
Abstract
Purpose:
Ureteral complications are among the most common types of complications following kidney transplantation (KT). In the past, these complications were often managed using endoscopic and open surgical approaches. However, the robot-assisted approach has been recently implemented. Nevertheless, the available data regarding the potential impact of robotic surgery in this field are sparse. This systematic review (SR) aims to summarize the available evidence of robot-assisted ureteral reconstruction following KT, focusing on postoperative outcomes and complications.
Methods:
Studies eligible for inclusion focused on evaluating the success and/or complications associated with robot-assisted ureteral reconstruction after KT. An SR was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. The literature search was performed using the Web of Science, PubMed, and Scopus databases, with no restrictions on the time period. Only articles published in English were considered.
Results:
After screening 5337 publications, this SR included 9 studies with a total of 127 patients. The most common indication for reconstruction was ureteral stricture (n = 108, 85%), and the most frequently performed procedure was ureteroneocystostomy (n = 59, 46.8%). Following robot-assisted ureteral reconstruction procedures, the average success rate was 91.3%. Regarding intraoperative complications, six patients (4.7%) required conversion to open surgery. As for postoperative complications, the number of patients experiencing Clavien–Dindo Grade 1, 2, 3, and 4 complications were 15/121 (12.4%), 20/121 (16.5%), 4/121 (3.3%), and 2/121 (1.6%), respectively.
Conclusion:
With the advancements in robotic platforms as well as KT surgeons’ expertise in minimally invasive surgery, robot-assisted ureteral reconstruction after KT is increasingly recognized as a safe and effective option for recipients with ureteral complications.
Introduction
Kidney transplantation (KT) is the gold-standard treatment for patients with end-stage renal disease, significantly improving quality of life and providing notable survival benefits. 1 However, KT is not without complications, a substantial portion of which are urological, primarily involving the transplanted kidney’s ureter. 2 Various reconstruction options are available for patients with ureteral complications following KT, including balloon dilations, ureteroneocystostomy, native or transplant ureteroureterostomy, pyelovesicostomy, pyeloureterostomy, or Boari flap procedures.3–5
Traditionally, these complications have been treated with reconstruction procedures performed through open surgery or endoscopic approaches. 6 However, in recent years, robot-assisted reconstruction has been implemented in referral centers, driven by the growing adoption of robotic surgery and advancements in surgical expertise.7–15 Despite these advancements, the outcomes of robot-assisted ureteral reconstruction procedures following KT have been reported in only a limited number of studies.
In this systematic review (SR), we aimed to assess the efficacy of robot-assisted ureteral reconstruction after KT, focusing on intra- and postoperative complications.
Materials and Methods
Data sources and searches
The review was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. This investigation included searches in the Web of Science, PubMed, and Scopus databases until January 2025. In PubMed and Web of Science, searches covered all fields, while in Scopus, the search was limited to article titles, abstracts, and keywords. This SR was registered under the protocol registration number CRD420250654622/PROSPERO.
Terms utilized for the search comprised: (“Robotic-assisted” OR “Robotic” OR “Minimally Invasive”) AND (“Kidney Transplantation” OR “Renal Transplantation” OR “Renal Transplant” OR “Kidney Transplant” OR “Kidney Graft” OR “Transplant Ureter” OR “Ureteroureterostomy” OR “Ureteroneocystostomy” OR “Pyeloureterostomy” OR “Ureteral Reconstruction” OR “Ureteral Stricture”).
Study selection
In order to meet the inclusion criteria, studies needed to evaluate the success and/or complications associated with robot-assisted reconstruction procedures in KT patients. All study designs were considered, except for reviews, editorials, book chapters, case reports, and studies published solely as conference abstracts. Studies involving four or fewer patients, classified as case series, were excluded from consideration. 16 Only studies published in English were included, and no restrictions were applied to the publication time or follow-up period. Two authors (H.B.H. and A.P.) independently reviewed the titles and abstracts of all screened studies. Subsequently, the full texts were assessed for eligibility. Any disagreements during the study selection process were resolved by a third author (A.T.).
Data collection and extraction
Two authors (H.B.H. and A.P.) independently extracted data from included reports, and any discrepancies were resolved by a third author (A.T.). A detailed data-extraction sheet encompassing various parameters—author’s name, journal’s name, year of publication, study country, recruitment period, total number of patients with robot-assisted reconstruction procedures after KT, reason for reconstruction surgery, prior reconstruction procedures, reconstruction surgery type, recipient age (years), recipient sex, recipient’s body mass index (BMI; kg/m2), conversion to open surgery rate, success rate, procedure time (minutes), intraoperative complications rate, postoperative complications and major postoperative complications rate (Clavien–Dindo classification ≥3), 17 and length of hospital stay—was created for this purpose. The post-procedure graft function was evaluated with 1-year, 5-year, 10-year, and last estimated glomerular filtration rate (mL/min/1.73 m2) and with 1-year, 5-year, 10-year, and last serum creatinine. Moreover, 1-year, 5-year, 10-year, and last graft survival rates and follow-up period (years) were considered.
Risk of bias assessment
Two reviewers (H.B.H. and A.P.) independently assessed the risk of bias (RoB) for each study included in the analysis. Any disagreements between their evaluations were resolved by a third reviewer (A.T.). The RoB assessment was performed using the Risk of Bias in Non-Randomized Studies—of Interventions, Version 2 (ROBINS-I) tool. 18 Since the analysis incorporated nonrandomized studies, a predefined list of key potential confounders, identified by the Young Academic Urologists Kidney Transplantation Working Group, was utilized to enhance the tool. These confounders included the interval between reconstruction and KT, the grade of vesicoureteral reflux (VUR), as well as the length and location of the stricture. Each study was carefully examined to assess whether these confounders were accounted for. Traffic light systems were used to evaluate the RoB in the included studies, with color coding: red for high risk, amber for moderate risk, and green for low risk.
Data synthesis
Given that this SR focused exclusively on outcomes following robot-assisted ureteral reconstructions, a narrative synthesis of the data was conducted instead of a quantitative analysis and meta-analysis. The primary outcomes assessed were the success rates of robot-assisted ureteral reconstructions, while secondary outcomes included intra- and postoperative complications. Studies that reported medians descriptively were converted into mean values using an appropriate method and then included in the analysis. 19 In this SR, conversion to open surgery—regardless of the procedure’s outcome—was considered a failure in postoperative success outcomes.
Results
Research results, patient demographics, and preoperative characteristics
After identifying 5337 publications and removing duplicates, 3327 articles were screened. Nine studies that met the inclusion criteria were selected, ultimately including 127 patients in the final analysis (Fig. 1). The studies analyzed were published between 2017 and 2024. The majority of patients included in this SR were from the United States. Gender information was unavailable for six patients, while among the remaining participants, males were more prevalent (n = 66 vs n = 55). The mean age of patients at the time of reconstruction was 55 years. An analysis of reconstruction indications showed that 108 patients (85%) underwent surgery for ureteral stricture, 18 (14.2%) for VUR, and 1 (0.8%) for a urinary leak. Table 1 summarizes study characteristics, patient demographics, and indications for reconstruction.

Flowchart of the study according to the PRISMA guidelines. PRISMA = Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Study and Patient Characteristics from the Included Studies
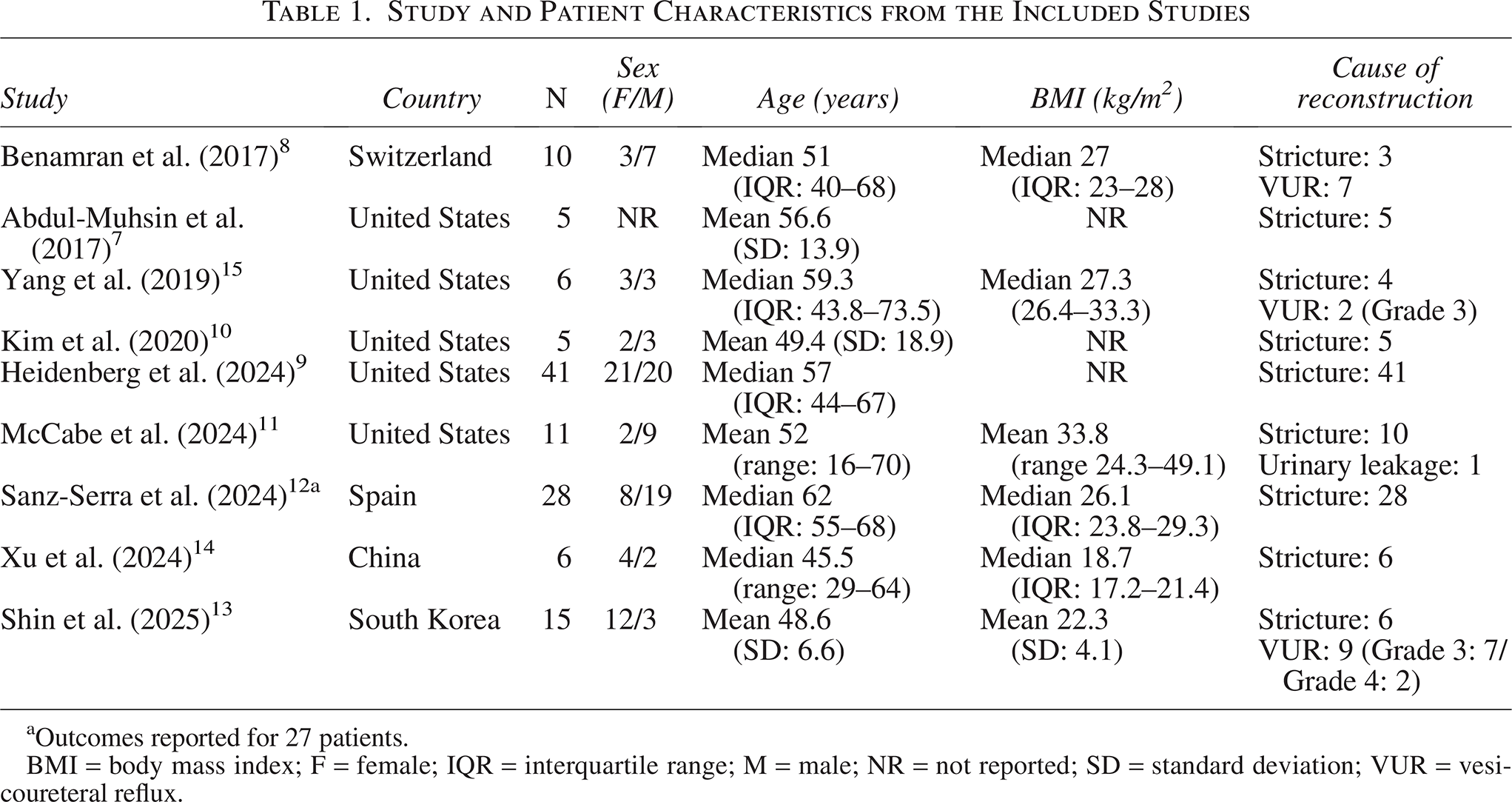
aOutcomes reported for 27 patients.
BMI = body mass index; F = female; IQR = interquartile range; M = male; NR = not reported; SD = standard deviation; VUR = vesicoureteral reflux.
Ureteral pathologies and reconstruction procedures
Evaluation of ureteral pathologies revealed that among the 18 patients with VUR, 9 (50%) had Grade 3, 2 (11.1%) had Grade 4 VUR, whereas the reflux grade was unspecified in 7 (38.9%). Among the 108 patients with ureteral strictures, 30 (27.8%) had proximal, 7 (6.5%) had mid, 56 (51.9%) had distal, and 7 (6.5%) had full-length strictures, while the data were unavailable for 8 (7.4%) patients (Table 2).
Stricture and Reconstruction Procedure Features of Included Patients

aOutcomes reported for 27 patients.
IQR = interquartile range; NR = not reported; SD = standard deviation; UNC = ureteroneocystostomy.
Details on prior interventions were reported in six studies. In two cases, a robot-assisted approach was performed following previous open revision surgery.7,9 Regarding reconstruction procedures, ureteroneocystostomy was the most common, performed in 59 patients (46.8%), followed by pyeloureterostomy in 22 (17.5%), Boari flap in 14 (11.1%), ureteroureterostomy in 13 (10.3%), pyelovesicostomy in 12 (9.5%), psoas hitch in 5 (4%), and a combined Boari flap and psoas hitch in 1 patient (0.8%). In patients who required reconstruction for VUR, six (33.3%) underwent Lich–Gregoir ureteroneocystostomy, whereas the others were managed with other reconstructive techniques (Boari flap, pyeloureterostomy, or ureteroureterostomy).
Surgical outcomes and postoperative complications
The mean duration of follow-up was 24 months. The operation time was provided in only 6 studies, and console time was specifically mentioned in one study. 13 Based on the evaluation of these studies, the average hospital stay was 4 days. Among the studies, postoperative success rates ranged from 50% to 100%, with an average of 91.3%.
Table 3 provides a comprehensive overview of intraoperative and postoperative complications among the 127 patients included. In terms of intraoperative complications, conversion to open surgery was required in only six patients (4.7%). Open conversion was necessary in three patients owing to adhesions that compromised procedural safety, and in another three patients due to the inability to identify the graft ureter or pelvis. Regarding postoperative complications, data were available for 121 patients. Clavien–Dindo Grade 1 and 2 complications were the most frequently reported, occurring in 15 (12.4%) and 20 (16.5%) patients, respectively. Grade 3 and 4 complications were less common, affecting 4 (3.3%) and 2 (1.6%) patients, respectively. One study noted that all complications were of low grade (Clavien–Dindo Grade 1–2) and that no high-grade complications were observed; however, specific details were not provided. 14 Among Grade 2 complications, infections—including urinary tract infections (UTIs) and orchitis—were the most prevalent, affecting 15 patients (12.4%), while 4 patients (3.3%) required blood transfusions. Although high-grade complications were less frequent, ileus (1.6%), pelvic abscess requiring washout (0.8%), kinking of the JJ stent requiring decompression via a nephrostomy tube (0.8%), sepsis (0.8%), and systemic tuberculosis (0.8%) were reported. This last complication occurred in a patient with multiple strictures of the urinary tract due to undiagnosed urinary tuberculosis at the time of surgery, which later progressed to severe systemic tuberculosis under immunosuppression. 12
Outcomes and Complication of the Included Studies

aOutcomes reported for 27 patients.
CTU = computed tomography urography; IQR = interquartile range; OC = open converted; RC = robotic completed; SD = standard deviation; US = ultrasound; UTI = urinary tract infection; VCUG = voiding cystourethrography; VUR = vesicoureteral reflux.
-> = VUR regression from grade 4 to 1.
Risk of bias assessment
Out of the nine studies, six exhibited a moderate RoB, while three displayed a low risk. Figure 2 presents the traffic light plot illustrating the RoB domains assessed using the ROBINS-I Version 2 tool for the studies encompassed in this SR. This tool indicated a generally low to moderate RoB across most assessed items. However, a moderate RoB was observed in areas related to confounding, outcome measurement, selection of reported results, and overall bias (Fig. 2).

“Risk of bias” assessment for each included study according to the Risk of Bias in Non-Randomized Studies—of Interventions, Version 2 tool.
Discussion
Robot-assisted surgery is becoming increasingly prevalent in the field of KT.20–22 In addition to its role in donor and transplantation procedures, robotic surgery has been implemented for managing postoperative complications. However, available data remain limited. Despite this, an evaluation of existing studies suggests that these procedures achieve high success rates with acceptable intraoperative and postoperative complication rates.
Particularly, this SR showed that the postoperative success rate of robot-assisted ureteral reconstruction for ureteral complications after KT ranged from 50% to 100%, with an average of 91.3%, highlighting its potential efficacy. Additionally, robot-assisted procedures have demonstrated feasibility even after open revision surgery7,9 or in patients with high BMI. 11 However, the success criteria were heterogeneous across included studies. While some studies relied on objective radiological parameters,9,10,13,14 others used graft function or clinical improvement alone as the measure of success.7,8,11,12 In one study, urinary strictures were evaluated using radiological imaging, while clinical improvement was considered sufficient in VUR patients. 15
While robot-assisted ureteral reconstruction is an effective treatment option after KT, it still carries risks. Given that the postoperative complications are low grade (Clavien–Dindo Grade 1–2) and primarily involve UTIs, ileus was reported in two patients,8,9 both of whom underwent surgery using a multi-port robotic system via a transperitoneal approach. This highlights some potential advantages of the single-port (SP) robotic system, which enables an extraperitoneal approach and a single incision, significantly reducing the risk of postoperative gastrointestinal complications. A study by Chen et al. demonstrated the feasibility of SP robot-assisted ureteral reconstruction in three patients, including one who underwent the procedure via an extraperitoneal approach. 23 As the SP system becomes more widely used, further data will likely emerge in the literature.
Conversion to open surgery is another consideration. In this SR, the conversion rate was 4.7%, which remains within acceptable limits. Several strategies can help minimize this risk. First, three-dimensional imaging with computed tomography (CT) or magnetic resonance imaging enhances visualization of the graft ureter’s course. Second, when feasible, retrograde catheterization of the graft ureter or nephrostomy tube placement may allow for indocyanine green visualization, aiding intraoperative identification. Third, ureteral catheterization enables the bedside assistant to mobilize the ureter transurethrally.8,14 Last, knowing the side of the graft kidney before surgery will help in better understanding the anatomy, and intraoperative ultrasound can help localize graft vessels, reducing the risk of injury to the renal hilum. 12 Given that open conversion is associated with a longer postoperative hospital stay, utilizing these techniques to complete the procedure robotically is highly beneficial. 7
In this patient group, particularly among those who develop post-KT ureteral strictures, a critical consideration is the decision regarding the appropriate treatment modality. As highlighted by Caamina et al., further prospectively designed studies are needed to establish standardized protocols and algorithms for these patients. 6 A review of the available literature indicates that, rather than the stricture location itself, the timing of stricture development (post-KT 3 months) and its length are more relevant for the success of endourological interventions.6,24 Taking these factors into account when planning treatment, the results of our review highlight that robotic surgery can be used as a viable option for open surgery in post-transplant surgical reconstruction.
This SR has several limitations. Primarily, most included studies are small case series, reflecting the limited availability of comprehensive data. However, the fact that all studies were published within the last 8 years—with more recent studies reporting larger patient cohorts—suggests that robot-assisted ureteral reconstruction is gaining wider adoption. A second notable limitation is the variability in surgical success criteria across studies. Some studies assessed success based on subjective symptom resolution, while others used objective measures such as renal function stability, radiological imaging (ultrasound or CT) showing hydronephrosis resolution, or functional assessments (renal scan or voiding cystourethrogram) to rule out obstruction or VUR. The third limitation is the lack of a control group, which is not addressed in the included studies. This limits direct comparisons between open, laparoscopic, and robotic approaches. Furthermore, the fact that this SR only included English-language articles has been considered a limitation. Finally, we did not perform a formal publication bias assessment, as the limited number of studies substantially reduces the statistical power of such analyses.
Despite these limitations, this SR makes a valuable contribution to the literature, representing the first comprehensive review focused on robot-assisted ureteral reconstruction for complications following KT. As robotic surgery continues to be integrated into transplantation practice, these findings provide important insights for transplant surgeons and urologists, supporting clinical decision-making and advancing the field of minimally invasive ureteral reconstruction after KT.
Conclusion
The findings of this SR highlight the effectiveness of the robot-assisted approach for managing ureteral complications after KT. This technique demonstrates high treatment success with low major postoperative complication rates, especially when performed in centers with extensive robotic experience.
Authors’ Contributions
H.B.H. and A.P.: Protocol development, data collection, data analysis, article writing, and editing. M.I.D., A.L.-A., B.B.M., T.P., and A.P.: Protocol development and article editing. A.T.: Data analysis and article editing.
Footnotes
Author Disclosure Statement
The authors have no conflicts of interest to declare.
Funding Information
No funding was received for this article.
Data Availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author (H.B.H.) upon reasonable request.
Consent to Publish
All authors gave informed consent for the publication of this study.
Ethical Approval
Ethical approval was not necessary, as we retrieved and analyzed data from previously published studies, where primary investigators obtained informed consent.