
Abstract
Objectives:
One of the major limitations of the current diagnostic techniques for upper urinary tract carcinoma (UTUC) is the risk of both understaging and overstaging, highlighting the need for real-time, high-resolution intraoperative imaging. We evaluated the diagnostic accuracy and safety of ureteral optical coherence tomography (OCT) under ureterorenoscopy for T staging of UTUC.
Materials and Methods:
In this study, patients with suspected UTUC were prospectively enrolled. The safety analysis set included 16 patients who underwent ureteral OCT for ureteral tumors. Because two (13%) patients underwent ureterorenoscopic ablation therapy, the diagnostic accuracy analysis set included 14 of 16 patients who had both ureteral OCT data and a final pathological T (pT) stage from surgical specimens. The concordance, underdiagnosis, and overdiagnosis rates were compared between radiographical imaging-based T (cT) and OCT-based T (octT) diagnoses. The primary outcome was the diagnostic accuracy of ureteral OCT in discriminating between pTis/Ta/T1 (non–muscle-invasive UTUC) and T2/T3 (muscle-invasive UTUC) cancers.
Results:
Concordance between cT-based and pT-based diagnoses was observed in 11 (79%) of the 14 patients, whereas a higher concordance rate (13/14, 93%) was noted for octT diagnosis. Additionally, the underdiagnosis and overdiagnosis rates of octT were 0% and 7.1%, respectively, which were lower than those of cT (7.1% and 14%, respectively). Although no intraprocedural urinary injury was observed, postprocedural complications included hematuria in five patients (31%), urinary tract pain in two (13%), and urinary tract infection in one patient (6.3%).
Conclusion:
Ureteral OCT exhibited a high diagnostic performance in discriminating between non–muscle-invasive UTUC and muscle-invasive UTUC with a safety profile. Further prospective trials with large sample sizes are necessary to determine the true diagnostic value and the wide use of ureteral OCT.
Introduction
Diagnosis of upper urinary tract carcinoma (UTUC) is based on radiographical imaging, ureterorenoscopy (URS), tumor histology, voiding urine cytology, and lavage cytology. A key limitation of current diagnostic techniques is their potential for understaging, undergrading, overstaging, and overgrading. Previous studies have evaluated the discrepancy between clinical staging and grading based on radiographical imaging, URS biopsy, and final pathological staging/grading of radical nephroureterectomy (RNU) specimens.1–3 Clinical understaging/undergrading during preoperative evaluation, as well as upstaging to muscle-invasive disease, are common in the clinical management of UTUC. Several guidelines recommend computed tomography–urography (CT-U) as the primary imaging procedure for detection and tumor staging because of the high diagnostic accuracy of the modality.4–7 Magnetic resonance urography (MRU) is recommended for patients unable to undergo CT-U, mostly when radiation or iodinated contrast media are contraindicated. 8 However, CT-U is more sensitive and specific for the diagnosis and staging of UTUC compared with MRU. 9
Honda et al. developed detailed criteria to differentiate between T2 and T3 ureteral tumors, with a special focus on smooth or irregular margins. 10 The diagnostic sensitivity and specificity were 87.5% (14/16) and 92.9% (13/14), respectively, for T3 ureteral tumors. 10 However, a significant lack of highly accurate imaging tools and techniques exists to differentiate Tis, Ta, T1, and T2 tumors. Recent guidelines recommend kidney-sparing surgery, including endoscopic ablation or segmental ureterectomy, for those with low-risk UTUC tumors or selected patients with high-risk UTUC.4,5 Thus, accurate T staging, tumor grading, and preoperative risk assessment are vital for planning risk-adapted treatment strategies.
Over the past two decades, real-time intraoperative imaging devices, including optical coherence tomography (OCT) and endoluminal ultrasound (ELUS), have been investigated for the following ureteral diseases: UTUC, stricture disease, and pelvic-ureteric junction obstruction. 11 Ureteral ELUS provides 360° imaging with a penetration depth of 15–20 mm, whereas ureteral OCT offers high-resolution imaging with a shallow penetration depth of 2–3 mm. 12 Bus et al. performed OCT, ELUS, and CT imaging on RNU specimens resected from patients with UTUC and compared the coregistered OCT and ELUS datasets with corresponding histopathology findings. 13 The authors concluded that OCT could provide high-resolution imaging of normal ureters and ureteral tumors, whereas ELUS had limited value in terms of low differentiation between noninvasive and invasive ureteral carcinomas.
Although OCT has been increasingly utilized in cardiology and ophthalmology, its use and evidence in urologic malignancies remain limited. 14 This study aimed to evaluate the diagnostic accuracy and safety of ureteral OCT for the T staging of UTUC.
Materials and Methods
Study design
DiagNostic accuracy of Optical Coherence Tomography for patients with UReteral caNcer was a prospective, single-center, single-arm study, abbreviated as NOCTURN study, which was conducted at Nara Medical University Hospital. This study was approved by the ethics committee, and all participants provided informed consent (reference ID: 3442). The clinical trial was prospectively registered with the University Hospital Medical Information Network Clinical Trials Registry on December 1, 2022 (reference number: UMIN000049594). The URL for the trial registry records is available at https://center6.umin.ac.jp/cgi-open-bin/ctr_e/ctr_view.cgi?recptno=R000056480. This study complied with the Declaration of Helsinki regarding human investigations. Informed and written consent forms were mandatory before participating in the study. The details of the study design, inclusion/exclusion criteria, intervention, and primary/secondary outcomes are illustrated in Figure 1. After screening and registration, the patients were enrolled in a single intervention group undergoing ureteral OCT under URS.
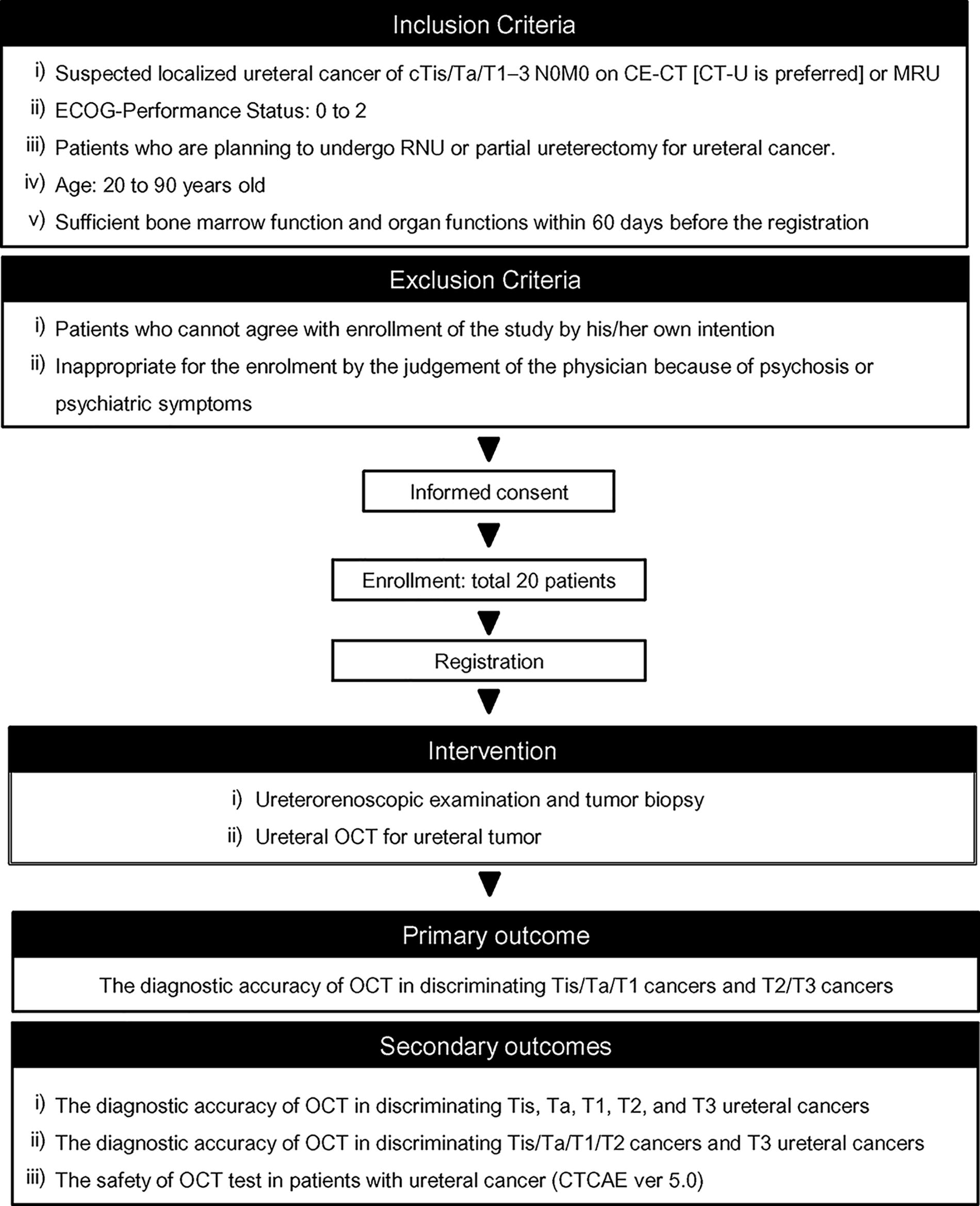
Design of the NOCTURN study: inclusion criteria and study outcomes. CE-CT = contrast-enhanced computed tomography; CKD = chronic kidney disease; CTCAE = Common Terminology Criteria for Adverse Events; ECOG-PS = Eastern Cooperative Oncology Group performance status; MRU = magnetic resonance imaging urography; RNU = radical nephroureterectomy; OCT = optical coherence tomography.
As this trial was performed as a pilot and feasibility study for a future full trial, the target sample size was not determined using descriptive statistics. According to a review of sample sizes for the pilot and feasibility studies in the United Kingdom Clinical Research Network database and the International Standardized Randomized Controlled Trial Number (ISRCTN) registry, the median target sample size per arm was 36 (range: 10–300) for trials with a dichotomous endpoint and 30 (range: 8–114) for those with a continuous endpoint. 15 Considering that the primary endpoint of this study was dichotomous and the average number of patients with ureteral cancer per year in our hospital was 10–15, we pragmatically planned to include a total of 20 cases in this study.
Procedures of diagnostic URS, ureteral OCT, and tissue biopsy
Diagnostic URS and ureteral OCT were performed by two experienced urologists (M.M. or T.S.) using semirigid (7F, Karl Storz or 7.8F, Olympus) and flexible ureterorenoscopes (7.5F Flex-X2, Karl Storz or 9.9F URF-V, Olympus) as appropriate. Biopsies were obtained after ureteral OCT measurement from visible lesions or at random in cases with suspected carcinoma in situ suspicion using disposable cup biopsy forceps (Shoei Japan Co., Ltd., Osaka, Japan).
An SJM FD-OCT integrated imaging system (Abbott Medical Japan Co., Ltd. and LightLab Imaging, Inc.) interfaced with a single-use Dragonfly OpStar™ imaging catheter probe (Abbott Medical Japan Co., Ltd., LightLab Imaging, Inc., and St. Jude Medical, Atrial Fibrillation Division, Inc.) was employed for ureteral OCT measurement. The sideward-looking OCT probe was introduced through an 8F ureteral stent placed at the distal location with the macroscopic presence of the tumor or suspected lesions. The probe position was confirmed by endoscopic and radiographical imaging using a mobile C-arm device (Shimadzu Corporation, Kyoto, Japan). The OCT, connected to a rotary junction with a pull-back system, scanned a longitudinal trajectory of 54 mm in approximately 5.4 seconds, producing a 540-frame helical dataset of raw OCT amplitude data. Previous studies have demonstrated that the urothelium, basement membrane, lamina propria, and muscularis propria can be distinguished using ureter OCT imaging.13,16 The OCT images were analyzed to determine the OCT-based T stage (octT) after surgery by two urologists (Y.O. and T.M.) who were blinded to URS examination, OCT measurement, and clinicopathologic information, including clinical T (cT) stage, pathological T (pT) stage, and tumor grade from biopsies and resection specimens.
Preoperative clinical T staging of ureter cancer
The 8th edition of the TNM Classification of Malignant Tumors 17 defines the T stage as follows: Ta, noninvasive papillary carcinoma; Tis, carcinoma in situ; T1, invasion of the lamina propria (subepithelial connective tissue); T2, invasion of the muscularis propria; T3, invasion beyond the muscularis into periureteric fat; and T4, invasion involving adjacent organs or perinephric fat. If the use of contrast media was contraindicated because of renal dysfunction, MRU was allowed in this study (only one patient with 31.8 mL/min/1.73 m2 of estimated glomerular filtration rate [eGFR] in this study). Experienced uroradiologists performed the radiographical examinations. Preoperative cT stage was determined comprehensively based on tumor appearance (papillary, nodular, and flat) on URS imaging and contrast-enhanced CT (CT-U was preferred if available) or MRU6,10,18 as follows: cTa, papillary-pedunculated appearance on URS and a smooth external surface on radiographical imaging; cTis, flat appearance on URS and a symmetrical circumferential ureteral wall thickening/a smooth external surface on radiographical imaging; cT1, mixture of papillary and nodular appearance on URS and a smooth external surface on radiographical imaging; cT2, nodular appearance on URS and a smooth external surface with mild spiculation around tumor lesion on radiographical imaging; cT3, nodular appearance on URS and an irregular external surface or conspicuous spiculation around tumor lesion on radiographical imaging.
Pathological tumor grading and pT staging of ureter cancer
URS biopsies and RNU specimens were pathologically evaluated by the Department of Diagnostic Pathology according to a standardized protocol. Tumor grade and pT were determined according to the 2004/2016 World Health Organization classification 19 and the 8th edition of the TNM Classification of Malignant Tumors. 17 Neoadjuvant systemic chemotherapy could modulate and downstage the tumor stage and grade. No patient received neoadjuvant chemotherapy (NAC) in our cohort.
Collection of baseline data and follow-up data
The baseline clinicopathological characteristics of the patients included age, sex, tumor location, tumor laterality, and laboratory data at URS examination obtained within 60 days prior to the day of URS. Follow-up laboratory data and urinalysis on post-URS days 0 (immediately after URS), 1, and 14 were gathered for safety assessment. Adverse events accompanied by URS and ureteral OCT were evaluated and graded prospectively using the Common Terminology Criteria for Adverse Events (CTCAE) version 5.0. Renal function was evaluated using the modification of diet in renal disease study formula for Japanese patients: eGFR mL/min/1.73 m2 = 194 × serum creatinine−1.094 × age−0.287 (×0.739, for women). 20 Baseline eGFR was defined as the pre-RNU data closest to the surgical date, within 30 days of surgery, and after completion of NAC. Chronic kidney disease (CKD) stages were defined according to the eGFR values as follows: CKD stage 1 (eGFR ≥ 90), 2 (60 ≤ eGFR < 90), 3a (45 ≤ eGFR < 60), 3b (30 ≤ eGFR < 45), 4 (15 ≤ eGFR < 30), and 5 (eGFR < 15). 21
Results
Figure 2 displays a flowchart describing the patient cohorts for this study. Sixteen patients underwent ureteral OCT for ureter tumors, and the diagnostic accuracy analysis set included 14 of these from the safety analysis set who had both ureteral OCT data and final pT from the surgical specimen. None of the patients received any NAC. Baseline demographics of the two analysis sets are presented in Table 1. Among the 16 patients in the safety analysis set, 6 (38%), 8 (50%), and 2 (13%) underwent RNU, partial ureterectomy (PU), and URS ablation therapy, respectively.
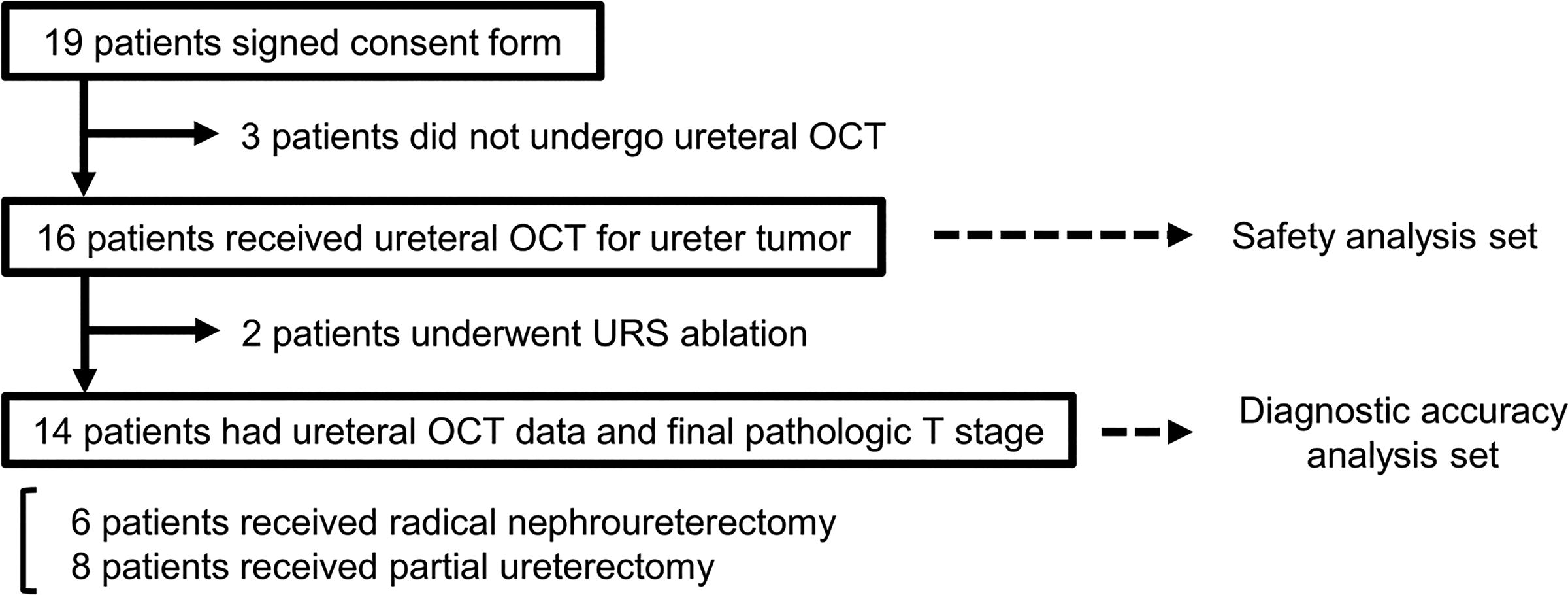
Flowchart describing patient cohorts of the NOCTURN study: diagnostic accuracy set and safety analysis set.
Characteristic of Patients with Ureteral Cancer Undergoing Ureteral Optical Coherence Tomography
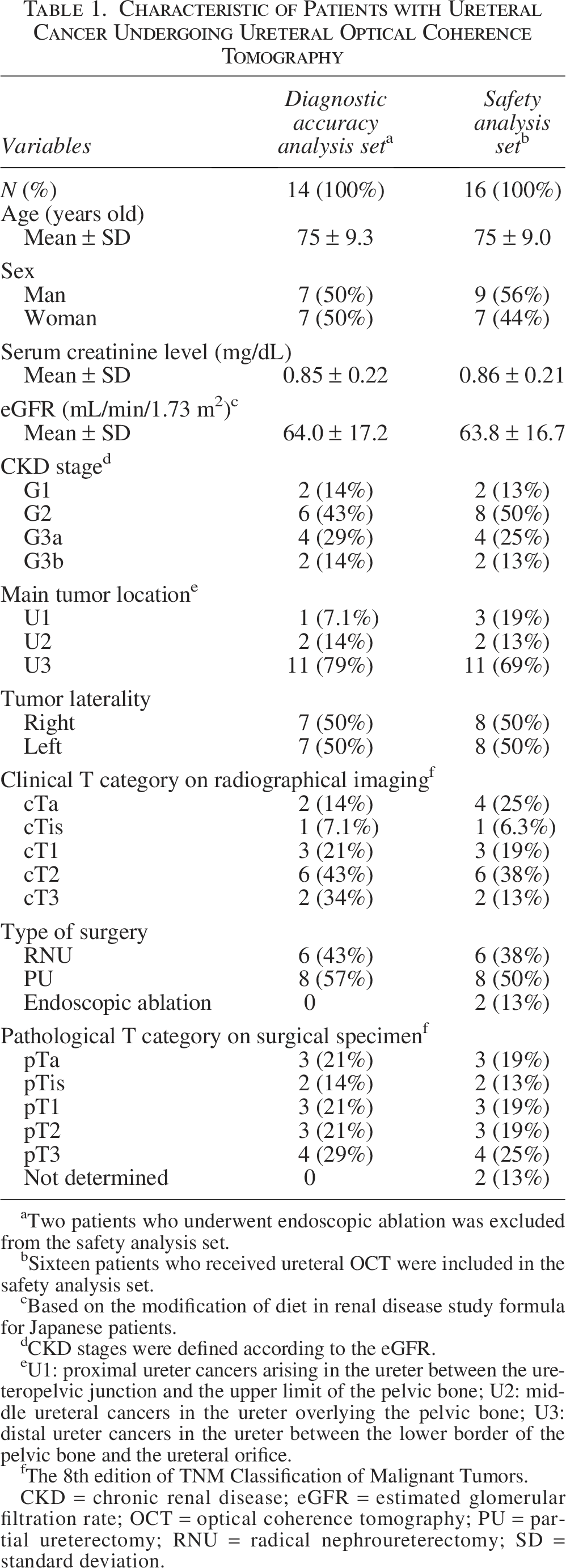
aTwo patients who underwent endoscopic ablation was excluded from the safety analysis set.
bSixteen patients who received ureteral OCT were included in the safety analysis set.
cBased on the modification of diet in renal disease study formula for Japanese patients.
dCKD stages were defined according to the eGFR.
eU1: proximal ureter cancers arising in the ureter between the ureteropelvic junction and the upper limit of the pelvic bone; U2: middle ureteral cancers in the ureter overlying the pelvic bone; U3: distal ureter cancers in the ureter between the lower border of the pelvic bone and the ureteral orifice.
fThe 8th edition of TNM Classification of Malignant Tumors.
CKD = chronic renal disease; eGFR = estimated glomerular filtration rate; OCT = optical coherence tomography; PU = partial ureterectomy; RNU = radical nephroureterectomy; SD = standard deviation.
Adverse Events After Ureterorenoscopy with Ureteral Optical Coherent Tomography

CTCAE = Common Terminology Criteria for Adverse Events.
Figure 3 demonstrates two representative cases of ureteral cancer that underwent preoperative URS with tumor biopsy and ureteral OCT in the diagnostic accuracy analysis set. High-resolution axial imaging obtained by OCT was able to distinguish the layers of the urothelium, lamina propria, muscularis propria, and periureteral fat in a normal ureter wall, as previously reported.13,16 In a 74-year-old man with right middle to distal ureteral tumors, perioperative octT staging was concordant with pT staging of cross-sectional RNU specimens (Fig. 3A). In contrast, an 87-year-old man was diagnosed with a right distal ureteral tumor demonstrating overstaging in the preoperative cT staging (cT1) and octT staging (cT1) according to the corresponding pT staging (pTa).
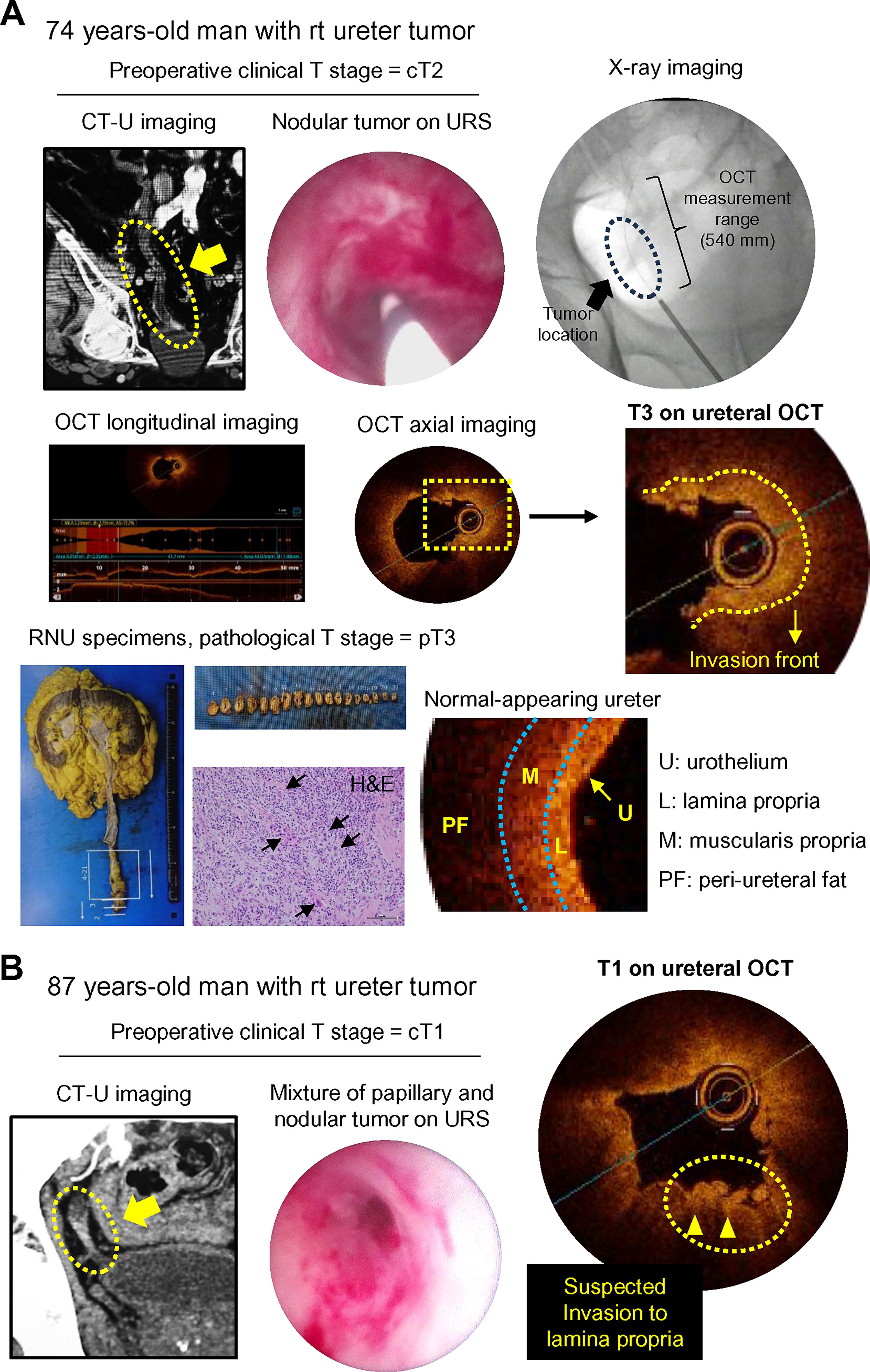
Two representative cases with ureteral cancer receiving preoperative ureterorenoscopy (URS) with ureteral optical coherence tomography (OCT).
The diagnostic performance of cT and octT in the 14 patients with ureteral cancer is illustrated in Figure 4. The primary outcome of this study was the diagnostic accuracy of ureteral OCT in discriminating between pTis/Ta/T1 cancers (non–muscle-invasive urothelial carcinoma, NMIUC) and T2/T3 cancers (muscle-invasive UC, MIUC) (Fig. 4A). Concordance between cT and pT diagnoses was observed in 11 (79%) of the 14 patients, whereas a higher concordance rate (13/14, 93%) was noted for octT diagnosis. Additionally, the underdiagnosis and overdiagnosis rates of octT were 0% and 7.1%, respectively, which were lower than those of cT (7.1% and 14%, respectively). Similar results were observed for the secondary outcomes: the diagnostic accuracy of OCT in discriminating Tis, Ta, T1, T2, and T3 ureteral cancers (Fig. 4B), as well as in discriminating Tis/Ta/T1/T2 cancers and T3 ureteral cancers (Fig. 4C). Remarkably, the concordance rate of octT staging was almost twice that of cT staging (57% and 29%, respectively).

Tabulation displaying diagnostic performance of preoperative cT diagnosis and octT diagnosis in ureter cancer.
Finally, we evaluated URS/OCT-related adverse events using ureteral OCT according to CTCAE version 5.0 (Table 2). Although no intraexamination urinary injury was noted, hematuria, urinary tract pain, and urinary tract infection were observed in five (31%), two (13%), and one (6.3%) patients, respectively. No significant changes were detected in the laboratory data examined on day 14 compared with the baseline data.
Discussion
This study investigated the diagnostic performance of ureteral OCT in 14 patients with ureteral cancer. We compared preoperative cT and octT diagnoses with final pT diagnosis from surgical specimens and identified that the concordance rate was higher for octT diagnosis than for cT diagnosis in the primary and secondary outcomes. Consistently, the underdiagnosis and overdiagnosis rates were lower for octT tumors than for cT tumors. As OCT was initially reported in 1991, the modality has been clinically tested across a diverse set of medical and surgical applications, including ophthalmology, cardiology, gastroenterology, dermatology, oncology, and urology. 22 However, experience and evidence in urologic malignancies remain scarce, partly because of several minor limitations, including high cost and low penetration depth and angle. The target urogenital organs included the bladder, ureter, renal pelvis, kidney, prostate, and scrotum. 23 Among these, ureteral OCT is expected to be a useful diagnostic tool for ureteral cancer, particularly for differentiating small and flat tumors.
Kidney-sparing surgery, such as PU and URS tumor ablation, can be selected for low- or high-risk UTUC.24,25 Accurately differentiating NMIUC from MIUC is crucial for informing future treatment plans, as lymph node dissection is typically unnecessary in patients with Ta/T1 NMIUC. 26 A previous case series of 26 ureters reported that ureteral OCT sensitivity and specificity for tumor invasion were 100% and 92%, respectively, with 83% of lesion staging matching the histological diagnosis. 27 Our findings revealed similar outcomes, with a 93% concordance rate in the analysis of ureteral OCT (octT diagnosis) for discriminating between NMIUC and MIUC, which was superior to radiographical imaging (79%, cT diagnosis). However, further evaluation is needed to assess the reproducibility of the diagnostic performance of ureteral OCT, such as interobserver variation, inter-URS examiner variation, and the learning curve for the assessment. Visualizing and accessing the upper urinary tract using URS and stable ureteral OCT would require expertise and training.
One of the technical limitations of OCT imaging is that the depth of scattering imaging is limited to about 2 mm. This study focused on patients with ureter cancer because the lumen of renal pelvis is anatomically wider compared with the ureter, and many of the renal pelvic tumors are large papillary exophytic masses. For the exophytic ureter tumor, we tried to place the OCT probe close to the tumor pedicle to obtain the image of tumor invasion front. Future improvement by increasing OCT imaging depth would solve this limitation. Another problem is diagnostic accuracy of Tis tumors. We had only two cases with pTis ureteral cancer in our cohort. Correct staging was given in one patient, and overstaging was given in another patient with only 50% of the diagnostic accuracy. We still accumulate the experience of octT testing for Tis tumors. In addition, we have to consider potential practical barriers to clinical adoption of OCT use to urologic field. The OCT testing requires expensive integrated imaging system and a single-use imaging catheter probe, which costs approximately 130,000 Japanese yen (equivalent to about 1000 USD as of July 2025).
To date, many efforts have been made to develop clinically applicable tools to predict the tumor grade and stage preoperatively in patients with UTUC. A recent publication demonstrated the potential of radiomics analyses using CT-U data combined with machine learning for grading and staging UTUC, comparing the performance with that of URS examination with tumor biopsies. 28 Among the 11 predictive models, the logistic regression model demonstrated the best performance with a sensitivity of 83% and specificity of 76% in UTUC staging, concluding that radiomics-based machine learning algorithms could provide a useful tool to predict preoperative UTUC grade and stage with implications for routine clinical practice. Another promising technology for cancer diagnosis is liquid biopsy, which utilizes plasma circulating tumor deoxyribonucleic acid (ctDNA). Huelster et al. investigated the potential of ctDNA as a predictor of MIUC/non–organ-confined UTUC in 30 patients with high-risk UTUC. 29 Preoperative ctDNAs were sequenced using a 152-gene panel and low-pass whole-genome sequencing. The detection of at least two panel-based molecular alterations yielded 71% sensitivity and 94% specificity for predicting MIUC/non–organ-confined UTUC. A combination of multiple diagnostic modalities, such as OCT, radiomics-based machine learning algorithms, plasma ctDNA, and urine biomarkers, is needed to increase the diagnostic accuracy of perioperative UTUC staging.
This study has some limitations as follows. First, this study is the single-center, small-scale design (20 planned total cases) with limited statistical power. Reproducibility, and generalizability of ureteral OCT should be validated in a future full trial. Second, this study did not include interobserver variability and learning curve of the OCT testing. The OCT procedure requires only simple endoscopic technique and took approximately 5 minutes on average. Specific caution and experience would be needed to evaluate the recorded OCT imaging. Third, this study evaluated only short-term outcomes including diagnostic performance and safety. Long-term outcomes, including oncologic and prognostic benefits, should be discussed in the future.
In conclusion, we reported the superior diagnostic performance of ureteral OCT for radiographical imaging diagnosis in patients with ureteral cancer. Further prospective trials with large sample sizes are necessary to determine the true diagnostic value and the wide use of ureteral OCT.
Authors’ Contributions
All authors contributed to the study conception and design. M.M.: Conceptualization, writing—original draft, data curation, formal Analysis, investigation, methodology. T.S., N.N., T.U., and K.Y.: Data curation, investigation, methodology. Y.O., T.M., and T.F.: Formal analysis, investigation. M.T., T.O., K.I., K.O., S.H., Y.M., D.G., and Y.N.: Resources, investigation. M.W. and N.T.: Supervision, methodology. K.F.: Writing—review and editing, conceptualization, project administration, supervision. All authors read and approved the final article. Each of the coauthors acknowledges their participation in conducting the research leading to this article and has agreed to its submission to be considered for publication.
Footnotes
Author Disclosure Statement
The authors have no relevant financial or nonfinancial interests to disclose.
Funding Information
This study was funded by The Japanese Urological Association Research Grant 2023.