
Abstract
Introduction:
This study aims to develop a predictive model for identifying patients at increased risk of prolonged hospital stay after robotic-assisted radical prostatectomy, either via multi-port or single-port techniques, to improve postoperative care and assist in selecting ideal candidates for same-day discharge.
Methods:
The study included patients who underwent robotic-assisted radical prostatectomy at the University of Illinois at Chicago between January 2013 and December 2022. The dataset comprises preoperative variables such as age, race, body mass index, comorbidities, prostate-specific antigen levels, Gleason score, surgical approach, and length of hospital stay. A logistic regression model was employed to predict the likelihood of a hospital stay exceeding 24 hours. The model’s performance was assessed using the area under the Receiver Operating Characteristic curve and fivefold cross-validation.
Results:
The predictive model identified significant factors associated with prolonged hospital stays, including body mass index, prostate-specific antigen levels, Gleason score, surgical approach, and specific comorbidities. The transperitoneal approach was strongly associated with lower chances of same-day discharge, demonstrating an odds ratio of 4.23 (p < 0.00001). The model achieved an accuracy of 73.7% as evaluated by cross-validation.
Discussion:
The nomogram effectively predicts the likelihood of prolonged hospital stay following robotic-assisted radical prostatectomy, enabling surgeons to make informed decisions about patient counseling, surgical planning, and postoperative management. This model may assist in identifying ideal candidates for same-day discharge while improving hospital resource utilization. Future studies should validate this model externally and explore the impact of additional perioperative and social factors.
Introduction
Recent advances in minimally invasive surgery have revolutionized perioperative management, particularly with respect to hospital length of stay (LOS). 1 In many countries where multi-port (MP) robotic surgery is well-established, an overnight stay following robotic-assisted radical prostatectomy (RARP) is the standard practice. 2 However, the introduction of the da Vinci Single-Port system in 2018, which offers a smaller surgical footprint, has shifted the focus toward optimizing postoperative care and improving patient satisfaction. 3
An innovative strategy that has emerged is the implementation of same-day discharge (SDD) protocols, designed to minimize the impact of surgery without compromising patient safety or postoperative outcomes. 4 These protocols, often supported by optimized anesthesia regimens such as total intravenous anesthesia, promise benefits including cost savings, a reduced risk of health care-associated infections, improved patient comfort, and a faster return to normal daily activities. 4 Nonetheless, MP robotic surgery has not consistently demonstrated the feasibility of SDD; indeed, a comparative study by Abaza et al. reported that while SDD is achievable with MP surgery, it is significantly more common in single-port (SP) procedures (51% vs 88%, respectively). 5
Given this background, identifying ideal candidates for SDD is crucial for personalized patient counseling and mitigating uncertainties in inpatient bed management arising from unscheduled admissions following failed SDD attempts. To address this, we aimed to develop a predictive model based on readily available preoperative variables to identify patients at higher risk of prolonged hospital stay after RARP. This nomogram would allow surgeons to objectively evaluate patient-specific variables and make informed decisions regarding postoperative management.
Material and Methods
Our Institutional Review Board approved the project with a study number 2019-0929. The dataset used for this analysis was extracted from the Electronic Health Record (EHR) of patients with prostate cancer who underwent either MP or SP procedures in RARP at the University of Illinois at Chicago between January 2013 to December 2022. All analyses were performed using R statistical software, version 4.3.1.
For each patient, we collected the following variables from the EHR. Age was defined as the patient’s age at the time of surgery. Race (categorized as Hispanic, Black or African American, White, Asian, or Other) was recorded as indicated in the EHR. Body mass index (BMI) referred to the patient’s body mass index. Comorbidity captured the presence of one or more additional medical conditions beyond prostate cancer. A decision was made not to include the Charlson Comorbidity Index (CCI) due to the confounding factor of all patients having a solid tumor—prostate cancer—at the time of surgery. 6 Instead, we listed each comorbidity singularly, as identified from the ICD and CPT diagnosis codes entered in their EHR.7,8 The comorbidities were categorized according to the body system they are associated with. In addition, comorbidity linked to prostatic malignancy was not included as assumed at the time of RARP. PSA indicated the prostate-specific antigen level found in the blood. Gleason score was the grading system used to determine the aggressiveness of prostate cancer, derived from the pathology report of the preoperative prostate biopsy. 9 Approach described whether the surgical method was transperitoneal or extraperitoneal. Finally, hospital stay was the number of hours the patient remained in the hospital following surgery prior to discharge.
We employed a logistic regression model using the variables outlined in the previous section as predictors to predict the probability of a hospital stay lasting over 24 hours. Fivefold cross-validation was used to assess the performance of a predictive model.
Results
A total of 559 patients underwent RARP at our institution between January 2013 and December 2022. After excluding 27 patients with incomplete data and one extreme outlier (hospital stay >2000 hours), 532 patients were included in the final analysis, of whom 82.5% underwent surgery with a transperitoneal approach and 17.5% with an extraperitoneal approach.
The study cohort had a mean age of 59 years. 54.3% of the patients were Black or African American, 20.3% Hispanic, 12.8% White, 11.3% Other, and 1.3% Asian. The median BMI was 28.35 kg/m2. PSA level values demonstrated significant right-skewness, with the median preoperative PSA being 7.80 ng/mL and the average PSA being 16.33 ng/mL. Estimated blood loss had a median of 100 mL, and the median hospital stay was 13 hours (mean 16.26, SD: 15.6 hours; range: 1 to 185, after exclusion of the outlier), indicating considerable variability in postoperative stay. Full summary statistics for these variables are provided in Table 1.
Summary of Demographic, Intraoperative, and Postoperative Information

The multivariable logistic regression model (Table 2) quantifies the impact of each predictor on the odds of a hospital stay exceeding 24 hours. In this model, a one-unit increase in predictors such as BMI, PSA, and Gleason score is associated with a corresponding change in the odds of prolonged hospitalization. Although predictors with p-values greater than 0.05 remain in the model to improve its overall predictive performance, a p-value below 0.05 was considered statistically significant.
Results of the Logistic Regression Model
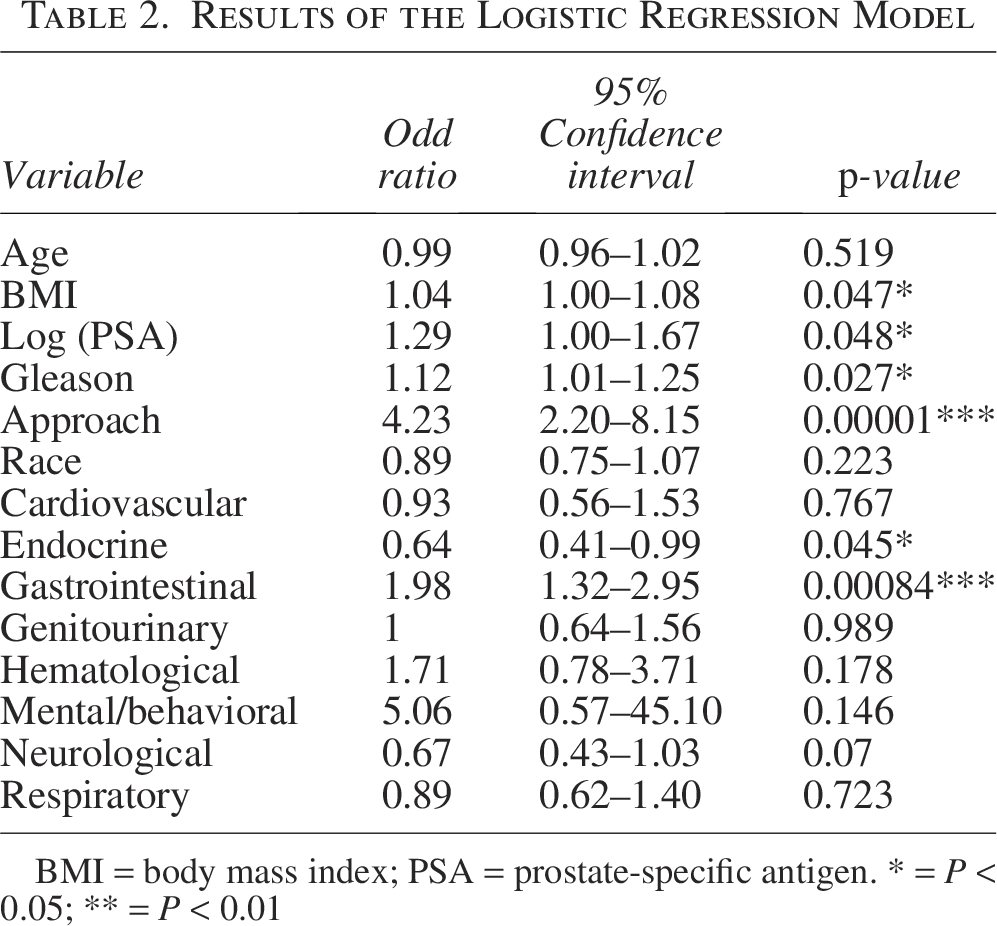
BMI = body mass index; PSA = prostate-specific antigen. * = P < 0.05; ** = P < 0.01
Model performance, assessed via fivefold cross-validation, yielded an overall accuracy of 73.7% (Figure 1).
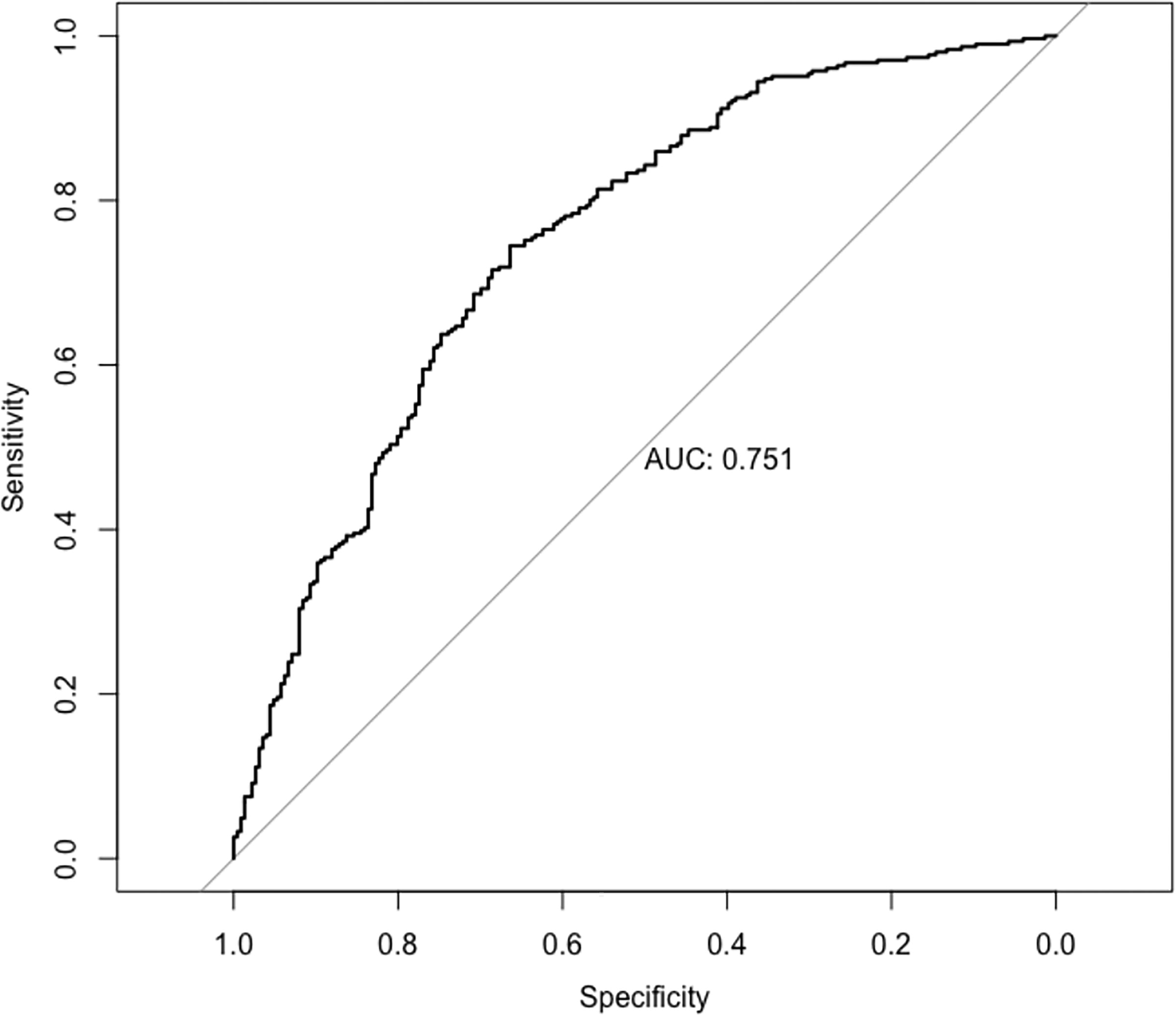
Model accuracy evaluated using AUC under the ROC curve.
To illustrate the clinical utility of the model, we provide example patient scenarios with varying baseline characteristics and their predicted probabilities of a hospital stay exceeding 24 hours in Table 3. These examples demonstrate how the nomogram can assist in preoperative risk stratification and decision-making regarding SDD feasibility.
Example Patient Scenarios with Demographic Characteristics, Comorbidities, and Predicted Probability of Hospital Stay Exceeding 24 Hours Following Robotic-Assisted Radical Prostatectomy, as Calculated by the Study’s Predictive Model

Predicted probability expressed as percentage with associated uncertainty (±standard error of prediction).
CV = cardiovascular comorbidity; EN = endocrine comorbidity; GI = gastrointestinal comorbidity; GU = genitourinary comorbidity; HE = hematological comorbidity; MH = mental health comorbidity; NE = neurological comorbidity; PSA = prostate-specific antigen; RE = respiratory comorbidity.
Clinicians can use the provided nomogram to input individual patient data and calculate the probability of SDD. The nomogram is available at: https://yvvijay121.shinyapps.io/Nomogram.
Discussion
To the best of our knowledge, this is the first study that aims to create a novel predictive model to identify the ideal patients undergoing SDD-RARP. Since its introduction, MP-RARP has shown better intra- and postoperative outcomes regarding blood loss and hospital stay when compared with open surgery. 10 The concept of SDD following RARP was introduced, showing no increase in readmission, emergency visits, and savings in health care costs. 11 Although feasible, SDD was found to be more common in SP procedures. 5 Therefore, it becomes increasingly important to identify the best candidates for outpatient RARP and to develop a safe and cost-effective tool that institutions can utilize. Our study described a predictive model for SDD after RARP, including patients who underwent both MP and SP procedures, considering both preoperative characteristics and intraoperative plans, and several findings are worth mentioning.
First, as already demonstrated in the literature, the SP system is more strongly associated with SDD, showing similar postoperative complications and readmission rates. 5 However, the association between the surgical approach and SDD is noteworthy. In this context, the versatility of the SP system has made it more accessible to perform RARP with an extraperitoneal approach, while transperitoneal access was the most preferred with the MP system. This robust association aligns with previous findings; for example, Uy et al. reported in a recent systematic review that extraperitoneal RARP, even in the context of an MP system, is associated with a shorter hospital stay and reduced rates of postoperative ileus and inguinal hernia formation compared with the transperitoneal approach. 12 In addition, studies comparing these approaches in SP populations have demonstrated that extraperitoneal RARP yields higher rates of SDD. 13 Our model reinforces the importance of the surgical approach, with the transperitoneal technique conferring a fourfold increase in the odds of prolonged hospital stay (OR: 4.23, p < 0.00001).
Second, preoperative factors such as BMI, preoperative PSA, and biopsy Gleason score are significantly associated with a lower chance of SDD. This observation contrasts with earlier work by Banapour et al., which, despite a limited sample size, found no differences in biopsy Gleason score between inpatient and outpatient RARP groups. 14 The roles of Gleason score and PSA in tumor staging—and their influence on decisions regarding the extent of lymph node dissection—appear to affect postoperative LOS, as demonstrated by our data. Unfortunately, we did not collect data on lymph node dissections in this analysis. At our institution, lymph node dissection is guided by the Memorial Sloan Kettering Cancer Center Pre-Radical Prostatectomy Nomogram, 15 with patients scoring >5% routinely referred for lymph node dissection. Detailed data on the number of nodes removed were not captured, limiting our understanding of its effect on hospital stay.
It is also noteworthy that while the literature debates the impact of BMI, our model indicates that SDD after RARP is generally safe regardless of BMI, with only a modest 4% increase in the odds of an extended hospital stay for each one-point rise in BMI. This is consistent with some reports, 16 though other studies have linked obesity with increased morbidity and longer hospitalizations; 17 nonetheless, our findings support the safety of SDD even for obese patients, as also suggested by Agrawal et al. 18
Third, the impact of comorbidities and age in our model offers additional insight into patient selection for SDD. Age was not significantly associated with a higher chance of SDD; in fact, older age, along with cardiovascular, endocrine, neurological, and respiratory comorbidities, emerged as a protective factor. This counterintuitive finding may reflect a more cautious clinical approach in older patients, warranting further investigation into how anesthesia protocols, surgical techniques, and postoperative care can be tailored to optimize outcomes in this group. Future studies should explore potential practice patterns or institutional protocols that may contribute to these findings. In addition, we did not capture key social factors, such as the presence of a partner or caregiver at home, which are known to influence discharge decisions. Incorporating such variables into future models could further improve patient selection for SDD.
This is the first study to develop a predictive nomogram to estimate the risk of prolonged hospital stay following RARP with acceptable accuracy. However, several additional limitations must be acknowledged.
Our study is retrospective and originates from a single center, which inherently introduces selection bias and limits the generalizability of our findings; external validation is essential before the nomogram can be widely adopted.
We did not systematically capture surgical platform (SP vs MP), which limits interpretation of the association between platform, surgical approach, and outcomes.
Due to the confounding factor that all patients had solid organ tumors, we excluded established risk scores such as the CCI 19 and the American Society of Anesthesiologists classification, 20 which may affect perioperative risk assessment. These variables could have provided additional insights for risk stratification in managing patients on the day of surgery.
Start time of the surgery (e.g., late-day surgeries) was not included, although this may influence overnight admissions for logistical rather than medical reasons.
Another important limitation is that we did not record whether a surgical drain was placed. Although the use of drains after RARP is not standard practice at our institution, it is sometimes employed and could affect the length of hospital stay, potentially reducing the generalizability of our findings to centers where drains are routinely used.
We did not assess factors such as patient motivation to be discharged, social determinants of health (such as the availability of home support), the utilization of epidural analgesia, specific pain management strategies, the extent of adhesiolysis or bowel handling during surgery, or the management of bladder spasms—all of which may influence postoperative recovery.
We did not investigate the role of preoperative teaching sessions, introduced in 2022 in our institution for all RARP candidates to better prepare them for SDD. This temporal variation may have influenced our data, as SDD practices appear to have become more common in recent years. 21
Finally, a deliberate decision was made to restrict our analysis to preoperative variables. While incorporating intraoperative factors such as blood loss, duration of surgery, and intraoperative complications might have improved the model’s predictive power, our focus on preoperative data ensures that the nomogram can be used to counsel patients and caregivers-and plan accordingly-prior to surgery, which was the key objective of this work.
Conclusion
The development and implementation of a predictive model to assess the risk of prolonged hospital stay in patients undergoing RARP, whether through MP or SP techniques, represents a significant advancement in optimizing health care delivery and improving patient and caregiver experiences.
Our findings highlight the critical role of the extraperitoneal surgical approach in shortening hospital stays, and the integration of comprehensive preoperative data into the model allows health care providers to make evidence-based decisions regarding postoperative management.
While external validation and inclusion of additional perioperative and social factors are needed to further refine this tool, this study lays the foundation for future external validation and refinement of the nomogram, ultimately paving the way for a more streamlined, efficient, and patient-centered approach to postoperative care in RARP. Only by using such predictive models to identify ideal candidates for SDD can clinicians significantly improve patient outcomes, improve satisfaction, and optimize resource utilization in minimally invasive urological surgeries.
Authors’ Contributions
Conceptualization: L.A.M. and S.C.; Methodology: L.A.M., P.S., and R.C.; Software: P.S. and Y.V.; Formal analysis: L.A.M., P.S., and R.C.; Investigation: A.P., G.P., and D.C.; Resources: S.C. and Y.V.; Data curation: P.S. and Y.V.; Writing—original draft: L.A.M., P.S., and H.K.; Writing—review and editing: L.A.M., P.S., A.P., G.P., D.C., H.K., R.C., and S.C.; Visualization: P.S.; Supervision: L.A.M. and S.C.; Project administration: L.A.M. and S.C.; Funding acquisition: N/A.
Footnotes
Funding Information
There were no funds received for the completion of the study.
Authors’ Disclosures Statement
There are no conflicts of interest to disclose.