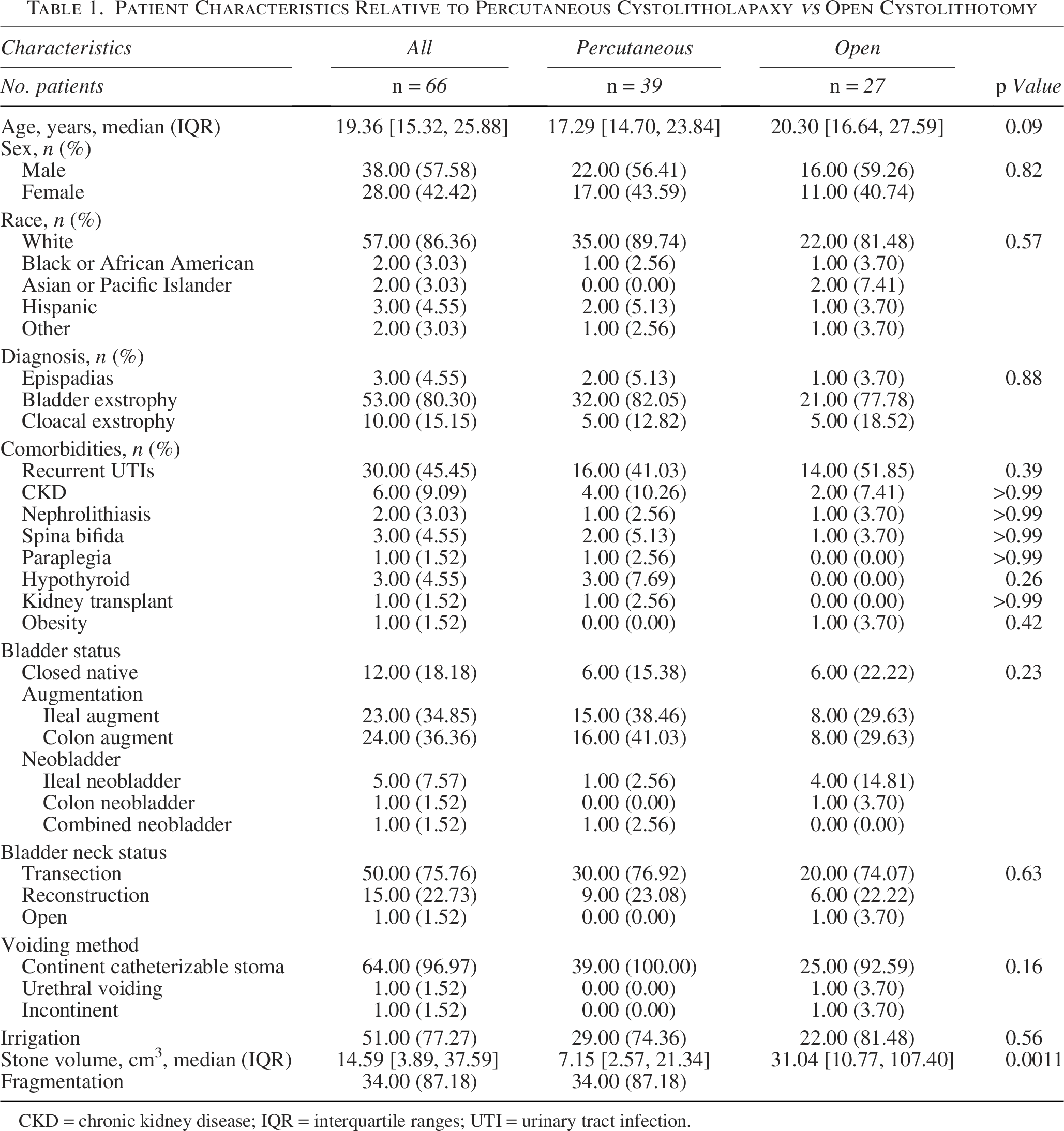
CKD = chronic kidney disease; IQR = interquartile ranges; UTI = urinary tract infection.
A total of 39 (59.10%) patients underwent percutaneous cystolitholapaxy, and 27 (40.91%) underwent open cystolithotomy. Among patients who underwent percutaneous cystolitholapaxy, 34 (87.18%) underwent stone fragmentation. The median stone volume was significantly smaller in the percutaneous group compared with the open group (7.15 cm3, IQR: 2.57–21.34 vs 31.04 cm3, IQR: 10.77–107.40, p = 0.0011). Patients who underwent percutaneous cystolitholapaxy were comparable relative to age, sex, race, diagnosis, comorbidities, bladder status, bladder neck status, voiding method, and irrigation compared with those who underwent open cystolithotomy (all p > 0.05).
Perioperative course and complications
Significant differences were observed in the perioperative course between percutaneous and open approaches (Table 2). Operative time differed significantly among groups, with the percutaneous groups having shorter median durations than the open groups (p = 0.0002). When stratified by stone fragmentation, percutaneous procedures without fragmentation had the shortest operative time, followed by those with fragmentation, whereas open cystolithotomy had the longest (p < 0.0001) (Table 3). No intraoperative complications occurred among groups. Hospital stay was significantly shorter for percutaneous groups compared with open surgery (p = 0.0044). Stone-free rate was 100% in the postoperative period. Median stone diameter was 4.50 cm (IQR: 2.45–5.70), and the most common primary stone components were carbonate apatite (n = 30, 45.45%) and ammonium magnesium phosphate (n = 26, 39.39%). Although stone diameters were comparable across percutaneous and open groups (p > 0.05), stone volumes differed significantly. Patients treated percutaneously had lower median stone volumes both without augmentation (11.75 cm3, IQR: 2.93–24.12) and with augmentation (7.15 cm3, IQR: 2.57–21.34), compared with those who underwent open surgery without augmentation (30.07 cm3, IQR: 17.30–69.92) and with augmentation (34.80 cm3, IQR: 5.43–110.50; p = 0.016). Additionally, duration of follow-up was comparable across groups (p = 0.38).
Operative Course and Complications

Operative Course Relative to Endoscopic Fragmentation

Postoperative complications are outlined in Table 2. Complications occurred in 4 patients (10.26%) in the percutaneous group, compared with 7 patients (25.93%) in the open group. The open groups had a significantly higher incidence of vesicocutaneous fistula compared with the percutaneous groups (p = 0.0002). The highest incidence was observed in the open cystolithotomy without augmentation group (n = 5, 45.45%), followed by the open cystolithotomy with augmentation group (n = 1, 6.25%), whereas none were observed in the percutaneous groups. All other complications, such as bleeding, pain, pyelonephritis, seroma, and SP tube dysfunction, were all comparable between both groups (p > 0.05).
Bladder stone recurrence
Cumulative incidence of recurrence is depicted in Figure 1. Cumulative incidence of recurrence was comparable between treatment groups (p = 0.38). The HR for recurrence during the study period in the percutaneous group as compared with the open surgery group was 0.76 (95% CI: 0.39–1.48). Although more recurrence occurred in the percutaneous group (n = 29, 74.36%) compared with the open cystolithotomy group (n = 15, 55.56%), the differences were not significant (p = 0.11). Additionally, recurrence rates did not significantly differ by augmentation status (p = 0.20). Specifically, in the percutaneous group, recurrence occurred in 6 (75.00%) of non-augmented vs 23 (74.19%) of augmented patients, whereas in the open group, recurrence occurred in 8 (72.73%) of non-augmented vs 7 (43.75%) of augmented patients (Table 2). When further stratified by augmentation type, recurrence rates remained comparable, with 13 (76.47%) colonic augments and 11 (73.33%) ileal augments experiencing recurrence in the percutaneous group, and 4 (50.00%) of colonic augments and 3 (37.50%) of ileal augments in the open group (p = 0.18). Regarding fragmentation, the recurrence rates were comparable across groups, with 5 (100%) patients without fragmentation, 24 (70.59%) with fragmentation, and 15 (55.56%) in the open procedure group experiencing recurrence (p = 0.13) (Table 3). Median time to stone recurrence was 3.01 years for percutaneous cystolitholapaxy and 2.97 years for open cystolithotomy.

Kaplan–Meier estimates of the cumulative incidence of recurrent bladder stones, according to type of surgical procedure.
Discussion
The management of bladder stones in patients with EEC presents unique challenges due to their altered anatomy, attenuated fascia, and increased risk of surgical complications.1–5 For patients with EEC, bladder stones are commonly managed through one of three approaches—endoscopic removal through the continent stoma, percutaneous cystolitholapaxy, or open cystolithotomy.1,2,9,14 Identifying the optimal surgical strategy is crucial in this population, given their unique anatomical considerations and increased vulnerability to complications.1–5 Although both percutaneous cystolitholapaxy and open cystolithotomy are well-established methods, direct comparisons of their efficacy and morbidity in patients with EEC have not been previously reported.8–13 As such, the present study addresses this gap by evaluating these approaches in the EEC population. Notably, our findings highlight the benefits of minimally invasive techniques. Percutaneous cystolitholapaxy was associated with significantly shorter operative times and reduced hospital stays compared with open cystolithotomy (Table 2). Furthermore, this approach demonstrated fewer postoperative complications, specifically a lower incidence of vesicocutaneous fistulas (Table 2). These findings underscore the advantages of percutaneous cystolitholapaxy in minimizing surgical morbidity in this uniquely challenging patient population.
In the current study, patients undergoing percutaneous cystolitholapaxy experienced significant perioperative advantages compared with those treated with open cystolithotomy. Specifically, the percutaneous approach was associated with shorter operative times and reduced hospital stays, highlighting its efficiency and reduced burden on health care resources (Table 2). This advantage was most pronounced in percutaneous cystolitholapaxy without fragmentation, which had the shortest operative times (Table 3). These differences coincided with significantly smaller median stone volumes in the percutaneous group compared with the open group, suggesting that total stone burden may be a key factor influencing operative time (Table 2). In our cohort, larger stones were more often managed with open cystolithotomy, reflecting institutional preference to reserve open procedures for cases with substantial stone burden, given the technical limitations of percutaneous clearance. The longer operative times observed in the open group likely reflect not only the greater stone volume but also the need for extensive exposure, careful dissection, and meticulous closure in the setting of complex anatomy. Importantly, all patients among groups achieved complete stone clearance, underscoring the comparable efficacy of these methods in achieving the primary surgical goal (Table 2). These findings expand on prior studies demonstrating the benefits of minimally invasive techniques, such as reduced operative times and shorter hospitalization durations when compared with open approaches.8,15,16 By combining excellent clinical outcomes with reduced perioperative morbidity, percutaneous cystolitholapaxy aligns with contemporary trends favoring patient-centered, resource-efficient surgical strategies.
Understanding factors that contribute to postoperative complications is essential for optimizing surgical outcomes in patients with EEC. Our findings reveal that patients undergoing percutaneous cystolitholapaxy experienced fewer postoperative complications compared with those undergoing open cystolithotomy, with a significantly higher incidence of vesicocutaneous fistulas observed in the open group (Table 2). This observation aligns with existing literature suggesting that the invasiveness of surgical techniques and the frequency of mucosal disruptions are key contributors to such complications.5,17 We previously reported that repeated mucosal violations in patients with cloacal exstrophy significantly increased the risk of vesicocutaneous fistulas, highlighting the heightened risk associated with open surgical interventions in this population. 5 Mucosal violations, which include procedures involving bladder mucosal opening or closure, are particularly relevant in patients with EEC. 17 Notably, all patients in this study had experienced at least one prior mucosal violation before undergoing their first bladder stone surgery, given their underlying diagnosis and bladder status. Although percutaneous cystolitholapaxy involves a mucosal violation, formation of vesicocutaneous fistulas may depend more on the extent and invasiveness of the procedure. Unlike open cystolithotomy, the percutaneous approach avoids a large abdominal incision and entry into the peritoneal cavity, making it less invasive. Importantly, the specific surgical technique used during open cystolithotomy may further influence complication rates. In the authors’ cohort, a lower midline abdominal approach was routinely used. However, other institutions may advocate for a rectus muscle-splitting incision tailored to bladder position, avoiding midline disruption. These differences in surgical strategy may partially explain variability in reported outcomes across centers. Conversely, although Al-Marhoon et al. reported fewer complications with open cystolithotomy compared with endourological approaches in children, their study did not evaluate these surgical techniques in the context of EEC, limiting its applicability to this unique population. 8 These findings underscore the importance of considering anatomical and procedural nuances when selecting the optimal approach for bladder stone management in patients with EEC.
Bladder stone recurrence is a critical consideration in the long-term management of patients with EEC. 2 Our findings demonstrated a trend toward higher recurrence rates with percutaneous cystolitholapaxy compared with open cystolithotomy, although this difference was not statistically significant (Tables 2 and 3). Residual debris may persist following percutaneous cystolitholapaxy due to limited visualization during the procedure or undetected calculi lodged within tissue pockets created by altered bladder anatomy after augmentation cystoplasty. Notably, the cumulative incidence of recurrence following stone surgery did not differ between the two groups (Fig. 1). These results align with prior studies suggesting that the surgical technique is not a significant determinant of stone recurrence. 12 Instead, recurrence appears influenced by other factors, including recurrent UTIs, suboptimal adherence to clean intermittent catheterization protocols, and acquired risk factors such as prior augmentation cystoplasty or bladder neck transection.1,2 These findings highlight the multifactorial nature of bladder stone recurrence in patients with EEC, suggesting that optimizing postoperative care and addressing modifiable risk factors may be more impactful than the choice of surgical technique in reducing long-term recurrence rates.
Our study has several limitations that warrant consideration. First, its retrospective design introduces inherent biases, as treatment selection may have been influenced by surgeon preference or patient-specific anatomical considerations. Additionally, variability in the surgical approach, including incision size and technique, may depend on surgeon preference. Although no intraoperative complications were observed in our cohort, retrospective data collection may limit the capture of minor events. Furthermore, a notable limitation is the reliance on direct intraoperative visualization to confirm stone clearance, particularly in augmented bladders where residual stones may be obscured due to the complex anatomy and limited visibility during endoscopic inspection. Stone-free rates are determined using CT imaging; however, it is the authors’ practice to limit radiation whenever feasible. Routine postoperative imaging, such as ultrasound, is not typically performed, as annual screening ultrasounds are already a component of the intensive follow-up protocols in patients with EEC, beginning from the time of closure or bladder reconstruction. Additionally, the absence of interim radiological follow-up may have hindered early detection of residual or recurrent stones, which could have contributed to the marginally higher recurrence rate observed with the percutaneous approach. An additional limitation of our study is the lack of standardization in bladder irrigation practices prior to 2021, with protocols varying among patients. In 2021, irrigation with 0.9% saline was standardized for those undergoing bladder reconstruction. Although no significant difference in stone formation or recurrence was observed between pre-2021 and post-2021 cohorts, the variability in irrigation practices prior to 2021 may have influenced the observed trends in stone formation and recurrence. Furthermore, another limitation of our study is the inability to objectively assess patient compliance with bladder irrigation, as adherence to this regimen was not formally monitored and may have varied among individuals. Additionally, a limitation of the study is the disparity in follow-up between percutaneous and open groups. The Kaplan–Meier curve suggests a trend toward longer follow-up in the percutaneous group, though comparisons of follow-up durations showed no significant differences. Variations in follow-up time may still influence recurrence rates, as unaccounted recurrences after loss to follow-up and extended follow-up periods could reveal differences not captured in the current data. Additionally, variability in surgical technique, specifically the use of a lower midline abdominal approach for open cystolithotomy, may influence postoperative complications such as vesicocutaneous fistula formation and may limit the generalizability of our findings to centers using alternative approaches. Furthermore, no mucoid-based stones were identified, which may limit the applicability of our findings to populations in which such stones are more prevalent and typically necessitate open surgical removal. Moreover, the relatively small sample size, reflecting both the rarity of EEC and its specialized management, may have limited the statistical power to detect significant differences in outcomes. This limitation underscores the need for larger, multicenter, prospective studies to validate our findings and provide more robust evidence to guide the optimal surgical approach for patients with EEC.
In conclusion, these data highlight the advantages of percutaneous cystolitholapaxy over open cystolithotomy in the management of bladder stones in patients with EEC. The percutaneous approach demonstrated reduced perioperative morbidity, including shorter operative times and decreased hospital stays while achieving comparable stone clearance rates. Furthermore, percutaneous cystolitholapaxy was associated with a significantly lower incidence of vesicocutaneous fistulas. These findings underscore the importance of tailoring surgical approaches to the unique anatomical and clinical complexities of patients with EEC. Therefore, these results suggest percutaneous approaches may offer a safer and more efficient alternative for managing bladder stones in patients with EEC.
Authors’ Contributions
J.Y.: Conceptualization, data curation, formal analysis, investigation, methodology, visualization, writing—original draft preparation, writing—review and editing. D.H.: Investigation, writing—review and editing. V.M.: Writing—review and editing. C.R.: Writing—review and editing. M.M.: Writing—review and editing. C.M.: Writing—review and editing. H.N.D.C.: Conceptualization, methodology, project administration, resources, supervision, validation, visualization, writing—review and editing. J.P.G.: Conceptualization, methodology, project administration, resources, supervision, validation, visualization, writing—review and editing. C.B.C.: Conceptualization, investigation, methodology, project administration, resources, supervision, validation, visualization, writing—original draft preparation, writing—review and editing.
Footnotes
Author Disclosure Statement
The authors have no financial or personal relationships with other people or organizations that could inappropriately influence their work.
Funding Information
The authors declare no funding for this original article.